
Integration of Clinical and CT-Based Radiomic Features for Pretreatment Prediction of Pathologic Complete Response to Neoadjuvant Systemic Therapy in Breast Cancer
 , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
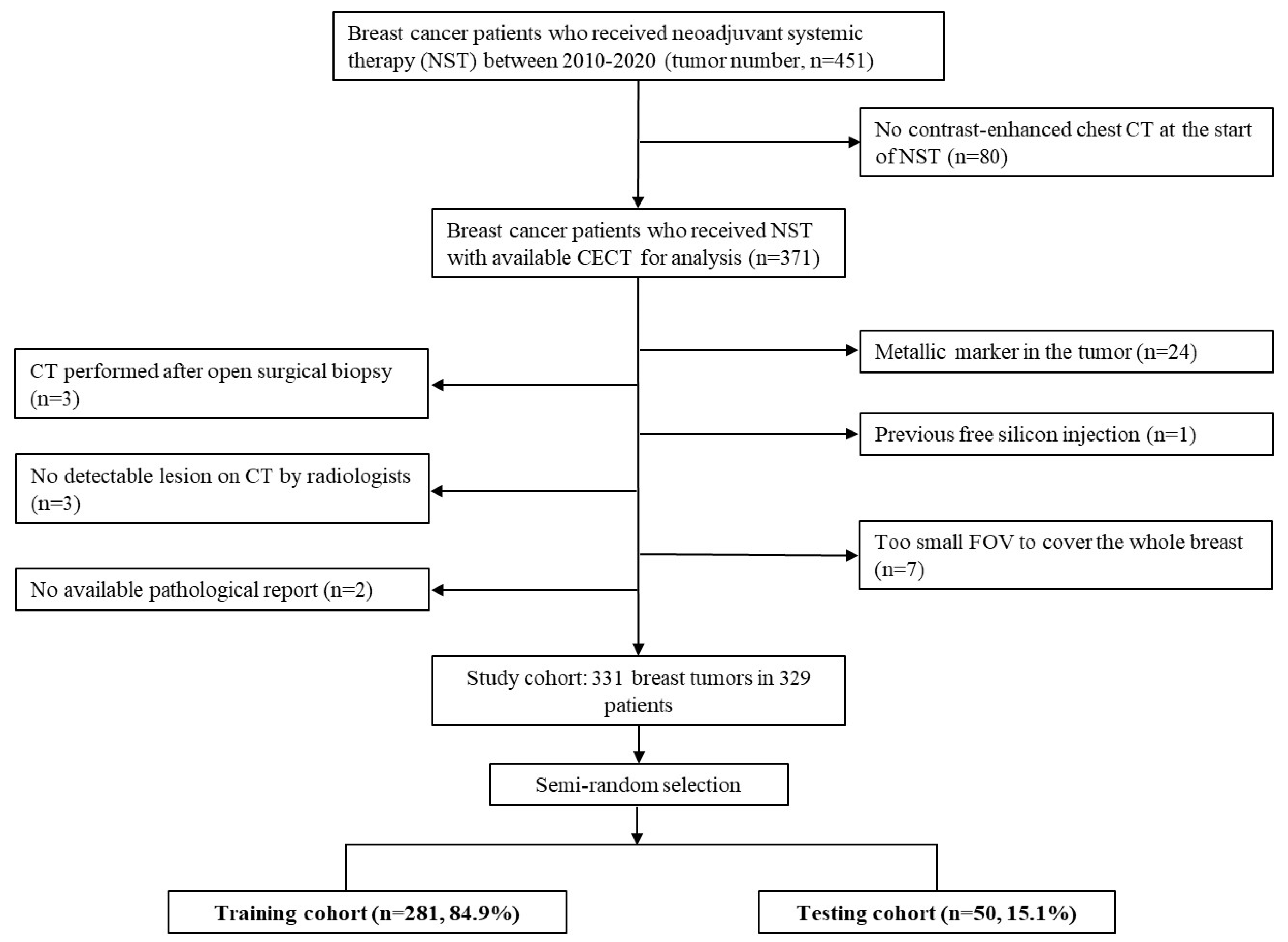
2.1. Study Subjects
2.2. Histopathology Evaluation and Clinical Feature Collection
2.3. Image Acquisition
2.4. Image Segmentation and Feature Extraction
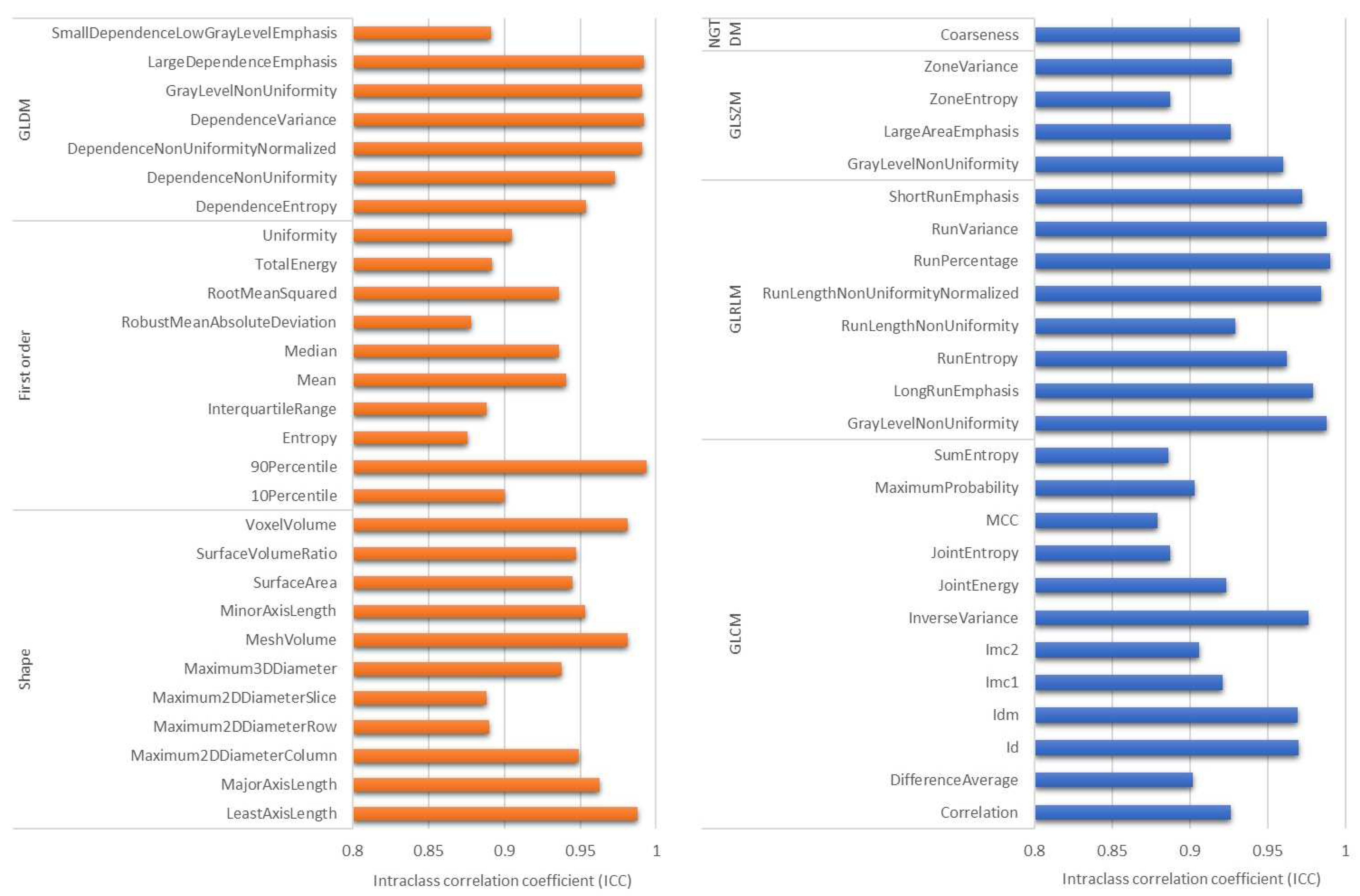
2.5. Inter-Rater Reliability and Feature Reproducibility
2.6. Feature Selection and Model Building
2.7. Statistics
3. Results
3.1. Characteristics of the Study Population
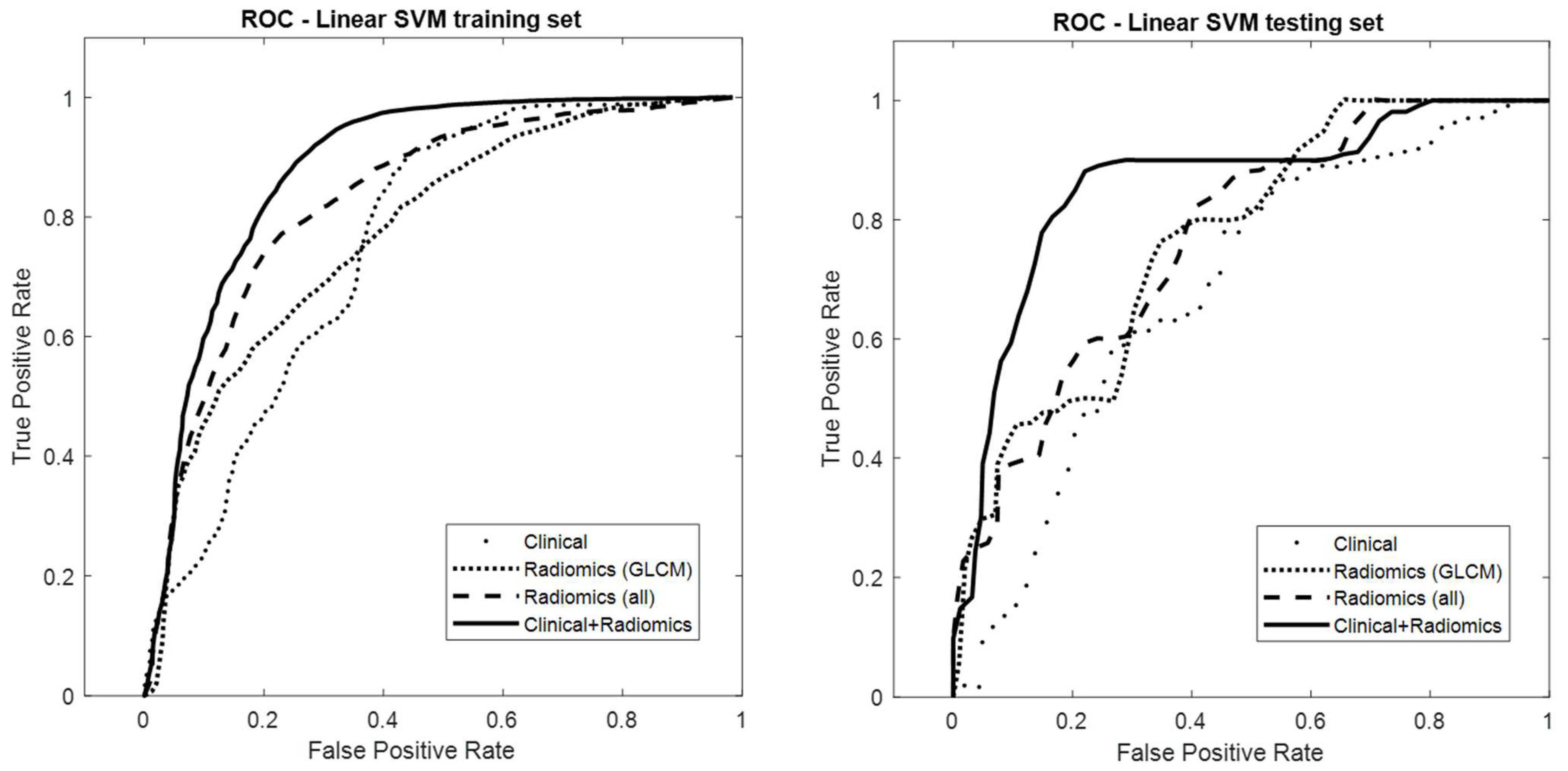
3.2. Model Performance
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- National Comprehensive Cancer Network. Breast Cancer, Version 7.2021. 2021. Available online: https://www.nccn.org/professionals/physician_gls/pdf/breast.pdf (accessed on 27 October 2021).
- Cortazar, P.; Zhang, L.; Untch, M.; Mehta, K.; Costantino, J.P.; Wolmark, N.; Bonnefoi, H.; Cameron, D.; Gianni, L.; Valagussa, P.; et al. Pathological complete response and long-term clinical benefit in breast cancer: The CTNeoBC pooled analysis. Lancet 2014, 384, 164–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Houssami, N.; Macaskill, P.; von Minckwitz, G.; Marinovich, M.L.; Mamounas, E. Meta-analysis of the association of breast cancer subtype and pathologic complete response to neoadjuvant chemotherapy. Eur. J. Cancer 2012, 48, 3342–3354. [Google Scholar] [CrossRef] [PubMed]
- Heil, J.; Kuerer, H.M.; Pfob, A.; Rauch, G.; Sinn, H.; Golatta, M.; Liefers, G.; Peeters, M.V. Eliminating the breast cancer surgery paradigm after neoadjuvant systemic therapy: Current evidence and future challenges. Ann. Oncol. 2020, 31, 61–71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miglietta, F.; Dieci, M.V.; Griguolo, G.; Guarneri, V. Neoadjuvant approach as a platform for treatment personalization: Focus on HER2-positive and triple-negative breast cancer. Cancer Treat. Rev. 2021, 98, 102222. [Google Scholar] [CrossRef]
- Yoon, G.Y.; Chae, E.Y.; Cha, J.H.; Shin, H.J.; Choi, W.J.; Kim, H.H.; Kim, J.E.; Kim, S.-B. Imaging and Clinicopathologic Features Associated with Pathologic Complete Response in HER2-positive Breast Cancer Receiving Neoadjuvant Chemotherapy with Dual HER2 Blockade. Clin. Breast Cancer 2020, 20, 25–32. [Google Scholar] [CrossRef]
- Savaridas, S.L.; Sim, Y.T.; Vinnicombe, S.J.; Purdie, C.A.; Thompson, A.M.; Evans, A. Are baseline ultrasound and mammographic features associated with rates of pathological completes response in patients receiving neoadjuvant chemotherapy for breast cancer? Cancer Imaging 2019, 19, 67. [Google Scholar] [CrossRef]
- Antunovic, L.; De Sanctis, R.; Cozzi, L.; Kirienko, M.; Sagona, A.; Torrisi, R.; Tinterri, C.; Santoro, A.; Chiti, A.; Zelic, R.; et al. PET/CT radiomics in breast cancer: Promising tool for prediction of pathological response to neoadjuvant chemotherapy. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 1468–1477. [Google Scholar] [CrossRef]
- Li, P.; Wang, X.; Xu, C.; Liu, C.; Zheng, C.; Fulham, M.J.; Feng, D.; Wang, L.; Song, S.; Huang, G. (18)F-FDG PET/CT radiomic predictors of pathologic complete response (pCR) to neoadjuvant chemotherapy in breast cancer patients. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 1116–1126. [Google Scholar] [CrossRef]
- Eun, N.L.; Kang, D.; Son, E.J.; Park, J.S.; Youk, J.H.; Kim, J.-A.; Gweon, H.M. Texture Analysis with 3.0-T MRI for Association of Response to Neoadjuvant Chemotherapy in Breast Cancer. Radiology 2020, 294, 31–41. [Google Scholar] [CrossRef]
- Chen, X.; Chen, X.; Yang, J.; Li, Y.; Fan, W.; Yang, Z. Combining Dynamic Contrast-Enhanced Magnetic Resonance Imaging and Apparent Diffusion Coefficient Maps for a Radiomics Nomogram to Predict Pathological Complete Response to Neoadjuvant Chemotherapy in Breast Cancer Patients. J. Comput. Assist. Tomogr. 2020, 44, 275–283. [Google Scholar] [CrossRef]
- Liu, Z.; Li, Z.; Qu, J.; Zhang, R.; Zhou, X.; Li, L.; Sun, K.; Tang, S.; Jiang, H.; Li, H.; et al. Radiomics of Multiparametric MRI for Pretreatment Prediction of Pathologic Complete Response to Neoadjuvant Chemotherapy in Breast Cancer: A Multicenter Study. Clin. Cancer Res. 2019, 25, 3538. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nemeth, A.; Chaudet, P.; Leporq, B.; Heudel, P.-E.; Barabas, F.; Tredan, O.; Treilleux, I.; Coulon, A.; Pilleul, F.; Beuf, O. Multicontrast MRI-based radiomics for the prediction of pathological complete response to neoadjuvant chemotherapy in patients with early triple negative breast cancer. Magma 2021, 34, 833–844. [Google Scholar] [CrossRef] [PubMed]
- Granzier, R.W.Y.; Ibrahim, A.; Primakov, S.P.; Samiei, S.; van Nijnatten, T.; de Boer, M.; Heuts, E.; Hulsmans, F.-J.; Chatterjee, A.; Lambin, P.; et al. MRI-Based Radiomics Analysis for the Pretreatment Prediction of Pathologic Complete Tumor Response to Neoadjuvant Systemic Therapy in Breast Cancer Patients: A Multicenter Study. Cancers 2021, 13, 2447. [Google Scholar] [CrossRef] [PubMed]
- Ha, R.; Chin, C.; Karcich, J.; Liu, M.Z.; Chang, P.; Mutasa, S.; Van Sant, E.P.; Wynn, R.T.; Connolly, E.; Jambawalikar, S. Prior to Initiation of Chemotherapy, Can We Predict Breast Tumor Response? Deep Learning Convolutional Neural Networks Approach Using a Breast MRI Tumor Dataset. J. Digit. Imaging 2019, 32, 693–701. [Google Scholar] [CrossRef] [PubMed]
- Cain, E.H.; Saha, A.; Harowicz, M.R.; Marks, J.R.; Marcom, P.K.; Mazurowski, M.A. Multivariate machine learning models for prediction of pathologic response to neoadjuvant therapy in breast cancer using MRI features: A study using an independent validation set. Breast Cancer Res. Treat. 2019, 173, 455–463. [Google Scholar] [CrossRef]
- Rizzo, S.; Botta, F.; Raimondi, S.; Origgi, D.; Fanciullo, C.; Morganti, A.G.; Bellomi, M. Radiomics: The facts and the challenges of image analysis. Eur. Radiol. Exp. 2018, 2, 36. [Google Scholar] [CrossRef]
- Valdora, F.; Houssami, N.; Rossi, F.; Calabrese, M.; Tagliafico, A.S. Rapid review: Radiomics and breast cancer. Breast Cancer Res. Treat. 2018, 169, 217–229. [Google Scholar] [CrossRef]
- Moghadas-Dastjerdi, H.; Sha-E-Tallat, H.R.; Sannachi, L.; Sadeghi-Naini, A.; Czarnota, G.J. A priori prediction of tumour response to neoadjuvant chemotherapy in breast cancer patients using quantitative CT and machine learning. Sci. Rep. 2020, 10, 10936. [Google Scholar] [CrossRef]
- Moghadas-Dastjerdi, H.; Rahman, S.H.; Sannachi, L.; Wright, F.C.; Gandhi, S.; Trudeau, M.E.; Sadeghi-Naini, A.; Czarnota, G.J. Prediction of chemotherapy response in breast cancer patients at pre-treatment using second derivative texture of CT images and machine learning. Transl. Oncol. 2021, 14, 101183. [Google Scholar] [CrossRef]
- Huang, X.; Mai, J.; Huang, Y.; He, L.; Chen, X.; Wu, X.; Li, Y.; Yang, X.; Dong, M.; Huang, J.; et al. Radiomic Nomogram for Pretreatment Prediction of Pathologic Complete Response to Neoadjuvant Therapy in Breast Cancer: Predictive Value of Staging Contrast-enhanced CT. Clin. Breast Cancer 2021, 21, e388–e401. [Google Scholar] [CrossRef]
- Zwanenburg, A.; Vallières, M.; Abdalah, M.A.; Aerts, H.J.W.L.; Andrearczyk, V.; Apte, A.; Ashrafinia, S.; Bakas, S.; Beukinga, R.J.; Boellaard, R.; et al. The Image Biomarker Standardization Initiative: Standardized Quantitative Radiomics for High-Throughput Image-based Phenotyping. Radiology 2020, 295, 328–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Griethuysen, J.J.M.; Fedorov, A.; Parmar, C.; Hosny, A.; Aucoin, N.; Narayan, V.; Beets-Tan, R.G.H.; Fillion-Robin, J.-C.; Pieper, S.; Aerts, H.J.W.L. Computational Radiomics System to Decode the Radiographic Phenotype. Cancer Res. 2017, 77, e104–e107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Velazquez, E.R.; Parmar, C.; Jermoumi, M.; Mak, R.H.; Van Baardwijk, A.; Fennessy, F.M.; Lewis, J.H.; De Ruysscher, D.; Kikinis, R.; Lambin, P.; et al. Volumetric CT-based segmentation of NSCLC using 3D-Slicer. Sci. Rep. 2013, 2013, 3529. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dice, L.R. Measures of the Amount of Ecologic Association Between Species. Ecology 1945, 26, 297–302. [Google Scholar] [CrossRef]
- DeLong, E.R.; DeLong, D.M.; Clarke-Pearson, D.L. Comparing the Areas under Two or More Correlated Receiver Operating Characteristic Curves: A Nonparametric Approach. Biometrics 1988, 44, 837–845. [Google Scholar] [CrossRef]
- Liu, H.; Cocea, M. Semi-random partitioning of data into training and test sets in granular computing context. Granul. Comput. 2017, 2, 357–386. [Google Scholar] [CrossRef] [Green Version]
- Larsen, B.S.; Synthetic Minority Over-sampling Technique (SMOTE). GitHub. 2022. Available online: https://github.com/dkbsl/matlab_smote/releases/tag/1.0 (accessed on 8 December 2022).
- Nitesh, V.C.; Kevin, W.B.; Lawrence, O.H.; Kegelmeyer, W. SMOTE: Synthetic minority over-sampling technique. J. Artif. Intellig. Res. 2002, 16, 321–357. [Google Scholar]
- Hou, Z.; Yang, Y.; Li, S.; Yan, J.; Ren, W.; Liu, J.; Wang, K.; Liu, B.; Wan, S. Radiomic analysis using contrast-enhanced CT: Predict treatment response to pulsed low dose rate radiotherapy in gastric carcinoma with abdominal cavity metastasis. Quant. Imaging Med. Surg. 2018, 8, 410–420. [Google Scholar] [CrossRef]
- Luo, H.-S.; Huang, S.-F.; Xu, H.-Y.; Li, X.-Y.; Wu, S.-X.; Wu, D.-H. A nomogram based on pretreatment CT radiomics features for predicting complete response to chemoradiotherapy in patients with esophageal squamous cell cancer. Radiat. Oncol. 2020, 15, 249. [Google Scholar] [CrossRef]
- Rundo, L.; Beer, L.; Escudero Sanchez, L.; Crispin-Ortuzar, M.; Reinius, M.; McCague, C.; Sahin, H.; Bura, V.; Pintican, R.; Zerunian, M.; et al. Clinically Interpretable Radiomics-Based Prediction of Histopathologic Response to Neoadjuvant Chemotherapy in High-Grade Serous Ovarian Carcinoma. Front. Oncol. 2022, 12, 868265. [Google Scholar] [CrossRef]
- Tewari, M.; Krishnamurthy, A.; Shukla, H.S. Predictive markers of response to neoadjuvant chemotherapy in breast cancer. Surg. Oncol. 2008, 17, 301–311. [Google Scholar] [CrossRef] [PubMed]
- Davey, M.G.; Ryan, É.J.; Boland, M.R.; Barry, M.K.; Lowery, A.J.; Kerin, M.J. Clinical utility of the 21-gene assay in predicting response to neoadjuvant endocrine therapy in breast cancer: A systematic review and meta-analysis. Breast 2021, 58, 113–120. [Google Scholar] [CrossRef] [PubMed]
- Fan, H.; Li, C.; Xiang, Q.; Xu, L.; Zhang, Z.; Liu, Q.; Zhang, T.; Zhou, Y.; Zhao, X.; Cui, Y. PIK3CA mutations and their response to neoadjuvant treatment in early breast cancer: A systematic review and meta-analysis. Thorac. Cancer 2018, 9, 571–579. [Google Scholar] [CrossRef]
- Tao, M.; Chen, S.; Zhang, X.; Zhou, Q. Ki-67 labeling index is a predictive marker for a pathological complete response to neoadjuvant chemotherapy in breast cancer: A meta-analysis. Medicine 2017, 96, e9384. [Google Scholar] [CrossRef] [PubMed]
- Gao, Z.H.; Li, C.X.; Liu, M.; Jiang, J.Y. Predictive and prognostic role of tumour-infiltrating lymphocytes in breast cancer patients with different molecular subtypes: A meta-analysis. BMC Cancer 2020, 20, 1150. [Google Scholar] [CrossRef]
- Qiu, Q.; Duan, J.; Gong, G.; Lu, Y.; Li, D.; Lu, J.; Yin, Y. Reproducibility of radiomic features with GrowCut and GraphCut semiautomatic tumor segmentation in hepatocellular carcinoma. Transl. Cancer Res. 2017, 6, 940–948. [Google Scholar] [CrossRef]
- Xue, C.; Yuan, J.; Lo, G.G.; Chang, A.T.Y.; Poon, D.M.C.; Wong, O.L.; Zhou, Y.; Chu, W.C.W. Radiomics feature reliability assessed by intraclass correlation coefficient: A systematic review. Quant. Imaging Med. Surg. 2021, 11, 4431–4460. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Training | Testing | Total | p-Value | |
|---|---|---|---|---|
| Clinical Variables | N = 280, 84.6% | N = 51, 15.4% | N = 331, 100% | |
| pCR ‡ | 0.804 | |||
| Negative | 232 (82.6) | 42 (84.0) | 274 (82.8) | |
| Positive | 49 (17.4) | 8 (16.0) | 57 (17.2) | |
| Age | 51.5 ± 9.8 | 52.5 ± 8.9 | 51.6 ± 9.7 | 0.5 |
| Clinical stage | 0.741 | |||
| 1 | 15 (5.3) | 1 (2.0) | 16 (4.8) | |
| 2 | 107 (38.1) | 21 (42.0) | 128 (38.7) | |
| 3 | 79 (28.1) | 13 (26.0) | 92 (27.8) | |
| 4 | 80 (28.5) | 15 (30.0) | 95 (28.7) | |
| Breast cancer subtype § | 0.951 | |||
| HR(+), HER2(−) | 123 (43.8) | 23 (46.0) | 146 (44.1) | |
| HR(+), HER2(+) | 68 (24.2) | 11 (22.0) | 79 (23.9) | |
| HR(−), HER2(+) | 45 (16.0) | 9 (18.0) | 54 (16.3) | |
| Triple-negative | 45 (16.0) | 7 (14.0) | 52 (15.7) | |
| Histology | 0.067 | |||
| Invasive carcinoma of no special type | 263 (93.6) | 42 (84.0) | 305 (92.1) | |
| Invasive lobular carcinoma | 7 (2.5) | 3 (6.0) | 10 (3.0) | |
| Others | 11 (3.9) | 5 (10.0) | 16 (4.8) | |
| Imaging variables | N = 279, 84.8% | N = 50, 15.2% | N = 329, 100% | |
| Manufacturer | 0.971 | |||
| GE Healthcare | 114 (40.9) | 20 (40.0) | 134 (40.7) | |
| PHILIPS | 48 (17.2) | 10 (20.0) | 58 (17.6) | |
| SIEMENS | 87 (31.2) | 15 (30.0) | 102 (31.0) | |
| TOSHIBA | 30 (10.8) | 5 (10.0) | 35 (10.6) | |
| Institution | 0.533 | |||
| KMUH † | 236 (84.6) | 44 (88.0) | 280 (85.1) | |
| Other hospitals | 43 (15.4) | 6 (12.0) | 49 (14.9) |
| Cancer Subtype | Non-pCR (n = 274, 82.8) | pCR (N = 57, 17.2) | Total (N = 331, 100) | p-Value |
|---|---|---|---|---|
| HR(+), HER2(−) | 137 (93.8) | 9 (6.2) | 146 (100) | <0.001 |
| HR(+), HER2(+) | 60 (75.9) | 19 (24.1) | 79 (100) | |
| HR(−), HER2(+) | 36 (66.7) | 18 (33.3) | 54 (100) | |
| Triple-negative | 41 (78.8) | 11 (21.2) | 52 (100) |
| Model | Features | Training Dataset | Testing Dataset | ||||
|---|---|---|---|---|---|---|---|
| AUC | Sensitivity | Specificity | AUC | Sensitivity | Specificity | ||
| LASSO | Clinical | 0.79 (0.78, 0.79) | 0.82 (0.80, 0.84) | 0.65 (0.63, 0.66) | 0.69 (0.68, 0.69) | 0.53 (0.44, 0.62) | 0.76 (0.73, 0.80) |
| Radiomics | 0.82 (0.82, 0.83) | 0.78 (0.75, 0.80) | 0.76 (0.74, 0.78) | 0.76 (0.75, 0.77) | 0.57 (0.54, 0.60) | 0.83 (0.80, 0.86) | |
| Clinical-Radiomics | 0.90 (0.90, 0.90) | 0.93 (0.92, 0.95) | 0.74 (0.72, 0.76) | 0.86 (0.86, 0.87) | 0.90 (0.90, 0.90) | 0.84 (0.83, 0.85) | |
| Linear SVM | Clinical | 0.76 (0.76, 0.77) | 0.89 (0.86, 0.91) | 0.60 (0.56, 0.63) | 0.69 (0.69, 0.70) | 0.53 (0.46, 0.60) | 0.77 (0.74, 0.80) |
| Radiomics | 0.83 (0.83, 0.83) | 0.76 (0.72, 0.79) | 0.79 (0.77, 0.82) | 0.78 (0.77, 0.79) | 0.59 (0.55, 0.63) | 0.84 (0.80, 0.87) | |
| Clinical-Radiomics | 0.88 (0.88, 0.89) | 0.90 (0.88, 0.92) | 0.75 (0.73, 0.76) | 0.87 (0.86, 0.88) | 0.90 (0.90, 0.90) | 0.82 (0.80, 0.84) | |
| All Radiomic Features (ICC ≥ 0.85) | GLCM-Based Features (ICC ≥ 0.85) | |||||
|---|---|---|---|---|---|---|
| Model | Clinical | Radiomics | Clinical–Radiomics | Clinical | Radiomics | Clinical–Radiomics |
| Clinical | 1 | <0.001 | <0.001 | 1 | <0.001 | <0.001 |
| Radiomics | 1 | <0.001 | 1 | <0.001 | ||
| Clinical–radiomics | 1 | 1 | ||||
| Features ‡ | Model | AUC | Sensitivity | Specificity | p-Value § |
|---|---|---|---|---|---|
| Radiomics (GLCM) | Linear SVM | 0.77 (0.77, 0.79) | 0.54 (0.51, 0.57) | 0.84 (0.80, 0.88) | 0.45 |
| Radiomics (All) | Linear SVM | 0.78 (0.77, 0.79) | 0.59 (0.55, 0.63) | 0.83 (0.80, 0.87) | |
| Clinical–radiomics (GLCM) | Linear SVM | 0.85 (0.84, 0.85) | 0.85 (0.79, 0.91) | 0.78 (0.74, 0.82) | 0.011 |
| Clinical–radiomics (All) | Linear SVM | 0.87 (0.86, 0.88) | 0.90 (0.90, 0.90) | 0.82 (0.80, 0.84) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsai, H.-Y.; Tsai, T.-Y.; Wu, C.-H.; Chung, W.-S.; Wang, J.-C.; Hsu, J.-S.; Hou, M.-F.; Chou, M.-C. Integration of Clinical and CT-Based Radiomic Features for Pretreatment Prediction of Pathologic Complete Response to Neoadjuvant Systemic Therapy in Breast Cancer. Cancers 2022, 14, 6261. https://doi.org/10.3390/cancers14246261
Tsai H-Y, Tsai T-Y, Wu C-H, Chung W-S, Wang J-C, Hsu J-S, Hou M-F, Chou M-C. Integration of Clinical and CT-Based Radiomic Features for Pretreatment Prediction of Pathologic Complete Response to Neoadjuvant Systemic Therapy in Breast Cancer. Cancers. 2022; 14(24):6261. https://doi.org/10.3390/cancers14246261
Chicago/Turabian StyleTsai, Huei-Yi, Tsung-Yu Tsai, Chia-Hui Wu, Wei-Shiuan Chung, Jo-Ching Wang, Jui-Sheng Hsu, Ming-Feng Hou, and Ming-Chung Chou. 2022. "Integration of Clinical and CT-Based Radiomic Features for Pretreatment Prediction of Pathologic Complete Response to Neoadjuvant Systemic Therapy in Breast Cancer" Cancers 14, no. 24: 6261. https://doi.org/10.3390/cancers14246261