
Promote Community Engagement in Participatory Research for Improving Breast Cancer Prevention: The P.I.N.K. Study Framework

 , , , , , , and
, , , , , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. The PINK Study Data and the Study Population
2.2. Traditional Statistical Analysis and Network Implementation
3. Results
3.1. Population Characteristics
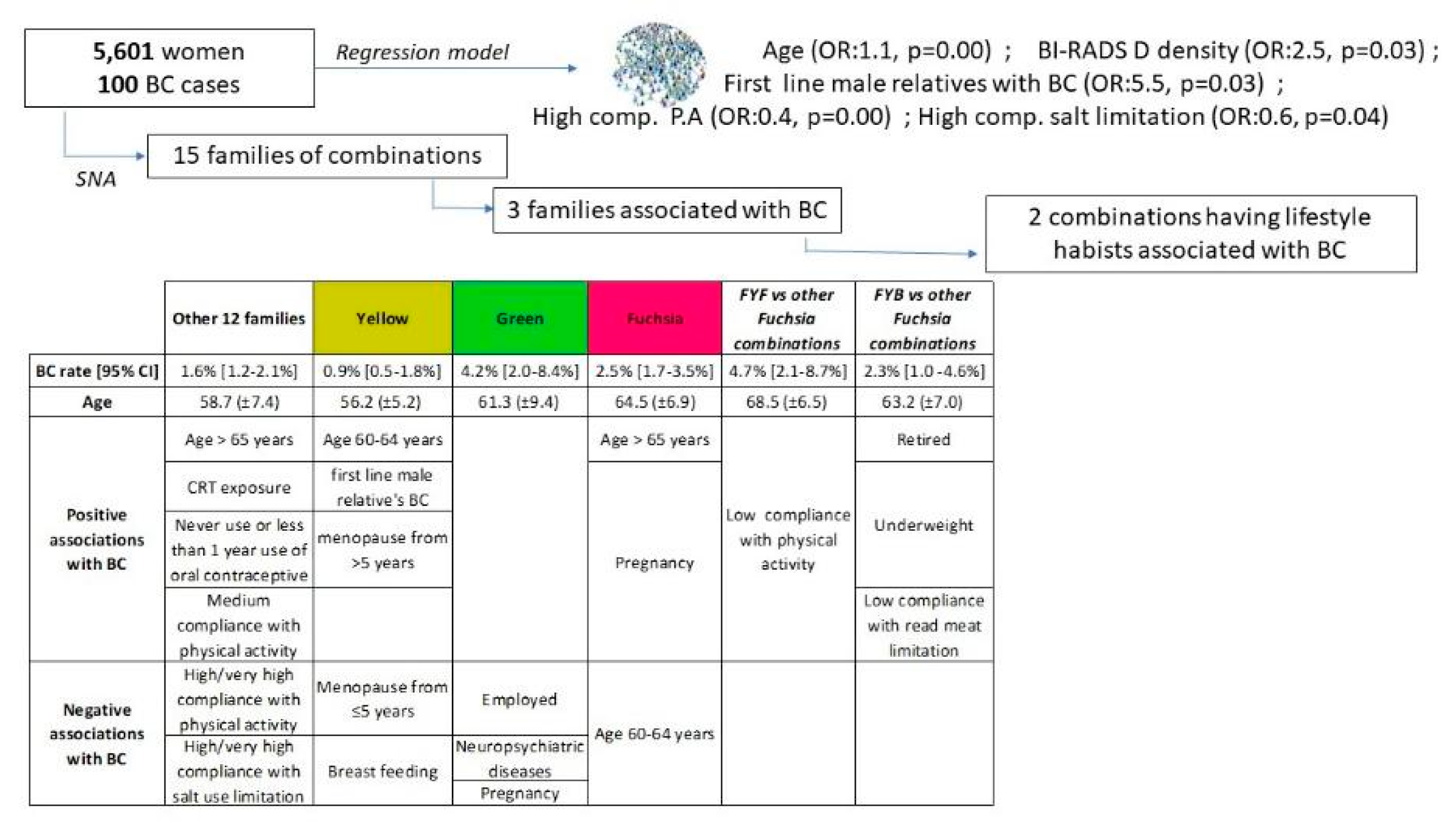
3.2. Binomial Logistic Model
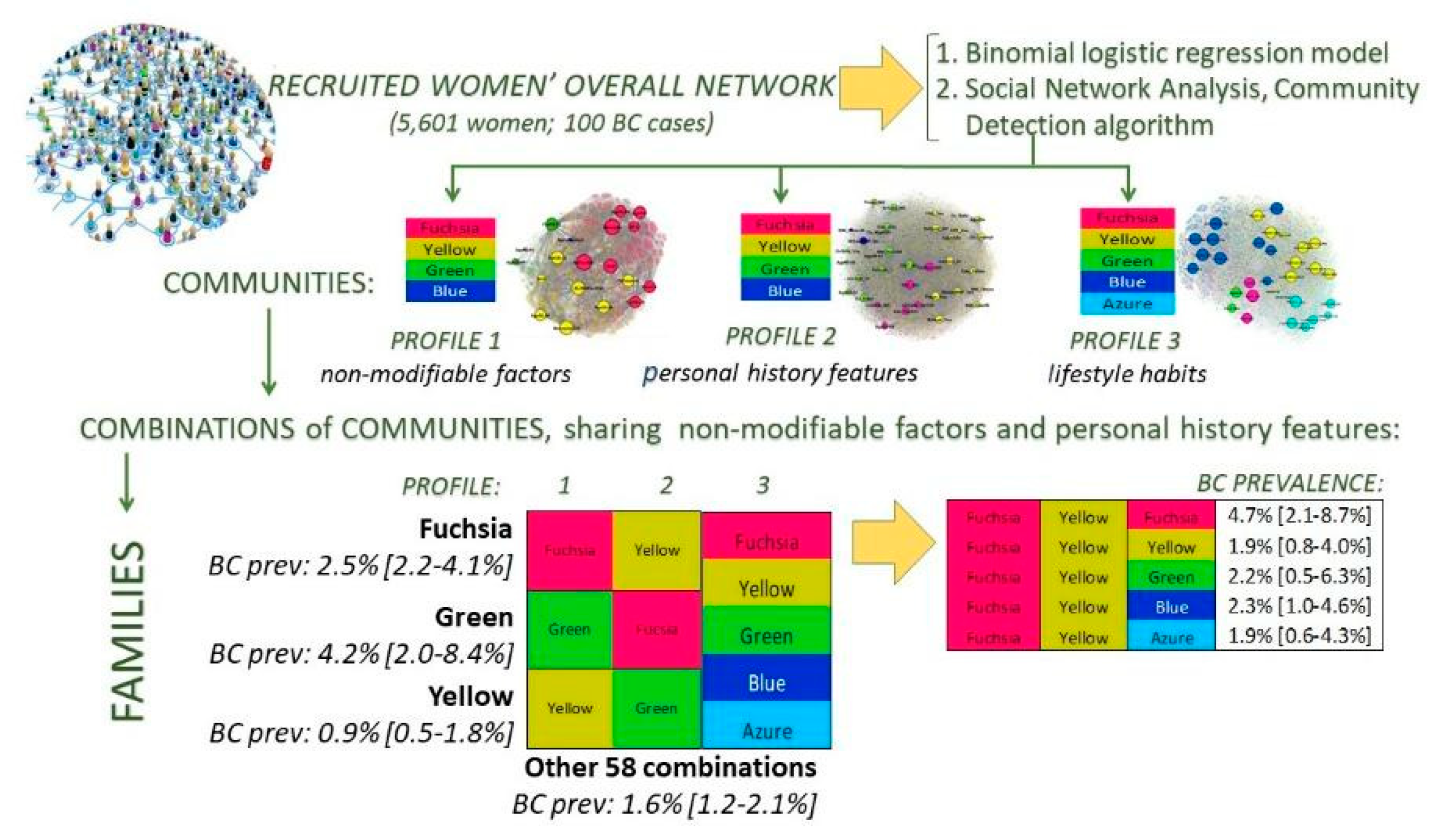
3.3. Social Network Analysis
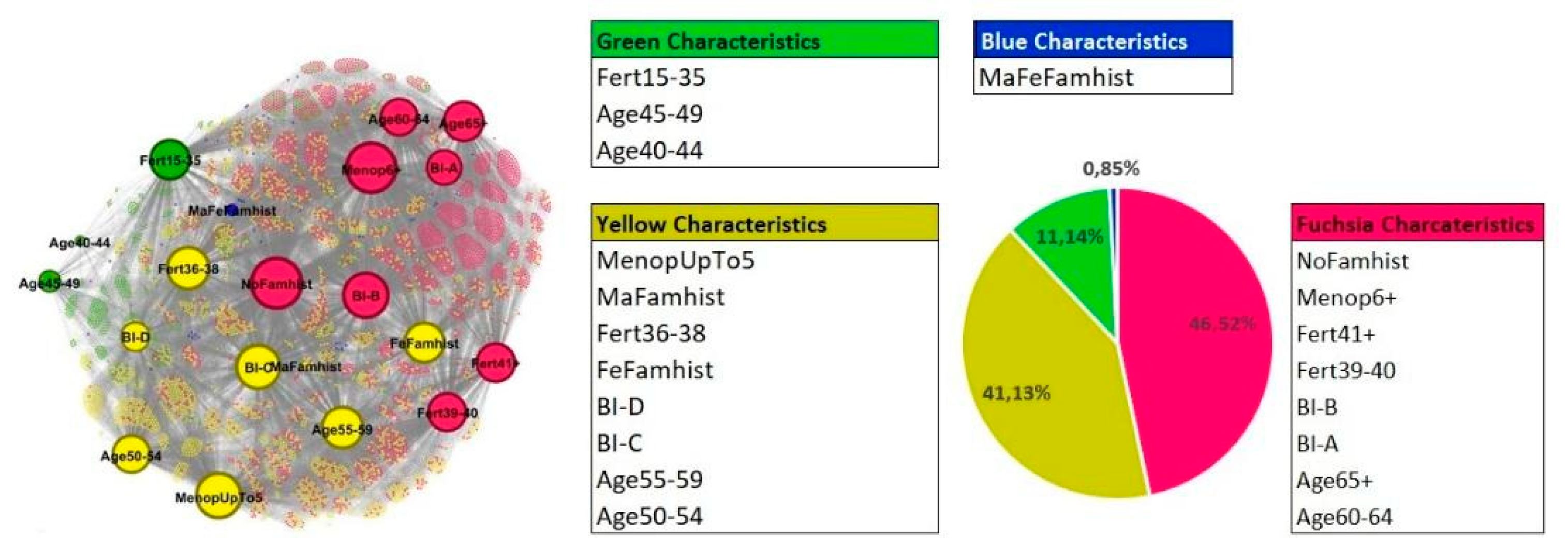
- Non-modifiable factors (Profile 1)
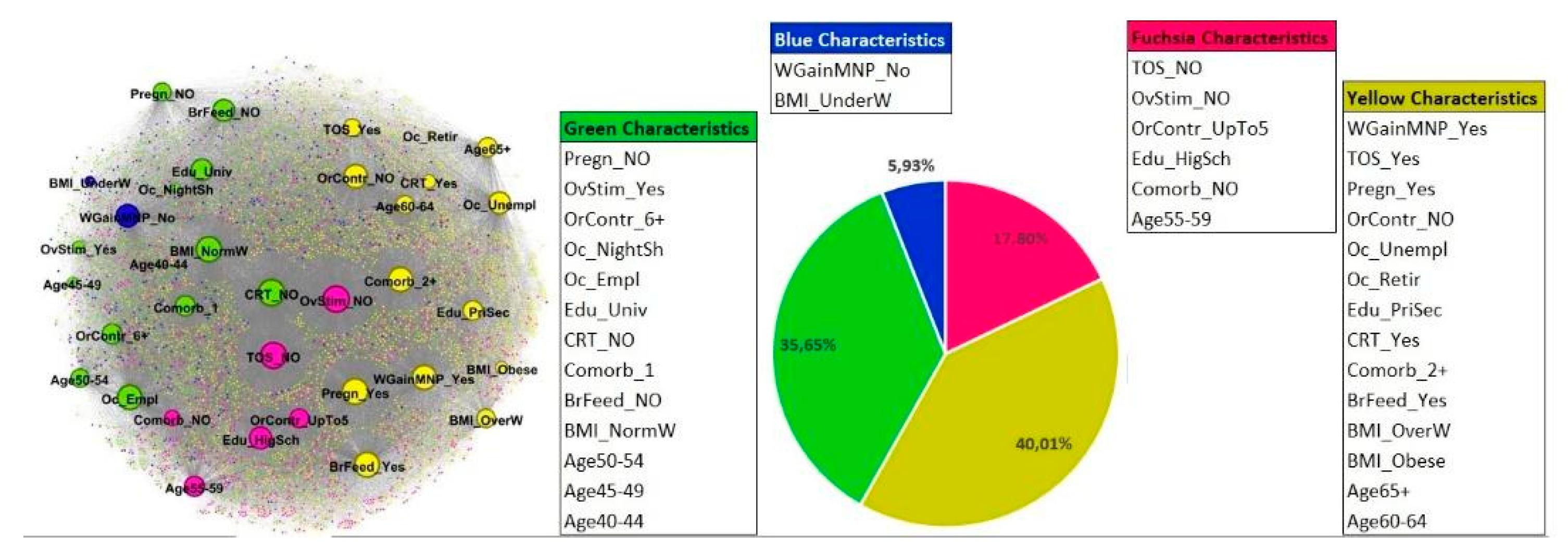
- Personal history features (Profile 2)
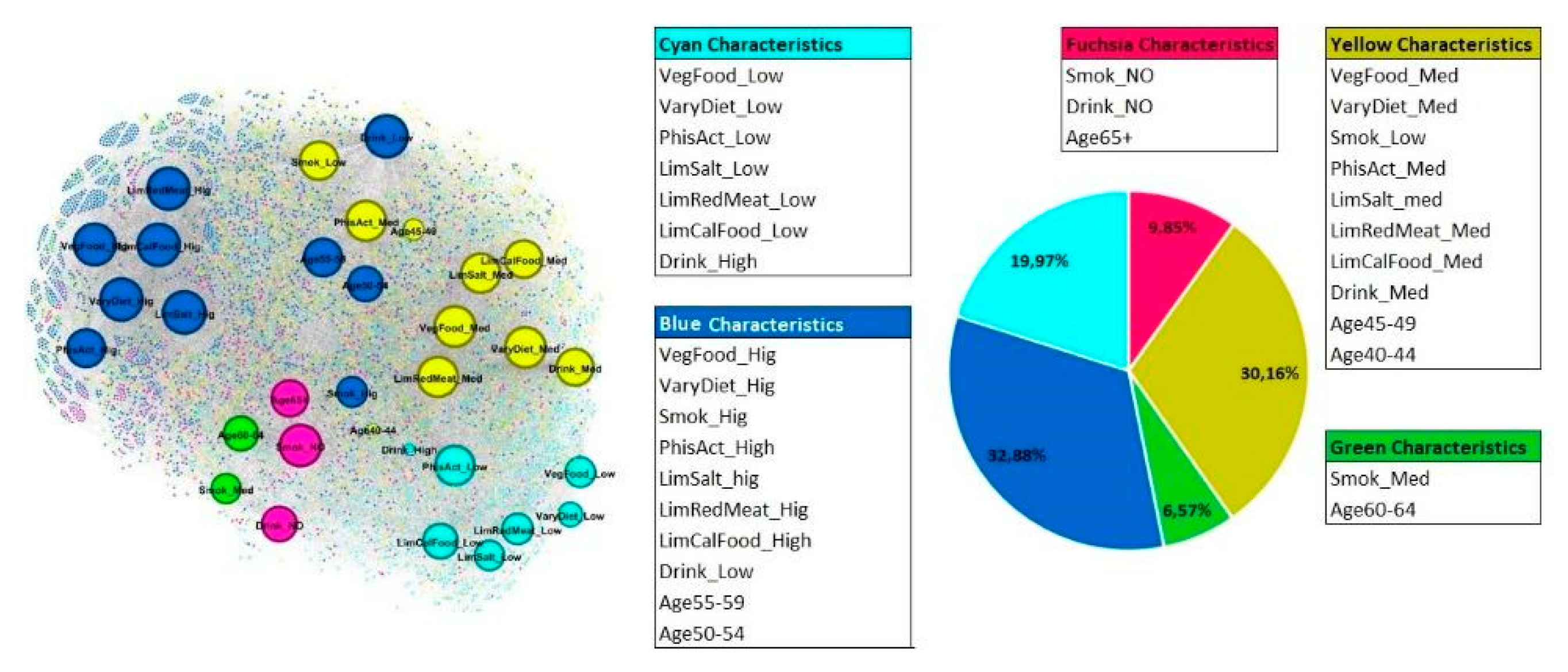
- Lifestyle habits (Profile 3)
3.4. Combination of Profiles
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Breast Cancer Now Most Common Form of Cancer: WHO Taking Action. Available online: https://www.who.int/news/item/03-02-2021-breast-cancer-now-most-common-form-of-cancer-who-taking-action (accessed on 11 November 2022).
- Ferlay, J.; Ervik, M.; Lam, F.; Colombet, M.; Mery, L.; Piñeros, M.; Znaor, A.; Soerjomataram, I.; Bray, F. Global Cancer Obser-Vatory: Cancer Today. International Agency for Research on Cancer; Lyon, France: 2020. Available online: https://gco.iarc.fr/today (accessed on 6 November 2022).
- Zielonke, N.; Gini, A.; Jansen, E.E.L.; Anttila, A.; Segnan, N.; Ponti, A.; Veerus, P.; de Koning, H.J.; van Ravesteyn, N.T.; Heijnsdijk, E.A.M.; et al. Evidence for reducing cancer-specific mortality due to screening for breast cancer in Europe: A systematic review. Eur. J. Cancer 2020, 127, 191–206. [Google Scholar] [CrossRef] [Green Version]
- Pashayan, N.; Morris, S.; Gilbert, F.J.; Pharoah, P.D.P. Cost-effectiveness and Benefit-to-Harm Ratio of Risk-Stratified Screening for Breast Cancer: A Life-Table Model. JAMA Oncol. 2018, 4, 1504–1510. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Onega, T.; Beaber, E.F.; Sprague, B.L.; Barlow, W.E.; Haas, J.S.; Tosteson, A.N.; Schnall, M.D.; Armstrong, K.; Schapira, M.M.; Geller, B.; et al. Breast cancer screening in an era of personalized regimens: A conceptual model and National Cancer Institute initiative for risk-based and preference-based approaches at a population level. Cancer 2014, 120, 2955–2964. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McWilliams, L.; Evans, D.G.; Payne, K.; Harrison, F.; Howell, A.; Howell, S.J.; French, D.P.; Breast Screening Risk-Stratification Agenda Setting Group. Implementing Risk-Stratified Breast Screening in England: An Agenda Setting Meeting. Cancers 2022, 14, 4636. [Google Scholar] [CrossRef] [PubMed]
- Vilmun, B.M.; Vejborg, I.; Lynge, E.; Lillholm, M.; Nielsen, M.; Nielsen, M.B.; Carlsen, J.F. Impact of adding breast density to breast cancer risk models: A systematic review. Eur. J. Radiol. 2020, 127, 109019. [Google Scholar] [CrossRef]
- Engmann, N.J.; Golmakani, M.K.; Miglioretti, D.L.; Sprague, B.L.; Kerlikowske, K.; Breast Cancer Surveillance Consortium. Population-Attributable Risk Proportion of Clinical Risk Factors for Breast Cancer. JAMA Oncol. 2017, 3, 1228–1236, Erratum in JAMA Oncol. 2019, 5, 1643. [Google Scholar] [CrossRef] [Green Version]
- Cintolo-Gonzalez, J.A.; Braun, D.; Blackford, A.L.; Mazzola, E.; Acar, A.; Plichta, J.K.; Griffin, M.; Hughes, K.S. Breast cancer risk models: A comprehensive overview of existing models, validation, and clinical applications. Breast Cancer Res. Treat. 2017, 164, 263–284. [Google Scholar] [CrossRef]
- Louro, J.; Posso, M.; Hilton Boon, M.; Román, M.; Domingo, L.; Castells, X.; Sala, M. A systematic review and quality assessment of individualised breast cancer risk prediction models. Br. J. Cancer 2019, 121, 76–85. [Google Scholar] [CrossRef] [Green Version]
- Clift, A.K.; Dodwell, D.; Lord, S.; Petrou, S.; Brady, S.M.; Collins, G.S.; Hippisley-Cox, J. The current status of risk-stratified breast screening. Br. J. Cancer 2022, 126, 533–550. [Google Scholar] [CrossRef]
- Nindrea, R.D.; Aryandono, T.; Lazuardi, L. Breast Cancer Risk From Modifiable and Non-Modifiable Risk Factors among Women in Southeast Asia: A Meta-Analysis. Asian Pac. J Cancer Prev. 2017, 18, 3201–3206. [Google Scholar] [CrossRef] [PubMed]
- Anothaisintawee, T.; Wiratkapun, C.; Lerdsitthichai, P.; Kasamesup, V.; Wongwaisayawan, S.; Srinakarin, J.; Hirunpat, S.; Woodtichartpreecha, P.; Boonlikit, S.; Teerawattananon, Y.; et al. Risk factors of breast cancer: A systematic review and meta-analysis. Asia Pac. J. Public Health 2013, 25, 368–387. [Google Scholar] [CrossRef] [PubMed]
- American Cancer Society. Breast Cancer Facts & Figures 2013–2014; American Cancer Society, Inc.: Atlanta, GA, USA, 2013. [Google Scholar]
- Endogenous Hormones and Breast Cancer Collaborative Group; Key, T.J.; Appleby, P.N.; Reeves, G.K.; Roddam, A.W.; Helzlsouer, K.J.; Alberg, A.J.; Rollison, D.E.; Dorgan, J.F.; Brinton, L.A.; et al. Circulating sex hormones and breast cancer risk factors in postmenopausal women: Reanalysis of 13 studies. Br. J. Cancer 2011, 105, 709–722. [Google Scholar] [CrossRef] [PubMed]
- Xue, F.; Michels, K.B. Intrauterine factors and risk of breast cancer: A systematic review and meta-analysis of current evidence. Lancet Oncol. 2007, 8, 1088–1100, Erratum in Lancet Oncol. 2014, 15, e106. [Google Scholar] [CrossRef] [PubMed]
- Brisken, C. Progesterone signalling in breast cancer: A neglected hormone coming into the limelight. Nat Rev Cancer. 2013, 13, 385–396. [Google Scholar] [CrossRef] [PubMed]
- Obr, A.E.; Edwards, D.P. The biology of progesterone receptor in the normal mammary gland and in breast cancer. Mol. Cell Endocrinol. 2012, 357, 4–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cleary, M.P.; Grossmann, M.E. Minireview: Obesity and breast cancer: The estrogen connection. Endocrinology 2009, 150, 2537–2542. [Google Scholar] [CrossRef]
- Collaborative Group on Hormonal Factors in Breast Cancer. Menarche, menopause, and breast cancer risk: Individual participant meta-analysis, including 118 964 women with breast cancer from 117 epidemiological studies. Lancet Oncol. 2012, 13, 1141–1151. [Google Scholar] [CrossRef]
- Macon, M.B.; Fenton, S.E. Endocrine disruptors and the breast: Early life effects and later life disease. J. Mammary Gland. Biol. Neoplasia. 2013, 18, 43–61. [Google Scholar] [CrossRef] [Green Version]
- World Cancer Research Fund/American Institute for Cancer Research. Diet, Nutrition, Physical Activity and Cancer: A Global Perspective. Continuous Update Project Expert Report 2018. 2018. Available online: http://www.dietandcancerreport.org (accessed on 29 August 2022).
- Chan, D.S.M.; Abar, L.; Cariolou, M.; Nanu, N.; Greenwood, D.C.; Bandera, E.V.; McTiernan, A.; Norat, T. World Cancer Research Fund International: Continuous Update Project-systematic literature review and meta-analysis of observational cohort studies on physical activity, sedentary behavior, adiposity, and weight change and breast cancer risk. Cancer Causes Control 2019, 30, 1183–1200. [Google Scholar] [CrossRef] [Green Version]
- Harvie, M.; Howell, A.; Evans, D.G. Can diet and lifestyle prevent breast cancer: What is the evidence? Am. Soc. Clin. Oncol. Educ. Book 2015, 35, e66–e73. [Google Scholar] [CrossRef]
- Hilakivi-Clarke, L.; Cabanes, A.; de Assis, S.; Wang, M.; Khan, G.; Shoemaker, W.J.; Stevens, R.G. In utero alcohol exposure increases mammary tumorigenesis in rats. Br. J. Cancer 2004, 90, 2225–2231. [Google Scholar] [CrossRef] [PubMed]
- Vona-Davis, L.; Rose, D.P. Type 2 diabetes and obesity metabolic interactions: Common factors for breast cancer risk and novel approaches to prevention and therapy. Curr. Diabetes Rev. 2012, 8, 116–130. [Google Scholar] [CrossRef] [PubMed]
- Carreras, G.; Lachi, A.; Boffi, R.; Clancy, L.; Gallus, S.; Fernández, E.; López, M.J.; Soriano, J.B.; López Nicolás, Á.; Semple, S.; et al. Burden of disease from breast cancer attributable to smoking and second-hand smoke exposure in Europe. Int. J. Cancer 2020, 147, 2387–2393. [Google Scholar] [CrossRef] [PubMed]
- Pizzato, M.; Carioli, G.; Rosso, S.; Zanetti, R.; Negri, E.; La Vecchia, C. Cigarettes smoking and androgen receptor-positive breast cancer. Eur. J. Cancer Prev. 2021, 30, 469–471. [Google Scholar] [CrossRef] [PubMed]
- Catsburg, C.; Miller, A.B.; Rohan, T.E. Adherence to cancer prevention guidelines and risk of breast cancer. Int. J. Cancer 2014, 135, 2444–2452. [Google Scholar] [CrossRef]
- Joukes, E.; Abu-Hanna, A.; Cornet, R.; de Keizer, N.F. Time Spent on Dedicated Patient Care and Documentation Tasks Before and After the Introduction of a Structured and Standardized Electronic Health Record. Appl. Clin. Inform. 2018, 9, 46–53. [Google Scholar] [CrossRef] [Green Version]
- Schmitz, K.H.; Campbell, A.M.; Stuiver, M.M.; Pinto, B.M.; Schwartz, A.L.; Morris, G.S.; Ligibel, J.A.; Cheville, A.; Galvão, D.A.; Alfano, C.M.; et al. Exercise is medicine in oncology: Engaging clinicians to help patients move through cancer. CA Cancer J. Clin. 2019, 69, 468–484. [Google Scholar] [CrossRef] [Green Version]
- Villarini, M.; Lanari, C.; Nucci, D.; Gianfredi, V.; Marzulli, T.; Berrino, F.; Borgo, A.; Bruno, E.; Gargano, G.; Moretti, M.; et al. Community-based participatory research to improve life quality and clinical outcomes of patients with breast cancer (DianaWeb in Umbria pilot study). BMJ Open 2016, 6, e009707. [Google Scholar] [CrossRef] [Green Version]
- Thomas, J.A.; Miller, E.R.; Ward, P.R. Lifestyle Interventions through Participatory Research: A Mixed-Methods Systematic Review of Alcohol and Other Breast Cancer Behavioural Risk Factors. Int. J. Env. Res. Public Health 2022, 19, 980. [Google Scholar] [CrossRef]
- Evans, D.G.; Astley, S.; Stavrinos, P.; Harkness, E.; Donnelly, L.S.; Dawe, S.; Jacob, I.; Harvie, M.; Cuzick, J.; Brentnall, A.; et al. Improvement in risk prediction, early detection and prevention of breast cancer in the NHS Breast Screening Programme and family history clinics: A dual cohort study. In Improvement in Risk Prediction, Early Detection and Prevention of Breast Cancer in the NHS Breast Screening Programme and Family History Clinics: A Dual Cohort Study; NIHR Journals Library: Perth, UK, 2016. [Google Scholar] [CrossRef]
- Hou, I.C.; Lan, M.F.; Shen, S.H.; Tsai, P.Y.; Chang, K.J.; Tai, H.-C.; Tsai, A.-J.; Chang, P.; Wang, T.-F.; Sheu, S.-J.; et al. The Development of a Mobile Health App for Breast Cancer Self-Management Support in Taiwan: Design Thinking Approach. JMIR Mhealth Uhealth 2020, 8, e15780. [Google Scholar] [CrossRef]
- Minkler, M.; Blackwell, A.G.; Thompson, M.; Tamir, H. Community-based participatory research: Implications for public health funding. Am. J. Public Health 2003, 93, 1210–1213. [Google Scholar] [CrossRef] [PubMed]
- Diefenbach, M.; Turner, G.; Carpenter, K.M.; Sheldon, L.K.; Mustian, K.M.; Gerend, M.A.; Rini, C.; von Wagner, C.; Gritz, E.R.; McQueen, A.; et al. Cancer and patient-physician communication. J. Health Commun. 2009, 14 (Suppl. 1), 57–65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hubbard, G.; Kidd, L.; Donaghy, E. Preferences for involvement in treatment decision making of patients with cancer: A review of the literature. Eur. J. Oncol. Nurs. 2008, 12, 299–318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wallerstein, N.; Duran, B. The conceptual, historical, and practice roots of community based participatory research and related participatory traditions. In Community Based Participatory Research for Health; Minkler, M., Wallerstein, N., Eds.; John Wiley & Sons, Inc.: San Francisco, CA, USA, 2003; pp. 27–52. [Google Scholar]
- Oehrlein, E.M.; Graff, J.S.; Harris, J.; Perfetto, E.M. Patient-Community Perspectives on Real-World Evidence: Enhancing Engagement, Understanding, and Trust. Patient 2019, 12, 375–381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramanadhan, S.; Davis, M.M.; Armstrong, R.; Baquero, B.; Ko, L.K.; Leng, J.C.; Salloum, R.G.; Vaughn, N.A.; Brownson, R.C. Participatory implementation science to increase the impact of evidence-based cancer prevention and control. Cancer Causes Control. 2018, 29, 363–369. [Google Scholar] [CrossRef]
- Sørensen, K.; van den Broucke, S.; Fullam, J.; Doyle, G.; Pelikan, J.; Slonska, Z.; Brand, H. Health literacy and public health: A systematic review and integration of definitions and models. BMC Public Health 2012, 12, 80. [Google Scholar] [CrossRef] [Green Version]
- Franchini, M.; Pieroni, S.; Montrucchio, E.; Nori Cucchiari, J.; Di Maggio, C.; Cassano, E.; Di Nubila, B.; Giuseppetti, G.M.; Nicolucci, A.; Scaperrotta, G.; et al. The P.I.N.K. Study Approach for Supporting Personalized Risk Assessment and Early Diagnosis of Breast Cancer. Int. J. Environ. Res. Public Health 2021, 18, 2456. [Google Scholar] [CrossRef]
- Blondel, V.D.; Guillaume, J.L.; Lambiotte, R.; Lefebvre, E. Fast unfolding of communities in large networks. J. Stat. Mech. 2008, 2008, P10008. [Google Scholar] [CrossRef] [Green Version]
- Sharpe, D. Chi-Square Test is Statistically Significant: Now What? Pract. Assess. Res. Eval. 2015, 20, 8. [Google Scholar] [CrossRef]
- European Commission Database. Available online: https://ec.europa.eu/eurostat/databrowser/explore/all/all_themes?lang=en (accessed on 8 November 2022).
- Berkman, N.D.; Sheridan, S.L.; Donahue, K.E.; Halpern, D.J.; Crotty, K. Low health literacy and health outcomes: An updated systematic review. Ann. Intern. Med. 2011, 155, 97–107. [Google Scholar] [CrossRef]
- Corvo, E.; De Caro, W. The paradox of the link between health literacy and health promotion: The case of COVID-19. Prof Inferm. 2020, 73, 219–222. (In English) [Google Scholar] [CrossRef] [PubMed]
- Michie, S.; van Stralen, M.M.; West, R. The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implement Sci. 2011, 6, 42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, Y.; Zhang, D.; Kang, S. Physical activity and risk of breast cancer: A meta-analysis of prospective studies. Breast Cancer Res. Treat. 2012, 137, 869–882. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Wang, Q.; Zhang, Y.; Xie, Q.; Tan, X. Physical Activity and Risk of Breast Cancer: A Meta-Analysis of 38 Cohort Studies in 45 Study Reports. Value Health 2019, 22, 104–128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pizot, C.; Boniol, M.; Mullie, P.; Koechlin, A.; Boniol, M.; Boyle, P.; Autier, P. Physical activity, hormone replacement therapy and breast cancer risk: A meta-analysis of prospective studies. Eur. J. Cancer 2016, 52, 138–154. [Google Scholar] [CrossRef] [Green Version]
- Han, M.A.; Zeraatkar, D.; Guyatt, G.H.; Vernooij, R.W.M.; El Dib, R.; Zhang, Y.; Algarni, A.; Leung, G.; Storman, D.; Valli, C.; et al. Reduction of Red and Processed Meat Intake and Cancer Mortality and Incidence: A Systematic Review and Meta-analysis of Cohort Studies. Ann. Intern. Med. 2019, 171, 711–720. [Google Scholar] [CrossRef] [Green Version]
- Kazemi, A.; Barati-Boldaji, R.; Soltani, S.; Mohammadipoor, N.; Esmaeilinezhad, Z.; Clark, C.C.T.; Babajafari, S.; Akbarzadeh, M. Intake of Various Food Groups and Risk of Breast Cancer: A Systematic Review and Dose-Response Meta-Analysis of Prospective Studies. Adv. Nutr. 2021, 12, 809–849. [Google Scholar] [CrossRef]
- Harpsøe, M.C.; Nielsen, N.M.; Friis-Møller, N.; Andersson, M.; Wohlfahrt, J.; Linneberg, A.; Nohr, E.A.; Jess, T. Body Mass Index and Risk of Infections Among Women in the Danish National Birth Cohort. Am. J. Epidemiol. 2016, 183, 1008–1017. [Google Scholar] [CrossRef] [Green Version]
- Wu, J.; Zeng, R.; Huang, J.; Li, X.; Zhang, J.; Ho, J.C.; Zheng, Y. Dietary Protein Sources and Incidence of Breast Cancer: A Dose-Response Meta-Analysis of Prospective Studies. Nutrients 2016, 8, 730. [Google Scholar] [CrossRef]
- Fiolet, T.; Srour, B.; Sellem, L.; Kesse-Guyot, E.; Allès, B.; Méjean, C.; Deschasaux, M.; Fassier, P.; Latino-Martel, P.; Beslay, M.; et al. Consumption of ultra-processed foods and cancer risk: Results from NutriNet-Santé prospective cohort. BMJ 2018, 360, k322. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.; Liu, X.; Huang, H.; Zhang, F.; Lu, Y.; Hu, H. High salt diet may promote progression of breast tumor through eliciting immune response. Int. Immunopharmacol. 2020, 87, 106816. [Google Scholar] [CrossRef] [PubMed]
- Franchini, M.; Pieroni, S.; Martini, N.; Ripoli, A.; Chiappino, D.; Denoth, F.; Liebman, M.N.; Molinaro, S.; Della Latta, D. Shifting the Paradigm: The Dress-COV Telegram Bot as a Tool for Participatory Medicine. Int. J. Environ. Res. Public Health 2020, 17, 8786. [Google Scholar] [CrossRef] [PubMed]
- Fottrell, E.; Jennings, H.; Kuddus, A.; Ahmed, N.; Morrison, J.; Akter, K.; Shaha, S.; Nahar, B.; Haghparast-Bidgoli, H.; Khan, A.; et al. The effect of community groups and mobile phone messages on the prevention and control of diabetes in rural Bangladesh: Study protocol for a three-arm cluster randomised controlled trial. Trials 2016, 17, 600. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Women Belonging to Other Families | Fuchsia Family | Yellow Family | Green Family | Chi-Square Test | All Women | |
|---|---|---|---|---|---|---|
| Number of women | 3247 | 1299 | 889 | 166 | 5601 | |
| BC prevalence [95% CI] | 1.6% [1.2–2.1%] | 2.5% [1.7–3.5%] (b) | 0.9% [0.5–1.8%] (a) | 4.2% [2.0–8.4%] (b) | p = 0.004 | 1.8% [1.5–2.2%] |
| Years of age (avg ± SD) focus on age classes | 58.7 (±7.4); > 65 * (b) | 64.5 (±6.9); 60–64 ** (a); >65 ** (b) | 56.2 (±5.2); 50–54 **; 55–59 **; 60–64 * (b) | 61.3 (±9.4); 45–49 **; 55–59 *; >65 ** | p < 0.001 | 59.7 (±7.6) |
| Breast density: | p < 0.001 | |||||
| BI-RADS A (less dense) | 14.6% * | 28.6% ** | 7.3% * | 21.7% | 16.9% | |
| BI-RADS B | 37.1% | 45.7% ** | 27.7% * | 45.8% ** | 37.9% | |
| BI-RADS C | 36.8% ** | 23.9% * | 46.5% ** | 25.9% * | 35.0% | |
| BI-RADS D | 11.5% ** | 1.7% * | 18.6% ** | 6.6% | 10.2% | |
| Family history of BC: | p < 0.001 | |||||
| no first line relatives | 72.5% * | 78.6% ** | 69.4% * | 76.5% | 73.5% | |
| first line female relatives | 25.5% | 21.4% * | 29.7% ** | 23.5% | 25.2% | |
| first line male relatives | 0.5% | 0.0% * | 0.9% ** (b) | 0.0% | 0.4% | |
| first line male and female rel. | 1.5% | 0.0% | 0.0% | 0.0% | 0.9% | |
| Menarche age (avg. years ± SD) | 12.6 (±1.4) | 12.4 (±1.4) | 12.7 (±1.4) | 12.8 (±1.5) | 12.6 (±1.4) | |
| Reproductive period length | 37.4 (±4.2) | 38.8 (±3.9) | 37.7 (±3.3) | 32.1 (±3.4) | 37.6 (±4.1) | |
| Menopause (avg. years ± SD). Focus on length classes | 8.6 (±7.3) ≤5 **; >5 * | 13.3 (±7.7) ≤5 *; >5 ** | 5.9 (±5.7); ≤5 ** (a); >5 * (b) | 16.5 (±10.2) ≤5 *; >5 ** | p < 0.001 | 9.5 (±7.7) |
| Women Belonging to Other Families | Fuchsia Family | Yellow Family | Green Family | Chi-Square Test | All Women | |
|---|---|---|---|---|---|---|
| Number of women | 3247 | 1299 | 889 | 166 | 5601 | |
| BC prevalence [95% CI] | 1.6% [1.2–2.1%] | 2.5% [1.7–3.5%] (b) | 0.9% [0.5–1.8%] (a) | 4.2% [2.0–8.4%] (b) | p = 0.004 | 1.8% [1.5–2.2%] |
| Qualification: | p < 0.0010 | |||||
| primary secondary education | 24.1% * | 34.4% ** | 19.1% * | 36.1% ** | 26.1% | |
| high school graduation | 40.9% ** | 35.0% * | 39.6% | 34.9% | 39.2% | |
| university/post graduate | 35.0% | 30.6% * | 41.3% ** | 28.9% | 34.8% | |
| Occupation: | p < 0.001 | |||||
| unemployed/housewife | 33.3% * | 59.3% ** | 19.7% * | 53.6% ** | 37.8% | |
| employed | 63.8% ** | 36.1% * | 73.1% ** | 42.8% * (a) | 58.2% | |
| retired | 0.6% * | 4.5% ** | 0.0% * | 3.6% ** | 1.5% | |
| work/worked night shifts | 2.3% | 0.0% * | 7.2% ** | 0.0% * | 2.5% | |
| Current or past Co-morbidities: | p < 0.001 | |||||
| 1 co-morbidity | 27.8% | 24.9% * | 35.5% ** | 26.5% | 28.3% | |
| at least 2 co-morbidities groups | 56.3% * | 68.0% ** | 51.9% * | 66.9% ** | 58.6% | |
| Types of comorbidities: | ||||||
| cardiometabolic diseases | 55.6% * | 70.4% ** | 51.5% * | 63.3% | p < 0.001 | 58.6% |
| endocrine diseases | 49.5% | 52.1% | 53.1% | 56.0% | p > 0.05 | 50.9% |
| intestinal diseases | 11.3% | 13.0% ** | 8.8% * | 11.4% | p = 0.024 | 11.3% |
| neuropsychiatric diseases | 39.3% * | 44.5% ** | 40.7% | 53.6% ** (a) | p < 0.001 | 41.2% |
| autoimmune diseases | 23.3% * | 30.1% ** | 21.8% * | 21.7% | p < 0.001 | 24.6% |
| Chest radiation therapy | 6.5%* (b) | 13.7% ** | 4.5% * | 18.1% ** | p < 0.001 | 8.2% |
| Pregnancy (at least one) | 80.0% | 88.8% ** (b) | 68.4% * | 86.1% (a) | p < 0.001 | 80.4% |
| Breast feeding | 63.1% | 73.2% ** | 53.5% * (a) | 69.3% | 64.1% | |
| BMI: | p < 0.001 | |||||
| underweight (<18.5) | 6.1% ** | 0.4% * | 0.3% * | 0.0% * | 3.7% | |
| normal weight (18.5–24.9) | 68.2% | 56.5% * | 80.9% ** | 59.0% * | 67.2% | |
| overweight (25–29.9) | 20.5% * | 29.6% ** | 15.0% * | 28.9% ** | 22.0% | |
| obese (≥30) | 5.2% * | 13.5% ** | 3.8% * | 12.0% ** | 7.1% | |
| Weight gain in menopause | 55.0% * | 67.9% ** | 54.2% * | 70.5% ** | p < 0.001 | 58.3% |
| Oral contraceptive use: | p < 0.001 | |||||
| never or less than 1 year | 46.9% * (b) | 59.3% ** | 42.4% * | 59.0% ** | 49.4% | |
| 1–5 years | 25.1% ** | 22.3% | 21.4% | 18.7% | 23.7% | |
| more than 5 years | 28.0% ** | 18.4% * | 36.2% ** | 22.3% | 26.9% | |
| Ovarian stimulation: | p < 0.001 | |||||
| at least 1 cycle of stimulation | 6.8% | 2.9% * | 14.1% ** | 3.0% | 6.9% | |
| HRT: | p < 0.001 | |||||
| more than 6 months | 17.9% * | 23.9% ** | 14.6% * | 38.6% ** | 19.4% |
| Women Belonging to Other Families | Fuchsia Family | Yellow Family | Green Family | Chi-Square Test | All Women | |
|---|---|---|---|---|---|---|
| Number of women | 3247 | 1299 | 889 | 166 | 5601 | |
| BC prevalence [95% CI] | 1.6% [1.2–2.1%] | 2.5% [1.7–3.5%] (b) | 0.9% [0.5–1.8%] (a) | 4.2% [2.0–8.4%] (b) | p = 0.004 | 1.8% [1.5–2.2%] |
| Smoking habits: | p = 0.010 | |||||
| never-smokers | 42.7% | 42.7% | 46.5% | 47.6% | 43.4% | |
| 1–5 cigarettes/day | 32.2% ** | 28.3% * | 29.2% | 24.7% | 30.6% | |
| 6–10 cigarettes/day | 12.4% | 14.7% ** | 10.9% | 10.2% | 12.6% | |
| more than 10 cigarettes/day | 12.8% | 14.3% | 13.4% | 17.5% | 13.4% | |
| Alcohol drinking habits: | p = 0.005 | |||||
| no alcohol drinker | 20.5% | 24.1% ** | 19.7% | 25.9% | 21.4% | |
| one time per week or less | 53.0% | 47.7% * | 56.6% ** | 45.8% | 52.1% | |
| more times per week | 26.2% | 27.9% | 23.5% | 28.3% | 26.2% | |
| binge-drinking at least one time/week | 0.2% | 0.4% | 0.2% | 0,0% | 0.3% | |
| WCRFs compliance | ||||||
| 1. Stay daily physically active: | p < 0.001 | |||||
| low | 33.2% | 35.6% | 30.8% | 41.6% ** | 33.6% | |
| medium | 37.4% (b) | 40.5% ** | 37.2% | 28.3% * | 37.8% | |
| high/very high | 29.4% (a) | 23.9% * | 31.9% ** | 30.1% | 28.5% | |
| 2. Limit energy-dense foods: | p > 0.05 | |||||
| low | 20.0% * | 23.6% ** | 19.8% | 33.7% ** | 21.2% | |
| medium | 28.6% | 29.0% | 27.0% | 21.1% * | 28.2% | |
| high/very high | 51.4% | 47.4% * | 53.2% | 45.2% | 50.6% | |
| 3. Follow a plant-based diet: | p > 0.05 | |||||
| low | 13.1% | 13.2% | 11.8% | 19.3% | 13.1% | |
| medium | 40.8% | 42.2% | 41.2% | 38.0% | 41.1% | |
| high/very high | 46.1% | 44.6% | 47.0% | 42.8% | 45.8% | |
| 4. Limit red/cured meats: | p > 0.05 | |||||
| low | 13.5% | 14.9% | 15.5% | 14.5% | 14.1% | |
| medium | 37.0% | 39.9% | 35.5% | 41.6% | 37.6% | |
| high/very high | 49.5% | 45.3% | 48.9% | 44.0% | 48.3% | |
| 5. Limit salt consumption: | p = 0.003 | |||||
| low | 11.8% * | 14.7% ** | 13.7% | 17.5% | 12.9% | |
| medium | 34.5% | 36.3% | 30.9% * | 32.5% | 34.3% | |
| high/very high | 53.7% (a) | 49.0%* | 55.3% | 50.0% | 52.8% | |
| 6. Follow a varied diet: | p = 0.012 | |||||
| low | 7.7% | 6.5% | 6.1% | 10.8% | 7.2% | |
| medium | 39.1% | 43.5% ** | 38.0% | 41.0% | 40.0% | |
| high/very high | 53.2% | 50.0% * | 55.9% | 48.2% | 52.8% |
| OR (95% CI) | p | ||
|---|---|---|---|
| Age | 1.08 (1.06–1.11) | 0.00 | |
| Brest density: | BI-Rads A | reference | |
| BI-Rads B | 1.78 (0.97–3.29) | 0.06 | |
| BI-Rads C | 1.43 (0.74–2.75) | 0.29 | |
| BI-Rads D | 2.52 (1.10–5.77) | 0.03 | |
| Oral contraceptive: | Never used | reference | |
| 1–5 years | 0.64 (0.37–1.11) | 0.11 | |
| more than 5 years | 0.56 (0.31–1.00) | 0.05 | |
| First line relatives with BC: | none | reference | |
| female | 1.16 (0.75–1.81) | 0.50 | |
| male | 5.55 (1.24–24.93) | 0.03 | |
| male and female | 0.00 (0.00–0.00) | 1.00 | |
| WCRF physical activity: | medium compliance | reference | |
| low compliance | 0.85 (0.55–1.32) | 0.48 | |
| high compliance | 0.41 (0.22–0.76) | 0.00 | |
| WCRF salt: | medium compliance | reference | |
| low compliance | 0.93 (0.52–1.66) | 0.81 | |
| high compliance | 0.62 (0.40–0.97) | 0.04 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Franchini, M.; Pieroni, S.; Denoth, F.; Scalese Urciuoli, M.; Colasante, E.; Salvatori, M.; Anastasi, G.; Frontignano, C.K.; Dogliotti, E.; Vidali, S.; et al. Promote Community Engagement in Participatory Research for Improving Breast Cancer Prevention: The P.I.N.K. Study Framework. Cancers 2022, 14, 5801. https://doi.org/10.3390/cancers14235801
Franchini M, Pieroni S, Denoth F, Scalese Urciuoli M, Colasante E, Salvatori M, Anastasi G, Frontignano CK, Dogliotti E, Vidali S, et al. Promote Community Engagement in Participatory Research for Improving Breast Cancer Prevention: The P.I.N.K. Study Framework. Cancers. 2022; 14(23):5801. https://doi.org/10.3390/cancers14235801
Chicago/Turabian StyleFranchini, Michela, Stefania Pieroni, Francesca Denoth, Marco Scalese Urciuoli, Emanuela Colasante, Massimiliano Salvatori, Giada Anastasi, Cinzia Katia Frontignano, Elena Dogliotti, Sofia Vidali, and et al. 2022. "Promote Community Engagement in Participatory Research for Improving Breast Cancer Prevention: The P.I.N.K. Study Framework" Cancers 14, no. 23: 5801. https://doi.org/10.3390/cancers14235801