
Differences in Cancer-Specific Mortality after Trimodal Therapy for T2N0M0 Bladder Cancer according to Histological Subtype
 , , , ,
, , , ,  ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Statistical Analyses
3. Results
3.1. Descriptive Characteristics of the Study Population
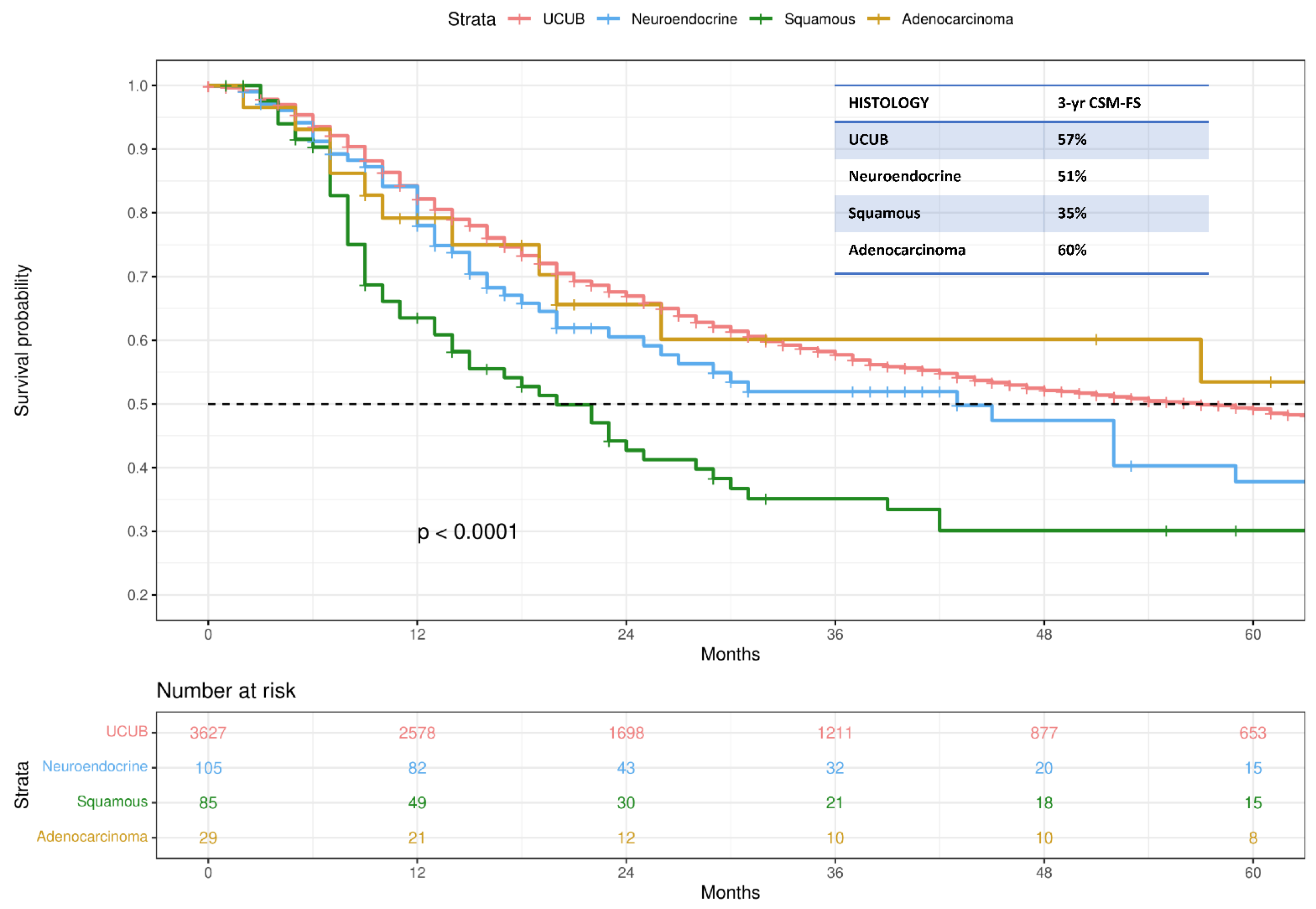
3.2. Kaplan–Meier Analyses Assessing CSM-Free Survival
3.3. Multivariable Cox Regression Models Predicting CSM
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Witjes, C.A.; Bruins, H.M.; Cathomas, R. Guideline: Muscle-invasive and Metastatic Bladder Cancer. Eur. Assoc. Urol. 2016, 34, 1945–1952. [Google Scholar]
- Shipley, W.U.; Prout, G.R.; Einstein, A.B.; Coombs, L.J.; Wajsman, Z.; Soloway, M.S.; Englander, L.; Barton, B.A.; Hafermann, M.D. Treatment of Invasive Bladder Cancer by Cisplatin and Radiation in Patients Unsuited for Surgery. JAMA J. Am. Med. Assoc. 1987, 258, 931–935. [Google Scholar] [CrossRef]
- Kulkarni, G.S.; Hermanns, T.; Wei, Y.; Bhindi, B.; Satkunasivam, R.; Athanasopoulos, P.; Bostrom, P.J.; Kuk, C.; Li, K.; Templeton, A.J.; et al. Propensity score analysis of radical cystectomy versus bladder-sparing trimodal therapy in the setting of a multidisciplinary bladder cancer clinic. J. Clin. Oncol. 2017, 35, 2299–2305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mak, R.H.; Hunt, D.; Shipley, W.U.; Efstathiou, J.A.; Tester, W.J.; Hagan, M.P.; Kaufman, D.S.; Heney, N.M.; Zietman, A.L. Long-term outcomes in patients with muscle-invasive bladder cancer after selective bladder-preserving combined-modality therapy: A pooled analysis of radiation therapy oncology group protocols 8802, 8903, 9506, 9706, 9906, and 0233. J. Clin. Oncol. 2014, 32, 3801–3809. [Google Scholar] [CrossRef] [PubMed]
- James, N.D.; Hussain, S.A.; Hall, E.; Jenkins, P.; Tremlett, J.; Rawlings, C.; Crundwell, M.; Sizer, B.; Sreenivasan, T.; Hendron, C.; et al. Radiotherapy with or without Chemotherapy in Muscle-Invasive Bladder Cancer. N. Engl. J. Med. 2012, 366, 1477–1488. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giacalone, N.J.; Shipley, W.U.; Clayman, R.H.; Niemierko, A.; Drumm, M.; Heney, N.M.; Michaelson, M.D.; Lee, R.J.; Saylor, P.J.; Wszolek, M.F.; et al. Long-term Outcomes After Bladder-preserving Tri-modality Therapy for Patients with Muscle-invasive Bladder Cancer: An Updated Analysis of the Massachusetts General Hospital Experience. Eur. Urol. 2017, 71, 952–960. [Google Scholar] [CrossRef] [PubMed]
- Alanee, S.; Alvarado-Cabrero, I.; Murugan, P.; Kumar, R.; Nepple, K.G.; Paner, G.P.; Patel, M.I.; Raspollini, M.R.; Lopez-Beltran, A.; Konety, B.R. Update of the International Consultation on Urological Diseases on bladder cancer 2018: Non-urothelial cancers of the urinary bladder. World J. Urol. 2019, 37, 107–114. [Google Scholar] [CrossRef] [PubMed]
- Veskimäe, E.; Espinos, E.L.; Bruins, H.M.; Yuan, Y.; Sylvester, R.; Kamat, A.M.; Shariat, S.F.; Witjes, J.A.; Compérat, E.M. What Is the Prognostic and Clinical Importance of Urothelial and Nonurothelial Histological Variants of Bladder Cancer in Predicting Oncological Outcomes in Patients with Muscle-invasive and Metastatic Bladder Cancer? A European Association of Urology Mus. Eur. Urol. Oncol. 2019, 2, 625–642. [Google Scholar] [CrossRef] [PubMed]
- Howlader, N.; Noone, A.; Krapcho, M. Cancer Stat Rev n.d.:SEER Statistics. Available online: https://seer.cancer.gov/csr/1975_2018/ (accessed on 25 August 2022).
- Janopaul-Naylor, J.R.; Zhong, J.; Liu, Y.; Zhang, C.; Osunkoya, A.O.; Joshi, S.S.; Bilen, M.A.; Carthon, B.; Kucuk, O.; Hartsell, L.M.; et al. Clinical and Translational Radiation Oncology Bladder preserving chemoradiotherapy compared to surgery for variants of urothelial carcinoma and other tumors types involving the bladder: An analysis of the National Cancer Database. Clin. Transl. Radiat. Oncol. 2021, 26, 30–34. [Google Scholar] [CrossRef] [PubMed]
- Fischer-Valuck, B.W.; Michalski, J.M.; Contreras, J.A.; Brenneman, R.; Christodouleas, J.P.; Abraham, C.D.; Kim, E.H.; Arora, V.K.; Bullock, A.D.; Carmona, R.; et al. Clinical and Translational Radiation Oncology Short Communication A propensity analysis comparing definitive chemo-radiotherapy for muscle-invasive squamous cell carcinoma of the bladder vs. urothelial carcinoma of the bladder using the National Cancer D. Clin. Transl. Radiat. Oncol. 2019, 15, 38–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krasnow, R.E.; Drumm, M.; Roberts, H.J.; Niemierko, A.; Wu, C.L.; Wu, S.; Zhang, J.; Heney, N.M.; Wszolek, M.F.; Blute, M.L.; et al. Clinical Outcomes of Patients with Histologic Variants of Urothelial Cancer Treated with Trimodality Bladder-sparing Therapy. Eur. Urol. 2017, 72, 54–60. [Google Scholar] [CrossRef] [PubMed]
- Bandini, M.; Pederzoli, F.; Madison, R.; Briganti, A.; Ross, J.S.; Niegisch, G.; Yu, E.Y.; Bamias, A.; Agarwal, N.; Sridhar, S.S.; et al. Unfavorable Cancer-specific Survival After Neoadjuvant Chemotherapy and Radical Cystectomy in Patients With Bladder Cancer and Squamous Cell Variant: A Multi-institutional Study. Clin. Genitourin. Cancer 2020, 18, e543–e556. [Google Scholar] [CrossRef] [PubMed]
- Vetterlein, M.W.; Wankowicz, S.A.M.; Seisen, T.; Lander, R.; Löppenberg, B.; Chun, F.K.; Menon, M.; Sun, M.; Barletta, J.A.; Choueiri, T.K.; et al. Neoadjuvant chemotherapy prior to radical cystectomy for muscle-invasive bladder cancer with variant histology. Cancer 2017, 123, 4346–4355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Necchi, A.; Raggi, D.; Gallina, A.; Madison, R.; Colecchia, M.; Lucianò, R.; Montironi, R.; Giannatempo, P.; Farè, E.; Pederzoli, F.; et al. Updated Results of PURE-01 with Preliminary Activity of Neoadjuvant Pembrolizumab in Patients with Muscle-invasive Bladder Carcinoma with Variant Histologies. Eur. Urol. 2019, 77, 447–448. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | Overall (n = 3846) |
|---|---|
| Age at diagnosis (years) | |
| Median | 77 |
| IQR | 70–83 |
| Histology | |
| Urothelial Carcinoma | 3627 (94.3) |
| Neuroendocrine Carcinoma | 105 (2.7) |
| Squamous Cell Carcinoma | 85 (2.2) |
| Adenocarcinoma | 29 (0.8) |
| Grade | |
| Low grade | 113 (3) |
| High grade | 3733 (97) |
| Sex | |
| Male | 2842 (74) |
| Female | 1004 (26) |
| Tumor Site | |
| Trigone | 293 (7.7) |
| Dome | 201 (5.2) |
| Lateral wall | 871 (22.6) |
| Anterior wall | 139 (3.6) |
| Posterior wall | 328 (8.5) |
| Bladder neck | 139 (3.6) |
| Ureteral orifice | 76 (2) |
| Lateral-posterior wall | 585 (15.2) |
| NOS | 1214 (31.6) |
| Follow-up (months) | |
| Median | 21 |
| IQR | 10–46 |
| Predictors | HR (95%CI) | p-Value |
|---|---|---|
| Histology | ||
| Urothelial Carcinoma | Ref. | - |
| Neuroendocrine Carcinoma | 1.28 (0.96–1.7) | 0.09 |
| Squamous Cell Carcinoma | 1.98 (1.5–2.61) | <0.001 |
| Adenocarcinoma | 1.02 (0.58–1.8) | 0.9 |
| Age at diagnosis (years) | 1.02 (1.02–1.03) | <0.001 |
| Sex | ||
| Female | Ref. | - |
| Male | 0.88 (0.78–0.97) | 0.02 |
| Grade | ||
| Low grade | Ref. | - |
| High grade | 1.08 (0.82–1.42) | 0.5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barletta, F.; Tappero, S.; Panunzio, A.; Incesu, R.-B.; Cano Garcia, C.; Piccinelli, M.L.; Tian, Z.; Gandaglia, G.; Moschini, M.; Terrone, C.; et al. Differences in Cancer-Specific Mortality after Trimodal Therapy for T2N0M0 Bladder Cancer according to Histological Subtype. Cancers 2022, 14, 5766. https://doi.org/10.3390/cancers14235766
Barletta F, Tappero S, Panunzio A, Incesu R-B, Cano Garcia C, Piccinelli ML, Tian Z, Gandaglia G, Moschini M, Terrone C, et al. Differences in Cancer-Specific Mortality after Trimodal Therapy for T2N0M0 Bladder Cancer according to Histological Subtype. Cancers. 2022; 14(23):5766. https://doi.org/10.3390/cancers14235766
Chicago/Turabian StyleBarletta, Francesco, Stefano Tappero, Andrea Panunzio, Reha-Baris Incesu, Cristina Cano Garcia, Mattia Luca Piccinelli, Zhe Tian, Giorgio Gandaglia, Marco Moschini, Carlo Terrone, and et al. 2022. "Differences in Cancer-Specific Mortality after Trimodal Therapy for T2N0M0 Bladder Cancer according to Histological Subtype" Cancers 14, no. 23: 5766. https://doi.org/10.3390/cancers14235766