
Preoperative Serum Markers and Risk Classification in Intrahepatic Cholangiocarcinoma: A Multicenter Retrospective Study

 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Clinicopathologic Variables
2.3. Statistical Analysis
3. Results
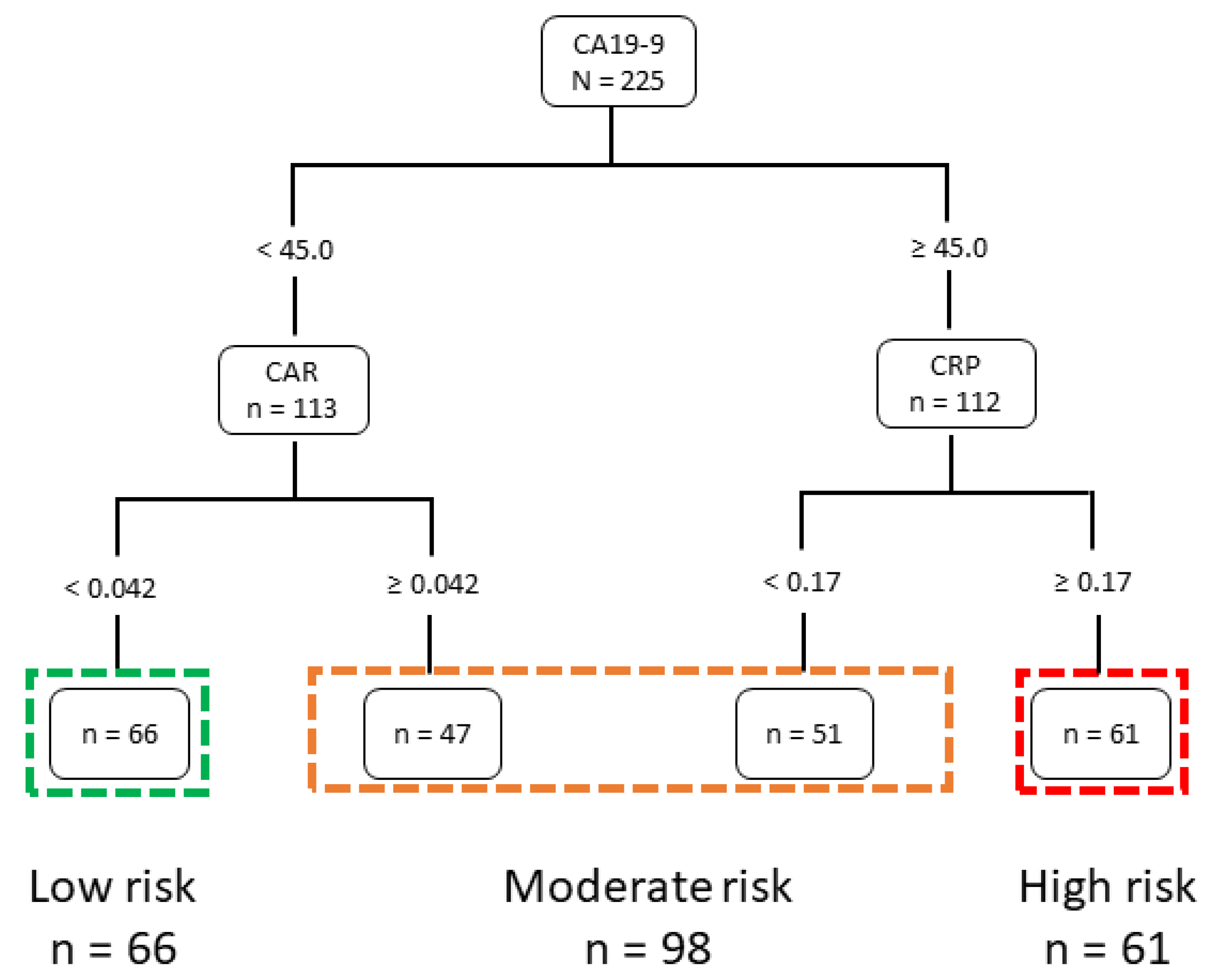
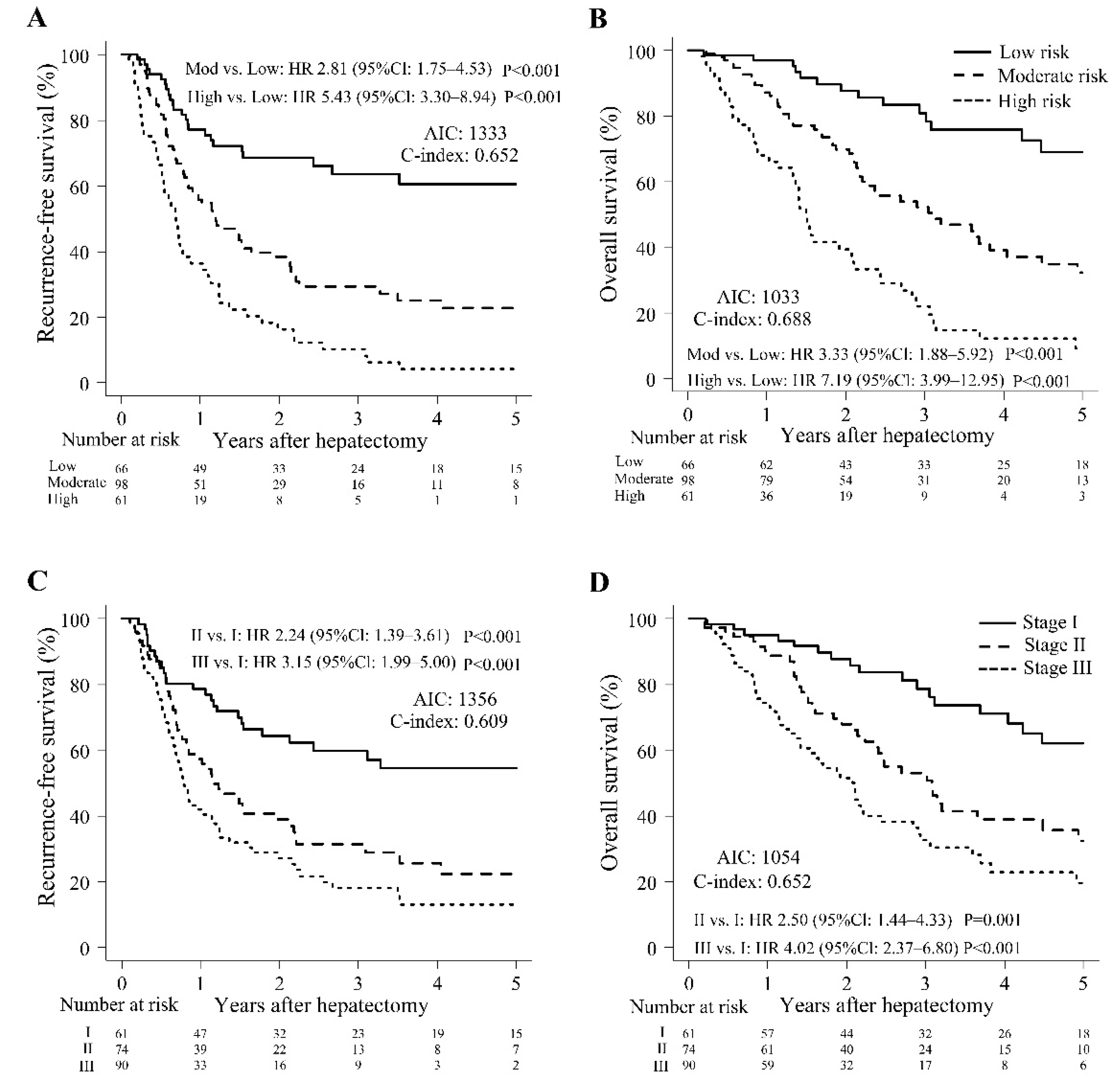
3.1. Preoperative Staging System using the CART Algorithm and Patients’ Perioperative Characteristics
3.2. Univariate and Multivariate Analysis of Prognostic Factors for Long-Term Survival
3.3. Effects of Postoperative Adjuvant Chemotherapy in the Three Risk Groups
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Buettner, S.; van Vugt, J.L.A.; IJzermans, J.N.; Koerkamp, B.G. Intrahepatic cholangiocarcinoma: Current perspectives. OncoTargets Ther. 2017, 10, 1131–1142. [Google Scholar] [CrossRef] [Green Version]
- Shaib, Y.H.; Davila, J.A.; McGlynn, K.; El-Serag, H.B. Rising incidence of intrahepatic cholangiocarcinoma in the United States: A true increase? J. Hepatol. 2004, 40, 472–477. [Google Scholar] [CrossRef]
- Zhang, X.F.; Xue, F.; Dong, D.H.; Weiss, M.; Popescu, I.; Marques, H.P.; Aldrighetti, L.; Maithel, S.K.; Pulitano, C.; Bauer, T.W.; et al. Number and station of lymph node metastasis after curative-intent resection of intrahepatic cholangiocarcinoma impact prognosis. Ann. Surg. 2021, 274, e1187–e1195. [Google Scholar] [CrossRef]
- Endo, I.; Gonen, M.; Yopp, A.C.; Dalal, K.M.; Zhou, Q.; Klimstra, D.; D’Angelica, M.; DeMatteo, R.P.; Fong, Y.; Schwartz, L.; et al. Intrahepatic cholangiocarcinoma: Rising frequency, improved survival, and determinants of outcome after resection. Ann. Surg. 2008, 248, 84–96. [Google Scholar] [CrossRef]
- Kosaka, H.; Kaibori, M.; Matsui, K.; Ishizaki, M.; Matsushima, H.; Sekimoto, M. Investigation of a tumor location-specific therapeutic strategy for intrahepatic cholangiocarcinoma. Asian Pac. J. Cancer Prev. 2021, 22, 1485–1493. [Google Scholar] [CrossRef]
- Siebenhüner, A.R.; Seifert, H.; Bachmann, H.; Seifert, B.; Winder, T.; Feilchenfeldt, J.; Breitenstein, S.; Clavien, P.A.; Stupp, R.; Knuth, A.; et al. Adjuvant treatment of resectable biliary tract cancer with cisplatin plus gemcitabine: A prospective single center phase II study. BMC Cancer 2018, 18, 72. [Google Scholar] [CrossRef] [Green Version]
- Primrose, J.N.; Fox, R.P.; Palmer, D.H.; Malik, H.Z.; Prasad, R.; Mirza, D.; Anthony, A.; Corrie, P.; Falk, S.; Finch-Jones, M.; et al. Capecitabine compared with observation in resected biliary tract cancer (BILCAP): A randomised, controlled, multicentre, phase 3 study. Lancet Oncol. 2019, 20, 663–673. [Google Scholar] [CrossRef] [Green Version]
- Edeline, J.; Benabdelghani, M.; Bertaut, A.; Watelet, J.; Hammel, P.; Joly, J.P.; Boudjema, K.; Fartoux, L.; Bouhier-Leporrier, K.; Jouve, J.L.; et al. Gemcitabine and oxaliplatin chemotherapy or surveillance in resected biliary tract cancer (Prodige 12-accord 18-Unicancer GI): A randomized phase III study. J. Clin. Oncol. 2019, 37, 658–667. [Google Scholar] [CrossRef]
- Yoh, T.; Cauchy, F.; Le Roy, B.; Seo, S.; Taura, K.; Hobeika, C.; Dokmak, S.; Farges, O.; Gelli, M.; Sa Cunha, A.; et al. Prognostic value of lymphadenectomy for long-term outcomes in node-negative intrahepatic cholangiocarcinoma: A multicenter study. Surgery 2019, 166, 975–982. [Google Scholar] [CrossRef]
- Yadav, S.; Xie, H.; Bin-Riaz, I.; Sharma, P.; Durani, U.; Goyal, G.; Borah, B.; Borad, M.J.; Smoot, R.L.; Roberts, L.R.; et al. Neoadjuvant vs. adjuvant chemotherapy for cholangiocarcinoma: A propensity score matched analysis. Eur. J. Surg. Oncol. 2019, 45, 1432–1438. [Google Scholar] [CrossRef]
- Buettner, S.; Galjart, B.; van Vugt, J.L.A.; Bagante, F.; Alexandrescu, S.; Marques, H.P.; Lamelas, J.; Aldrighetti, L.; Gamblin, T.C.; Maithel, S.K.; et al. Performance of prognostic scores and staging systems in predicting long-term survival outcomes after surgery for intrahepatic cholangiocarcinoma. J. Surg. Oncol. 2017, 116, 1085–1095. [Google Scholar] [CrossRef]
- Hyder, O.; Marques, H.; Pulitano, C.; Marsh, J.W.; Alexandrescu, S.; Bauer, T.W.; Gamblin, T.C.; Sotiropoulos, G.C.; Paul, A.; Barroso, E.; et al. A nomogram to predict long-term survival after resection for intrahepatic cholangiocarcinoma: An Eastern and Western experience. JAMA Surg. 2014, 149, 432–438. [Google Scholar] [CrossRef]
- Wang, Y.; Li, J.; Xia, Y.; Gong, R.; Wang, K.; Yan, Z.; Liu, G.; Wu, D.; Shi, L.; Lau, W.; et al. Prognostic nomogram for intrahepatic cholangiocarcinoma after partial hepatectomy. J. Clin. Oncol. 2013, 20, 1188–1195. [Google Scholar] [CrossRef]
- Qi, X.; Li, J.; Deng, H.; Li, H.; Su, C.; Guo, X. Neutrophil-to-lymphocyte ratio for the prognostic assessment of hepatocellular carcinoma: A systematic review and meta-analysis of observational studies. Oncotarget 2016, 7, 45283–45301. [Google Scholar] [CrossRef] [Green Version]
- Feng, J.F.; Huang, Y.; Liu, J.S. Combination of neutrophil lymphocyte ratio and platelet lymphocyte ratio is a useful predictor of postoperative survival in patients with esophageal squamous cell carcinoma. OncoTargets Ther. 2013, 6, 1605–1612. [Google Scholar]
- Salati, M.; Filippi, R.; Vivaldi, C.; Caputo, F.; Leone, F.; Salani, F.; Cerma, K.; Aglietta, M.; Fornaro, L.; Sperti, E.; et al. The prognostic nutritional index predicts survival and response to first-line chemotherapy in advanced biliary cancer. Liver Int. 2020, 40, 704–711. [Google Scholar] [CrossRef]
- Zhao, Y.; Si, G.; Zhu, F.; Hui, J.; Cai, S.; Huang, C.; Cheng, S.; Fathy, A.H.; Xiang, Y.; Li, J. Prognostic role of platelet to lymphocyte ratio in hepatocellular carcinoma: A systematic review and meta-analysis. Oncotarget 2017, 8, 22854–22862. [Google Scholar] [CrossRef] [Green Version]
- Ito, T.; Shinkawa, H.; Takemura, S.; Tanaka, S.; Nishioka, T.; Miyazaki, T.; Ishihara, A.; Kubo, S. Impact of the preoperative C-reactive protein to albumin ratio on the long-term outcomes of hepatic resection for intrahepatic cholangiocarcinoma. Asian Pac. J. Cancer Prev. 2020, 21, 2373–2379. [Google Scholar] [CrossRef]
- Iida, H.; Tani, M.; Komeda, K.; Nomi, T.; Matsushima, H.; Tanaka, S.; Ueno, M.; Nakai, T.; Maehira, M.; Mori, H.; et al. Superiority of CRP-albumin-lymphocyte index (CALLY index) as a non-invasive prognostic biomarker after hepatectomy for hepatocellular carcinoma. HPB 2022, 4, 101–115. [Google Scholar] [CrossRef]
- Liu, D.; Heij, L.R.; Czigany, Z.; Dahl, E.; Dulk, M.D.; Lang, S.A.; Ulmer, T.F.; Neumann, U.P.; Bednarsch, J. The prognostic value of neutrophil-to-lymphocyte ratio in cholangiocarcinoma: A systematic review and meta-analysis. Sci. Rep. 2022, 12, 12691. [Google Scholar] [CrossRef]
- Akgül, Ö.; Bagante, F.; Olsen, G.; Cloyd, J.M.; Weiss, M.; Merath, K.; Alexandrescu, S.; Marques, H.P.; Aldrighetti, L.; Maithel, S.K.; et al. Preoperative prognostic nutritional index predicts survival of patients with intrahepatic cholangiocarcinoma after curative resection. J. Surg. Oncol. 2018, 118, 422–430. [Google Scholar]
- Cui, H.; Li, Y.; Li, S.; Liu, G. Prognostic utility of preoperative inflammatory markers in patients with intrahepatic cholangiocarcinoma after hepatic resection: A systematic review and meta-analysis. Cancer Med. 2022; Online ahead of print. [Google Scholar] [CrossRef]
- Kano, H.; Midorikawa, Y.; Song, P.; Nakayama, H.; Moriguchi, M.; Higaki, T.; Tsuji, S.; Takayama, T. High C-reactive protein/albumin ratio associated with reduced survival due to advanced stage of intrahepatic cholangiocarcinoma. Biosci. Trends 2020, 14, 304–309. [Google Scholar] [CrossRef]
- Kosaka, H.; Ueno, M.; Komeda, K.; Hokuto, D.; Iida, H.; Hirokawa, F.; Matsui, K.; Sekimoto, M.; Kaibori, M. The impact of a preoperative staging system on accurate prediction of prognosis in intrahepatic cholangiocarcinoma. Cancers 2022, 14, 1107. [Google Scholar] [CrossRef]
- Bagante, F.; Spolverato, G.; Merath, K.; Weiss, M.; Alexandrescu, S.; Marques, H.P.; Aldrighetti, L.; Maithel, S.K.; Pulitano, C.; Bauer, T.W.; et al. Intrahepatic cholangiocarcinoma tumor burden: A classification and regression tree model to define prognostic groups after resection. Surgery 2019, 166, 983–990. [Google Scholar] [CrossRef]
- Wiener, M.; Acland, K.M.; Shaw, H.M.; Soong, S.J.; Lin, H.Y.; Chen, D.T.; Scolyer, R.A.; Winstanley, J.B.; Thompson, J.F. Sentinel node positive melanoma patients: Prediction and prognostic significance of nonsentinel node metastases and development of a survival tree model. Ann. Surg. Oncol. 2010, 17, 1995–2005. [Google Scholar] [CrossRef]
- Tsilimigras, D.I.; Mehta, R.; Moris, D.; Sahara, K.; Bagante, F.; Paredes, A.Z.; Moro, A.; Guglielmi, A.; Aldrighetti, L.; Weiss, M.; et al. A machine-based approach to preoperatively identify patients with the most and least benefit associated with resection for intrahepatic cholangiocarcinoma: An international multi-institutional analysis of 1146 patients. Ann. Surg. Oncol. 2020, 27, 1110–1119. [Google Scholar] [CrossRef]
- Amin, M.B.; Edge, S.B.; Greene, F.L.; Page, D.L.; Byrd, D.R.; Brookland, R.K.; Washington, M.K.; Gershenwald, J.E.; Compton, C.C.; Hess, K.R.; et al. AJCC Cancer Staging Manual, 8th ed.; Springer: New York, NY, USA, 2017. [Google Scholar]
- Cao, F.; Shen, L.; Qi, H.; Xie, L.; Song, Z.; Chen, S.; Fan, W. Tree-based classification system incorporating the HVTT-PVTT score for personalized management of hepatocellular carcinoma patients with macroscopic vascular invasion. Aging 2019, 11, 9544–9555. [Google Scholar] [CrossRef]
- Shimose, S.; Tanaka, M.; Iwamoto, H.; Niizeki, T.; Shirono, T.; Aino, H.; Noda, Y.; Kamachi, N.; Okamura, S.; Nakano, M.; et al. Prognostic impact of transcatheter arterial chemoembolization (TACE) combined with radiofrequency ablation in patients with unresectable hepatocellular carcinoma: Comparison with TACE alone using decision-tree analysis after propensity score matching. Hepatol. Res. 2019, 49, 919–928. [Google Scholar] [CrossRef]
- Feng, L.H.; Sun, H.C.; Zhu, X.D.; Liu, X.F.; Zhang, S.Z.; Li, X.L.; Li, Y.; Tang, Z.Y. Prognostic nomograms and risk classifications of outcomes in very early-stage hepatocellular carcinoma patients after hepatectomy. Eur. J. Surg. Oncol. 2021, 47, 681–689. [Google Scholar] [CrossRef]
- Grajski, K.A.; Breiman, L.; Viana Di Prisco, G.; Freeman, W.J. Classification of EEG spatial patterns with a tree-structured methodology: CART. IEEE Trans. Biomed. Eng. 1986, 33, 1076–1086. [Google Scholar] [CrossRef]
- Massarweh, N.N.; El-Serag, H.B. Epidemiology of hepatocellular carcinoma and intrahepatic cholangiocarcinoma. Cancer Control 2017, 24, 1073274817729245. [Google Scholar] [CrossRef]
- Le Roy, B.; Gelli, M.; Pittau, G.; Allard, M.A.; Pereira, B.; Serji, B.; Vibert, E.; Castaing, D.; Adam, R.; Cherqui, D.; et al. Neoadjuvant chemotherapy for initially unresectable intrahepatic cholangiocarcinoma. Br. J. Surg. 2018, 105, 839–847. [Google Scholar] [CrossRef]
- Konstantinidis, I.T.; Groot Koerkamp, B.; Do, R.K.; Gönen, M.; Fong, Y.; Allen, P.J.; D’Angelica, M.I.; Kingham, T.P.; DeMatteo, R.P.; Klimstra, D.S.; et al. Unresectable intrahepatic cholangiocarcinoma: Systemic plus hepatic arterial infusion chemotherapy is associated with longer survival in comparison with systemic chemotherapy alone. Cancer 2016, 122, 758–765. [Google Scholar] [CrossRef]
- Hu, L.S.; Zhang, X.F.; Weiss, M.; Popescu, I.; Marques, H.P.; Aldrighetti, L.; Maithel, S.K.; Pulitano, C.; Bauer, T.W.; Shen, F.; et al. Recurrence patterns and timing courses following curative-intent resection for intrahepatic cholangiocarcinoma. Ann. Surg. Oncol. 2019, 26, 2549–2557. [Google Scholar] [CrossRef]
- Valera, V.A.; Walter, B.A.; Yokoyama, N.; Koyama, Y.; Iiai, T.; Okamoto, H.; Hatakeyama, K. Prognostic groups in colorectal carcinoma patients based on tumor cell proliferation and classification and regression tree (CART) survival analysis. Ann. Surg. Oncol. 2007, 14, 34–40. [Google Scholar] [CrossRef]
- Hyer, J.M.; Ejaz, A.; Tsilimigras, D.I.; Paredes, A.Z.; Mehta, R.; Pawlik, T.M. Novel machine learning approach to identify preoperative risk factors associated with super-utilization of Medicare expenditure following surgery. JAMA Surg. 2019, 154, 1014–1021. [Google Scholar] [CrossRef]
- Sobin, L.H. TNM: Evolution and relation to other prognostic factors. Semin. Surg. Oncol. 2003, 21, 3–7. [Google Scholar] [CrossRef]
- Moro, A.; Mehta, R.; Sahara, K.; Tsilimigras, D.I.; Paredes, A.Z.; Farooq, A.; Hyer, J.M.; Endo, I.; Shen, F.; Guglielmi, A.; et al. The impact of preoperative CA19-9 and CEA on outcomes of patients with intrahepatic cholangiocarcinoma. Ann. Surg. Oncol. 2020, 27, 2888–2901. [Google Scholar] [CrossRef]
- Pan, Q.X.; Su, Z.J.; Zhang, J.H.; Wang, C.R.; Ke, S.Y. Glasgow prognostic score predicts prognosis of intrahepatic cholangiocarcinoma. Mol. Clin. Oncol. 2017, 6, 566–574. [Google Scholar] [CrossRef]
- Miyata, T.; Yamashita, Y.I.; Higashi, T.; Taki, K.; Izumi, D.; Kosumi, K.; Tokunaga, R.; Nakagawa, S.; Okabe, H.; Imai, K.; et al. The prognostic impact of controlling nutritional status (CONUT) in intrahepatic cholangiocarcinoma following curative hepatectomy: A retrospective single institution study. World J. Surg. 2018, 42, 1085–1091. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | High Risk (n = 66) | Moderate Risk (n = 98) | Low Risk (n = 61) | p | Variables | High Risk (n = 66) | Moderate Risk (n = 98) | Low Risk (n = 61) | p | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Age, years | 0.257 | PLR | 0.666 | ||||||||||||
| <70 | 20 | (30%) | 42 | (43%) | 22 | (36%) | <131.4 | 32 | (48%) | 46 | (47%) | 25 | (41%) | ||
| ≥70 | 46 | (70%) | 56 | (57%) | 39 | (64%) | ≥131.4 | 34 | (52%) | 52 | (53%) | 36 | (59%) | ||
| Gender | 0.091 | CAR | <0.001 | ||||||||||||
| Male | 50 | (76%) | 71 | (72%) | 36 | (59%) | <0.042 | 66 | (100%) | 48 | (49%) | 3 | (5%) | ||
| Female | 16 | (24%) | 27 | (28%) | 25 | (41%) | ≥0.042 | 0 | (0%) | 50 | (51%) | 58 | (95%) | ||
| HBsAg | 0.507 | ALBI | <0.001 | ||||||||||||
| Negative | 55 | (83%) | 80 | (82%) | 54 | (89%) | <2.82 | 44 | (67%) | 43 | (44%) | 18 | (30%) | ||
| Positive | 11 | (17%) | 18 | (18%) | 7 | (11%) | ≥2.82 | 22 | (33%) | 55 | (56%) | 43 | (70%) | ||
| HCVAb | 0.093 | ICGR15 (%) | 0.995 | ||||||||||||
| Negative | 56 | (85%) | 91 | (93%) | 58 | (95%) | <9.6 | 27 | (43%) | 41 | (44%) | 25 | (43%) | ||
| Positive | 10 | (15%) | 7 | (7%) | 3 | (5%) | ≥9.6 | 36 | (57%) | 53 | (56%) | 33 | (57%) | ||
| WBC (/μL) | <0.001 | CEA (ng/mL) | 0.006 | ||||||||||||
| <5500 | 40 | (61%) | 48 | (49%) | 17 | (28%) | <2.7 | 36 | (55%) | 48 | (49%) | 17 | (28%) | ||
| ≥5500 | 26 | (39%) | 50 | (51%) | 44 | (72%) | ≥2.7 | 30 | (45%) | 50 | (51%) | 44 | (72%) | ||
| Neutrophil (/μL) | 0.013 | CA19-9 (U/mL) | <0.001 | ||||||||||||
| <3535 | 42 | (64%) | 48 | (49%) | 23 | (38%) | <45 | 66 | (100%) | 47 | (48%) | 0 | (0%) | ||
| ≥3535 | 24 | (36%) | 50 | (51%) | 38 | (62%) | ≥45 | 0 | (0%) | 51 | (52%) | 61 | (100%) | ||
| Lymphocyte (/μL) | 0.837 | Type of hepatectomy | 0.016 | ||||||||||||
| <1347 | 29 | (44%) | 46 | (47%) | 30 | (49%) | 0 or 1 | 30 | (45%) | 35 | (36%) | 13 | (21%) | ||
| ≥1347 | 37 | (56%) | 52 | (53%) | 31 | (51%) | 2 or 3 | 36 | (55%) | 63 | (64%) | 48 | (79%) | ||
| Hemoglobin (g/dL) | 0.151 | Operative blood loss (mL) | 0.117 | ||||||||||||
| <12.8 | 26 | (39%) | 39 | (40%) | 33 | (54%) | <540 | 36 | (55%) | 51 | (52%) | 23 | (38%) | ||
| ≥12.8 | 40 | (61%) | 59 | (60%) | 28 | (46%) | ≥540 | 30 | (45%) | 47 | (48%) | 38 | (62%) | ||
| Platelet (×104/μL) | 0.210 | Morphologic type | 0.956 | ||||||||||||
| <20.1 | 38 | (58%) | 44 | (45%) | 27 | (44%) | MF or IG | 57 | (86%) | 82 | (86%) | 50 | (85%) | ||
| ≥20.1 | 28 | (42%) | 54 | (55%) | 34 | (56%) | PI or MF + PI or others | 9 | (14%) | 13 | (14%) | 9 | (15%) | ||
| Albumin (g/dL) | <0.001 | Differentiation | 0.309 | ||||||||||||
| <4.0 | 15 | (23%) | 44 | (45%) | 33 | (54%) | Well or moderate | 55 | (83%) | 76 | (78%) | 53 | (87%) | ||
| ≥4.0 | 51 | (77%) | 54 | (55%) | 28 | (46%) | Poor or other | 11 | (17%) | 22 | (22%) | 8 | (13%) | ||
| Total bilirubin (mg/dL) | 0.460 | Lymph node status | <0.001 | ||||||||||||
| <0.67 | 32 | (48%) | 44 | (45%) | 23 | (38%) | Negative | 64 | (97%) | 79 | (81%) | 36 | (59%) | ||
| ≥0.67 | 34 | (52%) | 54 | (55%) | 38 | (62%) | Positive | 2 | (3%) | 19 | (19%) | 25 | (41%) | ||
| AST (IU/L) | 0.326 | Number of tumors | 0.098 | ||||||||||||
| <25 | 29 | (44%) | 36 | (37%) | 19 | (31%) | Solitary | 60 | (91%) | 83 | (85%) | 47 | (77%) | ||
| ≥25 | 37 | (56%) | 62 | (63%) | 42 | (69%) | Multiple | 6 | (9%) | 15 | (15%) | 14 | (23%) | ||
| ALT (IU/L) | 0.037 | Tumor size (cm) | 0.037 | ||||||||||||
| <23 | 41 | (62%) | 43 | (44%) | 26 | (43%) | <3.5 | 35 | (53%) | 46 | (47%) | 19 | (31%) | ||
| ≥23 | 25 | (38%) | 55 | (56%) | 35 | (57%) | ≥3.5 | 31 | (47%) | 52 | (53%) | 42 | (69%) | ||
| ALP (U/L) | 0.053 | Major vascular invasion | 0.010 | ||||||||||||
| <298 | 39 | (59%) | 49 | (51%) | 23 | (38%) | Negative | 63 | (95%) | 80 | (82%) | 47 | (77%) | ||
| ≥298 | 27 | (41%) | 48 | (49%) | 38 | (62%) | Positive | 3 | (5%) | 18 | (18%) | 14 | (23%) | ||
| CRP (mg/dL) | <0.001 | Adjuvant chemotherapy | 0.456 | ||||||||||||
| <0.17 | 65 | (98%) | 52 | (53%) | 0 | (0%) | No | 35 | (53%) | 50 | (51%) | 26 | (43%) | ||
| ≥0.17 | 1 | (2%) | 46 | (47%) | 61 | (100%) | Yes | 31 | (47%) | 48 | (49%) | 35 | (57%) | ||
| NLR | 0.105 | AJCC staging | <0.001 | ||||||||||||
| <2.4 | 35 | (53%) | 45 | (46%) | 21 | (34%) | I | 32 | (48%) | 24 | (24%) | 5 | (8%) | ||
| ≥2.4 | 31 | (47%) | 53 | (54%) | 40 | (66%) | II | 22 | (33%) | 36 | (37%) | 16 | (26%) | ||
| PNI | 0.005 | III | 12 | (18%) | 38 | (39%) | 40 | (66%) | |||||||
| <47 | 17 | (26%) | 41 | (42%) | 33 | (54%) | |||||||||
| ≥47 | 49 | (74%) | 57 | (58%) | 28 | (46%) | |||||||||
| Recurrence-Free Survival | Overall Survival | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Variables | Univariate Analysis | Multivariate Analysis | Univariate Analysis | Multivariate Analysis | ||||||||
| HR | (95% CI) | p | HR | (95% CI) | p | HR | (95% CI) | p | HR | (95% CI) | p | |
| Age ≥ 70 years (vs. <70 years) | 0.76 | (0.55–1.07) | 0.113 | 0.98 | (0.65–1.47) | 0.910 | 0.81 | (0.56–1.17) | 0.263 | 1.08 | (0.69–1.70) | 0.724 |
| Neutrophil ≥ 3535 (vs. <3535/μL) | 1.16 | (0.84–1.61) | 0.372 | 0.93 | (0.58–1.49) | 0.776 | 1.07 | (0.74–1.54) | 0.731 | 0.72 | (0.42–1.23) | 0.235 |
| Lymphocyte ≥ 1347 (vs. <1347/μL) | 0.74 | (0.53–1.03) | 0.075 | 0.69 | (0.41–1.14) | 0.148 | 0.71 | (0.49–1.02) | 0.066 | 0.55 | (0.30–1.00) | 0.050 |
| Platelet ≥ 20.1 (vs. <20.1 × 104/μL) | 0.89 | (0.64–1.24) | 0.500 | 0.96 | (0.58–1.59) | 0.889 | 0.83 | (0.57–1.20) | 0.320 | 1.20 | (0.67–2.14) | 0.535 |
| Albumin ≥ 4.0 (vs. <4.0 g/dL) | 0.68 | (0.49–0.95) | 0.023 | 0.67 | (0.46–0.97) | 0.036 | ||||||
| Total bilirubin ≥ 0.67 (vs. <0.67 mg/dL) | 1.55 | (1.10–2.18) | 0.011 | 1.62 | (1.09–2.41) | 0.018 | 1.69 | (1.15–2.48) | 0.008 | 1.81 | (1.13–2.88) | 0.013 |
| ALT ≥ 23 (vs. <23 IU/L) | 1.07 | (0.77–1.48) | 0.691 | 0.75 | (0.48–1.17) | 0.209 | 1.33 | (0.92–1.92) | 0.133 | 0.76 | (0.47–1.25) | 0.282 |
| ALP ≥ 298 (vs. <298 U/L) | 1.48 | (1.06–2.06) | 0.021 | 1.83 | (1.20–2.79) | 0.005 | 1.44 | (1.00–2.09) | 0.052 | 2.01 | (1.24–3.26) | 0.005 |
| CRP ≥ 0.17 (vs. <0.17) | 2.55 | (1.82–3.57) | <0.001 | 2.49 | (1.71–3.63) | < 0.001 | ||||||
| NLR ≥ 2.4 (vs. <2.4) | 1.33 | (0.95–1.85) | 0.093 | 1.03 | (0.60–1.76) | 0.927 | 1.18 | (0.82–1.71) | 0.375 | 0.96 | (0.52–1.80) | 0.909 |
| PNI ≥ 47.0 (vs. <47.0) | 0.63 | (0.45–0.88) | 0.007 | 0.75 | (0.42–1.36) | 0.349 | 0.60 | (0.42–0.88) | 0.008 | 0.65 | (0.32–1.32) | 0.235 |
| PLR ≥ 131.4 (vs. <131.4) | 0.87 | (0.63–1.21) | 0.400 | 0.64 | (0.38–1.10) | 0.105 | 0.81 | (0.56–1.17) | 0.263 | 0.54 | (0.29–1.01) | 0.056 |
| CAR ≥ 0.042 (vs. <0.042) | 2.79 | (1.99–3.91) | <0.001 | 2.67 | (1.83–3.89) | <0.001 | ||||||
| ALBI ≥ 2.82 (vs. <2.82) | 1.71 | (1.23–2.39) | 0.002 | 0.93 | (0.53–1.62) | 0.786 | 1.72 | (1.18–2.50) | 0.005 | 0.67 | (0.35–1.28) | 0.222 |
| ICGR15 ≥ 9.6 (vs. <9.6 %) | 0.96 | (0.69–1.35) | 0.833 | 0.88 | (0.58–1.34) | 0.566 | 1.11 | (0.76–1.61) | 0.601 | 0.95 | (0.59–1.51) | 0.815 |
| CEA ≥ 2.7 (vs. <2.7 ng/mL) | 1.52 | (1.09–2.14) | 0.015 | 0.86 | (0.57–1.31) | 0.492 | 1.59 | (1.09–2.33) | 0.017 | 1.03 | (0.64–1.67) | 0.900 |
| CA19-9 ≥ 45.0 (vs. <45.0 U/mL) | 2.19 | (1.56–3.07) | <0.001 | 2.93 | (1.98–4.33) | <0.001 | ||||||
| Type of hepatectomy 2 or 3 (vs. 0 or 1) | 1.08 | (0.76–1.52) | 0.677 | 0.66 | (0.41–1.05) | 0.082 | 1.07 | (0.73–1.57) | 0.726 | 0.47 | (0.27–0.81) | 0.006 |
| Blood loss ≥ 540 (vs. <540 mL) | 1.78 | (1.27–2.49) | <0.001 | 1.29 | (0.84–1.99) | 0.240 | 1.68 | (1.15–2.45) | 0.007 | 1.10 | (0.67–1.80) | 0.699 |
| Morphologic type PI or MF + PI or others (vs. MF or IG) | 0.75 | (0.44–1.26) | 0.272 | 0.77 | (0.41–1.44) | 0.414 | 0.95 | (0.55–1.64) | 0.849 | 1.26 | (0.62–2.55) | 0.524 |
| Differentiation, poor or others (vs. well or moderate) | 1.56 | (1.04–2.36) | 0.033 | 0.99 | (0.60–1.65) | 0.978 | 1.18 | (0.73–1.90) | 0.493 | 0.66 | (0.36–1.20) | 0.173 |
| Lymph node status, positive (vs. negative) | 2.98 | (2.06–4.31) | <0.001 | 1.97 | (1.09–3.54) | 0.024 | 3.63 | (2.43–5.41) | <0.001 | 3.48 | (1.75–6.94) | <0.001 |
| Number of tumors, multiple (vs. solitary) | 2.47 | (1.65–3.69) | <0.001 | 1.49 | (0.90–2.46) | 0.120 | 2.33 | (1.51–3.58) | <0.001 | 1.83 | (1.08–3.09) | 0.024 |
| Tumor size ≥ 3.5 (vs. <3.5 cm) | 2.07 | (1.47–2.92) | <0.001 | 1.91 | (1.23–2.98) | 0.004 | 2.11 | (1.44–3.10) | <0.001 | 2.55 | (1.53–4.25) | <0.001 |
| Major vascular invasion, positive (vs. negative) | 2.45 | (1.63–3.69) | <0.001 | 1.34 | (0.79–2.29) | 0.279 | 2.36 | (1.48–3.75) | <0.001 | 1.51 | (0.81–2.79) | 0.191 |
| Adjuvant chemotherapy, yes (vs. no) | 1.04 | (0.75–1.45) | 0.802 | 0.89 | (0.60–1.33) | 0.565 | 0.85 | (0.59–1.23) | 0.399 | 0.59 | (0.37–0.92) | 0.020 |
| AJCC staging II (vs. I) | 2.24 | (1.39–3.61) | <0.001 | 1.89 | (1.09–3.29) | 0.024 | 2.50 | (1.44–4.33) | 0.001 | 2.04 | (1.11–3.76) | 0.022 |
| AJCC staging III (vs. I) | 3.15 | (1.99–5.00) | <0.001 | 1.16 | (0.60–2.22) | 0.658 | 4.02 | (2.37–6.80) | <0.001 | 1.21 | (0.55–2.66) | 0.632 |
| Preoperative marker, moderate (vs. low) | 2.81 | (1.75–4.53) | <0.001 | 2.93 | (1.71–5.01) | <0.001 | 3.33 | (1.88–5.92) | <0.001 | 3.75 | (1.96–7.15) | <0.001 |
| Preoperative marker, high (vs. low) | 5.43 | (3.30–8.94) | <0.001 | 5.42 | (2.88–10.22) | <0.001 | 7.19 | (3.99–12.95) | <0.001 | 7.18 | (3.33–15.46) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kaibori, M.; Yoshii, K.; Kosaka, H.; Ota, M.; Komeda, K.; Ueno, M.; Hokutou, D.; Iida, H.; Matsui, K.; Sekimoto, M. Preoperative Serum Markers and Risk Classification in Intrahepatic Cholangiocarcinoma: A Multicenter Retrospective Study. Cancers 2022, 14, 5459. https://doi.org/10.3390/cancers14215459
Kaibori M, Yoshii K, Kosaka H, Ota M, Komeda K, Ueno M, Hokutou D, Iida H, Matsui K, Sekimoto M. Preoperative Serum Markers and Risk Classification in Intrahepatic Cholangiocarcinoma: A Multicenter Retrospective Study. Cancers. 2022; 14(21):5459. https://doi.org/10.3390/cancers14215459
Chicago/Turabian StyleKaibori, Masaki, Kengo Yoshii, Hisashi Kosaka, Masato Ota, Koji Komeda, Masaki Ueno, Daisuke Hokutou, Hiroya Iida, Kosuke Matsui, and Mitsugu Sekimoto. 2022. "Preoperative Serum Markers and Risk Classification in Intrahepatic Cholangiocarcinoma: A Multicenter Retrospective Study" Cancers 14, no. 21: 5459. https://doi.org/10.3390/cancers14215459