
Oncological Outcomes of Distal Ureterectomy for High-Risk Urothelial Carcinoma: A Multicenter Study by The French Bladder Cancer Committee
 ,
,  , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Material & Methods
2.1. Patients’ Selection (Figure 1: Flow Chart)

2.2. Variables Retrieval and Definition
2.2.1. Patient Characteristics
2.2.2. Surgical Technique
2.2.3. Perioperative Variables
2.2.4. Pathological Variables
2.3. Endpoints
2.4. Statistical Analysis
3. Results
3.1. Patients’ Characteristics
3.2. Operative and Pathological Characteristics (Table 2)

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total | 155 |
|---|---|
| Surgical approach - Open - Mini-invasive - Missing | 141 (91%) 11 (9%) 3 (1.9%) |
| Operative time Mean (SD) | 165.6 (58.9) |
| Blood loss (mL) Mean (SD) | 268.1 (246.4) |
| Lymphadenectomy | 55 (35.4%) |
| Distal ureter management - Extravesical - Transvesical - Endoscopic - Missing | 103 (66.4%) 37 (23.8%) 7 (4.6%) 8 (5.2%) |
| LOS Mean (SD) | 8.7 (7.6) |
| Post-operative complications - Clavien 1 - Clavien 2 - Clavien 3a/3b - Clavien 4 - Clavien 5 | 14 (9%) 24 (15.5%) 1/9 (0.6%/5.8%) 3 (1.9%) 1 (0.6%) |
| 1973 DU grade - G1 - G2 - G3 - Missing | 16 (10.3%) 39 (25.1%) 90 (58%) 10 (6.4%) |
| 2004 DU grade - LG - HG - Missing | 44 (28.3%) 102 (65.8%) 9 (5.8%) |
| pT - pT0 - pTa - pT1 - pTis - pT2 - pT3 - pT4 | 6 (3.9%) 73 (47.1%) 32 (20.7%) 1 (0.6%) 20 (12.9%) 20 (12.9%) 3 (1.9%) |
| pN - pN0 - pN1 - pN2 - pNx | 49 (31.7%) 1 (0.6%) 2 (1.3%) 103 (66.4%) |
| Total Nodes Mean (SD) | 5.8 (5.5) |
| Margins - Distal positive margins - Lateral positive margins | 23 (14.8%) 11 (7%) |
3.3. Oncological Outcomes
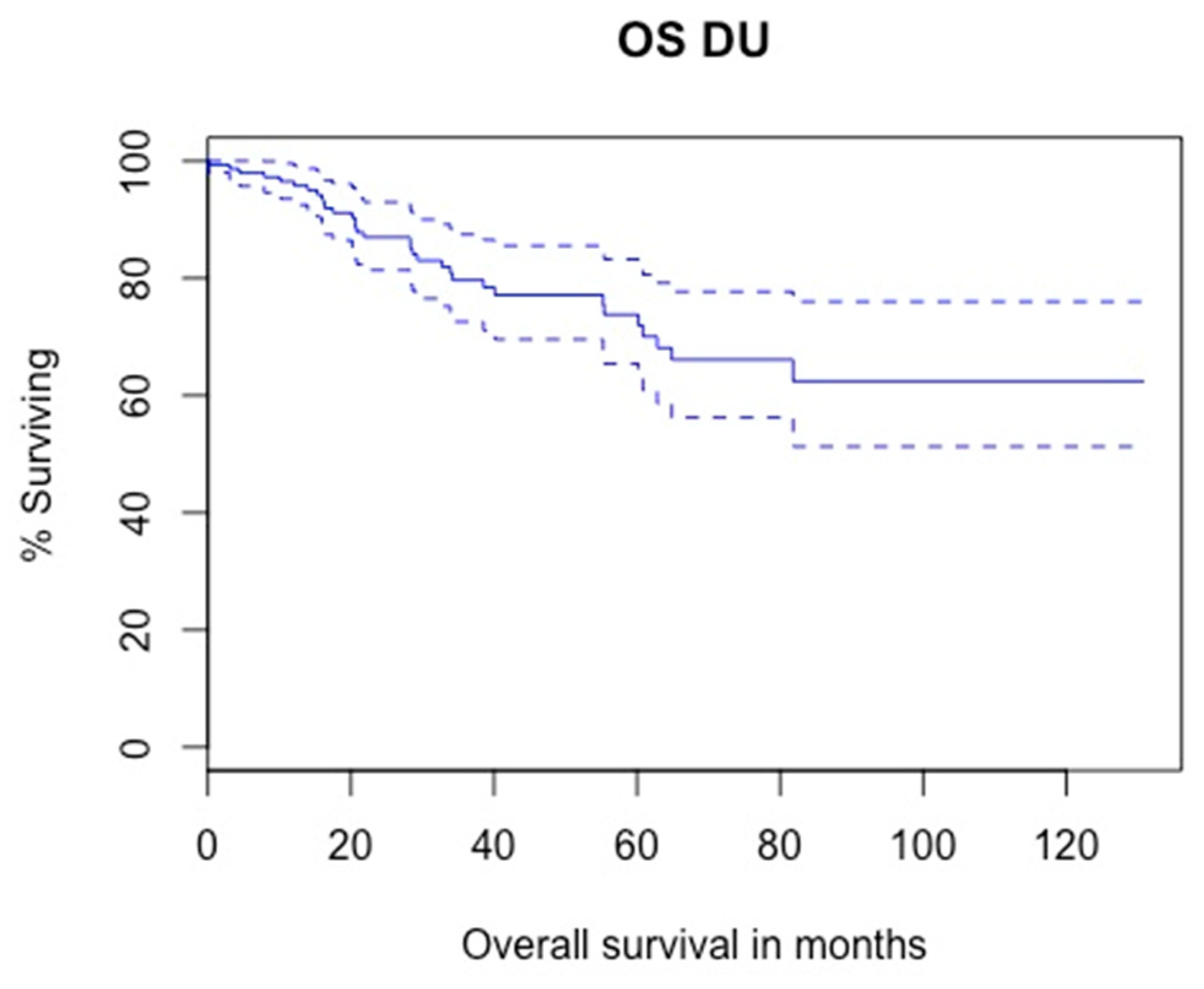
3.3.1. Overall Survival
3.3.2. Cancer-Specific Survival
3.3.3. Intra Vesical Recurrence
3.3.4. Homolateral Upper Tract Recurrence
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2022. CA A Cancer J. Clin. 2022, 72, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Ouzzane, A.; Rouprêt, M.; Leon, P.; Yates, D.R.; Colin, P. Épidémiologie et facteurs de risque des tumeurs de la voie excrétrice urinaire supérieure: Revue de la littérature pour le rapport annuel de l’Association française d’urologie. Progrès Urol. 2014, 24, 966–976. [Google Scholar] [CrossRef] [PubMed]
- Pignot, G.; Colin, P.; Rouprêt, M.; Traxer, O. Conservative management of urothelial carcinomas of the upper tract: Systematic review for the yearly scientific report of the French National Association of Urology. Prog. Urol. 2014, 24, 1011–1020. [Google Scholar] [CrossRef] [PubMed]
- Xylinas, E.; Rink, M.; Cha, E.K.; Clozel, T.; Lee, R.K.; Fajkovic, H.; Comploj, E.; Novara, G.; Margulis, V.; Raman, J.D.; et al. Impact of Distal Ureter Management on Oncologic Outcomes Following Radical Nephroureterectomy for Upper Tract Urothelial Carcinoma. Eur. Urol. 2014, 65, 210–217. [Google Scholar] [CrossRef] [PubMed]
- Fukushima, H.; Saito, K.; Ishioka, J.; Matsuoka, Y.; Numao, N.; Koga, F.; Masuda, H.; Fujii, Y.; Sakai, Y.; Arisawa, C.; et al. Equivalent Survival and Improved Preservation of Renal Function after Distal Ureterectomy Compared with Nephroureterectomy in Patients with Urothelial Carcinoma of the Distal Ureter: A Propensity Score-Matched Multicenter Study: Clinical Outcomes of Distal Ureterectomy. Int. J. Urol. 2014, 21, 1098–1104. [Google Scholar] [CrossRef] [Green Version]
- Birtle, A.; Johnson, M.; Chester, J.; Jones, R.; Dolling, D.; Bryan, R.T.; Harris, C.; Winterbottom, A.; Blacker, A.; Catto, J.W.F.; et al. Adjuvant Chemotherapy in Upper Tract Urothelial Carcinoma (the POUT Trial): A Phase 3, Open-Label, Randomised Controlled Trial. Lancet 2020, 395, 1268–1277. [Google Scholar] [CrossRef]
- Rouprêt, M.; Babjuk, M.; Burger, M.; Capoun, O.; Cohen, D.; Compérat, E.M.; Cowan, N.C.; Dominguez-Escrig, J.L.; Gontero, P.; Hugh Mostafid, A.; et al. European Association of Urology Guidelines on Upper Urinary Tract Urothelial Carcinoma: 2020 Update. Eur. Urol. 2021, 79, 62–79. [Google Scholar] [CrossRef]
- Colin, P.; Ouzzane, A.; Pignot, G.; Ravier, E.; Crouzet, S.; Ariane, M.M.; Audouin, M.; Neuzillet, Y.; Albouy, B.; Hurel, S.; et al. Comparison of Oncological Outcomes after Segmental Ureterectomy or Radical Nephroureterectomy in Urothelial Carcinomas of the Upper Urinary Tract: Results from a Large French Multicentre Study. BJU Int. 2012, 110, 1134–1141. [Google Scholar] [CrossRef]
- Charlson, M.E.; Carrozzino, D.; Guidi, J.; Patierno, C. Charlson Comorbidity Index: A Critical Review of Clinimetric Properties. Psychother. Psychosom. 2022, 91, 8–35. [Google Scholar] [CrossRef]
- Clavien, P.A.; Barkun, J.; de Oliveira, M.L.; Vauthey, J.N.; Dindo, D.; Schulick, R.D.; de Santibañes, E.; Pekolj, J.; Slankamenac, K.; Bassi, C.; et al. The Clavien-Dindo Classification of Surgical Complications: Five-Year Experience. Ann. Surg. 2009, 250, 187–196. [Google Scholar] [CrossRef]
- Fang, C.; Xie, X.; Xu, T.; He, W.; He, H.; Wang, X.; Zhu, Y.; Shen, Z.; Shao, Y. Segmental Ureterectomy Is Not Inferior to Radical Nephroureterectomy for Either Middle or Distal Ureter Urothelial Cell Carcinomas within 3.5 cm. Int. Urol. Nephrol. 2017, 49, 1177–1182. [Google Scholar] [CrossRef] [PubMed]
- Katayama, S.; Mori, K.; Schuettfort, V.M.; Pradere, B.; Mostafaei, H.; Quhal, F.; Rajwa, P.; Motlagh, R.S.; Laukhtina, E.; Moschini, M.; et al. Accuracy and Clinical Utility of a Tumor Grade- and Stage-Based Predictive Model in Localized Upper Tract Urothelial Carcinoma. Eur. Urol. Focus 2021, 8, 761–768. [Google Scholar] [CrossRef] [PubMed]
- Marcq, G.; Foerster, B.; Abufaraj, M.; Matin, S.F.; Azizi, M.; Gupta, M.; Li, W.-M.; Seisen, T.; Clinton, T.; Xylinas, E.; et al. Novel Classification for Upper Tract Urothelial Carcinoma to Better Risk-Stratify Patients Eligible for Kidney-Sparing Strategies: An International Collaborative Study. Eur. Urol. Focus 2022, 8, 491–497. [Google Scholar] [CrossRef] [PubMed]
- Foerster, B.; Abufaraj, M.; Matin, S.F.; Azizi, M.; Gupta, M.; Li, W.-M.; Seisen, T.; Clinton, T.; Xylinas, E.; Mir, M.C.; et al. Pretreatment Risk Stratification for Endoscopic Kidney-Sparing Surgery in Upper Tract Urothelial Carcinoma: An International Collaborative Study. Eur. Urol. 2021, 80, 507–515. [Google Scholar] [CrossRef] [PubMed]
- Lane, B.R.; Smith, A.K.; Larson, B.T.; Gong, M.C.; Campbell, S.C.; Raghavan, D.; Dreicer, R.; Hansel, D.E.; Stephenson, A.J. Chronic Kidney Disease after Nephroureterectomy for Upper Tract Urothelial Carcinoma and Implications for the Administration of Perioperative Chemotherapy. Cancer 2010, 116, 2967–2973. [Google Scholar] [CrossRef]
- Fang, D.; Seisen, T.; Yang, K.; Liu, P.; Fan, X.; Singla, N.; Xiong, G.; Zhang, L.; Li, X.; Zhou, L. A Systematic Review and Meta-Analysis of Oncological and Renal Function Outcomes Obtained after Segmental Ureterectomy versus Radical Nephroureterectomy for Upper Tract Urothelial Carcinoma. Eur. J. Surg. Oncol. 2016, 42, 1625–1635. [Google Scholar] [CrossRef] [PubMed]
- Weight, C.J.; Larson, B.T.; Fergany, A.F.; Gao, T.; Lane, B.R.; Campbell, S.C.; Kaouk, J.H.; Klein, E.A.; Novick, A.C. Nephrectomy Induced Chronic Renal Insufficiency Is Associated with Increased Risk of Cardiovascular Death and Death From Any Cause in Patients With Localized CT1b Renal Masses. J. Urol. 2010, 183, 1317–1323. [Google Scholar] [CrossRef]
- Jeldres, C.; Lughezzani, G.; Sun, M.; Isbarn, H.; Shariat, S.F.; Budaus, L.; Lattouf, J.-B.; Widmer, H.; Graefen, M.; Montorsi, F.; et al. Segmental Ureterectomy Can Safely Be Performed in Patients with Transitional Cell Carcinoma of the Ureter. J. Urol. 2010, 183, 1324–1329. [Google Scholar] [CrossRef]
- Piraino, J.A.; Snow, Z.A.; Edwards, D.C.; Hager, S.; McGreen, B.H.; Diorio, G.J. Nephroureterectomy vs. Segmental Ureterectomy of Clinically Localized, High-Grade, Urothelial Carcinoma of the Ureter: Practice Patterns and Outcomes. Urol. Oncol. Semin. Orig. Investig. 2020, 38, 851-e1. [Google Scholar] [CrossRef]
- Seisen, T.; Nison, L.; Remzi, M.; Klatte, T.; Mathieu, R.; Lucca, I.; Bozzini, G.; Capitanio, U.; Novara, G.; Cussenot, O.; et al. Oncologic Outcomes of Kidney Sparing Surgery versus Radical Nephroureterectomy for the Elective Treatment of Clinically Organ Confined Upper Tract Urothelial Carcinoma of the Distal Ureter. J. Urol. 2016, 195, 1354–1361. [Google Scholar] [CrossRef]
- Dalpiaz, O.; Ehrlich, G.; Quehenberger, F.; Pummer, K.; Zigeuner, R. Distal Ureterectomy Is a Safe Surgical Option in Patients with Urothelial Carcinoma of the Distal Ureter. Urol. Oncol. 2014, 32, 34-e1. [Google Scholar] [CrossRef] [PubMed]
- Ito, Y.; Kikuchi, E.; Tanaka, N.; Miyajima, A.; Mikami, S.; Jinzaki, M.; Oya, M. Preoperative Hydronephrosis Grade Independently Predicts Worse Pathological Outcomes in Patients Undergoing Nephroureterectomy for Upper Tract Urothelial Carcinoma. J. Urol. 2011, 185, 1621–1626. [Google Scholar] [CrossRef] [PubMed]
- Verhoest, G.; Shariat, S.F.; Chromecki, T.F.; Raman, J.D.; Margulis, V.; Novara, G.; Seitz, C.; Remzi, M.; Rouprêt, M.; Scherr, D.S.; et al. Predictive Factors of Recurrence and Survival of Upper Tract Urothelial Carcinomas. World J. Urol. 2011, 29, 495–501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ng, C.K.; Shariat, S.F.; Lucas, S.M.; Bagrodia, A.; Lotan, Y.; Scherr, D.S.; Raman, J.D. Does the Presence of Hydronephrosis on Preoperative Axial CT Imaging Predict Worse Outcomes for Patients Undergoing Nephroureterectomy for Upper-Tract Urothelial Carcinoma? Urol. Oncol. 2011, 29, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Jia, Z.; Gong, Y.-Q.; Zhang, C.-J.; Bao, Z.-Q.; Li, X.-S.; Hao, H.; Xiong, G.-Y.; Zhang, L.; Fang, D.; He, Z.-S.; et al. Segmental Ureterectomy Can Be Performed Safely in Patients with Urothelial Carcinoma of Distal Ureter. Can. Urol. Assoc. J. 2019, 13, E202–E209. [Google Scholar] [CrossRef]
- Pieras, E.; Frontera, G.; Ruiz, X.; Vicens, A.; Ozonas, M.; Pizá, P. Concomitant Carcinoma in Situ and Tumour Size Are Prognostic Factors for Bladder Recurrence after Nephroureterectomy for Upper Tract Transitional Cell Carcinoma. BJU Int. 2010, 106, 1319–1323. [Google Scholar] [CrossRef]
- Otto, W.; Shariat, S.F.; Fritsche, H.-M.; Gupta, A.; Matsumoto, K.; Kassouf, W.; Martignoni, G.; Walton, T.J.; Tritschler, S.; Baba, S.; et al. Concomitant Carcinoma in Situ as an Independent Prognostic Parameter for Recurrence and Survival in Upper Tract Urothelial Carcinoma: A Multicenter Analysis of 772 Patients. World J. Urol. 2011, 29, 487–494. [Google Scholar] [CrossRef]
- Wheat, J.C.; Weizer, A.Z.; Wolf, J.S.; Lotan, Y.; Remzi, M.; Margulis, V.; Wood, C.G.; Montorsi, F.; Roscigno, M.; Kikuchi, E.; et al. Concomitant Carcinoma in Situ Is a Feature of Aggressive Disease in Patients with Organ Confined Urothelial Carcinoma Following Radical Nephroureterectomy. Urol. Oncol. Semin. Orig. Investig. 2012, 30, 252–258. [Google Scholar] [CrossRef]
- Sharma, V.; Miest, T.S.; Juvet, T.S.; Toussi, A.; Packiam, V.; Chamie, K.; Matin, S.F.; Boorjian, S.A.; Thompson, R.H.; Frank, I.; et al. The Impact of Upper Tract Urothelial Carcinoma Diagnostic Modality on Intravesical Recurrence after Radical Nephroureterectomy: A Single Institution Series and Updated Meta-Analysis. J. Urol. 2021, 206, 558–567. [Google Scholar] [CrossRef]
- Sountoulides, P.; Pyrgidis, N.; Brookman-May, S.; Mykoniatis, I.; Karasavvidis, T.; Hatzichristou, D. Does Ureteral Stenting Increase the Risk of Metachronous Upper Tract Urothelial Carcinoma in Patients with Bladder Tumors? A Systematic Review and Meta-Analysis. J. Urol. 2021, 205, 956–966. [Google Scholar] [CrossRef]




| Total | 155 |
|---|---|
| AgeMean (SD) | 72.6 (10.5) |
| Gender - Male Female | 113 (72.9 %) 42 (27.1 %) |
| Charlson score Mean (SD) | 6.19 (2.4) |
| BMI Mean (SD) | 25.47 (4.9) |
| Pre-operative GFR - <60 mL/min - > or = 60 mL/lmin Missing | 55 (35.5%) 66 (42.5%) 34 (22%) |
| Prior BC Synchronous BC | 43 (27.7%) 28 (18%) |
| Abdominal CT report - Local invasion (>T2) - Hydronephrosis Enlarged pelvic nodes | 5 (3.2%) 114 (73.5%) 8 (5.1%) |
| 1973 Biopsy grade - G1 - G2 - G3 Missing | 22 (21.2%) 35 (33.6%) 34 (32.7%) 13 (12.5%) |
| 2004 Biopsy grade - LG - HG Missing | 51 (49%) 41 (39.4%) 12 (11.6%) |
| cTNM - cTxN0M0 - cTaN0M0 - cTaN1M0 - cT1N0M0 - cT2N0M0 - cTxN1M0 - cTxN2M0 cT2N2M0 | 60 (38.7%) 69 (44.6%) 2 (1.3%) 16 (10.3%) 4 (2.6%) 2 (1.3%) 1 (0.6%) 1 (0.6%) |
| Multifocality | 7 (4.5%) |
| Size (in mm) Mean (SD) | 25.76 (14.1) |
| Location - Meatus - Distal ureter - Meatus + distal ureter Missing | 7 (4.5%) 96 (61.9%) 39 (25.1%) 13 (8.3%) |
| Preoperative JJ stent | 74 (47.7%) |
| EAU risk group Low High | 14 (9%) 141 (91%) |
| Univariate | Multivariate | |||||
|---|---|---|---|---|---|---|
| Variable | p | HR | 95% CI | p | HR | 95% CI |
| Age (continuous) | 0.01 * | 1.05 | 1.01–1.09 | 0.15 | 1.06 | 0.97–1.16 |
| Gender Male Female | 0.70 | 1.15 | 0.53–2.59 | |||
| Charlson (continuous) | 0.07 | 1.14 | 0.98–1.33 | |||
| GFR >60 mL/min <60 mL/min | Ref 0.01 * | 2.67 | 1.21–5.87 | 0.39 | 0.55 | 0.14–2.17 |
| cTN cTaN0 cT1N0 cT2N0 cTanyN1–2 cTxN0M0 | Ref 0.62 0.08 0.002 * 0.19 | 1.37 6.20 7.80 1.67 | 0.38–4.86 0.76–50.41 2.08–29.13 0.77–3.62 | |||
| Multifocality No Yes | Ref 0.01 * | 3.95 | 1.38–11.42 | 0.08 | 4.98 | 0.80–30.93 |
| 2004 biopsy grade LG HG | Ref 0.08 | 2.29 | 0.88–5.92 | 0.04 * | 3.46 | 1.01–11.96 |
| Hydronephrosis No Yes | Ref 0.70 | 0.85 | 0.38–1.91 | |||
| Size (continuous) | 0.03 * | 1.02 | 1.00–1.04 | 0.004 * | 1.07 | 1.02–1.12 |
| Univariate | Multivariate | |||||
|---|---|---|---|---|---|---|
| Variable | p | HR | 95% CI | p | HR | 95% CI |
| Age (continuous) | 0.09 | 1.04 | 0.99–1.10 | |||
| Hydronephrosis No yes | Ref 0.99 | 1.00 | 0.32–3.08 | |||
| Size (continuous) | 0.01 * | 1.03 | 1.00–1.05 | 0.004 * | 1.09 | 1.02–1.15 |
| cTN cTaN0 cT1N0 cT2N0 cTanyN1–2 cTxN0M0 | Ref 0.69 0.025 * 0.007 * 0.03 * | 1.58 13.96 12.23 4.15 | 0.16–15.19 1.39–140.20 1.98–75.35 1.14–15.10 | |||
| Multifocality No Yes | Ref 0.06 | 4.02 | 0.90–17.91 | 0.12 | 6.05 | 0.60–61.05 |
| 2004 biopsy grade LG HG | Ref 0.07 | 7.25 | 0.84–62.14 | 0.05 * | 8.77 | 0.96–79.53 |
| Cytology Neg Atypical Positive for HG No Diag | Ref 0.86 0.09 0.20 | 0.81 4.00 2.99 | 0.07–9.02 0.77–20.69 0.54–16.40 | |||
| Past history NMIBC No Yes | Ref 0.55 | 0.71 | 0.23–2.18 | |||
| Synchronous NMIBC No Yes | Ref 0.99 | 1.00 | 0.28–3.50 | |||
| Distal margins Negative Positive | Ref <0.01 * | 5.20 | 1.95–13.8 | |||
| Lateral Margins Negative Positive | Ref <0.01 * | 13.72 | 5.02–37.46 | |||
| Univariate | Multivariate | |||||
|---|---|---|---|---|---|---|
| Variable | p | HR | 95% CI | p | HR | 95% CI |
| Gender Male Female | 0.8 | 0.92 | 0.52–1.65 | |||
| GFR >60 mL/min <60 mL/min | Ref 0.31 | 1.31 | 0.76–2.28 | |||
| Tobacco use Never Present Past | Ref 0.78 0.15 | 0.91 1.53 | 0.46–1.79 0.85–2.74 | |||
| Past history NMIBC No Yes | Ref 0.57 | 0.85 | 0.50–1.45 | |||
| Synchronous NMIBC No Yes | Ref 0.67 | 1.13 | 0.61–2.08 | |||
| Hydronephrosis No yes | Ref 0.95 | 1.01 | 0.57–1.78 | |||
| Size (continuous) | 0.04 * | 1.01 | 1.00–1.03 | 0.06 | 1.01 | 0.99–1.03 |
| cTN cTaN0 cT1N0 cT2N0 cTanyN1–2 cTxN0M0 | Ref 0.33 0.09 * 0.23 0.07 * | 1.50 3.47 2.06 1.61 | 0.65–3.45 0.80–14.96 0.62–6.87 0.94–2.74 | |||
| Multifocality No Yes | Ref 0.36 | 1.60 | 0.58–4.41 | |||
| 2004 biopsy grade LG HG | Ref 0.20 | 1.50 | 0.80–2.79 | |||
| Cytology Neg Atypical Positive for HG No Diag | Ref 0.11 0.16 0.74 | 2.01 1.89 0.85 | 0.85–4.77 0.76–4.68 0.32–2.24 | |||
| JJ preop No Yes | 0.70 | 1.10 | 0.65–1.86 | |||
| URSS diag No Yes | Ref 0.35 | 0.78 | 0.47–1.31 | |||
| Distal ureter management - Extravesical - Transvesical - Endoscopic | Ref 0.44 0.37 | 0.79 1.51 | 0.43–1.44 0.60–3.83 | |||
| Distal margins Negative Positive | Ref 0.018 * | 2.09 | 1.13–3.86 | Ref 0.04 * | 1.93 | 1.01–3.70 |
| Univariate | Multivariate | |||||
|---|---|---|---|---|---|---|
| Variable | p | HR | 95% CI | p | HR | 95% CI |
| Hydronephrosis No yes | Ref 0.72 | 1.17 | 0.47–2.90 | |||
| Size <2 cm >= 2 cm | Ref 0.02 * | 3.33 | 1.13–9.76 | 0.02 * | 3.59 | 1.22–10.60 |
| cTN cTaN0 cT1N0 cT2N0 cTanyN1–2 cTxN0M0 | Ref 0.87 0.99 0.41 0.03 * | 0.90 NA 1.85 0.34 | 0.26–3.07 0.42–8.12 0.12–0.93 | |||
| Multifocality No Yes | Ref 0.07 * | 3.04 | 0.91–10.2 | 0.04 * | 3.44 | 1.01–11.71 |
| 2004 biopsy grade LG HG | Ref 0.24 | 1.63 | 0.71–3.70 | |||
| JJ preop No Yes | 0.29 | 1.52 | 0.69–3.33 | |||
| URSS diag No Yes | Ref 0.25 | 1.66 | 0.69–3.97 | |||
| Past history NMIBC No Yes | Ref 0.36 | 1.42 | 0.66–3.04 | |||
| Synchronous NMIBC No Yes | Ref 0.37 | 1.47 | 0.62–3.49 | |||
| Distal margins Negative Postive | Ref 0.76 | 1.17 | 0.40–3.41 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Masson-Lecomte, A.; Vaillant, V.; Roumiguié, M.; Lévy, S.; Pradère, B.; Peyromaure, M.; Duquesne, I.; De La Taille, A.; Lebâcle, C.; Panis, A.; et al. Oncological Outcomes of Distal Ureterectomy for High-Risk Urothelial Carcinoma: A Multicenter Study by The French Bladder Cancer Committee. Cancers 2022, 14, 5452. https://doi.org/10.3390/cancers14215452
Masson-Lecomte A, Vaillant V, Roumiguié M, Lévy S, Pradère B, Peyromaure M, Duquesne I, De La Taille A, Lebâcle C, Panis A, et al. Oncological Outcomes of Distal Ureterectomy for High-Risk Urothelial Carcinoma: A Multicenter Study by The French Bladder Cancer Committee. Cancers. 2022; 14(21):5452. https://doi.org/10.3390/cancers14215452
Chicago/Turabian StyleMasson-Lecomte, Alexandra, Victoire Vaillant, Mathieu Roumiguié, Stéphan Lévy, Benjamin Pradère, Michaël Peyromaure, Igor Duquesne, Alexandre De La Taille, Cédric Lebâcle, Adrien Panis, and et al. 2022. "Oncological Outcomes of Distal Ureterectomy for High-Risk Urothelial Carcinoma: A Multicenter Study by The French Bladder Cancer Committee" Cancers 14, no. 21: 5452. https://doi.org/10.3390/cancers14215452