
Human Papillomavirus Oncoproteins Confer Sensitivity to Cisplatin by Interfering with Epidermal Growth Factor Receptor Nuclear Trafficking Related to More Favorable Clinical Survival Outcomes in Non-Small Cell Lung Cancer

 , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Cell Culture, Plasmids, and Transfection
2.2. Flow Cytometry
2.3. Kinetic Study of Nuclear Localization of EGFR
2.4. MTT Assay
2.5. Animal Studies
2.6. Patient Population
2.7. Immunohistochemistry
2.8. Statistical Analyses
3. Results
3.1. High EGFR Protein Expression in Transfected H292-HPV16E5, H292-HPV16E6, and H292-HPV16E7 Cells
3.2. Increased Phosphorylated Nuclear EGFR Protein Levels after EGF Stimulus in Transfected H292-HPV16E5, H292-HPV16E6, and H292-HPV16E7 Cells
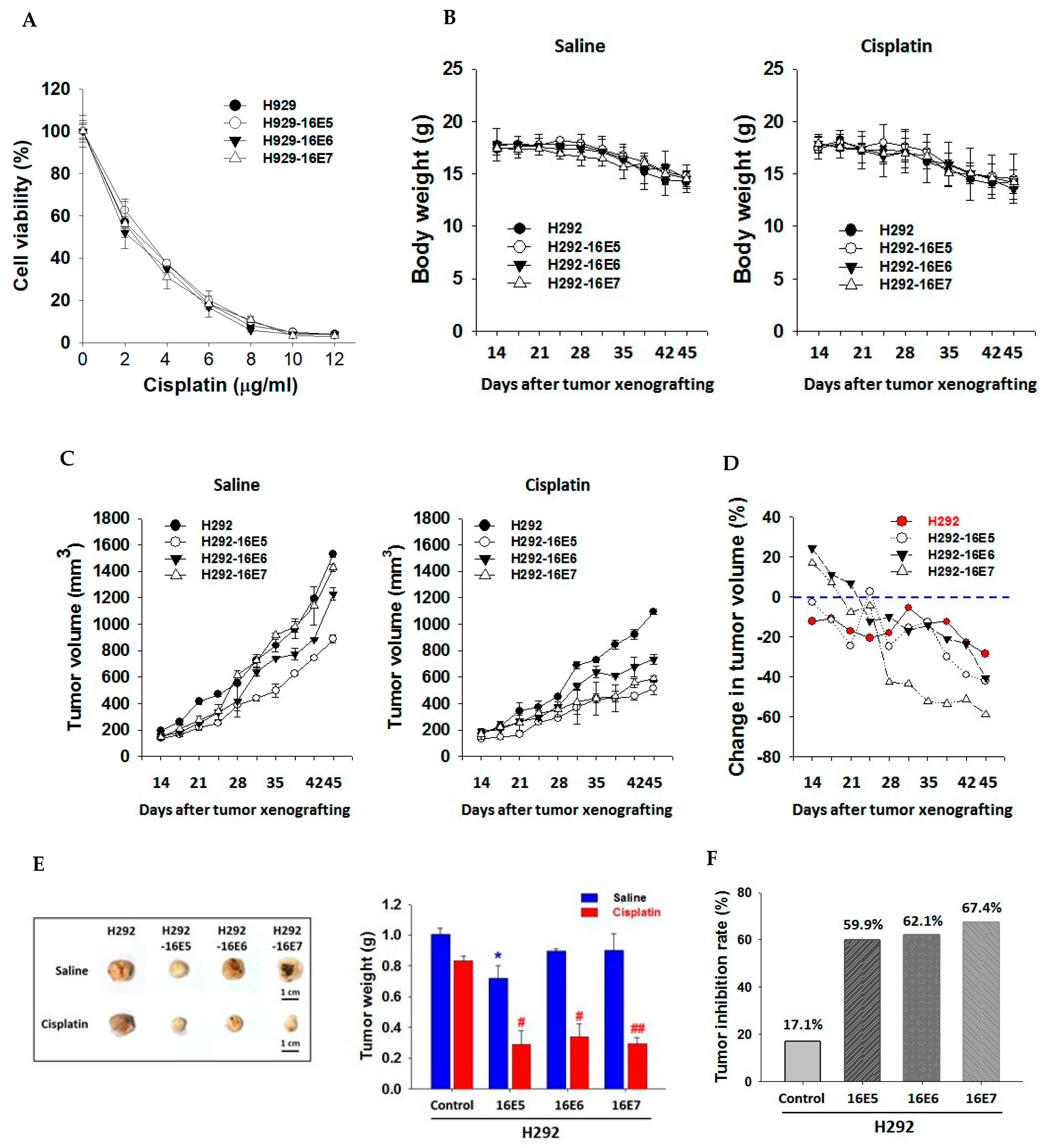
3.3. Better Treatment Responses to Cisplatin in Transfected H292-HPV16E5, H292-HPV16E6, and H292-HPV16E7 H292 Cells
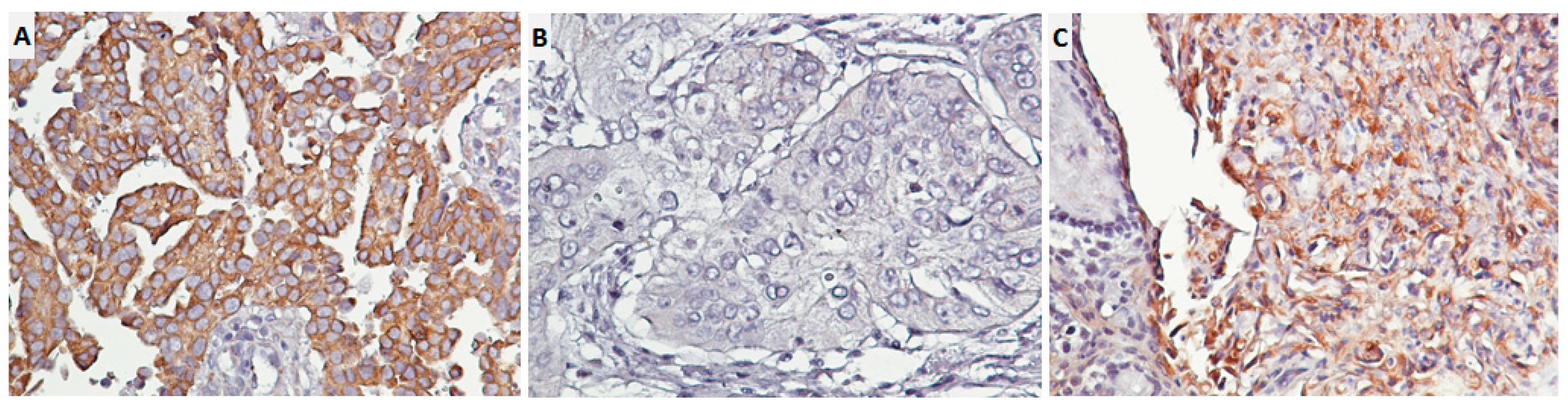
3.4. High HPV 16E6/18E6 Expression Related to High Nuclear and Membranous EGFR Expression in 243 Primary Lung Cancer Tissues
3.5. Lower Prevalence of E6+tEGFR+ Expression in Lung Adenocarcinoma Patients at an Advanced Stage
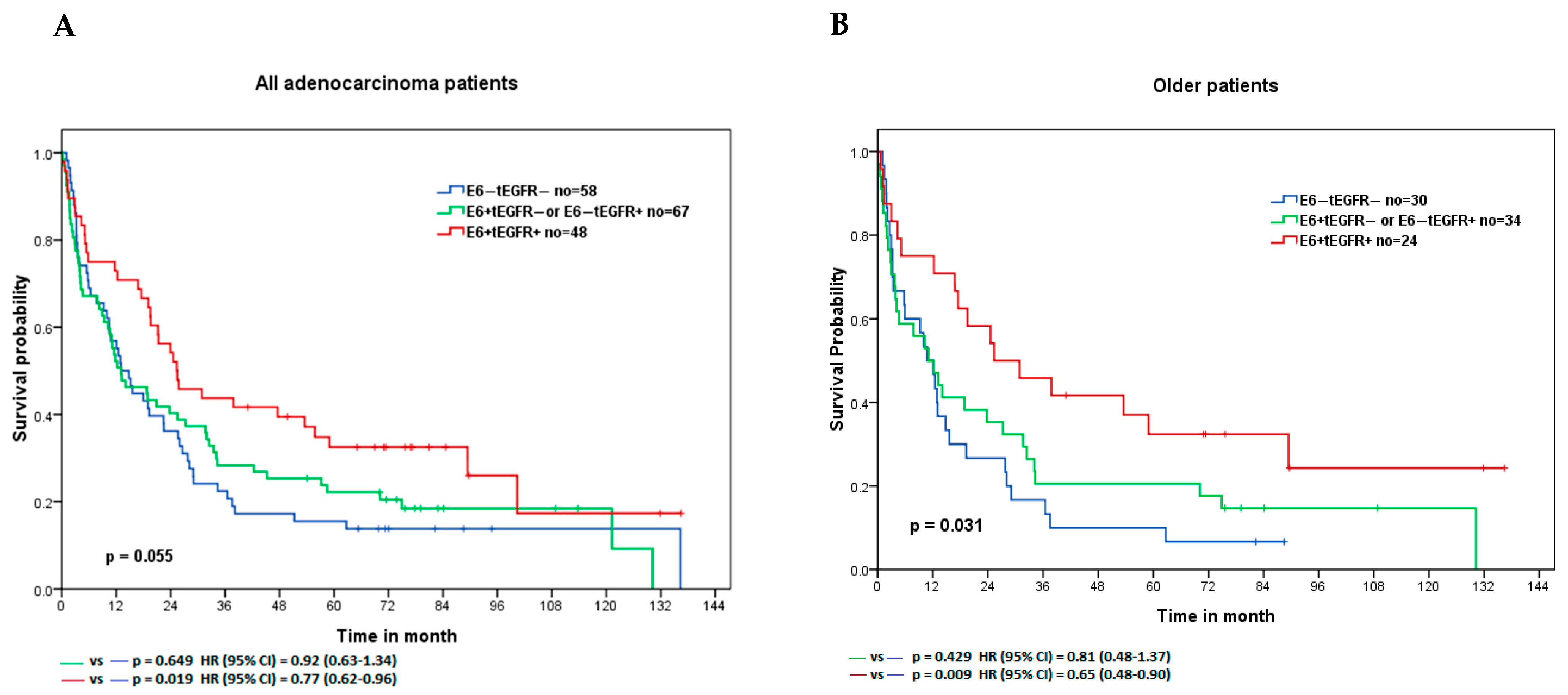
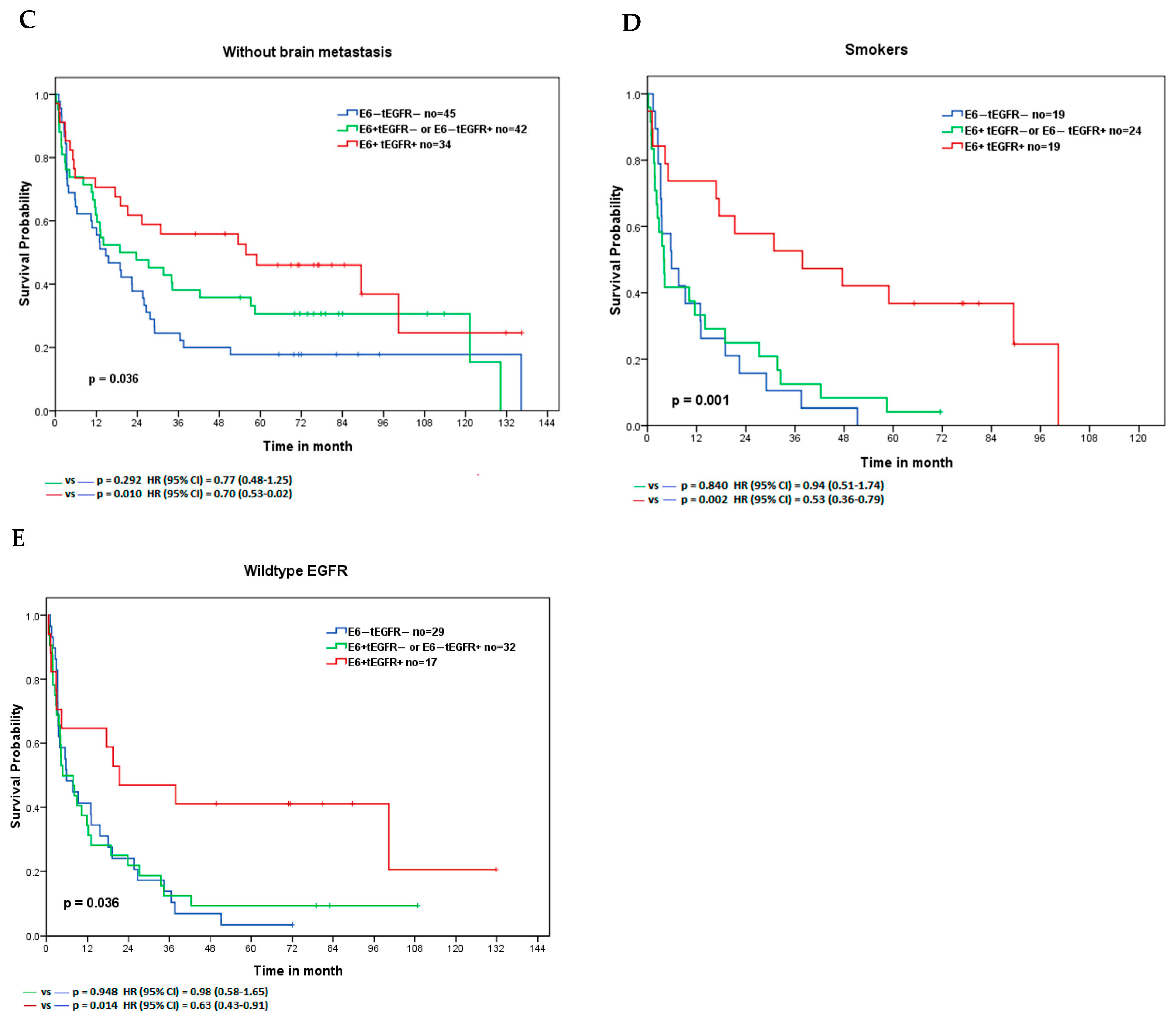
3.6. Lung Adenocarcinoma Patients with E6+tEGFR+ Expression Had the Longest Survival Time with a Better Treatment Response to Cisplatin
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.C.; Chen, J.H.; Richard, K.; Chen, P.Y.; Christiani, D.C. Lung adenocarcinoma and human papillomavirus infection. Cancer 2004, 101, 1428–1436. [Google Scholar] [CrossRef] [PubMed]
- Tsyganov, M.M.; Pevzner, A.M.; Ibragimova, M.K.; Deryusheva, I.V.; Litviakov, N.V. Human papillomavirus and lung cancer: An overview and a meta-analysis. J. Cancer Res. Clin. Oncol. 2019, 145, 1919–1937. [Google Scholar] [CrossRef] [PubMed]
- Ragin, C.; Obikoya-Malomo, M.; Kim, S.; Chen, Z.; Flores-Obando, R.; Gibbs, D.; Koriyama, C.; Aguayo, F.; Koshiol, J.; Caporaso, N.E.; et al. HPV-associated lung cancers: An international pooled analysis. Carcinogenesis 2014, 35, 1267–1275. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.L.; Fang, C.L.; Wang, M.; Yu, M.C.; Bai, K.J.; Lu, P.C.; Liu, H.E. Human papillomavirus infections as a marker to predict overall survival in lung adenocarcinoma. Int. J. Cancer 2014, 134, 65–71. [Google Scholar] [CrossRef]
- Sigismund, S.; Avanzato, D.; Lanzetti, L. Emerging functions of the EGFR in cancer. Mol. Oncol. 2018, 12, 3–20. [Google Scholar] [CrossRef] [Green Version]
- Bethune, G.; Bethune, D.; Ridgway, N.; Xu, Z. Epidermal growth factor receptor (EGFR) in lung cancer: An overview and update. J. Thorac. Dis. 2010, 2, 48–51. [Google Scholar]
- Carcereny, E.; Moran, T.; Capdevila, L.; Cros, S.; Vila, L.; de Los Llanos Gil, M.; Remon, J.; Rosell, R. The epidermal growth factor receptor (EGRF) in lung cancer. Transl. Respir. Med. 2015, 3, 1. [Google Scholar] [CrossRef] [Green Version]
- Brand, T.M.; Iida, M.; Li, C.; Wheeler, D.L. The nuclear epidermal growth factor receptor signaling network and its role in cancer. Discov. Med. 2011, 12, 419–432. [Google Scholar]
- Wang, Y.N.; Hung, M.C. Nuclear functions and subcellular trafficking mechanisms of the epidermal growth factor receptor family. Cell Biosci. 2012, 2, 13. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.L.; Fang, C.L.; Tzeng, Y.T.; Hsu, H.L.; Lin, S.E.; Yu, M.C.; Bai, K.J.; Wang, L.S.; Liu, H.E. Prognostic value of localization of epidermal growth factor receptor in lung adenocarcinoma. J. Biomed. Sci. 2018, 25, 53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ilahi, N.E.; Bhatti, A. Impact of HPV E5 on viral life cycle via EGFR signaling. Microb. Pathog. 2020, 139, 103923. [Google Scholar] [CrossRef] [PubMed]
- Akerman, G.S.; Tolleson, W.H.; Brown, K.L.; Zyzak, L.L.; Mourateva, E.; Engin, T.S.; Basaraba, A.; Coker, A.L.; Creek, K.E.; Pirisi, L. Human papillomavirus type 16 E6 and E7 cooperate to increase epidermal growth factor receptor (EGFR) mRNA levels, overcoming mechanisms by which excessive EGFR signaling shortens the life span of normal human keratinocytes. Cancer Res. 2001, 61, 3837–3843. [Google Scholar]
- Hochmann, J.; Parietti, F.; Martinez, J.; Lopez, A.C.; Carreno, M.; Quijano, C.; Boccardo, E.; Sichero, L.; Moller, M.N.; Mirazo, S.; et al. Human papillomavirus type 18 E5 oncoprotein cooperates with E6 and E7 in promoting cell viability and invasion and in modulating the cellular redox state. Mem. Inst. Oswaldo Cruz 2020, 115, e190405. [Google Scholar] [CrossRef] [PubMed]
- Werness, B.A.; Levine, A.J.; Howley, P.M. Association of human papillomavirus types 16 and 18 E6 proteins with p53. Science 1990, 248, 76–79. [Google Scholar] [CrossRef] [PubMed]
- Dyson, N.; Howley, P.M.; Munger, K.; Harlow, E. The human papilloma virus-16 E7 oncoprotein is able to bind to the retinoblastoma gene product. Science 1989, 243, 934–937. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Acosta, P.; Romero-Rojas, A.; Vial, N.; Huertas, A.; Acosta, J.; Mayorga, D.; Carrillo, S.; Molano, M.; Gamboa, O.; Cotes, M.; et al. Persistent High-Risk HPV Infection and Molecular Changes Related to the Development of Cervical Cancer. Case Rep. Obstet. Gynecol. 2020, 2020, 6806857. [Google Scholar] [CrossRef] [PubMed]
- Zhai, Q.L.; Hu, X.D.; Xiao, J.; Yu, D.Q. [Astragalus polysaccharide may increase sensitivity of cervical cancer HeLa cells to cisplatin by regulating cell autophagy]. Zhongguo Zhong Yao Za Zhi 2018, 43, 805–812. [Google Scholar] [CrossRef]
- Doorbar, J. The E4 protein; structure, function and patterns of expression. Virology 2013, 445, 80–98. [Google Scholar] [CrossRef] [Green Version]
- Yajid, A.I.; Zakariah, M.A.; Mat Zin, A.A.; Othman, N.H. Potential Role of E4 Protein in Human Papillomavirus Screening: A Review. Asian Pac. J. Cancer Prev. 2017, 18, 315–319. [Google Scholar] [CrossRef]
- Klein, M.; Vignaud, J.M.; Hennequin, V.; Toussaint, B.; Bresler, L.; Plenat, F.; Leclere, J.; Duprez, A.; Weryha, G. Increased expression of the vascular endothelial growth factor is a pejorative prognosis marker in papillary thyroid carcinoma. J. Clin. Endocrinol. Metab. 2001, 86, 656–658. [Google Scholar] [CrossRef] [PubMed]
- Fedchenko, N.; Reifenrath, J. Different approaches for interpretation and reporting of immunohistochemistry analysis results in the bone tissue—A review. Diagn. Pathol. 2014, 9, 221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doeberitz, M.V.; Gissmann, L.; Hausen, H.Z. Growth-Regulating Functions of Human Papillomavirus Early Gene-Products in Cervical-Cancer Cells Acting Dominant over Enhanced Epidermal Growth-Factor Receptor Expression. Cancer Res. 1990, 50, 3730–3736. [Google Scholar]
- Crusius, K.; Auvinen, E.; Steuer, B.; Gaissert, H.; Alonso, A. The human papillomavirus type 16 E5-protein modulates ligand-dependent activation of the EGF receptor family in the human epithelial cell line HaCaT. Exp. Cell Res. 1998, 241, 76–83. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.M.; Chou, C.Y.; Hsu, Y.C.; Chen, M.J.; Wing, L.Y.C. The role of human papillomavirus type 16 E6/E7 oncoproteins in cervical epithelial-mesenchymal transition and carcinogenesis. Oncol. Lett. 2012, 3, 667–671. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spangle, J.M.; Munger, K. The HPV16 E6 Oncoprotein Causes Prolonged Receptor Protein Tyrosine Kinase Signaling and Enhances Internalization of Phosphorylated Receptor Species. PLoS Pathog. 2013, 9, e1003237. [Google Scholar] [CrossRef] [Green Version]
- Mathur, S.P.; Mathur, R.S.; Rust, P.F.; Young, R.C. Human papilloma virus (HPV)-E6/E7 and epidermal growth factor receptor (EGF-R) protein levels in cervical cancer and cervical intraepithelial neoplasia (CIN). Am. J. Reprod. Immunol. 2001, 46, 280–287. [Google Scholar] [CrossRef]
- Antonioli, M.; Pagni, B.; Vescovo, T.; Ellis, R.; Cosway, B.; Rollo, F.; Bordoni, V.; Agrati, C.; Labus, M.; Covello, R.; et al. HPV sensitizes OPSCC cells to cisplatin-induced apoptosis by inhibiting autophagy through E7-mediated degradation of AMBRA1. Autophagy 2021, 17, 2842–2855. [Google Scholar] [CrossRef]
- Banerjee, N.S.; Moore, D.; Parker, C.J.; Broker, T.R.; Chow, L.T. Targeting DNA Damage Response as a Strategy to Treat HPV Infections. Int. J. Mol. Sci. 2019, 20, 5455. [Google Scholar] [CrossRef] [Green Version]
- Liccardi, G.; Hartley, J.A.; Hochhauser, D. EGFR nuclear translocation modulates DNA repair following cisplatin and ionizing radiation treatment. Cancer Res. 2011, 71, 1103–1114. [Google Scholar] [CrossRef] [Green Version]
- Kontic, M.; Colovic, Z.; Paladin, I.; Gabelica, M.; Baric, A.; Pesutic-Pisac, V. Association between EGFR expression and clinical outcome of laryngeal HPV squamous cell carcinoma. Acta Otolaryngol. 2019, 139, 913–917. [Google Scholar] [CrossRef] [PubMed]
- Romanitan, M.; Nasman, A.; Munck-Wikland, E.; Dalianis, T.; Ramqvist, T. EGFR and Phosphorylated EGFR in Relation to HPV and Clinical Outcome in Tonsillar Cancer. Anticancer. Res. 2013, 33, 1575–1583. [Google Scholar] [PubMed]
- Alsbeih, G.; Al-Harbi, N.; Bin Judia, S.; Al-Qahtani, W.; Khoja, H.; El-Sebaie, M.; Tulbah, A. Prevalence of Human Papillomavirus (HPV) Infection and the Association with Survival in Saudi Patients with Head and Neck Squamous Cell Carcinoma. Cancers 2019, 11, 820. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whitmarsh, A.; Pring, M.; Thomas, S.J.; Waylen, A.; Ness, A.R.; Dudding, T.; Pawlita, M.; Brenner, N.; Waterboer, T.; Schroeder, L. Survival advantage in patients with human papillomavirus-driven oropharyngeal cancer and variation by demographic characteristics and serologic response: Findings from Head and Neck 5000. Cancer 2021, 127, 2442–2452. [Google Scholar] [CrossRef]
- Theocharis, S.; Giaginis, C.; Dana, E.; Thymara, I.; Rodriguez, J.; Patsouris, E.; Klijanienko, J. Phosphorylated Epidermal Growth Factor Receptor Expression Is Associated With Clinicopathologic Parameters and Patient Survival in Mobile Tongue Squamous Cell Carcinoma. J. Oral. Maxillofac. Surg. 2017, 75, 632–640. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | HPV 16E6/18E6 Expression | p-Value | ||
|---|---|---|---|---|
| Low | High | |||
| Nuclear EGFR | Low | 121 (79.1) a | 42 (46.7) | <0.0001 * |
| High | 32 (20.9) | 48 (53.3) | ||
| Membranous EGFR | Low | 106 (69.3) | 35 (38.9) | <0.0001 * |
| High | 47 (30.7) | 55 (61.1) | ||
| Characteristics | E6−tEGFR− (N = 58) | E6+tEGFR− or E6−tEGFR+ (N = 67) | E6+tEGFR+ (N = 48) | p-Value |
|---|---|---|---|---|
| Age (median = 71 yr) | 0.984 | |||
| Younger | 28 (48.28) a | 33 (49.25) | 24 (50.00) | |
| Older > 70 yr | 30 (51.72) | 34 (50.75) | 24 (50.00) | |
| Gender | 0.811 | |||
| Female | 35 (60.34) | 39 (58.21) | 26 (54.17) | |
| Male | 23 (39.66) | 28 (41.79) | 22 (45.83) | |
| Smoking | 0.767 | |||
| Never | 39 (67.24) | 43 (64.18) | 29 (60.42) | |
| Current or past | 19 (32.76) | 24 (35.82) | 19 (39.58) | |
| Tumor stage (2 missing) | 0.239 | |||
| T1/T2 | 24 (42.10) | 37 (56.06) | 21 (43.75) | |
| T3/T4 | 33 (57.90) | 29 (43.94) | 27 (56.25) | |
| Nodal stage (1 missing) | 0.039 | |||
| L0/L1 | 16 (27.59) | 30 (45.45) b | 24 (50.00) c | |
| L2/L3 | 42 (72.41) | 36 (54.55) | 24 (50.00) | |
| Metastasis | 0.155 | |||
| without | 18 (31.03) | 30 (44.78) | 23 (47.92) | |
| with | 40 (68.97) | 37 (55.22) | 25 (52.08) | |
| TNM stage | 0.084 | |||
| Localized (stage I/II) | 11 (18.97) | 16 (23.88) d | 18 (37.50) e | |
| Distant (stage III/IV) | 47 (81.03) | 51 (76.12) | 30 (62.50) | |
| Brain metastasis | 0.191 | |||
| without | 45 (77.59) | 42 (62.69) | 34 (70.83) | |
| with | 13 (22.41) | 25 (37.31) | 14 (29.17) | |
| EGFR mutations f (20 missing) | 0.362 | |||
| Wildtype | 29 (54.72) | 32 (54.24) | 17 (41.46) | |
| Mutationse | 24 (45.28) | 27 (45.76) | 24 (58.53) |
| Parameters | No | Median (m) | HR (95% CI) | p-Value |
|---|---|---|---|---|
| Total | ||||
| E6+/tEGFR+ | 36 | 31.4 | 0.58 (0.32–1.04) | 0.066 |
| E6−tEGFR− | 20 | 20.8 | 1 | |
| Older patients | ||||
| E6+/tEGFR+ | 18 | 31.7 | 0.35 (0.13–0.96) | 0.042 * |
| E6−tEGFR− | 8 | 16.1 | 1 | |
| No brain metastasis | ||||
| E6+/tEGFR+ | 20 | 57.2 | 0.42 (0.19–0.91) | 0.028 * |
| E6−tEGFR− | 14 | 20.8 | 1 | |
| Smokers | ||||
| E6+/tEGFR+ | 12 | 44.9 | 0.27 (0.09–0.84) | 0.024 * |
| E6−tEGFR− | 6 | 17.7 | 1 | |
| Wildtype EGFR | ||||
| E6+/tEGFR+ | 12 | 29.0 | 0.38 (0.15–0.96) | 0.041 * |
| E6−tEGFR− | 9 | 18.0 | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, J.-L.; Lee, W.-J.; Fang, C.-L.; Hsu, H.-L.; Chen, B.-J.; Liu, H.-E. Human Papillomavirus Oncoproteins Confer Sensitivity to Cisplatin by Interfering with Epidermal Growth Factor Receptor Nuclear Trafficking Related to More Favorable Clinical Survival Outcomes in Non-Small Cell Lung Cancer. Cancers 2022, 14, 5333. https://doi.org/10.3390/cancers14215333
Wang J-L, Lee W-J, Fang C-L, Hsu H-L, Chen B-J, Liu H-E. Human Papillomavirus Oncoproteins Confer Sensitivity to Cisplatin by Interfering with Epidermal Growth Factor Receptor Nuclear Trafficking Related to More Favorable Clinical Survival Outcomes in Non-Small Cell Lung Cancer. Cancers. 2022; 14(21):5333. https://doi.org/10.3390/cancers14215333
Chicago/Turabian StyleWang, Jinn-Li, Wei-Jiunn Lee, Chia-Lang Fang, Han-Lin Hsu, Bo-Jung Chen, and Hsingjin-Eugene Liu. 2022. "Human Papillomavirus Oncoproteins Confer Sensitivity to Cisplatin by Interfering with Epidermal Growth Factor Receptor Nuclear Trafficking Related to More Favorable Clinical Survival Outcomes in Non-Small Cell Lung Cancer" Cancers 14, no. 21: 5333. https://doi.org/10.3390/cancers14215333