
Individualized Decision Making in Transperineal Prostate Biopsy: Should All Men Undergo an Additional Systematic Biopsy?

 ,
,  ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Patients and Methods
2.1. Study Population
2.2. MR Imaging, Biopsy Procedure and Histopathological Analysis
2.3. Data collection and Statistical Analysis
3. Results
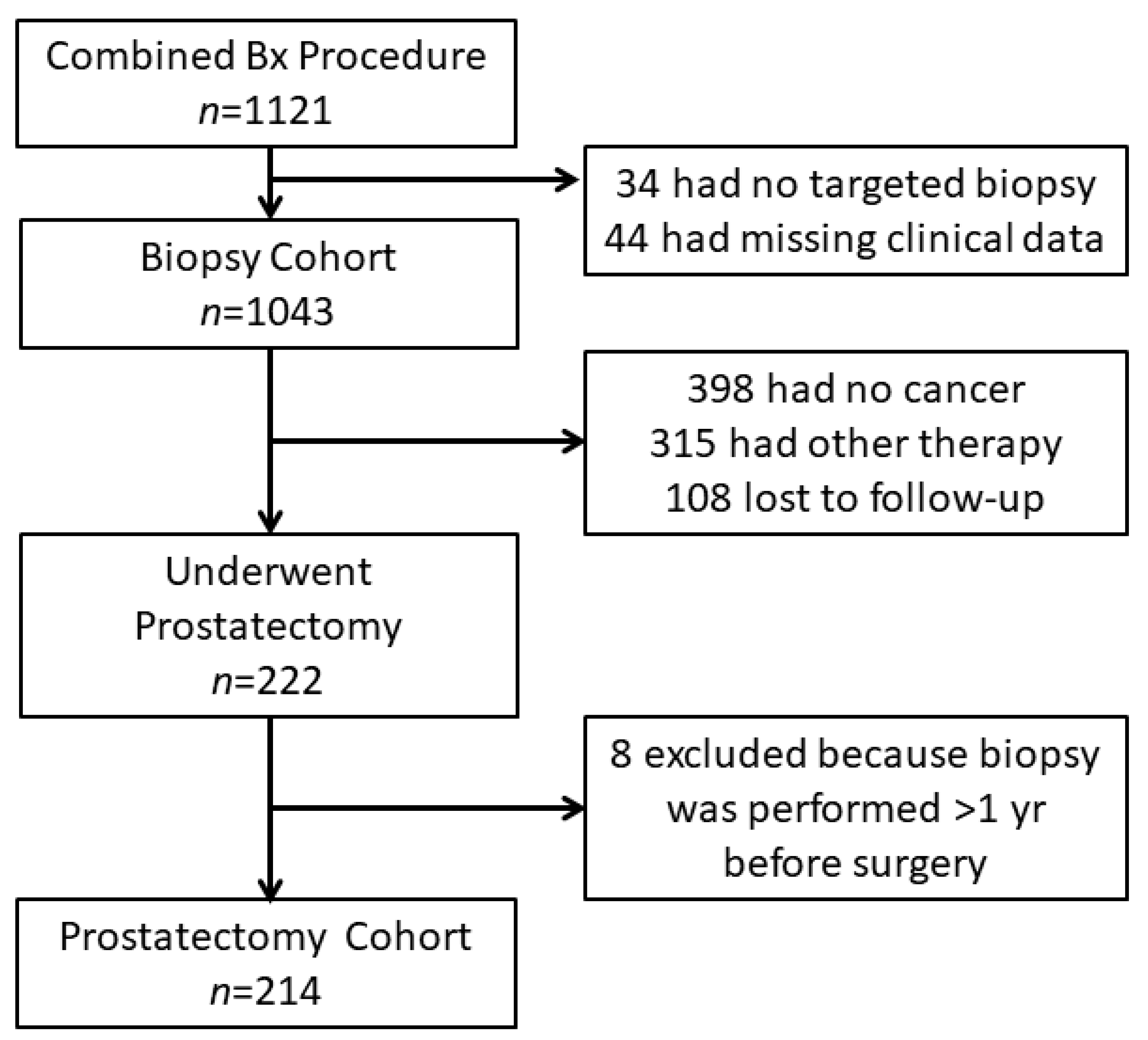
3.1. Study Cohort
3.2. Baseline Characteristics
3.3. Cancer Detection Rates and Upgrading in Systematic Versus MRI–Targeted Biopsy
3.4. Regression Analysis for the Upgrading to sPC by Systematic Biopsy
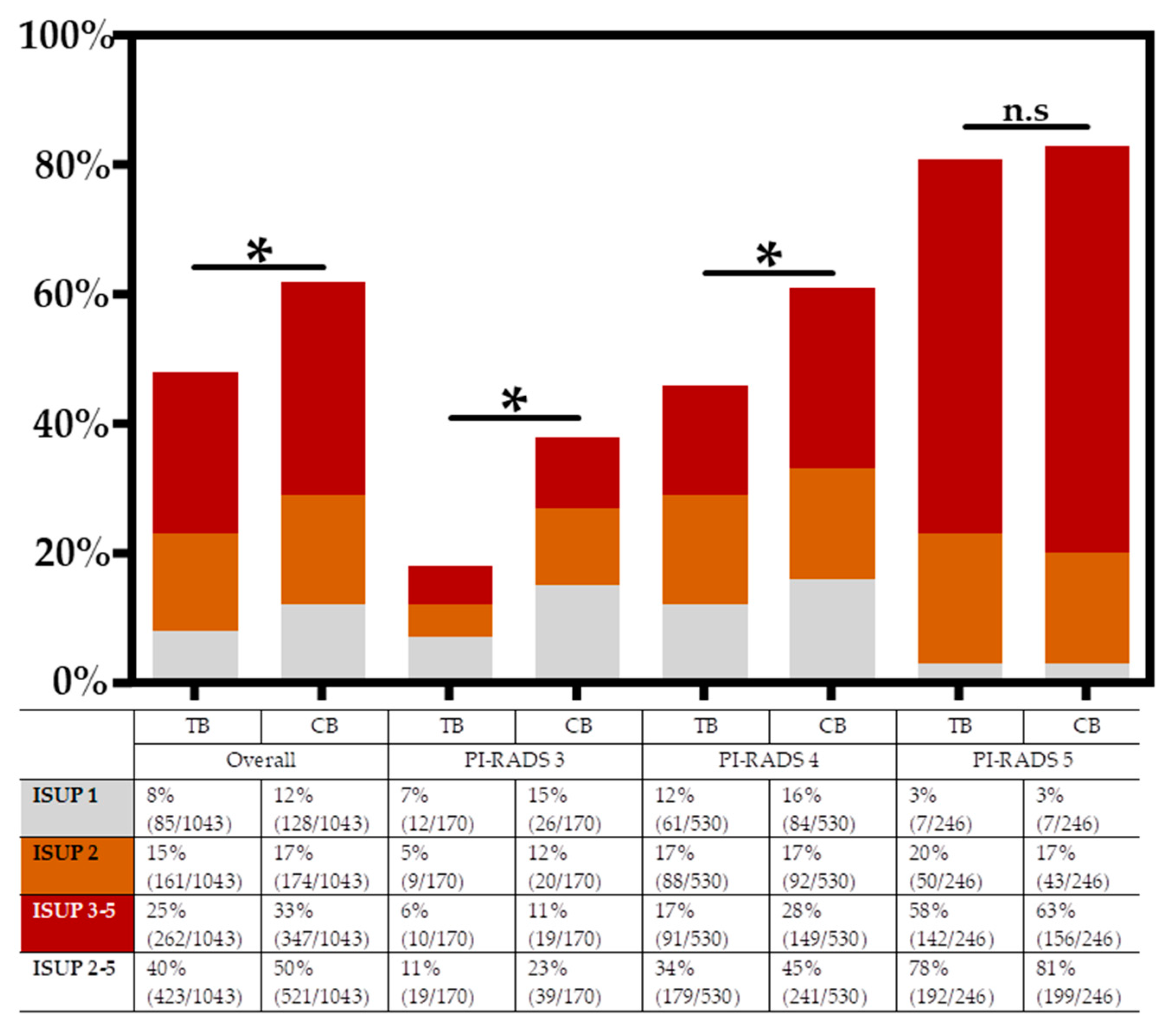
3.5. Cancer Detection Rates Stratified by PI-RADS Score
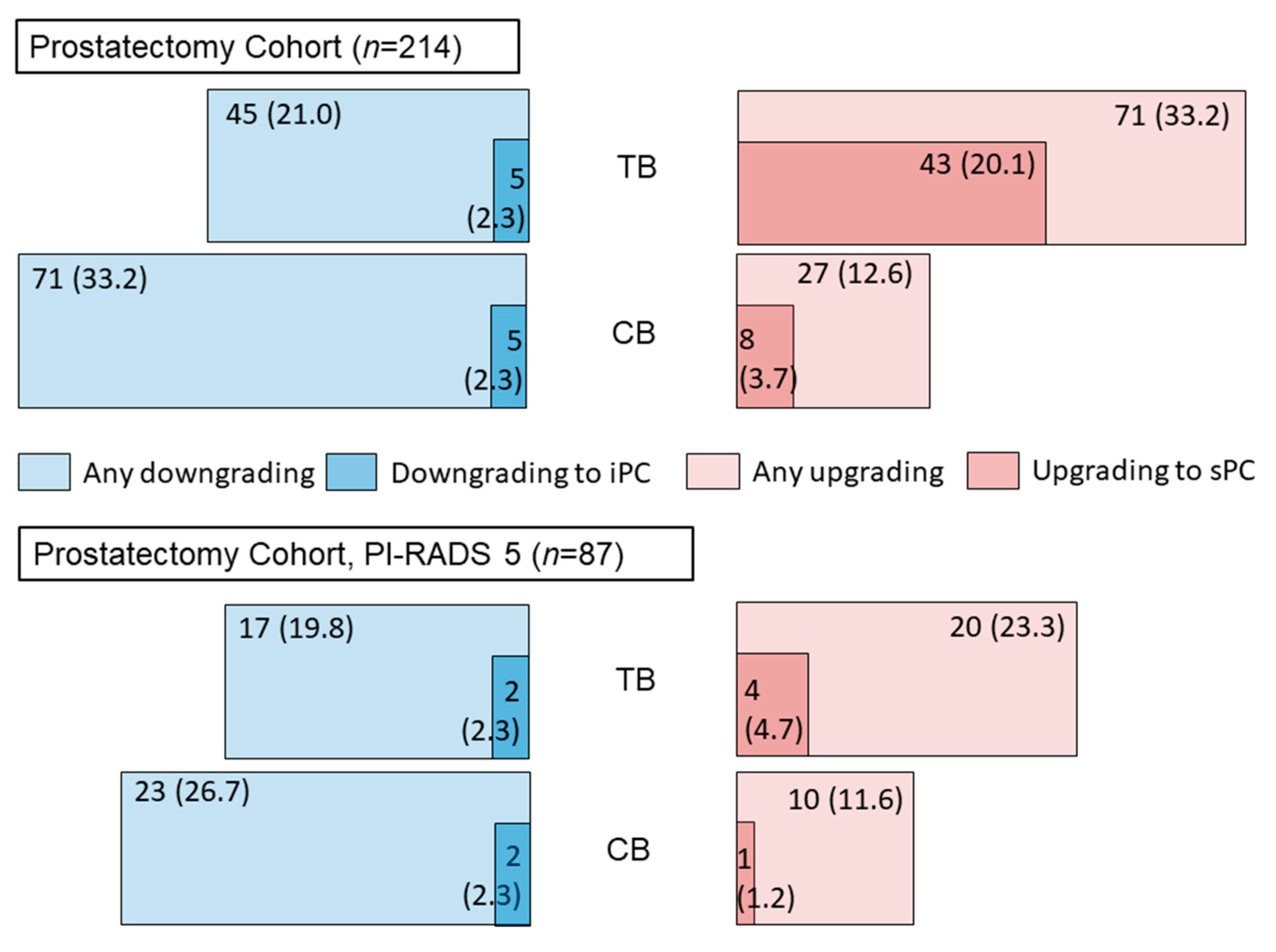
3.6. Reclassification in Subsequent Radical Prostatectomy
4. Discussion
4.1. Frequency of Upgrading to sPC by Additional Systematic Biopsy
4.2. Predictors for Upgrading to sPC
4.3. Stratification of Cancer Detection Rates by Patient’s PI-RADS Scores
4.4. Reclassification in Subsequent Radical Prostatectomy
4.5. Limitations and Strengths of the Study
4.6. Individualized Decision-Making
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ahmed, H.U.; El-Shater Bosaily, A.; Brown, L.C.; Gabe, R.; Kaplan, R.; Parmar, M.K.; Collaco-Moraes, Y.; Ward, K.; Hindley, R.G.; Freeman, A.; et al. Diagnostic accuracy of multi-parametric mri and trus biopsy in prostate cancer (promis): A paired validating confirmatory study. Lancet 2017, 389, 815–822. [Google Scholar] [CrossRef] [Green Version]
- Kasivisvanathan, V.; Rannikko, A.S.; Borghi, M.; Panebianco, V.; Mynderse, L.A.; Vaarala, M.H.; Briganti, A.; Budäus, L.; Hellawell, G.; Hindley, R.G.; et al. Mri-targeted or standard biopsy for prostate-cancer diagnosis. N. Engl. J. Med. 2018, 378, 1767–1777. [Google Scholar] [CrossRef] [PubMed]
- Rouvière, O.; Puech, P.; Renard-Penna, R.; Claudon, M.; Roy, C.; Mège-Lechevallier, F.; Decaussin-Petrucci, M.; Dubreuil-Chambardel, M.; Magaud, L.; Remontet, L.; et al. Use of prostate systematic and targeted biopsy on the basis of multiparametric mri in biopsy-naive patients (mri-first): A prospective, multicentre, paired diagnostic study. Lancet Oncol. 2019, 20, 100–109. [Google Scholar] [CrossRef]
- Muthigi, A.; George, A.K.; Sidana, A.; Kongnyuy, M.; Simon, R.; Moreno, V.; Merino, M.J.; Choyke, P.L.; Turkbey, B.; Wood, B.J.; et al. Missing the mark: Prostate cancer upgrading by systematic biopsy over magnetic resonance imaging/transrectal ultrasound fusion biopsy. J. Urol. 2017, 197, 327–334. [Google Scholar] [CrossRef] [PubMed]
- Kasivisvanathan, V.; Stabile, A.; Neves, J.B.; Giganti, F.; Valerio, M.; Shanmugabavan, Y.; Clement, K.D.; Sarkar, D.; Philippou, Y.; Thurtle, D.; et al. Magnetic resonance imaging-targeted biopsy versus systematic biopsy in the detection of prostate cancer: A systematic review and meta-analysis. Eur. Urol. 2019, 76, 284–303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kohl, T.; Sigle, A.; Kuru, T.; Salem, J.; Rolfs, H.; Kowalke, T.; Suarez-Ibarrola, R.; Michaelis, J.; Binder, N.; Jilg, C.A.; et al. Comprehensive analysis of complications after transperineal prostate biopsy without antibiotic prophylaxis: Results of a multicenter trial with 30 days’ follow-up. Prostate Cancer Prostatic Dis. 2022, 25, 264–268. [Google Scholar] [CrossRef] [PubMed]
- Deniffel, D.; Perlis, N.; Ghai, S.; Girgis, S.; Healy, G.M.; Fleshner, N.; Hamilton, R.; Kulkarni, G.; Toi, A.; van der Kwast, T.; et al. Prostate biopsy in the era of mri-targeting: Towards a judicious use of additional systematic biopsy. Eur. Radiol. 2022. [Google Scholar] [CrossRef] [PubMed]
- Sathianathen, N.J.; Warlick, C.A.; Weight, C.J.; Ordonez, M.A.; Spilseth, B.; Metzger, G.J.; Murugan, P.; Konety, B.R. A clinical prediction tool to determine the need for concurrent systematic sampling at the time of magnetic resonance imaging-guided biopsy. BJU Int. 2019, 123, 612–617. [Google Scholar] [CrossRef] [PubMed]
- Coker, M.A.; Glaser, Z.A.; Gordetsky, J.B.; Thomas, J.V.; Rais-Bahrami, S. Targets missed: Predictors of mri-targeted biopsy failing to accurately localize prostate cancer found on systematic biopsy. Prostate Cancer Prostatic Dis. 2018, 21, 549–555. [Google Scholar] [CrossRef] [PubMed]
- Ahdoot, M.; Lebastchi, A.H.; Long, L.; Wilbur, A.R.; Gomella, P.T.; Mehralivand, S.; Daneshvar, M.A.; Yerram, N.K.; O’Connor, L.P.; Wang, A.Z.; et al. Using prostate imaging-reporting and data system (pi-rads) scores to select an optimal prostate biopsy method: A secondary analysis of the trio study. Eur. Urol. Oncol. 2022, 5, 176–186. [Google Scholar] [CrossRef] [PubMed]
- Mottet, N.P.C.; van den Bergh, R.C.N.; Briers, E.; Gillessen, M.D.S.S.; Grummet, J.; van der Kwast, A.M.H.T.H.; Lam, T.B.; Mason, M.D.S.O.H.; Oprea-Lager, D.E.; Ploussard, G.; et al. EAU-EANM-ESTRO-ESUR-SIOG Guidelines on Prostate Cancer—2020. Eur. Assoc. Urol. 2020, 1, 11–143. [Google Scholar]
- Turkbey, B.; Rosenkrantz, A.B.; Haider, M.A.; Padhani, A.R.; Villeirs, G.; Macura, K.J.; Tempany, C.M.; Choyke, P.L.; Cornud, F.; Margolis, D.J.; et al. Prostate imaging reporting and data system version 2.1: 2019 Update of prostate imaging reporting and data system version 2. Eur. Urol. 2019, 76, 340–351. [Google Scholar] [CrossRef] [PubMed]
- Kuru, T.H.; Wadhwa, K.; Chang, R.T.M.; Echeverria, L.M.C.; Roethke, M.; Polson, A.; Rottenberg, G.; Koo, B.; Lawrence, E.M.; Seidenader, J.; et al. Definitions of terms, processes and a minimum dataset for transperineal prostate biopsies: A standardization approach of the ginsburg study group for enhanced prostate diagnostics: A standardization approach for transperineal prostate biopsies. BJU Int. 2013, 112, 568–577. [Google Scholar] [CrossRef] [PubMed]
- Kroenig, M.; Schaal, K.; Benndorf, M.; Soschynski, M.; Lenz, P.; Krauss, T.; Drendel, V.; Kayser, G.; Kurz, P.; Werner, M.; et al. Diagnostic accuracy of robot-guided, software based transperineal mri/trus fusion biopsy of the prostate in a high risk population of previously biopsy negative men. BioMed Res. Int. 2016, 2016, 2384894. [Google Scholar] [CrossRef] [PubMed]
- Epstein, J.I.; Allsbrook, W.C., Jr.; Amin, M.B.; Egevad, L.L.; Committee, I.G. The 2005 international society of urological pathology (isup) consensus conference on gleason grading of prostatic carcinoma. Am. J. Surg. Pathol. 2005, 29, 1228–1242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Connor, M.J.; Eldred-Evans, D.; van Son, M.; Hosking-Jervis, F.; Bertoncelli Tanaka, M.; Reddy, D.; Bass, E.J.; Powell, L.; Ahmad, S.; Pegers, E.; et al. A multicenter study of the clinical utility of nontargeted systematic transperineal prostate biopsies in patients undergoing pre-biopsy multiparametric magnetic resonance imaging. J. Urol. 2020, 204, 1195–1201. [Google Scholar] [CrossRef] [PubMed]
- Ahdoot, M.; Wilbur, A.R.; Reese, S.E.; Lebastchi, A.H.; Mehralivand, S.; Gomella, P.T.; Bloom, J.; Gurram, S.; Siddiqui, M.; Pinsky, P.; et al. Mri-targeted, systematic, and combined biopsy for prostate cancer diagnosis. N. Engl. J. Med. 2020, 382, 917–928. [Google Scholar] [CrossRef] [PubMed]
- Nakanishi, Y.; Ito, M.; Fukushima, H.; Yokoyama, M.; Kataoka, M.; Ikuta, S.; Sakamoto, K.; Takemura, K.; Suzuki, H.; Tobisu, K.I.; et al. Who can avoid systematic biopsy without missing clinically significant prostate cancer in men who undergo magnetic resonance imaging-targeted biopsy? Clin. Genitourin. Cancer 2019, 17, e664–e671. [Google Scholar] [CrossRef] [PubMed]
- Drobish, J.N.; Bevill, M.D.; Tracy, C.R.; Sexton, S.M.; Rajput, M.; Metz, C.M.; Gellhaus, P.T. Do patients with a pi-rads 5 lesion identified on magnetic resonance imaging require systematic biopsy in addition to targeted biopsy? Urol. Oncol. 2021, 39, e231–e234. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Gomez, E.; Moreno Sorribas, S.; Valero-Rosa, J.; Blanca, A.; Mesa, J.; Salguero, J.; Carrasco-Valiente, J.; Lopez-Ruiz, D.; Anglada-Curado, F.J. Does adding standard systematic biopsy to targeted prostate biopsy in pi-rads 3 to 5 lesions enhance the detection of clinically significant prostate cancer? Should all patients with pi-rads 3 undergo targeted biopsy? Diagnostics 2021, 11, 1335. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | All Men | Prostatectomy Cohort |
|---|---|---|
| Cases, n | 1043 | 214 |
| Age (years), median, IQR | 67.0 (61.0–72.0) | 67.0 (62.0–72.0) |
| Previous Negative Biopsy, n (%) | 244 (23.4) | 43 (20.1) |
| Active Surveillance, n (%) | 141 (13.5) | 29 (13.6) |
| PSA (ng/mL), median, IQR | 8.8 (6.0–12.6) | 9.3 (6.3–14.0) |
| Volume (mL), median, IQR | 53.0 (38.5–75.0) | 47.6 (37.0–63.3) |
| PI-RADS, n (%) | ||
| n/a | 54 (5.2) | 8 (3.7) |
| 1 | 0 (0.0) | 0 (0) |
| 2 | 43 (4.2) | 6 (2.8) |
| 3 | 170 (16.3) | 17 (7.9) |
| 4 | 530 (50.8) | 97 (43.5) |
| 5 | 246 (23.6) | 86 (40.2) |
| Target Localization, n (%) | ||
| Unilateral | 595 (57.0) | 116 (54.2) |
| Bilateral | 448 (43.0) | 98 (45.8) |
| Non-peripheral Zone | 221 (21.2) | 33 (15.4) |
| Peripheral Zone | 444 (42.6) | 103 (48.1) |
| Bi-zonal | 378 (36.2) | 78 (36.4) |
| Index Lesion Volume (mL), median, IQR | 0.58 (0.32–1.14) | 0.64 (0.30–1.52) |
| Number of Lesions, n (%) | ||
| 1 | 481 (46.1) | 104 (48.6) |
| 2 | 394 (37.8) | 80 (37.4) |
| 3 | 136 (13.0) | 24 (11.2) |
| 4 or more | 32 (3.1) | 6 (2.8) |
| Number of Cores, median, IQR | ||
| Total | 35 (31–40) | 34 (30–39) |
| From Target | 5 (3–7) | 4 (4–7) |
| Systematic | 31 (26–34) | 30 (25–32) |
| Cancer Grading according to ISUP, n (%) | ||
| No Cancer | 394 (37.8) | n/a |
| 1 | 128 (12.3) | 8 (3.7) |
| 2 | 174 (16.7) | 71 (33.2) |
| 3 | 142 (13.6) | 82 (38.3) |
| 4 | 162 (15.5) | 26 (12.1) |
| 5 | 43 (4.1) | 27 (12.6) |
| Upgrading to sPC (ISUP2-5) by Systematic Biopsy | ||||
|---|---|---|---|---|
| Univariate Analysis | Multivariate Analysis | |||
| OR (95% CI) | p | OR (95% CI) | p | |
| Age, years | 1.00 (0.97–1.03) | 0.90 | ||
| Previous Negative Biopsy | ||||
| ≥1 vs. none | 0.94 (0.58–1.52) | 0.78 | ||
| Active Surveillance | ||||
| Yes vs. No | 0.86 (0.44–1.66) | 0.65 | ||
| PSA level, ng/mL | 0.99 (0.94–1.04) | 0.72 | ||
| Prostate volume, mL | 0.99 (0.98–1.00) | 0.18 | 0.99 (0.98–1.00) | <0.03 * |
| PI-RADS Score | ||||
| PI-RADS 5 | Ref. | Ref. | ||
| PI-RADS 4 vs. | 3.70 (1.66–8.28) | <0.01 ** | 4.62 (2.08–10.28) | <0.01 ** |
| PI-RADS 3 vs. | 4.43 (1.82–10.79) | <0.01 ** | 5.54 (2.26–13.57) | <0.01 ** |
| PI-RADS 2 vs. | 5.73 (1.80–18.26) | <0.01 ** | 7.37 (2.41–22.53) | <0.01 ** |
| Target Localization | ||||
| Unilateral vs. Bilateral | 0.99 (0.64–1.54) | 0.97 | ||
| Non-peripheral Zone vs. Peripheral Zone | 0.44 (0.23–0.85) | <0.01 ** | 0.42 (0.22–0.81) | <0.01 ** |
| Bizonal vs. Peripheral Zone | 0.55 (0.33–0.90) | 0.02 * | 0.70 (0.44–1.20) | 0.14 |
| Index Lesion Volume | ||||
| <0.6 mL vs. ≥ 0.6 mL | 2.15 (1.38–3.34) | <0.01 ** | ||
| Number of lesions (n) | ||||
| 1 vs. >1 | 0.99 (0.64–1.43) | 0.97 | ||
| Number of Target Cores (n) | 0.98 (0.89–1.07) | 0.61 | ||
| Number of Systematic Cores (n) | 1.03 (0.99–1.07) | 0.11 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sigle, A.; Suarez-Ibarrola, R.; Benndorf, M.; Weishaar, M.; Morlock, J.; Miernik, A.; Gratzke, C.; Jilg, C.A.; Grabbert, M. Individualized Decision Making in Transperineal Prostate Biopsy: Should All Men Undergo an Additional Systematic Biopsy? Cancers 2022, 14, 5230. https://doi.org/10.3390/cancers14215230
Sigle A, Suarez-Ibarrola R, Benndorf M, Weishaar M, Morlock J, Miernik A, Gratzke C, Jilg CA, Grabbert M. Individualized Decision Making in Transperineal Prostate Biopsy: Should All Men Undergo an Additional Systematic Biopsy? Cancers. 2022; 14(21):5230. https://doi.org/10.3390/cancers14215230
Chicago/Turabian StyleSigle, August, Rodrigo Suarez-Ibarrola, Matthias Benndorf, Moritz Weishaar, Jonathan Morlock, Arkadiusz Miernik, Christian Gratzke, Cordula A. Jilg, and Markus Grabbert. 2022. "Individualized Decision Making in Transperineal Prostate Biopsy: Should All Men Undergo an Additional Systematic Biopsy?" Cancers 14, no. 21: 5230. https://doi.org/10.3390/cancers14215230