
Low-Dose Computed Tomography Scanning Protocols for Online Adaptive Proton Therapy of Head-and-Neck Cancers
 , , , ,
, , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Cohort and Treatment Planning
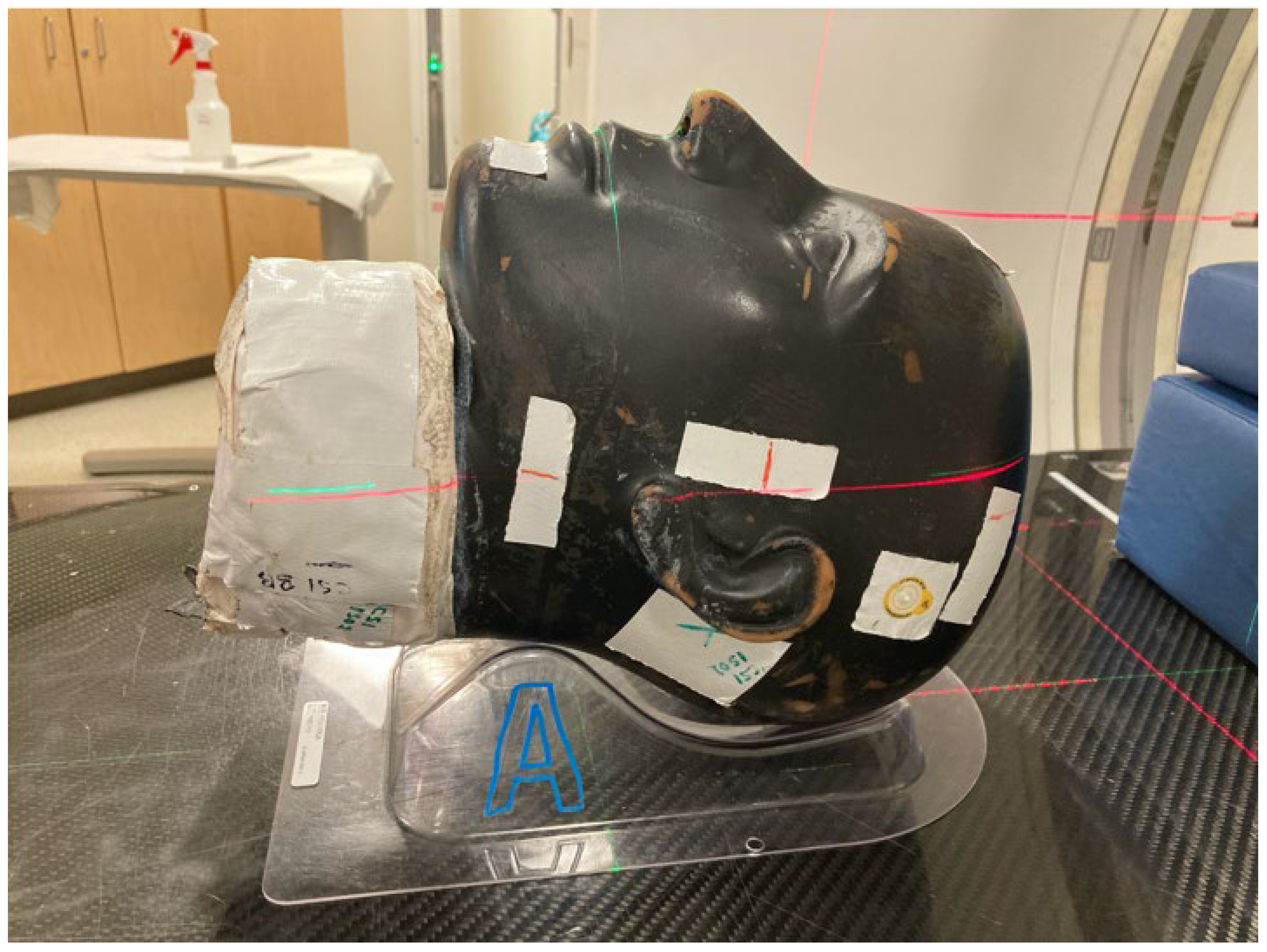
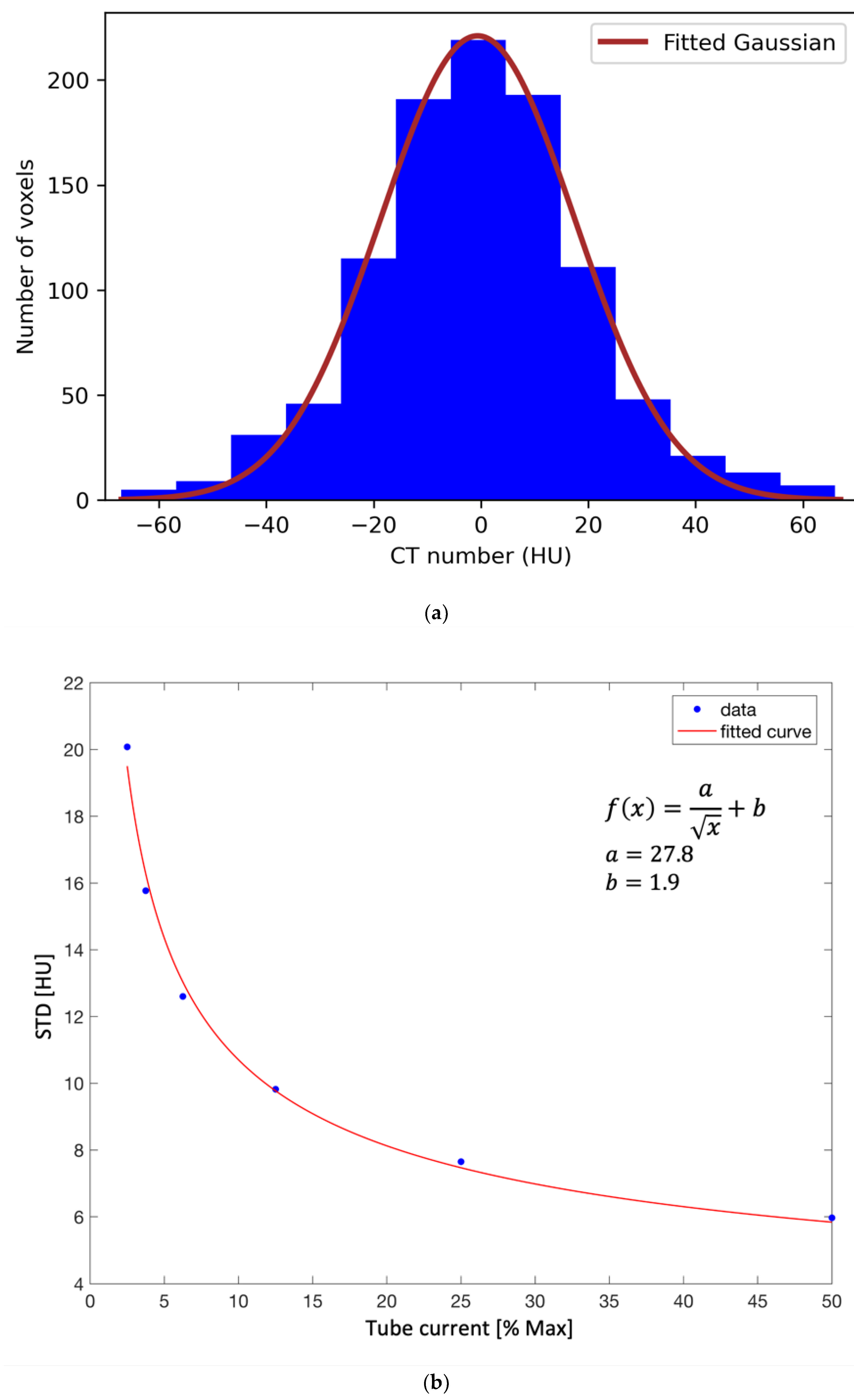
2.2. Phantom Measurements and Low-Dose CT Scanning Protocols
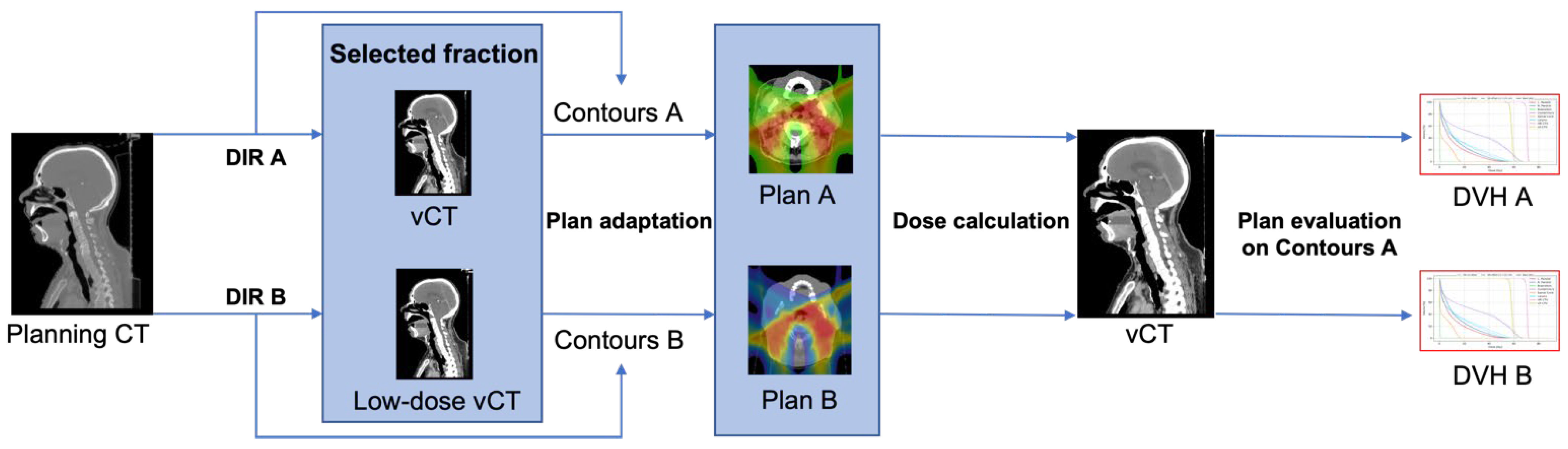
2.3. Influence of Low-Dose Scanning Protocols on Online Adaptive Treatments
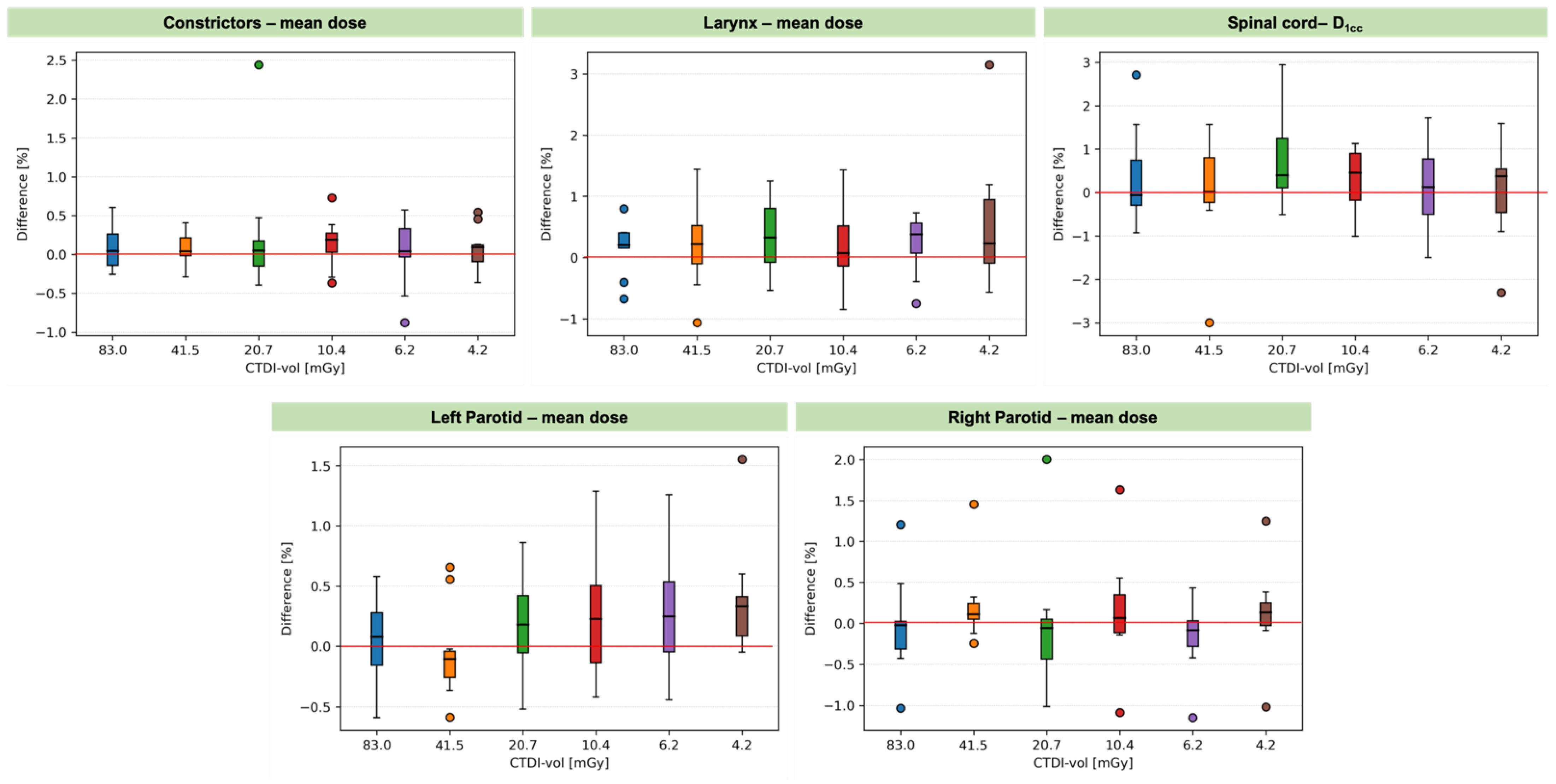
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Paganetti, H.; Botas, P.; Sharp, G.C.; Winey, B. Adaptive proton therapy. Phys. Med. Biol. 2021, 66, 22TR01. [Google Scholar] [CrossRef] [PubMed]
- Kurz, C.; Nijhuis, R.; Reiner, M.; Ganswindt, U.; Thieke, C.; Belka, C.; Parodi, K.; Landry, G. Feasibility of automated proton therapy plan adaptation for head and neck tumors using cone beam CT images. Radiat. Oncol. 2016, 11, 64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bernatowicz, K.; Geets, X.; Barragan, A.; Janssens, G.; Souris, K.; Sterpin, E. Feasibility of online IMPT adaptation using fast, automatic and robust dose restoration. Phys. Med. Biol. 2018, 63, 085018. [Google Scholar] [CrossRef] [PubMed]
- Jagt, T.Z.; Breedveld, S.; van Haveren, R.; Nout, R.A.; Astreinidou, E.; Heijmen, B.J.M.; Hoogeman, M.S. Plan-library supported automated replanning for online-adaptive intensity-modulated proton therapy of cervical cancer. Acta Oncol. 2019, 58, 1440–1445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moriya, S.; Tachibana, H.; Hotta, K.; Nakamura, N.; Sakae, T.; Akimoto, T. Range optimization for target and organs at risk in dynamic adaptive passive scattering proton beam therapy—A proof of concept. Phys. Med. Eur. J. Med. Phys. 2018, 56, 66–73. [Google Scholar] [CrossRef] [PubMed]
- Nenoff, L.; Matter, M.; Hedlund Lindmar, J.; Weber, D.C.; Lomax, A.J.; Albertini, F. Daily adaptive proton therapy–the key to innovative planning approaches for paranasal cancer treatments. Acta Oncol. 2019, 58, 1423–1428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jagt, T.; Breedveld, S.; Van De Water, S.; Heijmen, B.; Hoogeman, M. Near real-time automated dose restoration in IMPT to compensate for daily tissue density variations in prostate cancer. Phys. Med. Biol. Phys. Med. Biol. 2017, 62, 4254–4272. [Google Scholar] [CrossRef] [PubMed]
- Bobić, M.; Lalonde, A.; Sharp, G.C.; Grassberger, C.; Verburg, J.M.; Winey, B.A.; Lomax, A.J.; Paganetti, H. Comparison of weekly and daily online adaptation for head and neck intensity-modulated proton therapy. Phys. Med. Biol. 2021, 66, 055023. [Google Scholar] [CrossRef] [PubMed]
- Botas, P.; Kim, J.; Winey, B.; Paganetti, H. Online adaption approaches for intensity modulated proton therapy for head and neck patients based on cone beam CTs and Monte Carlo simulations. Phys. Med. Biol. 2019, 64, 015004. [Google Scholar] [CrossRef] [PubMed]
- Matter, M.; Nenoff, L.; Meier, G.; Weber, D.C.; Lomax, A.J.; Albertini, F. Intensity modulated proton therapy plan generation in under ten seconds. Acta Oncol. 2019, 58, 1435–1439. [Google Scholar] [CrossRef] [PubMed]
- Jagt, T.; Breedveld, S.; Van Haveren, R.; Heijmen, B.; Hoogeman, M. An automated planning strategy for near real-time adaptive proton therapy in prostate cancer. Phys. Med. Biol. 2018, 63, 135017. [Google Scholar] [CrossRef] [PubMed]
- Rehani, M.M.; Melick, E.R.; Alvi, R.M.; Doda Khera, R.; Batool-Anwar, S.; Neilan, T.G.; Bettmann, M. Patients undergoing recurrent CT exams: Assessment of patients with non-malignant diseases, reasons for imaging and imaging appropriateness. Eur. Radiol. 2020, 30, 1839–1846. [Google Scholar] [CrossRef] [PubMed]
- Rühm, W.; Harrison, R.M. High CT doses return to the agenda. Radiat. Environ. Biophys. 2019, 59, 3–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hälg, R.A.; Besserer, J.; Schneider, U. Systematic measurements of whole-body imaging dose distributions in image-guided radiation therapy. Med. Phys. 2012, 39, 7650–7661. [Google Scholar] [CrossRef]
- Nesteruk, K.P.; Bobić, M.; Lalonde, A.; Winey, B.A.; Lomax, A.J.; Paganetti, H. Ct-on-rails versus in-room cbct for online daily adaptive proton therapy of head-and-neck cancers. Cancers 2021, 13, 5991. [Google Scholar] [CrossRef] [PubMed]
- Nenoff, L.; Matter, M.; Charmillot, M.; Krier, S.; Uher, K.; Weber, D.C.; Lomax, A.J.; Albertini, F. Experimental validation of daily adaptive proton therapy. Phys. Med. Biol. 2021, 66, 205010. [Google Scholar] [CrossRef] [PubMed]
- Elhamiasl, M.; Nuyts, J. Low-dose X-ray CT simulation from an available higher-dose scan. Phys. Med. Biol. 2020, 65, 135010. [Google Scholar] [CrossRef] [PubMed]
- Elhamiasl, M.; Salvo, K.; Poels, K.; Defraene, G.; Lambrecht, M.; Geets, X.; Sterpin, E.; Nuyts, J. Low-dose CT allows for accurate proton therapy dose calculation and plan optimization. Phys. Med. Biol. 2022, 67, 195015. [Google Scholar] [CrossRef]
- Lalonde, A.; Bobić, M.; Winey, B.; Verburg, J.; Sharp, G.C.; Paganetti, H. Anatomic changes in head and neck intensity-modulated proton therapy: Comparison between robust optimization and online adaptation. Radiother. Oncol. 2021, 159, 39–47. [Google Scholar] [CrossRef] [PubMed]
- Lowekamp, B.C.; Chen, D.T.; Ibáñez, L.; Blezek, D. The design of simpleITK. Front. Neuroinform. 2013, 7, 45. [Google Scholar] [CrossRef] [PubMed]
- Yaniv, Z.; Lowekamp, B.C.; Johnson, H.J.; Beare, R. SimpleITK Image-Analysis Notebooks: A Collaborative Environment for Education and Reproducible Research. J. Digit. Imaging 2018, 31, 290–303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beare, R.; Lowekamp, B.; Yaniv, Z. Image Segmentation, Registration and Characterization in R with SimpleITK. J. Stat. Softw. 2018, 86, 1–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mccormick, M.; Liu, X.; Jomier, J.; Marion, C.; Ibanez, L. Itk: Enabling reproducible research and open science. Front. Neuroinform. 2014, 8, 13. [Google Scholar] [CrossRef] [Green Version]
- Giantsoudi, D.; Schuemann, J.; Jia, X.; Dowdell, S.; Jiang, S.; Paganetti, H. Validation of a GPU-based Monte Carlo code (gPMC) for proton radiation therapy: Clinical cases study. Phys. Med. Biol. 2015, 60, 2257. [Google Scholar] [CrossRef] [PubMed]
- Qin, N.; Botas, P.; Giantsoudi, D.; Schuemann, J.; Tian, Z.; Jiang, S.B.; Paganetti, H.; Jia, X. Recent developments and comprehensive evaluations of a GPU-based Monte Carlo package for proton therapy. Phys. Med. Biol. 2016, 61, 7347. [Google Scholar] [CrossRef] [PubMed]
- Jia, X.; Schümann, J.; Paganetti, H.; Jiang, S.B. GPU-based fast Monte Carlo dose calculation for proton therapy. Phys. Med. Biol. 2012, 57, 7783. [Google Scholar] [CrossRef]
- Jia, X.; Gu, X.; Graves, Y.J.; Folkerts, M.; Jiang, S.B. GPU-based fast Monte Carlo simulation for radiotherapy dose calculation. Phys. Med. Biol. 2011, 56, 7017. [Google Scholar] [CrossRef]
- Lee, H.; Shin, J.; Verburg, J.M.; Bobić, M.; Winey, B.; Schuemann, J.; Paganetti, H. MOQUI: An open-source GPU-based Monte Carlo code for proton dose calculation with efficient data structure. Phys. Med. Biol. 2022, 67, 174001. [Google Scholar] [CrossRef]
- Shackleford, J.A.; Shusharina, N.; Verberg, J.; Warmerdam, G.; Winey, B.; Neuner, M.; Steininger, P.; Arbisser, A.; Golland, P.; Lou, Y.; et al. Plastimatch 1.6-Current Capabilities and Future Directions. Available online: https://www.researchgate.net/publication/234115614_Plastimatch_16_--_current_capabilities_and_future_directions (accessed on 14 October 2022).
- Shackleford, J.A.; Kandasamy, N.; Sharp, G.C. On developing B-spline registration algorithms for multi-core processors. Phys. Med. Biol. 2010, 55, 6329–6351. [Google Scholar] [CrossRef]
- Trofimov, A.; Rietzel, E.; Lu, H.-M.; Martin, B.; Jiang, S.; Chen, G.T.Y.; Bortfeld, T. Temporo-spatial IMRT optimization: Concepts, implementation and initial results. Phys. Med. Biol. 2005, 50, 2779. [Google Scholar] [CrossRef]
- Dice, L.R. Measures of the Amount of Ecologic Association Between Species. Ecology 1945, 26, 297–302. [Google Scholar] [CrossRef]
- Nash, D.; Juneja, S.; Palmer, A.L.; van Herk, M.; McWilliam, A.; Osorio, E.V. The geometric and dosimetric effect of algorithm choice on propagated contours from CT to cone beam CTs. Phys. Med. 2022, 100, 112–119. [Google Scholar] [CrossRef] [PubMed]
- Nenoff, L.; Matter, M.; Amaya, E.J.; Josipovic, M.; Knopf, A.C.; Lomax, A.J.; Persson, G.F.; Ribeiro, C.O.; Visser, S.; Walser, M.; et al. Dosimetric influence of deformable image registration uncertainties on propagated structures for online daily adaptive proton therapy of lung cancer patients. Radiother. Oncol. 2021, 159, 136–143. [Google Scholar] [CrossRef] [PubMed]
- Greffier, J.; Frandon, J.; Larbi, A.; Beregi, J.P.; Pereira, F. CT iterative reconstruction algorithms: A task-based image quality assessment. Eur. Radiol. 2019, 30, 487–500. [Google Scholar] [CrossRef] [PubMed]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Tube Current | CTDIvol | Tube Voltage | Pitch Factor | Slice Thickness |
|---|---|---|---|---|
| 400 mA (STD) | 166 mGy | 140 kV | 0.6 | 2.5 mm |
| 200 mA | 83 mGy | 140 kV | 0.6 | 2.5 mm |
| 100 mA | 41.5 mGy | 140 kV | 0.6 | 2.5 mm |
| 50 mA | 20.7 mGy | 140 kV | 0.6 | 2.5 mm |
| 25 mA | 10.4 mGy | 140 kV | 0.6 | 2.5 mm |
| 15 mA | 6.2 mGy | 140 kV | 0.6 | 2.5 mm |
| 10 mA | 4.2 mGy | 140 kV | 0.6 | 2.5 mm |
| ROI | DVH Metric | CTDIvol (mGy) | ||||||
|---|---|---|---|---|---|---|---|---|
| 166.0 | 83.0 | 41.5 | 20.7 | 10.4 | 6.2 | 4.2 | ||
| High-risk CTV | D98 (%) | 97.1 (94.5–98.5) | 97.1 (94.8–98.6) | 97.1 (94.6–98.5) | 97.1 (94.6–98.5) | 97.2 (94.9–98.5) | 97.2 (95.0–98.5) | 97.2 (94.7–98.5) |
| Low-risk CTV | D98 (%) | 97.3 (95.5–98.3) | 97.4 (95.5–98.5) | 97.4 (95.6–98.4) | 97.4 (95.6–98.3) | 97.5 (95.6–98.6) | 97.4 (95.6–98.6) | 97.5 (95.5–98.6) |
| Constrictors | Dmean (Gy) | 29.7 (7.0–61.2) | 29.7 (7.0–61.3) | 29.8 (7.0–61.2) | 29.7 (7.0–61.2) | 29.7 (7.0–61.3) | 29.8 (6.9–61.3) | 29.8 (7.0–61.1) |
| Right parotid | Dmean (Gy) | 19.2 (12.5–55.4) | 19.2 (12.4–55.4) | 19.2 (12.5–55.3) | 19.2 (12.5–55.3) | 19.2 (12.5–55.4) | 19.1 (12.5–55.4) | 19.2 (12.5–55.4) |
| Left parotid | Dmean (Gy) | 17.0 (9.9–52.4) | 17.0 (9.9–52.2) | 17.0 (10.0–52.4) | 17.0 (10.0–52.4) | 17.0 (10.0–52.5) | 17.0 (10.0–52.5) | 17.0 (10.0–52.4) |
| Larynx | Dmean (Gy) | 20.5 (6.3–34.8) | 20.6 (6.4–34.6) | 20.5 (6.4–34.6) | 20.5 (6.4–34.6) | 20.4 (6.4–34.6) | 20.4 (6.4–34.5) | 20.5 (6.5–34.6) |
| Spinal cord | D1cc (Gy) | 12.1 (8.7–23.2) | 12.4 (8.6–23.2) | 12.3 (8.4–23.2) | 12.2 (8.9–23.2) | 12.2 (8.6–23.1) | 12.2 (8.6–23.1) | 12.2 (8.5–23.1) |
| Beam | Mean (%) | Min–Max (%) |
|---|---|---|
| Posterior-Anterior | 99.99 | 99.96–100.00 |
| Left-Anterior | 99.98 | 99.94–100.00 |
| Right-Anterior | 99.98 | 99.93–100.00 |
| Combined | 99.99 | 99.96–100.00 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nesteruk, K.P.; Bobić, M.; Sharp, G.C.; Lalonde, A.; Winey, B.A.; Nenoff, L.; Lomax, A.J.; Paganetti, H. Low-Dose Computed Tomography Scanning Protocols for Online Adaptive Proton Therapy of Head-and-Neck Cancers. Cancers 2022, 14, 5155. https://doi.org/10.3390/cancers14205155
Nesteruk KP, Bobić M, Sharp GC, Lalonde A, Winey BA, Nenoff L, Lomax AJ, Paganetti H. Low-Dose Computed Tomography Scanning Protocols for Online Adaptive Proton Therapy of Head-and-Neck Cancers. Cancers. 2022; 14(20):5155. https://doi.org/10.3390/cancers14205155
Chicago/Turabian StyleNesteruk, Konrad P., Mislav Bobić, Gregory C. Sharp, Arthur Lalonde, Brian A. Winey, Lena Nenoff, Antony J. Lomax, and Harald Paganetti. 2022. "Low-Dose Computed Tomography Scanning Protocols for Online Adaptive Proton Therapy of Head-and-Neck Cancers" Cancers 14, no. 20: 5155. https://doi.org/10.3390/cancers14205155