
Longitudinal Body Composition Changes Detected by [18F]FDG PET/CT during and after Chemotherapy and Their Prognostic Role in Elderly Hodgkin Lymphoma
 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. [18F]FDG-PET/CT Protocol and Evaluation
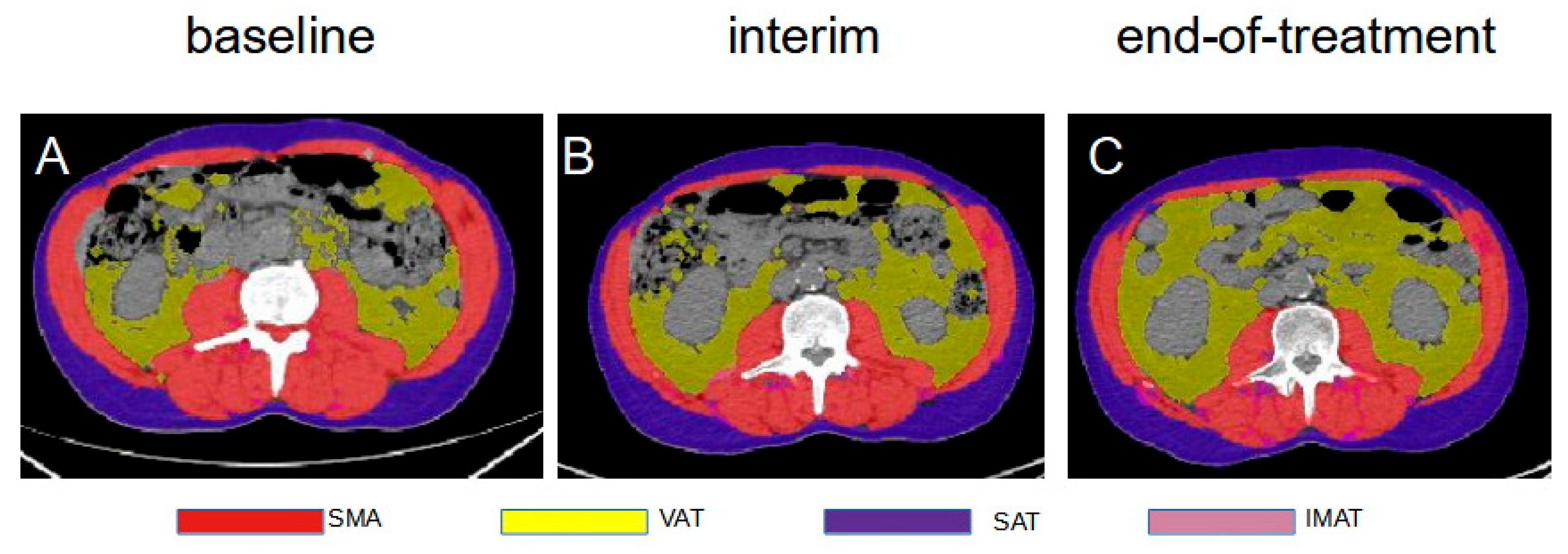
2.2. Body Composition Analysis
2.3. Statistical Analysis
3. Results
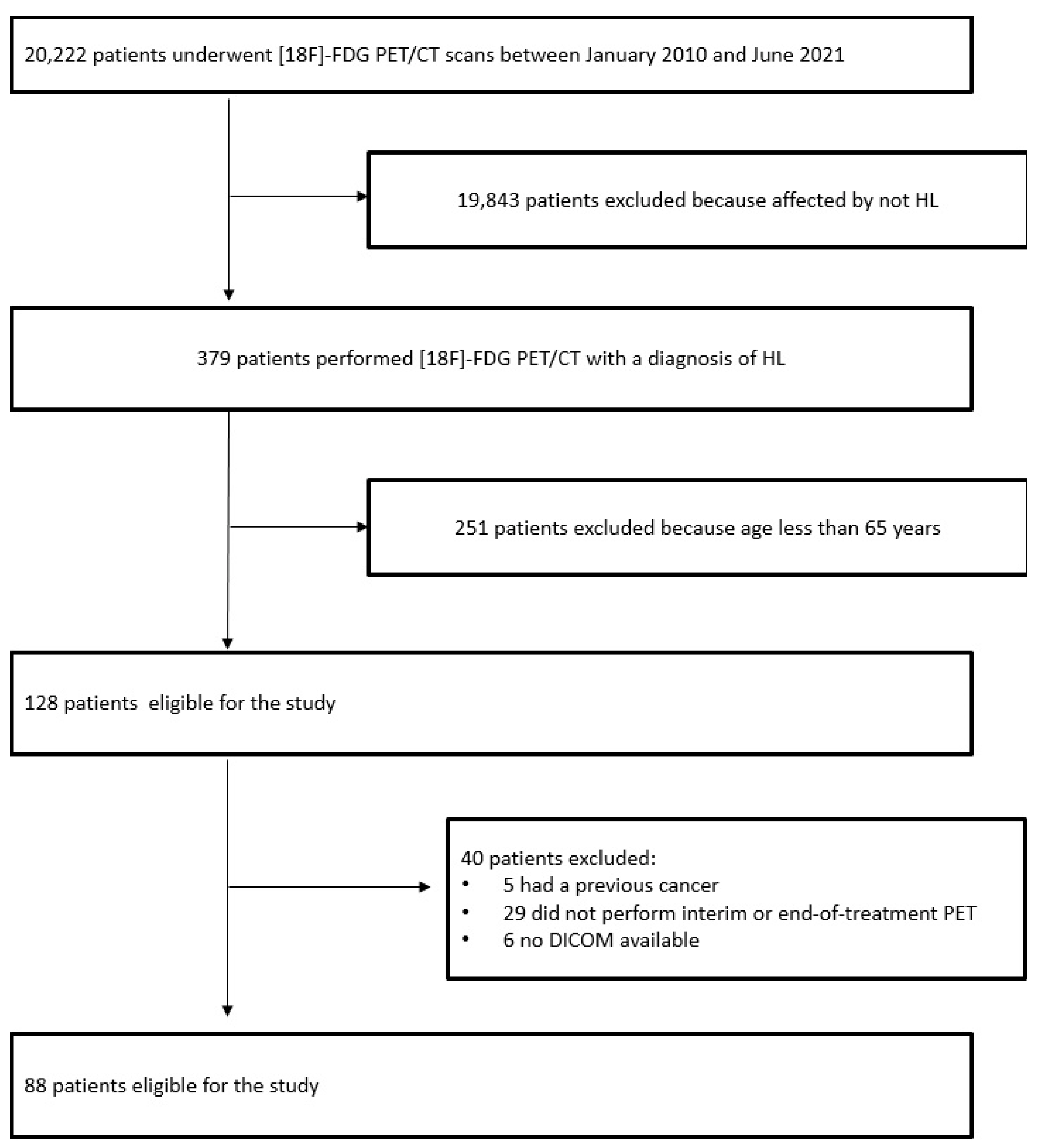
3.1. Patients Features
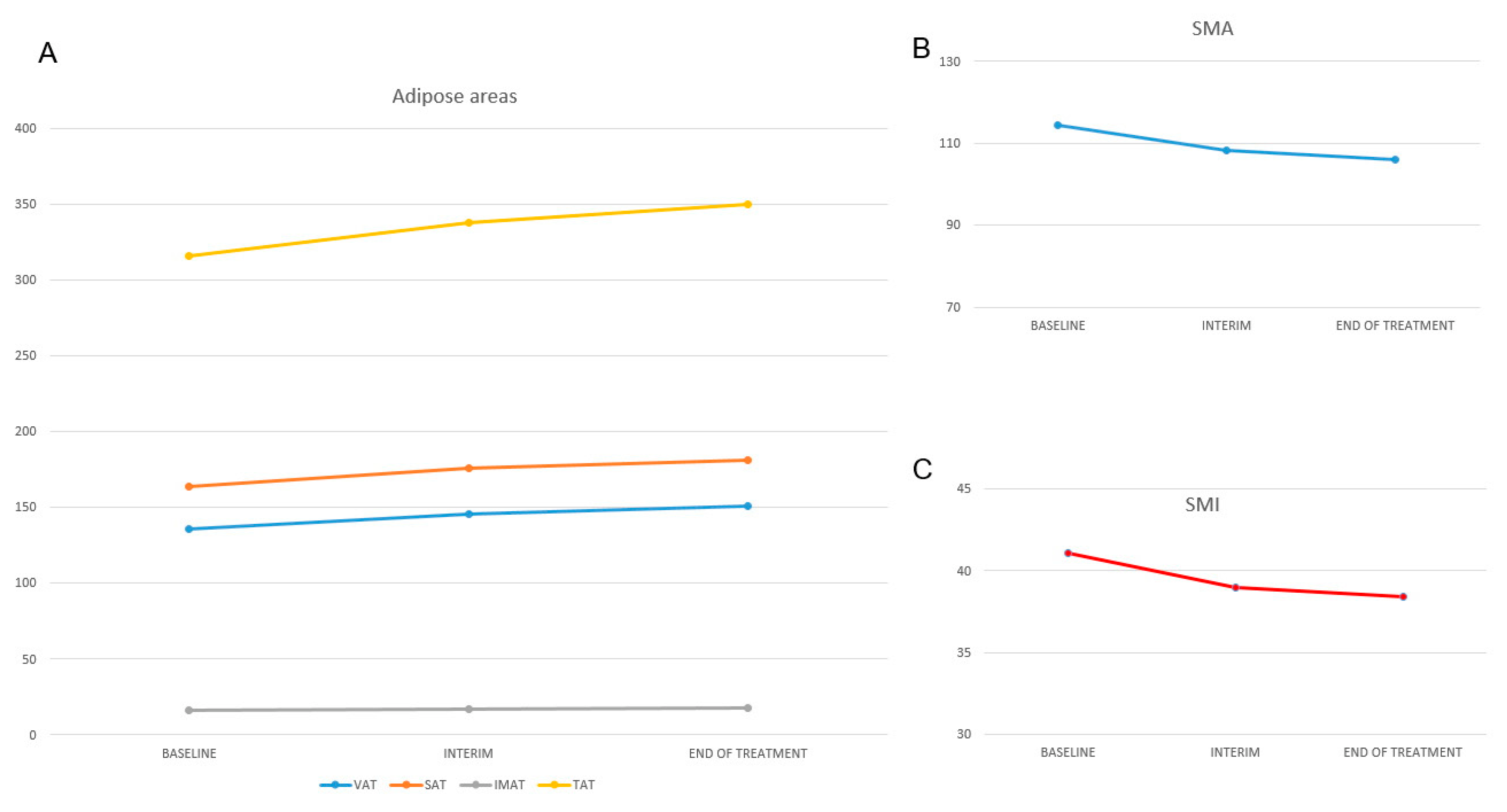
3.2. Body Composition Changes
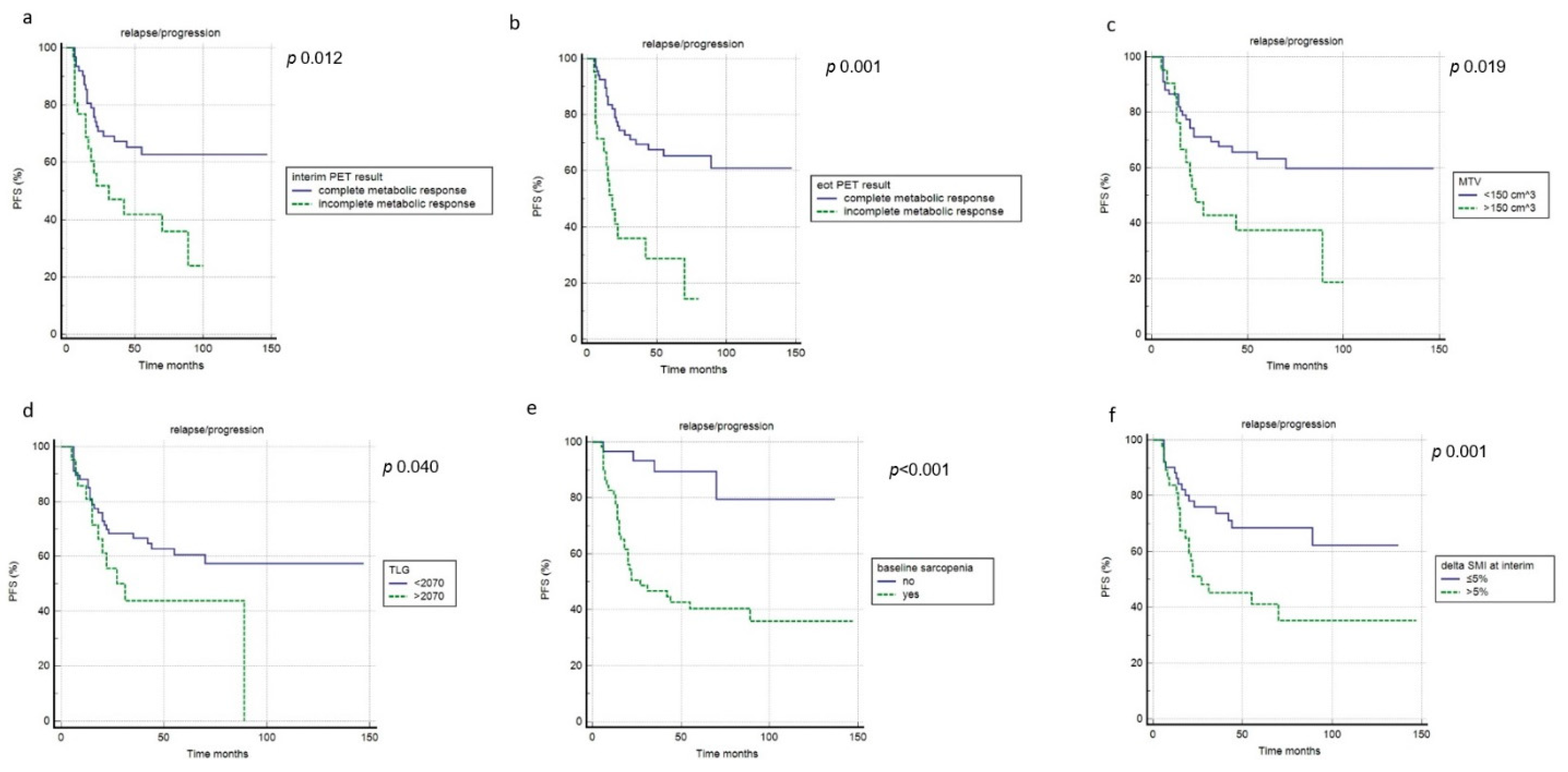
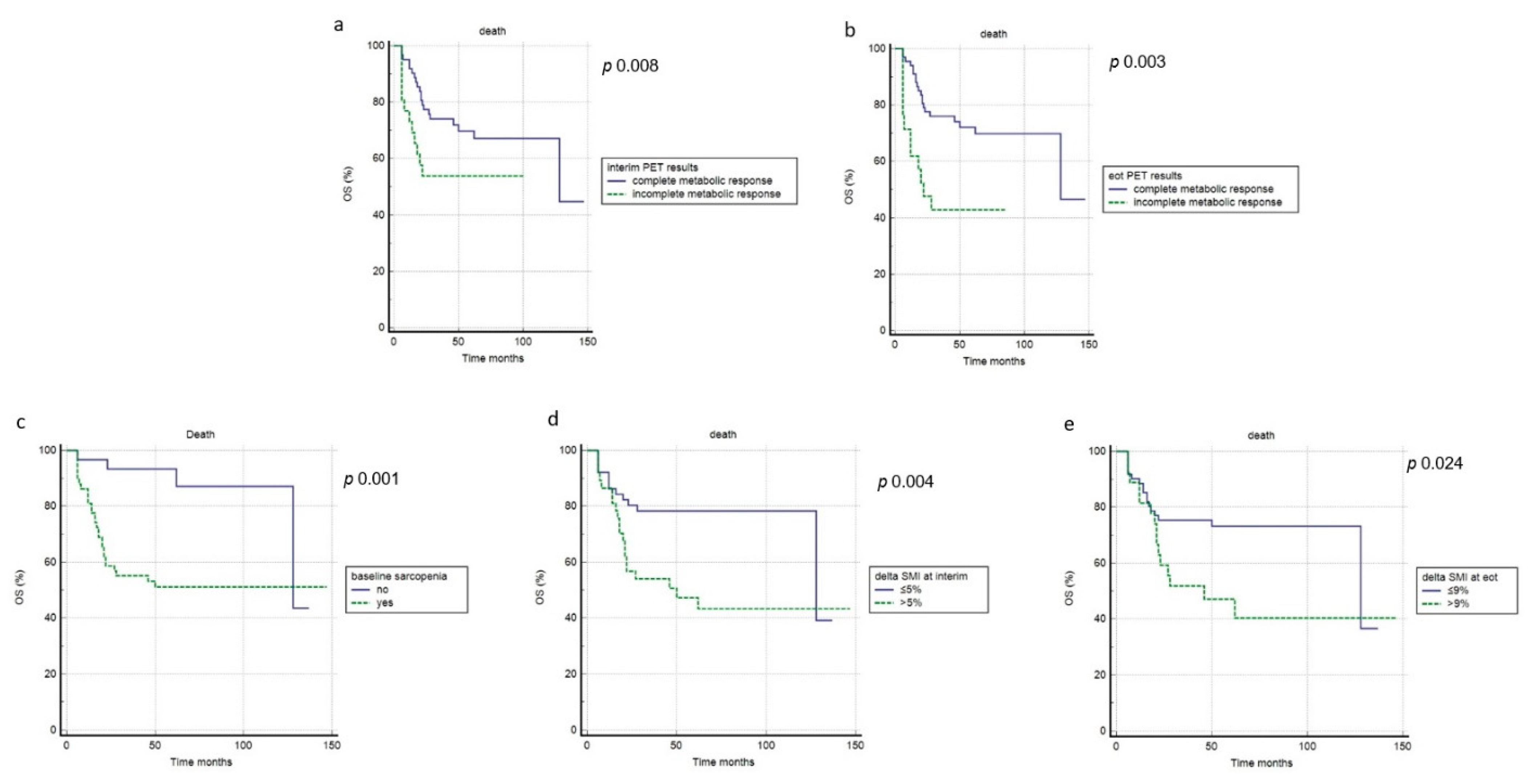
3.3. Prognostic Impact
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Halbsguth, T.V.; Böll, B.; Borchmann, P.; Diehl, V. The unique characteristics and management of patients over 60 years of age with classic Hodgkin lymphoma. Curr. Hematol. Malig. Rep. 2011, 6, 164–171. [Google Scholar] [CrossRef] [PubMed]
- Evens, A.M.; Sweetenham, J.W.; Horning, S.J. Hodgkin lymphoma in older patients: An uncommon disease in need of study. Oncology 2008, 22, 369–379. [Google Scholar]
- Klimm, B.; Diehl, V.; Engert, A. Hodgkin’s Lymphoma in the elderly: A different disease in patients over 60. Oncology 2007, 21, 982–990. [Google Scholar]
- Albano, D.; Mazzoletti, A.; Zilioli, V.R.; Muzi, C.; Crucitti, L.; Tucci, A.; Pagani, C.; Re, A.; Rossetti, C.; Giubbini, R.; et al. Clinical and prognostic role of interim 18F-FDG PET/CT in elderly Hodgkin lymphoma: A dual-center experience. Leuk. Lymphoma. 2020, 61, 3209–3216. [Google Scholar] [CrossRef] [PubMed]
- Albano, D.; Mazzoletti, A.; Spallino, M.; Muzi, C.; Zilioli, V.R.; Pagani, C.; Tucci, A.; Rossetti, C.; Giubbini, R.; Bertagna, F. Prognostic role of baseline 18F-FDG PET/CT metabolic parameters in elderly HL: A two-center experience in 123 patients. Ann. Hematol. 2020, 99, 1321–1330. [Google Scholar] [CrossRef]
- Albano, D.; Dondi, F.; Ravanelli, M.; Tucci, A.; Farina, D.; Giubbini, R.; Treglia, G.; Bertagna, F. Prognostic Role of "Radiological" Sarcopenia in Lymphoma: A Systematic Review. Clin. Lymphoma Myeloma Leuk. 2022, 22, e340–e349. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cederholm, T.; Barazzoni, R.; Austin, P.; Ballmer, P.; Biolo, G.; Bischoff, S.C.; Compher, C.; Correia, I.; Higashiguchi, T.; Holst, M.; et al. ESPEN guidelines on definitions and terminology of clinical nutrition. Clin. Nutr. 2017, 36, 49–64. [Google Scholar] [CrossRef]
- Albano, D.; Camoni, L.; Rinaldi, R.; Tucci, A.; Zilioli, V.R.; Muzi, C.; Ravanelli, M.; Farina, D.; Coppola, A.; Camalori, M.; et al. Comparison between skeletal muscle and adipose tissue measurements with high-dose CT and low-dose attenuation correction CT of 18F-FDG PET/CT in elderly Hodgkin lymphoma patients: A two-centre validation. Br. J. Radiol. 2021, 94, 20200672. [Google Scholar] [CrossRef] [PubMed]
- Jabbour, J.; Manana, B.; Zahreddine, A.; Saade, C.; Charafeddine, M.; Bazarbachi, A.; Blaise, D.; El-Cheikh, J. Sarcopenic obesity derived from PET/CT predicts mortality in lymphoma patients undergoing hematopoietic stem cell transplantation. Curr. Res. Transl. Med. 2019, 67, 93–99. [Google Scholar] [CrossRef] [PubMed]
- DeFilipp, Z.; Troschel, F.M.; Qualls, D.A.; Li, S.; Kuklinski, M.W.; Kempner, M.E.; Hochberg, E.; Chen, Y.B.; El-Jawahri, A.; Fintelmann, F.J. Evolution of Body Composition Following Autologous and Allogeneic Hematopoietic Cell Transplantation: Incidence of Sarcopenia and Association with Clinical Outcomes. Biol. Blood Marrow Transplant. 2018, 24, 1741–1747. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, R.J.; Michaud, L.; Lobaugh, S.M.; Nakajima, R.; Mauguen, A.; Elko, T.A.; Ruiz, J.D.; Maloy, M.A.; Sauter, C.S.; Dahi, P.B.; et al. The geriatric syndrome of sarcopenia impacts allogeneic hematopoietic cell transplantation outcomes in older lymphoma patients. Leuk. Lymphoma. 2020, 61, 1833–1841. [Google Scholar] [CrossRef] [PubMed]
- Xiao, D.Y.; Luo, S.; O’Brian, K.; Sanfilippo, K.M.; Ganti, A.; Riedell, P.; Lynch, R.C.; Liu, W.; Kahl, B.S.; Cashen, A.F.; et al. Longitudinal Body Composition Changes in Diffuse Large B-cell Lymphoma Survivors: A Retrospective Cohort Study of United States Veterans. J. Natl. Cancer Inst. 2016, 108, djw145. [Google Scholar] [CrossRef] [Green Version]
- Boellaard, R.; Delgado-Bolton, R.; Oyen, W.J.G.; Giammarile, F.; Tatsch, K.; Eschner, W.; Verzijlbergen, F.J.; Barrington, S.F.; Pike, L.C.; Weber, W.A.; et al. FDG PET/CT: EANM procedure guidelines for tumour imaging: Version 2.0. Eur. J. Nucl. Med. Mol. Imaging. 2015, 42, 328–354. [Google Scholar] [CrossRef] [PubMed]
- Cheson, B.D.; Fisher, R.I.; Barrington, S.F.; Cavalli, F.; Schwartz, L.H.; Zucca, E.; Lister, T.A. Recommendations for initial evaluation, staging, and response assessment of Hodgkin and non-Hodgkin lymphoma: The Lugano classification. J. Clin. Oncol. 2014, 32, 3059–3068. [Google Scholar] [CrossRef]
- Barrington, S.F.; Mikhaeel, N.G.; Kostakoglu, L.; Meignan, M.; Hutchings, M.; Müeller, S.P.; Schwartz, L.H.; Zucca, E.; Fisher, R.I.; Trotman, J.; et al. Role of imaging in the staging and response assessment of lymphoma: Consensus of the International Conference on Malignant Lymphomas Imaging Working Group. J. Clin. Oncol. 2014, 32, 3048–3058. [Google Scholar] [CrossRef]
- Küppers, R.; Schwering, I.; Bräuninger, A.; Rajewsky, K.; Hansmann, M.L. Biology of Hodgkin’s lymphoma. Ann. Oncol. 2002, 13 (Suppl. 1), 11. [Google Scholar] [CrossRef] [PubMed]
- Schmitz, R.; Stanelle, J.; Hansmann, M.L.; Küppers, R. Pathogenesis of classical and lymphocyte-predominant Hodgkin lymphoma. Annu. Rev. Pathol. 2009, 4, 151–174. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.R.; Shipp, M.A. Signaling pathways and immune evasion mechanisms in classical Hodgkin lymphoma. Blood 2017, 130, 2265–2270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zilioli, V.R.; Albano, D.; Arcari, A.; Merli, F.; Coppola, A.; Besutti, G.; Marcheselli, L.; Gramegna, D.; Muzi, C.; Manicone, M.; et al. Clinical and prognostic role of sarcopenia in elderly patients with classical Hodgkin lymphoma: A multicentre experience. J. Cachexia Sarcopenia Muscle 2021, 12, 1042–1055. [Google Scholar] [CrossRef] [PubMed]
- Bas, V.; Umit, E.G.; Korkmaz, U.; Baysal, M.; Karaman Gulsaran, S.; Demirci, U.; Kirkizlar, H.O.; Durmus Altun, G.; Demir, A.M. Sarcopenia in Hodgkin’s lymphoma evaluated with 18-FDG PET/CT, focus on age, performance, and treatment. Support. Care Cancer. 2021, 29, 2475–2480. [Google Scholar] [CrossRef] [PubMed]
- Tucci, A.; Martelli, M.; Rigacci, L.; Riccomagno, P.; Cabras, M.G.; Salvi, F.; Stelitano, C.; Fabbri, A.; Storti, S.; Fogazzi, S.; et al. Comprehensive geriatric assessment is an essential tool to support treatment decisions in elderly patients with diffuse large B-cell lymphoma: A prospective multicenter evaluation in 173 patients by the Lymphoma Italian Foundation (FIL). Leuk. Lymphoma 2015, 56, 921–926. [Google Scholar] [CrossRef] [PubMed]
- Merli, F.; Luminari, S.; Rossi, G.; Mammi, C.; Marcheselli, L.; Alvarez, I.; Tucci, A.; Stelitano, C.; Ilariucci, F.; Musso, M.; et al. Outcome of elderly frail patients with diffuse large B-cell lymphoma (DLBCL) prospectively identified by comprehensive geriatric assessment (CGA). Results from a study of the Intergruppo Italiano Linfomi (IIL). Leuk. Lymphoma 2014, 55, 38–43. [Google Scholar] [CrossRef]
- Merli, F.; Luminari, S.; Tucci, A.; Arcari, A.; Rigacci, L.; Hawkes, E.; Chiattone, C.S.; Cavallo, F.; Cabras, G.; Alvarez, I.; et al. Simplified geriatric assessment in older patients with diffuse large B-cell lymphoma: The prospective elderly project of the Fondazione Italiana Linfomi. J. Clin. Oncol. 2021, 39, 1214–1222. [Google Scholar] [CrossRef] [PubMed]
- Bertagna, F.; Giubbini, R.; Albano, D. Evidence-Based PET for Haematological Tumours. Chapter 9. In Evidence-Based Positron Emission Tomography. Book: Summary of Recent Meta-analyses on PET; Springer: Berlin/Heidelberg, Germany, 2020. [Google Scholar] [CrossRef]
- Albano, D.; Bosio, G.; Pagani, C.; Re, A.; Tucci, A.; Giubbini, R.; Bertagna, F. Prognostic role of baseline 18F-FDG PET/CT metabolic parameters in Burkitt lymphoma. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 87–96. [Google Scholar] [CrossRef]
- Albano, D.; Bosio, G.; Bianchetti, N.; Pagani, C.; Re, A.; Tucci, A.; Giubbini, R.; Bertagna, F. Prognostic role of baseline 18F-FDG PET/CT metabolic parameters in mantle cell lymphoma. Ann. Nucl. Med. 2019, 33, 449–458. [Google Scholar] [CrossRef] [PubMed]
- Albano, D.; Bertoli, M.; Battistotti, M.; Rodella, C.; Statuto, M.; Giubbini, R.; Bertagna, F. Prognostic role of pretreatment 18F-FDG PET/CT in primary brain lymphoma. Ann. Nucl. Med. 2018, 32, 532–541. [Google Scholar] [CrossRef]
- Guo, B.; Tan, X.; Cen, H. Prognostic value of baseline tumor volume and total lesion glycolysis in patients with lymphoma: A meta-analysis. PLoS ONE 2019, 14, e0210224. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Mean ± SD (Range) | n (%) |
|---|---|---|
| Age, years | 72.8 ± 5.6 (65–91) | |
| Gender | ||
| Female | 47 (53%) | |
| Male | 41 (47%) | |
| BMI kg/m2 | 24.9 ± 4.7 (16.9–41.1) | |
| Normal | 41 (47%) | |
| Overweight | 43 (49%) | |
| Underweight | 4 (5%) | |
| Symptoms B | 40 (45%) | |
| Bulky disease | 7 (7%) | |
| LDH > normal level | 50 (57%) | |
| Stage | ||
| I-II | 22 (25%) | |
| III-IV | 66 (75%) | |
| Histology | ||
| Nodular sclerosis | 46 (52%) | |
| Mixed cellularity | 23 (26%) | |
| Lymphocyte rich | 5 (6%) | |
| Lymphocyte deplete | 4 (5%) | |
| Not specified | 10 (11%) | |
| CGA | ||
| FIT | 60 (68%) | |
| UNFIT | 20 (23%) | |
| FRAIL | 8 (9%) | |
| Treatment | ||
| ABVD/ABVD-like | 63 (72%) | |
| BCVPP | 16 (18%) | |
| BEACOPP | 7 (7%) | |
| R-CHOP | 2 (3%) | |
| Interim PET/CT results | ||
| DS 1–3 | 62 (70%) | |
| DS 4–5 | 26 (30%) | |
| End-of-treatment PET/CT results | ||
| DS 1–3 | 67 (76%) | |
| DS 4–5 | 21 (24%) | |
| Baseline MTV | 129.9 ± 150.6 (4–981) | |
| Baseline TLG | 1608 ± 1859 (9–11,627) |
| Variable | Baseline | Interim | End-of-Treatment |
|---|---|---|---|
| SMA (cm2), mean ± SD (range) | 114.5 ± 28.8 (66.8–188.8) | 108.3 ± 26.2 (66–172) | 106 ± 26 (62.6–171) |
| Δ% from baseline | −5% | −7% | |
| SMI (cm2/m2), mean ± SD (range) | 41.4 ± 8.9 (22.5–63) | 39.1 ± 8.1 (22.3–57) | 38.4 ± 8.3 (21–56.7) |
| Δ% from baseline | −5% | −7% | |
| VAT (cm2), mean ± SD (range) | 135.5 ± 89.1 (6.4–375) | 145.2 ± 93.6 (7.9–385) | 151 ± 96.3 (8.9–399) |
| Δ% from baseline | +7% | +11% | |
| SAT (cm2), mean ± SD (range) | 163.7 ± 136 (14.6–1201) | 175.6 ± 150.8 (16.5–1350) | 181.3 ± 153.3 (18–1360) |
| Δ% from baseline | +7% | +11% | |
| IMAT (cm2), mean ± SD (range) | 16.3 ± 13.5 (1.2–95) | 17.1 ± 13.8 (1.35–98) | 18 ± 14 (1.5–98) |
| Δ% from baseline | +5% | +10% | |
| TAT (cm2), mean ± SD (range) | 315.5 ± 182.9 (24–1313) | 337.7 ± 198 (24–1468) | 350 ± 202.5 (24–1485) |
| Δ% from baseline | +7% | +11% | |
| Sarcopenia, n (%) | 58 (66%) | 68 (77%) | 73 (83%) |
| Δ% from baseline | +11% | +17% |
| Variable | Baseline | ||
|---|---|---|---|
| Sarcopenia n = 58 | Not Sarcopenia n = 30 | p Value | |
| Age (average ± SD) | 72.6 ± 5.7 | 73.2 ± 5 | 0.697 |
| Female:male | 29:29 | 18:12 | 0.258 |
| BMI (average ± SD) | 23.8 ± 3.7 | 27.3 ± 5.5 | <0.001 |
| Tumor stage III-IV | 43 (74%) | 23 (77%) | 0.518 |
| Symptoms B | 32 (55%) | 8 (27%) | 0.011 |
| Bulky disease | 6 (10%) | 1 (3%) | 0.278 |
| LDH > normal level | 28 (47%) | 12 (40%) | 0.832 |
| Nodular sclerosis variant | 29 (50%) | 17 (57%) | 0.091 |
| CGA FIT:UNFIT:FRAIL | 37:14:7 | 23:6:1 | 0.019 |
| Treatment ABVD/ABVD like | 18 (31%) | 8 (27%) | 0.674 |
| iPET complete metabolic response | 41 (71%) | 21 (70%) | 0.443 |
| eotPET complete metabolic response | 42 (72%) | 25 (83%) | 0.312 |
| Baseline MTV (average ± SD) | 139.4 ± 137.7 | 110.7 ± 161.9 | 0.404 |
| Baseline TLG (average ± SD) | 1682 ± 1729 | 1459 ± 1916 | 0.600 |
| Interim | |||
| Sarcopenia n = 68 | Not sarcopenia n = 20 | ||
| Age (average ± SD) | 72.8 ± 5.7 | 72.85 ± 5.3 | 0.993 |
| Female:male | 33:35 | 14:6 | 0.092 |
| BMI (average ± SD) | 24.1 ± 4 | 27.8 ± 5.8 | 0.001 |
| Tumor stage III-IV | 49 (73%) | 17 (85%) | 0.562 |
| Symptoms B | 33 (48%) | 7 (35%) | 0.298 |
| Bulky disease | 6 (9%) | 1 (5%) | 0.583 |
| LDH > normal level | 32 (47%) | 8 (40%) | 0.767 |
| Nodular sclerosis variant | 34 (50%) | 12 (60%) | 0.316 |
| CGA FIT:UNFIT:FRAIL | 43:18:7 | 17:2:1 | 0.009 |
| Treatment ABVD/ABVD like | 21 (31%) | 5 (25%) | 0.617 |
| eotPET complete metabolic response | 52 (76%) | 15 (75%) | 0.893 |
| Baseline MTV (average ± SD) | 131.7 ± 130 | 123.9 ± 208.8 | 0.840 |
| Baseline TLG (average ± SD) | 1627 ± 637 | 1545 ± 2522 | 0.863 |
| End of treatment | |||
| Sarcopenia n = 73 | Not sarcopenia n = 15 | ||
| Age (average ± SD) | 72.5 ± 5.6 | 74.3 ± 5.3 | 0.256 |
| Female:male | 35:38 | 12:3 | 0.023 |
| BMI (average ± SD) | 24.6 ± 4.4 | 27 ± 5.8 | 0.065 |
| Tumor stage III-IV | 56 (77%) | 10 (67%) | 0.871 |
| Symptoms B | 35 (48%) | 5 (33%) | 0.645 |
| Bulky disease | 7 (14%) | 0 (0%) | 0.215 |
| LDH > normal level | 36 (49%) | 4 (27%) | 0.798 |
| Nodular sclerosis variant | 38 (52%) | 8 (53%) | 0.248 |
| CGA FIT:UNFIT:FRAIL | 47:18:8 | 13:2:0 | 0.003 |
| Treatment ABVD/ABVD like | 21 (29%) | 5 (33%) | 0.727 |
| Baseline MTV (average ± SD) | 142.2 ± 161 | 69.9 ± 47.4 | 0.090 |
| Baseline TLG (average ± SD) | 1751 ± 1988 | 912 ± 725 | 0.111 |
| Variable | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| HR (95% CI) | p Value | HR (95% CI) | p Value | |
| PFS | ||||
| Gender | 1.528 (0.800–2.925) | 0.198 | ||
| Age > 75 | 2.021 (1.026–3.979) | 0.041 | 1.314 (0.667–2.590) | 0.429 |
| BMI | 1.989 (0.450–3.456) | 0.450 | ||
| Tumor Stage | 1.704 (0.837–3.471) | 0.145 | ||
| Symptoms B | 1.970 (1.026–3.783) | 0.041 | 1.807 (0.931–3.508) | 0.080 |
| LDH level > normal value | 1.340 (0.701–2.345) | 0.222 | ||
| Bulky disease | 1.546 (0.457–5.221) | 0.484 | ||
| Nodular sclerosis variant | 0.995 (0.520–1.899) | 0.989 | ||
| CGA FIT | 0.785 (0.393–1.570) | 0.495 | ||
| Treatment ABVD/ABVD like | 1.918 (0.911–4.038) | 0.086 | ||
| iPET complete metabolic response | 1.259 (1.230–5.464) | 0.012 | 2.878 (1.340–5.009) | 0.023 |
| eotPET complete metabolic response | 5.888 (2.448–14.181) | 0.001 | 3.303 (1.571–6.940) | 0.001 |
| MTV > 150 cm3 | 2.547 (1.163–5.579) | 0.019 | 2.085 (1.062–4.092) | 0.032 |
| TLG > 2070 | 2.936 (1.876–4.278) | 0.040 | 2.430 (1.201–4.332) | 0.043 |
| Baseline sarcopenia | 3.725 (1.934–7.174) | <0.001 | 3.881 (1.009–7.021) | 0.001 |
| Interim-ΔSMI > 5% | 2.391 (1.230–4.646) | 0.010 | 3.768 (0.800–5-987) | 0.124 |
| End-of-treatment-ΔSMI > 9% | 1.909 (0.923–3.950) | 0.081 | ||
| OS | ||||
| Gender | 1.098 (9.537–2.246) | 0.796 | ||
| Age > 75 | 2.929 (1.381–6.213) | 0.005 | 1.545 (0.682–3.492) | 0.297 |
| BMI | 1.888 (0.560–2.987) | 0.230 | ||
| Tumor Stage | 2.007 (0.918–4.383) | 0.080 | ||
| Symptoms B | 1.660 (0.807–3.412) | 0.168 | ||
| LDH level > normal value | 0.685 (0.386–1.909) | 0.546 | ||
| Bulky disease | 1.546 (0.457–5.221) | 0.484 | ||
| Nodular sclerosis variant | 0.884 (0.437–1.787) | 0.732 | ||
| CGA FIT | 1.520 (0.711–3.250) | 0.279 | ||
| Treatment ABVD/ABVD like | 4.473 (1.949–10.263) | <0.001 | 2.874 (0.309–6.310) | 0.222 |
| iPET complete metabolic response | 2.067 (1.090–4.669) | 0.008 | 2.222 (1.101–5.234) | 0.012 |
| eotPET complete metabolic response | 3.890 (1.554–9.740) | 0.003 | 2.402 (1.080–5.336) | 0.019 |
| MTV > 150 cm3 | 1.346 (0.582–3.109) | 0.483 | ||
| TLG > 2070 | 2.118 (0.904–4.966) | 0.084 | ||
| Baseline sarcopenia | 3.275 (1.592–6.737) | 0.001 | 3.661 (1.111–7.321) | 0.001 |
| Interim-ΔSMI > 5% | 2.789 (1.365–5.737) | 0.004 | 2.324 (1.130–4.021) | 0.009 |
| End-of-treatment-ΔSMI >9% | 2.438 (1.124–5.288) | 0.024 | 4.001 (2.245–6.091) | 0.031 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Albano, D.; Dondi, F.; Treglia, G.; Tucci, A.; Ravanelli, M.; Farina, D.; Bertagna, F. Longitudinal Body Composition Changes Detected by [18F]FDG PET/CT during and after Chemotherapy and Their Prognostic Role in Elderly Hodgkin Lymphoma. Cancers 2022, 14, 5147. https://doi.org/10.3390/cancers14205147
Albano D, Dondi F, Treglia G, Tucci A, Ravanelli M, Farina D, Bertagna F. Longitudinal Body Composition Changes Detected by [18F]FDG PET/CT during and after Chemotherapy and Their Prognostic Role in Elderly Hodgkin Lymphoma. Cancers. 2022; 14(20):5147. https://doi.org/10.3390/cancers14205147
Chicago/Turabian StyleAlbano, Domenico, Francesco Dondi, Giorgio Treglia, Alessandra Tucci, Marco Ravanelli, Davide Farina, and Francesco Bertagna. 2022. "Longitudinal Body Composition Changes Detected by [18F]FDG PET/CT during and after Chemotherapy and Their Prognostic Role in Elderly Hodgkin Lymphoma" Cancers 14, no. 20: 5147. https://doi.org/10.3390/cancers14205147