Cutaneous Melanoma versus Vulvovaginal Melanoma—Risk Factors, Pathogenesis and Comparison of Immunotherapy Efficacy

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
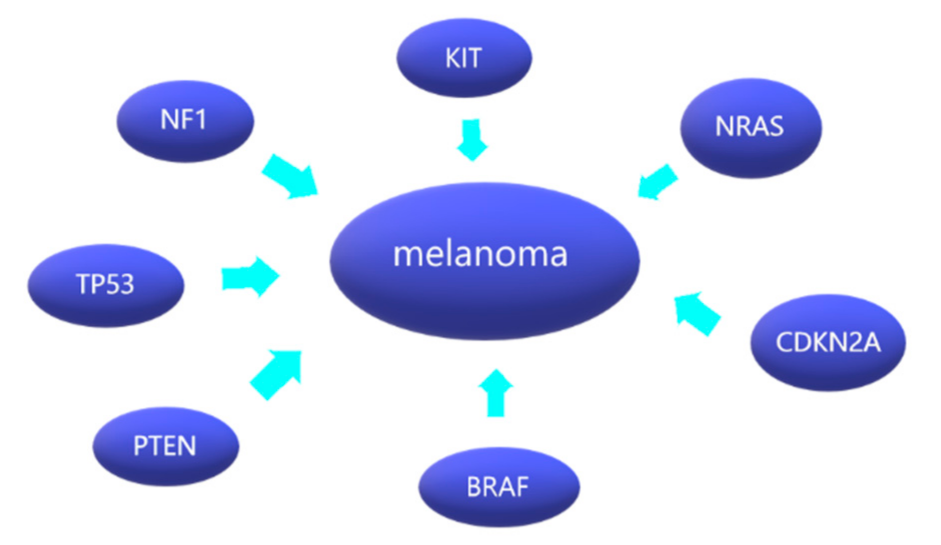
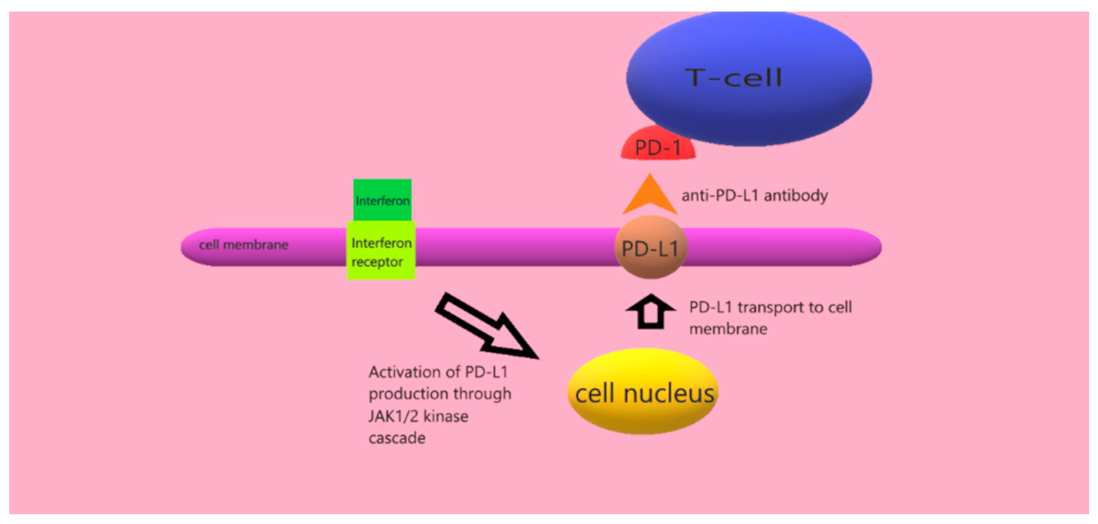
2. Pathogenesis
3. Immunotherapy of Cutaneous Melanoma
4. Immunotherapy of Vulvar and Vaginal Melanoma
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Schadendorf, D.; van Akkooi, A.C.J.; Berking, C.; Griewank, K.G.; Gutzmer, R.; Hauschild, A.; Stang, A.; Roesch, A.; Ugurel, S. Melanoma. Lancet 2018, 392, 971–984. [Google Scholar] [CrossRef]
- Eggermont, A.M.; Spatz, A.; Robert, C. Cutaneous melanoma. Lancet 2014, 383, 816–827. [Google Scholar] [CrossRef]
- Crocetti, E.; Mallone, S.; Robsahm, T.E.; Gavin, A.; Agius, D.; Ardanaz, E.; Lopez, M.-D.C.; Innos, K.; Minicozzi, P.; Borgognoni, L.; et al. Survival of patients with skin melanoma in Europe increases further: Results of the EUROCARE-5 study. Eur. J. Cancer 2015, 51, 2179–2190. [Google Scholar] [CrossRef] [Green Version]
- Bataille, V.; Winnett, A.; Sasieni, P.; Bishop, J.N.; Cuzick, J. Exposure to the sun and sunbeds and the risk of cutaneous melanoma in the UK: A case–control study. Eur. J. Cancer 2004, 40, 429–435. [Google Scholar] [CrossRef]
- Titus-Ernstoff, L.; Perry, A.E.; Spencer, S.K.; Gibson, J.J.; Cole, B.F.; Ernstoff, M.S. Pigmentary characteristics and moles in relation to melanoma risk. Int. J. Cancer 2005, 116, 144–149. [Google Scholar] [CrossRef] [PubMed]
- JGrob, J.-J.; Gouvernet, J.; Aymar, D.; Mostaque, A.; Romano, M.H.; Collet, A.M.; Noe, M.C.; DiConstanzo, M.P.; Bonerandi, J.J. Count of benign melanocytic nevi as a major indicator of risk for nonfamilial nodular and superficial spreading melanoma. Cancer 1990, 66, 387–395. [Google Scholar] [CrossRef]
- Ford, D.; Bliss, J.M.; Swerdlow, A.J.; Armstrong, B.K.; Franceschi, S.; Green, A.; Holly, E.A.; Mack, T.; Mackie, R.M.; Østerlind, A.; et al. Risk of cutaneous melanoma associated with a family history of the disease. Int. J. Cancer 1995, 62, 377–381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spanogle, J.P.; Clarke, C.A.; Aroner, S.; Swetter, S.M. Risk of second primary malignancies following cutaneous melanoma diagnosis: A population-based study. J. Am. Acad. Dermatol. 2010, 62, 757–767. [Google Scholar] [CrossRef]
- Sitenga, J.L.; Aird, G.; Ahmed, A.; Walters, R.; Silberstein, P.T. Socioeconomic status and survival for patients with melanoma in the United States: An NCDB analysis. Int. J. Dermatol. 2018, 57, 1149–1156. [Google Scholar] [CrossRef]
- Chang, E.; Karnell, L.H.; Menck, H.R. The National Cancer Data Base report on cutaneous and noncutaneous melanoma. Cancer 1998, 83, 1664–1678. [Google Scholar] [CrossRef]
- Rachidi, S.; Deng, Z.; Sullivan, D.Y.; Lipson, E.J. Shorter survival and later stage at diagnosis among unmarried patients with cutaneous melanoma: A US national and tertiary care center study. J. Am. Acad. Dermatol. 2020, 83, 1012–1020. [Google Scholar] [CrossRef] [PubMed]
- Wohlmuth, C.; Wohlmuth-Wieser, I.; May, T.; Vicus, D.; Gien, L.T.; Laframboise, S. Malignant Melanoma of the Vulva and Vagina: A US Population-Based Study of 1863 Patients. Am. J. Clin. Dermatol. 2020, 21, 285–295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balch, C.M.; Soong, S.-J.; Atkins, M.B.; Buzaid, A.C.; Cascinelli, N.; Coit, D.G.; Fleming, I.D.; Gershenwald, J.E.; Houghton, A.; Kirkwood, J.M.; et al. An evidence-based staging system for cutaneous melanoma. CA A Cancer J. Clin. 2004, 54, 131–149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goodson, A.G.; Grossman, D. Strategies for early melanoma detection: Approaches to the patient with nevi. J. Am. Acad. Dermatol. 2009, 60, 719–735. [Google Scholar] [CrossRef] [Green Version]
- September, P. Mitotic activity in non-neoplastic melanocytes in vivo. Prospects 1975, 66, 23. [Google Scholar]
- Hodis, E.; Watson, I.R.; Kryukov, G.V.; Arold, S.T.; Imielinski, M.; Theurillat, J.-P.; Nickerson, E.; Auclair, D.; Li, L.; Place, C.; et al. A Landscape of Driver Mutations in Melanoma. Cell 2012, 150, 251–263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The Cancer Genome Atlas Network. Genomic Classification of Cutaneous Melanoma. Cell 2015, 161, 1681–1696. [Google Scholar] [CrossRef] [Green Version]
- Libra, M.; Malaponte, G.; Navolanic, P.M.; Gangemi, P.; Bevelacqua, V.; Proietti, L.; Bruni, B.; Stivala, F.; Mazzarino, M.C.; Travali, S.; et al. Analysis of BRAF Mutation in Primary and Metastatic Melanoma Brief Report ABBREVIATIONS ND KEY WORDS ES CE INTRODUCTION RIB. Cell Cycle 2005, 4, 1382–1384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yun, J.; Lee, J.; Jang, J.; Lee, E.J.; Jang, K.T.; Kim, J.H.; Kim, K.-M. KIT amplification and gene mutations in acral/mucosal melanoma in Korea. APMIS 2011, 119, 330–335. [Google Scholar] [CrossRef] [PubMed]
- Nassar, K.; Tan, A.C. The mutational landscape of mucosal melanoma. Semin. Cancer Biol. 2020, 61, 139–148. [Google Scholar] [CrossRef]
- Darman, R.B.; Seiler, M.; Agrawal, A.A.; Lim, K.H.; Peng, S.; Aird, D.; Bailey, S.L.; Bhavsar, E.B.; Chan, B.; Colla, S.; et al. Cancer-Associated SF3B1 Hotspot Mutations Induce Cryptic 3′ Splice Site Selection through Use of a Different Branch Point. Cell Rep. 2015, 13, 1033–1045. [Google Scholar] [CrossRef] [PubMed]
- Hintzsche, J.D.; Gorden, N.T.; Amato, C.M.; Kim, J.; Wuensch, K.E.; Robinson, S.E.; Applegate, A.J.; Couts, K.L.; Medina, T.M.; Wells, K.R.; et al. Whole-exome sequencing identifies recurrent SF3B1 R625 mutation and comutation of NF1 and KIT in mucosal melanoma. Melanoma Res. 2017, 27, 189–199. [Google Scholar] [CrossRef] [PubMed]
- Quek, C.; Rawson, R.V.; Ferguson, P.M.; Shang, P.; Silva, I.; Saw, R.P.; Shannon, K.; Thompson, J.F.; Hayward, N.K.; Long, G.V.; et al. Recurrent hotspot SF3B1 mutations at codon 625 in vulvovaginal mucosal melanoma identified in a study of 27 Australian mucosal melanomas. Oncotarget 2019, 10, 930–941. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dhawan, P.; Singh, A.B.; Ellis, D.L.; Richmond, A. Constitutive activation of Akt/protein kinase B in melanoma leads to up-regulation of nuclear factor-κB and tumor progression. Cancer Res. 2002, 62, 7335–7342. [Google Scholar] [PubMed]
- Kong, Y.; Si, L.; Li, Y.; Wu, X.; Xu, X.; Dai, J.; Tang, H.; Ma, M.; Chi, Z.; Sheng, X.; et al. Analysis of mTOR Gene Aberrations in Melanoma Patients and Evaluation of Their Sensitivity to PI3K–AKT–mTOR Pathway Inhibitors. Clin. Cancer Res. 2016, 22, 1018–1027. [Google Scholar] [CrossRef] [Green Version]
- Wu, H.; Goel, V.; Haluska, F.G. PTEN signaling pathways in melanoma. Oncogene 2003, 22, 3113–3122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garcia-Diaz, A.; Shin, D.S.; Moreno, B.H.; Saco, J.; Escuin-Ordinas, H.; Rodriguez, G.A.; Zaretsky, J.M.; Sun, L.; Hugo, W.; Wang, X.; et al. Interferon Receptor Signaling Pathways Regulating PD-L1 and PD-L2 Expression. Cell Rep. 2017, 19, 1189–1201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Freeman, G.J.; Long, A.J.; Iwai, Y.; Bourque, K.; Chernova, T.; Nishimura, H.; Fitz, L.J.; Malenkovich, N.; Okazaki, T.; Byrne, M.C.; et al. Engagement of the Pd-1 Immunoinhibitory Receptor by a Novel B7 Family Member Leads to Negative Regulation of Lymphocyte Activation. J. Exp. Med. 2000, 192, 1027–1034. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirkwood, J.M.; Richards, T.; Zarour, H.M.; Sosman, J.; Ernstoff, M.; Whiteside, T.L.; Ibrahim, J.; Blum, R.; Wieand, S.; Mascari, R. Immunomodulatory effects of high-dose and low-dose interferon ?2b in patients with high-risk resected melanoma. Cancer 2002, 95, 1101–1112. [Google Scholar] [CrossRef] [PubMed]
- Tasseron, E.W.; Van Der Esch, E.P.; Hart, A.; De La Rivière, G.B.; Aartsen, E.J. A clinicopathological study of 30 melanomas of the vulva. Gynecol. Oncol. 1992, 46, 170–175. [Google Scholar] [CrossRef]
- Moxley, K.; Fader, A.; Rose, P.; Case, A.; Mutch, D.; Berry, E.; Schink, J.; Kim, C.; Chi, D.; Moore, K. Malignant melanoma of the vulva: An extension of cutaneous melanoma? Gynecol. Oncol. 2011, 122, 612–617. [Google Scholar] [CrossRef] [PubMed]
- Cancer-1 March 1993-Ragnarsson-Olding-Malignant Melanoma of the Vulva and Vagina Trends in Incidence Age.pdf. Available online: https://acsjournals.onlinelibrary.wiley.com/doi/abs/10.1002/1097-0142(19930301)71:5%3C1893::AID-CNCR2820710528%3E3.0.CO;2-7 (accessed on 30 August 2022).
- Weinstock, M.A. Malignant melanoma of the vulva and vagina in the United States: Patterns of incidence and popu lation-based estimates of survival. Am. J. Obstet. Gynecol. 1994, 171, 1225–1230. [Google Scholar] [CrossRef]
- Mert, I.; Semaan, A.; Winer, I.; Morris, R.T.; Ali-Fehmi, R. Vulvar/Vaginal Melanoma. Int. J. Gynecol. Cancer 2013, 23, 1118–1126. [Google Scholar] [CrossRef]
- Curtin, J.A.; Busam, K.; Pinkel, D.; Bastian, B.C. Somatic Activation of KIT in Distinct Subtypes of Melanoma. J. Clin. Oncol. 2006, 24, 4340–4346. [Google Scholar] [CrossRef]
- Willmore-Payne, C.; Holden, J.A.; Tripp, S.; Layfield, L.J. Human malignant melanoma: Detection of BRAF- and c-kit–activating mutations by high-resolution amplicon melting analysis. Hum. Pathol. 2005, 36, 486–493. [Google Scholar] [CrossRef] [PubMed]
- Hou, J.Y.; Baptiste, C.; Mbbs, R.B.H.; Tergas, A.I.; Feldman, R.; Jones, N.L.; Chatterjee-Paer, S.; Bus-Kwolfski, A.; Wright, J.D.; Burke, W.M. Vulvar and vaginal melanoma: A unique subclass of mucosal melanoma based on a comprehensive molecular analysis of 51 cases compared with 2253 cases of nongynecologic melanoma. Cancer 2017, 123, 1333–1344. [Google Scholar] [CrossRef]
- Udager, A.M.; Frisch, N.K.; Hong, L.J.; Stasenko, M.; Johnston, C.M.; Liu, J.R.; Chan, M.; Harms, P.; Fullen, D.R.; Orsini, A.; et al. Gynecologic melanomas: A clinicopathologic and molecular analysis. Gynecol. Oncol. 2017, 147, 351–357. [Google Scholar] [CrossRef]
- Aulmann, S.; Sinn, H.-P.; Penzel, R.; Gilks, C.B.; Schott, S.; Hassel, J.C.; Schmidt, D.; Kommoss, F.; Schirmacher, P.; Kommoss, S. Comparison of molecular abnormalities in vulvar and vaginal melanomas. Mod. Pathol. 2014, 27, 1386–1393. [Google Scholar] [CrossRef] [Green Version]
- Wohlmuth, C.; Wohlmuth-Wieser, I. Vulvar Melanoma: Molecular Characteristics, Diagnosis, Surgical Management, and Medical Treatment. Am. J. Clin. Dermatol. 2021, 22, 639–651. [Google Scholar] [CrossRef]
- Grunsven, A.C.V.E.-V.; Küsters-Vandevelde, H.V.; De Hullu, J.; van Duijn, L.M.; Rijntjes, J.; Bovée, J.V.; Groenen, P.J.; Blokx, W.A. NRAS mutations are more prevalent than KIT mutations in melanoma of the female urogenital tract—A study of 24 cases from the Netherlands. Gynecol. Oncol. 2014, 134, 10–14. [Google Scholar] [CrossRef]
- Saleh, B.; Kriegsmann, J.; Falk, S.; Aulmann, S. Frequent PD-L1 Expression in Malignant Melanomas of the Vulva. Int. J. Gynecol. Pathol. 2018, 37, 477–481. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.-Y.; Wu, X.-Y.; Zhang, X.; Yang, X.-H.; Long, Y.-K.; Feng, Y.-F.; Wang, F. Prevalence of NRAS Mutation, PD-L1 Expression and Amplification, and Overall Survival Analysis in 36 Primary Vaginal Melanomas. Oncologist 2020, 25, e291–e301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsai, K.K.; Zarzoso, I.; Daud, A.I. PD-1 and PD-L1 antibodies for melanoma. Hum. Vaccines Immunother. 2014, 10, 3111–3116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larkin, J.; Chiarion-Sileni, V.; Gonzalez, R.; Grob, J.-J.; Cowey, C.L.; Lao, C.D.; Schadendorf, D.; Dummer, R.; Smylie, M.; Rutkowski, P.; et al. Combined Nivolumab and Ipilimumab or Monotherapy in Untreated Melanoma. N. Engl. J. Med. 2015, 373, 23–34. [Google Scholar] [CrossRef] [Green Version]
- Wolchok, J.D.; Kluger, H.; Callahan, M.K.; Postow, M.A.; Rizvi, N.A.; Lesokhin, A.M.; Segal, N.H.; Ariyan, C.E.; Gordon, R.-A.; Reed, K.; et al. Nivolumab plus Ipilimumab in Advanced Melanoma. N. Engl. J. Med. 2013, 369, 122–133. [Google Scholar] [CrossRef] [Green Version]
- Wolchok, J.D.; Chiarion-Sileni, V.; Gonzalez, R.; Rutkowski, P.; Grob, J.-J.; Cowey, C.L.; Lao, C.D.; Wagstaff, J.; Schadendorf, D.; Ferrucci, P.F.; et al. Overall Survival with Combined Nivolumab and Ipilimumab in Advanced Melanoma. N. Engl. J. Med. 2017, 377, 1345–1356. [Google Scholar] [CrossRef]
- Larkin, J.; Chiarion-Sileni, V.; Gonzalez, R.; Grob, J.-J.; Rutkowski, P.; Lao, C.D.; Cowey, C.L.; Schadendorf, D.; Wagstaff, J.; Dummer, R.; et al. Five-Year Survival with Combined Nivolumab and Ipilimumab in Advanced Melanoma. N. Engl. J. Med. 2019, 381, 1535–1546. [Google Scholar] [CrossRef] [Green Version]
- Robert, C.; Long, G.V.; Brady, B.; Dutriaux, C.; Maio, M.; Mortier, L.; Hassel, J.C.; Rutkowski, P.; McNeil, C.; Kalinka-Warzocha, E.; et al. Nivolumab in Previously Untreated Melanoma without BRAF Mutation. N. Engl. J. Med. 2015, 372, 320–330. [Google Scholar] [CrossRef] [Green Version]
- Helgadottir, H.; Ghiorzo, P.; van Doorn, R.; Puig, S.; Levin, M.; Kefford, R.; Lauss, M.; Queirolo, P.; Pastorino, L.; Kapiteijn, E.; et al. Efficacy of novel immunotherapy regimens in patients with metastatic melanoma with germline CDKN2A mutations. J. Med. Genet. 2020, 57, 316–321. [Google Scholar] [CrossRef] [Green Version]
- Adib, E.; Nassar, A.H.; Akl, E.W.; Alaiwi, S.A.; Nuzzo, P.V.; Mouhieddine, T.H.; Sonpavde, G.; Haddad, R.I.; Mouw, K.W.; Giannakis, M.; et al. CDKN2A Alterations and Response to Immunotherapy in Solid Tumors. Clin. Cancer Res. 2021, 27, 4025–4035. [Google Scholar] [CrossRef]
- Horn, S.; Leonardelli, S.; Sucker, A.; Schadendorf, D.; Griewank, K.G.; Paschen, A. Tumor CDKN2A-Associated JAK2 Loss and Susceptibility to Immunotherapy Resistance. JNCI: J. Natl. Cancer Inst. 2018, 110, 677–681. [Google Scholar] [CrossRef] [PubMed]
- DeLeon, T.T.; Almquist, D.R.; Kipp, B.R.; Langlais, B.T.; Mangold, A.; Winters, J.L.; Kosiorek, H.E.; Joseph, R.W.; Dronca, R.S.; Block, M.S.; et al. Assessment of clinical outcomes with immune checkpoint inhibitor therapy in melanoma patients with CDKN2A and TP53 pathogenic mutations. PLoS ONE 2020, 15, e0230306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirchberger, M.C.; Ugurel, S.; Mangana, J.; Heppt, M.V.; Eigentler, T.K.; Berking, C.; Schadendorf, D.; Schuler, G.; Dummer, R.; Heinzerling, L. MEK inhibition may increase survival of NRAS-mutated melanoma patients treated with checkpoint blockade: Results of a retrospective multicentre analysis of 364 patients. Eur. J. Cancer 2018, 98, 10–16. [Google Scholar] [CrossRef]
- Hu-Lieskovan, S. Improved antitumor activity of immunotherapy with BRAF and MEK inhibitors in BRAFV600E melanoma. Cancer 2012, 17, 1310–1314. [Google Scholar]
- Eggermont, A.M.M.; Blank, C.U.; Mandala, M.; Long, G.V.; Atkinson, V.G.; Dalle, S.; Haydon, A.M.; Meshcheryakov, A.; Khattak, A.; Carlino, M.S.; et al. Longer Follow-Up Confirms Recurrence-Free Survival Benefit of Adjuvant Pembrolizumab in High-Risk Stage III Melanoma: Updated Results From the EORTC 1325-MG/KEYNOTE-054 Trial. J. Clin. Oncol. 2020, 38, 3925–3936. [Google Scholar] [CrossRef] [PubMed]
- Robert, C.; Ribas, A.; Schachter, J.; Arance, A.; Grob, J.-J.; Mortier, L.; Daud, A.; Carlino, M.S.; McNeil, C.M.; Lotem, M.; et al. Pembrolizumab versus ipilimumab in advanced melanoma (KEYNOTE-006): Post-hoc 5-year results from an open-label, multicentre, randomised, controlled, phase 3 study. Lancet Oncol. 2019, 20, 1239–1251. [Google Scholar] [CrossRef]
- Petrella, T.M.; Robert, C.; Richtig, E.; Miller, W.H.; Masucci, G.V.; Walpole, E.; Lebbe, C.; Steven, N.; Middleton, M.R.; Hille, D.; et al. Patient-reported outcomes in KEYNOTE-006, a randomised study of pembrolizumab versus ipilimumab in patients with advanced melanoma. Eur. J. Cancer 2017, 86, 115–124. [Google Scholar] [CrossRef]
- Carlino, M.S.; Long, G.V.; Schadendorf, D.; Robert, C.; Ribas, A.; Richtig, E.; Nyakas, M.; Caglevic, C.; Tarhini, A.; Blank, C.; et al. Outcomes by line of therapy and programmed death ligand 1 expression in patients with advanced melanoma treated with pembrolizumab or ipilimumab in KEYNOTE-006: A randomised clinical trial. Eur. J. Cancer 2018, 101, 236–243. [Google Scholar] [CrossRef] [Green Version]
- Daud, A.; Puzanov, I.; Dummer, R.; Schadendorf, D.; Hamid, O.; Robert, C.; Hodi, F.; Schachter, J.; Sosman, J.; Pavlick, A.; et al. Analysis of response and survival in patients (pts) with ipilimumab (ipi)-refractory melanoma treated with pembrolizumab (pembro) in KEYNOTE-002. Ann. Oncol. 2017, 28, v434. [Google Scholar] [CrossRef] [Green Version]
- Schadendorf, D.; Dummer, R.; Hauschild, A.; Robert, C.; Hamid, O.; Daud, A.; Eertwegh, A.V.D.; Cranmer, L.; O’Day, S.; Puzanov, I.; et al. Health-related quality of life in the randomised KEYNOTE-002 study of pembrolizumab versus chemotherapy in patients with ipilimumab-refractory melanoma. Eur. J. Cancer 2016, 67, 46–54. [Google Scholar] [CrossRef] [Green Version]
- Ribas, A.; Puzanov, I.; Dummer, R.; Schadendorf, D.; Hamid, O.; Robert, C.; Hodi, F.S.; Schachter, J.; Pavlick, A.C.; Lewis, K.D.; et al. Pembrolizumab versus investigator-choice chemotherapy for ipilimumab-refractory melanoma (KEYNOTE-002): A randomised, controlled, phase 2 trial. Lancet Oncol. 2015, 16, 908–918. [Google Scholar] [CrossRef] [Green Version]
- Albert, A.; Lee, A.; Allbright, R.; Vijayakumar, S. Vulvar melanoma: An analysis of prognostic factors and treatment patterns. J. Gynecol. Oncol. 2020, 31, e66. [Google Scholar] [CrossRef] [PubMed]
- D’Angelo, S.P.; Larkin, J.; Sosman, J.A.; Lebbé, C.; Brady, B.; Neyns, B.; Schmidt, H.; Hassel, J.C.; Hodi, F.S.; Lorigan, P.; et al. Efficacy and Safety of Nivolumab Alone or in Combination With Ipilimumab in Patients With Mucosal Melanoma: A Pooled Analysis. J. Clin. Oncol. 2017, 35, 226–235. [Google Scholar] [CrossRef]
- Hamid, O.; Robert, C.; Ribas, A.; Hodi, F.S.; Walpole, E.; Daud, A.; Arance, A.S.; Brown, E.; Hoeller, C.; Mortier, L.; et al. Antitumour activity of pembrolizumab in advanced mucosal melanoma: A post-hoc analysis of KEYNOTE-001, 002, 006. Br. J. Cancer 2018, 119, 670–674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Egger, E.K.; Stope, M.B.; Recker, F.; Konsgen, D.; Landsberg, J.; Frohlich, A.; Abramian, A.; Mustea, A. Lower Genital Tract Melanomas: Staging, Predictors of Outcome, and New Therapeutic Options. Anticancer Res. 2021, 41, 999–1004. [Google Scholar] [CrossRef]
- Tasaka, R.; Fukuda, T.; Wada, T.; Kawanishi, M.; Imai, K.; Kasai, M.; Hashiguchi, Y.; Ichimura, T.; Yasui, T.; Sumi, T. A retrospective clinical analysis of 5 cases of vaginal melanoma. Mol. Clin. Oncol. 2017, 6, 373–376. [Google Scholar] [CrossRef] [Green Version]
- Wilhite, A.; Wu, S.; Xiu, J.; Korn, W.M.; Phung, T.; Herzog, T.; In, G.; Gibney, G.; Brown, J.; Rocconi, R.; et al. Too much skin in the game? A paradigm shift in our understanding of vulvar and vaginal melanomas as distinct tumor types compared with cutaneous melanomas. Gynecol. Oncol. 2021, 162, S33–S34. [Google Scholar] [CrossRef]
- Skovsted, S.; Nielsen, K.; Blaakær, J. Melanomas of the vulva and vagina. Dan. Med. J. 2017, 64. [Google Scholar]
- Boer, F.L.; Eikelder, M.L.T.; van Geloven, N.; Kapiteijn, E.H.; Gaarenstroom, K.N.; Hughes, G.; Nooij, L.S.; Jozwiak, M.; Tjiong, M.Y.; de Hullu, J.M.; et al. Evaluation of treatment, prognostic factors, and survival in 198 vulvar melanoma patients: Implications for clinical practice. Gynecol. Oncol. 2021, 161, 202–210. [Google Scholar] [CrossRef]
- Palareti, G.; Legnani, C.; Cosmi, B.; Antonucci, E.; Erba, N.; Poli, D.; Testa, S. The DULCIS (D-Dimer-ULtrasonography In Combination Italian Study) Investigators. Comparison between different D-Dimer cutoff values to assess the individual risk of recurrent venous thromboembolism: Analysis of results obtained in the DULCIS study. Int. J. Lab. Hematol. 2016, 38, 42–49. [Google Scholar] [CrossRef]
- Chłopik, A.; Selim, M.A.; Peng, Y.; Wu, C.-L.; Tell-Marti, G.; Paral, K.M.; Shalin, S.C.; Kraft, S.; Hsu, C.-K.; Shea, C.R.; et al. Prognostic role of tumoral PDL1 expression and peritumoral FoxP3+ lymphocytes in vulvar melanomas. Hum. Pathol. 2018, 73, 176–183. [Google Scholar] [CrossRef]
- Indini, A.; Di Guardo, L.; Cimminiello, C.; Lorusso, D.; Raspagliesi, F.; Del Vecchio, M. Investigating the role of immunotherapy in advanced/recurrent female genital tract melanoma: A preliminary experience. J. Gynecol. Oncol. 2019, 30, e94. [Google Scholar] [CrossRef] [PubMed]
- Sezen, D.; Patel, R.R.; Tang, C.; Onstad, M.; Nagarajan, P.; Patel, S.P.; Welsh, J.W.; Lin, L.L. Immunotherapy combined with high- and low-dose radiation to all sites leads to complete clearance of disease in a patient with metastatic vaginal melanoma. Gynecol. Oncol. 2021, 161, 645–652. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Song, J.; Sun, Y.; Cui, Z. Multiple metastases after surgery for a rare vulvar malignant melanoma combined with immunotherapy: A case report. J. Int. Med. Res. 2020, 48, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Chanal, J.; Kramkimel, N.; Guegan, S.; Moguelet, P.; Fourchotte, V.; Avril, M.-F. Locally Advanced Unresectable Vaginal Melanoma: Response With Anti–Programmed Death Receptor 1. J. Low. Genit. Tract Dis. 2016, 20, e4–e5. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Survival (%) | Diagnosis (%) | Stage of Neoplasm in SEER Staging |
|---|---|---|
| 95 | 70 | I |
| 70 | 15.2 | II |
| 46 | 9.8 | III |
| 12 | 5 | IV |
| Vaginal Melanoma (%) | Vulvar Melanoma (%) | |||
|---|---|---|---|---|
| Overall Survival | Percent of Diagnosed with Given Stage | Overall Survival | Percent of Diagnosed with Given Stage | Stage of Neoplasm in SEER Staging |
| 23.3 | 36.7 | 70.6 | 52.6 | localized |
| 21.2 | 21.4 | 35.4 | 24.9 | regional |
| 6.3 | 25.1 | 13.4 | 6.7 | distant |
| 17.9 | 16.8 | 59.4 | 15.8 | unstaged |
| Treatment Response | Progression-Free Survival (Months) | Median Overall Survival | References |
|---|---|---|---|
| % | |||
| 43.7 (nivolumab) | 6.9 (nivolumab) | nd | Larkin et al. [37] |
| 57.6 (combined) | 11.5 (combined) | ||
| 19 (ipilimumab) | 2.9 (ipilimumab) | ||
| 40 | nd | nd | Wolchok et al. [38] |
| 44 (nivolumab) | nd | 37.6 (nivolumab) | Wolchok et al. [39] |
| 58 (combined) | 19.9 (ipilimumab) | ||
| 19 (ipilimumab) | not reached (combined) | ||
| 45 (nivolumab) | 6.9 (nivolumab) | 36.9 (nivolumab) | Larkin et al. [40] |
| 58 (combined) | 11.5 (combined) | 19.9 (ipilimumab) | |
| 19 (ipilimumab) | 2.9 (ipilimumab) | not reached (combined) | |
| 40 (nivolumab) | 5.1 (nivolumab) | Robert et al. [41] | |
| 13 (dacarbazine) | 2.2 (dacarbazine) | ||
| 58 | nd | nd | Helgadottir et al. [42] |
| Statistically insignificant | nd | 27.2 (with mutation) | Adib et al. [43] |
| not reached(without mutation) | |||
| 47.4 (TP53 mut) vs. 34.3(TP53 WT) | nd | 8.0 (TP53 mut) vs. 6.0 (TP53 WT) | DeLeon et al. [45] |
| 45.5 (CDKN2A mut) vs. 36% (CDKN2A WT) | 14.0 (CDKN2A mut) vs. 6.0 (CDKN2A WT) | ||
| Ipilimumab—15 (mutation) vs. 13 (WT) | 3 | 21.0 (NRAS mutation) | Kirchberger et al. [46] |
| monotherapy anti-PD-L1—21 (mutation) vs. 13 (WT) | 33.0 (NRAS wild type) | ||
| combined 40 (mutation) vs. 39 (WT) | |||
| RFS after 3-years—63.7% (pembrolizumab) vs. 44.1 (placebo) | Eggermont et al. [48] | ||
| 42 (combined pembrolizumab) | 8.4 (combined pembrolizumab) | 32.7 (combined pembrolizumab) | Robert et al. [54] |
| 17 (ipilimumab) | 3.4 (ipilimumab) | 15.9 (ipilimumab) | |
| 39.4 (pembrolizumab) | T-N: 6.6 (pembrolizumab) vs. 2.8 (ipilimumab) | T-N—not reached (pembrolizumab) vs. 17.1 (ipilimumab) | Carlino et al. [50] |
| 13.3 (ipilimumab) | P-T: 2.9 (pembrolizumab) vs. 2.8 (ipilimumab) | P-T—23.5 (pembrolizumab) vs. 13.6 (ipilimumab) |
| Treatment Response (%) | Progression-Free Survival (Months) | Median Overall Survival (Months) | References |
|---|---|---|---|
| 33 | nd | 55.8 (L) | Albert et al. [63] |
| 22.2 (R) | |||
| 5.1 (D) | |||
| 34.1 | nd | 19 (VVM) | Wilhite et al. [68] |
| 37 (CM) | |||
| 45 | 11(with immunotherapy) | 16 | Boer et al. [70] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lorenz, A.; Kozłowski, M.; Lenkiewicz, S.; Kwiatkowski, S.; Cymbaluk-Płoska, A. Cutaneous Melanoma versus Vulvovaginal Melanoma—Risk Factors, Pathogenesis and Comparison of Immunotherapy Efficacy. Cancers 2022, 14, 5123. https://doi.org/10.3390/cancers14205123
Lorenz A, Kozłowski M, Lenkiewicz S, Kwiatkowski S, Cymbaluk-Płoska A. Cutaneous Melanoma versus Vulvovaginal Melanoma—Risk Factors, Pathogenesis and Comparison of Immunotherapy Efficacy. Cancers. 2022; 14(20):5123. https://doi.org/10.3390/cancers14205123
Chicago/Turabian StyleLorenz, Anna, Mateusz Kozłowski, Sebastian Lenkiewicz, Sebastian Kwiatkowski, and Aneta Cymbaluk-Płoska. 2022. "Cutaneous Melanoma versus Vulvovaginal Melanoma—Risk Factors, Pathogenesis and Comparison of Immunotherapy Efficacy" Cancers 14, no. 20: 5123. https://doi.org/10.3390/cancers14205123