
The Diagnostic Value of the CA19-9 and Bilirubin Ratio in Patients with Pancreatic Cancer, Distal Bile Duct Cancer and Benign Periampullary Diseases, a Novel Approach

 , , , , ,
, , , , ,  , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population and Design
2.2. Detection of CA19-9 and Bilirubin Levels
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Characteristics of the Subset of Patients for Calculation of the CA19-9 and Bilirubin Ratio
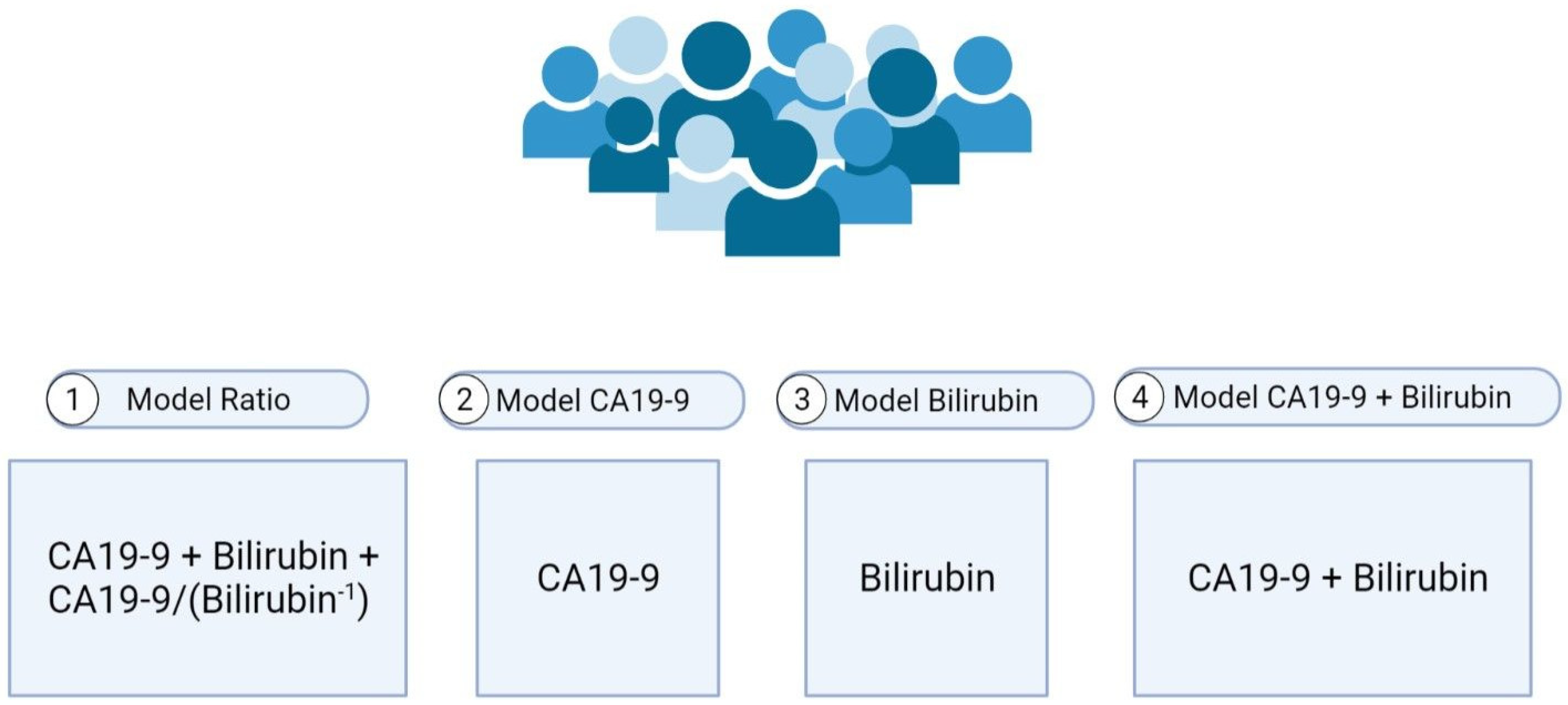
3.3. Prediction Models
3.4. Comparisons of the Prediction Models
3.5. Model Ratio ROC Curves
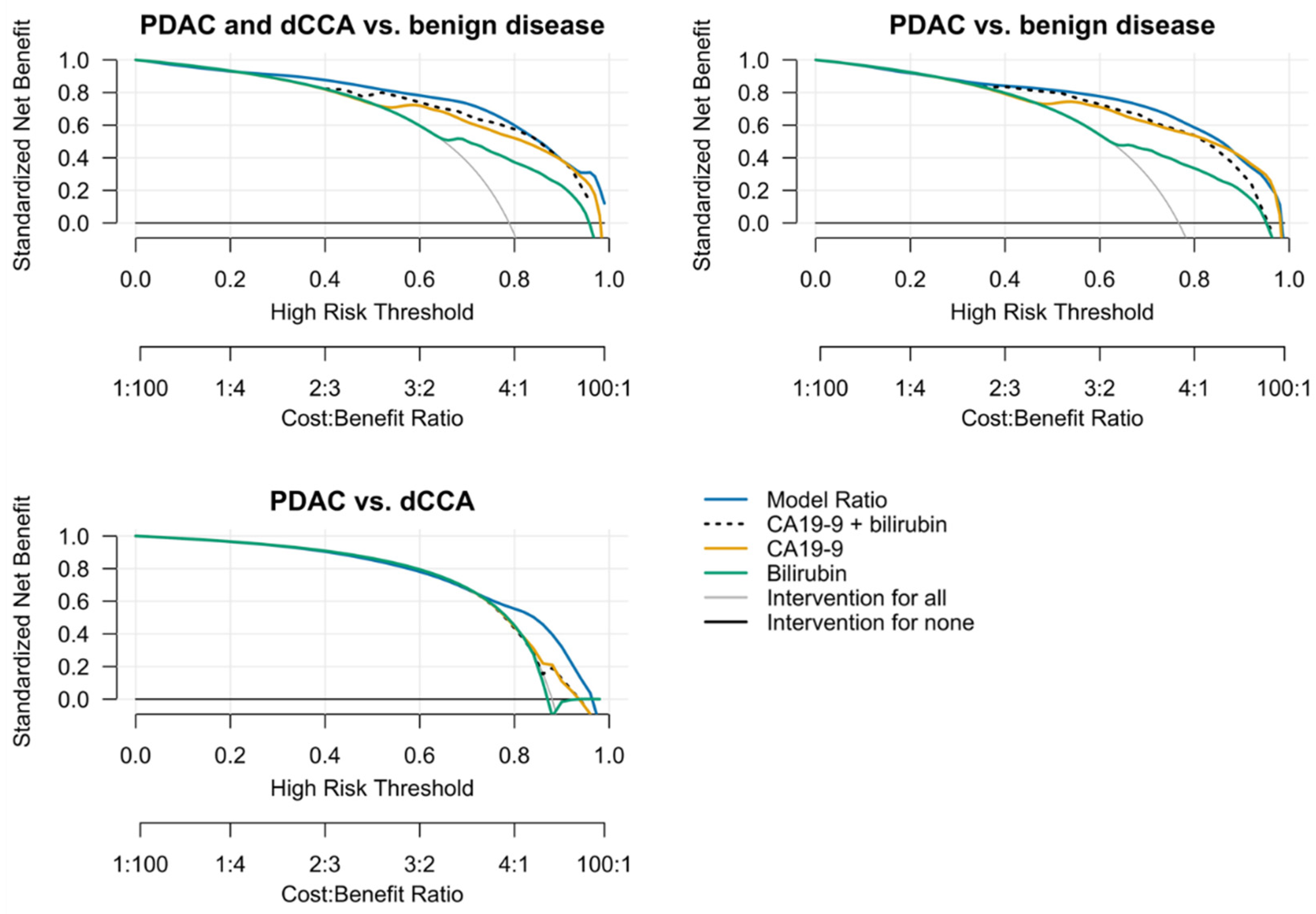
3.6. Standardized Net Benefit Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| PDAC | Pancreatic ductal adenocarcinoma |
| dCCA | Distal cholangiocarcinoma |
| AUC | Area Under the Curve |
| ctDNA | Circulating tumour DNA |
| TEPs | Tumour-educated platelets |
| miRNAs | MicroRNAs |
| ULN | Upper limit of normal |
| IPMN | Intraductal papillary mucinous neoplasm |
| RCS | Restricted cubic splines |
| MFP | Multivariable fractional polynomials |
| SEN | Sensitivity |
| SPE | Specificity |
| PPV | Positive predictive value |
| NPV | Negative predictive value |
References
- Cancer Statistics—Cancer Stat Facts: Pancreatic Cancer. Available online: https://seer.cancer.gov/statfacts/html/pancreas.html (accessed on 8 October 2021).
- Boyd, L.N.C.; Andini, K.D.; Peters, G.J.; Kazemier, G.; Giovannetti, E. Heterogeneity and Plasticity of Cancer-Associated Fibroblasts in the Pancreatic Tumor Microenvironment. In Seminars in Cancer Biology; Academic Press: Cambridge, MA, USA, 2021. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics. CA A Cancer J. Clin. 2021, 71, 7–33. [Google Scholar]
- Blackford, A.L.; Canto, M.I.; Klein, A.P.; Hruban, R.H.; Goggins, M. Recent Trends in the Incidence and Survival of Stage 1A Pancreatic Cancer: A Surveillance, Epidemiology, and End Results Analysis. JNCI J. Natl. Cancer Inst. 2020, 112, 1162–1169. [Google Scholar] [CrossRef] [PubMed]
- Schmuck, R.B.; Carvalho-Fischer, C.V.; Neumann, C.; Pratschke, J.; Bahra, M. Distal Bile Duct Carcinomas and Pancreatic Ductal Adenocarcinomas: Postulating a Common Tumor Entity. Cancer Med. 2016, 5, 88–99. [Google Scholar] [CrossRef]
- Ethun, C.G.; Lopez-Aguiar, A.G.; Pawlik, T.M.; Poultsides, G.; Idrees, K.; Fields, R.C.; Weber, S.M.; Cho, C.; Martin, R.C.; Scoggins, C.R.; et al. Distal Cholangiocarcinoma and Pancreas Adenocarcinoma: Are They Really the Same Disease? A 13-Institution Study from the US Extrahepatic Biliary Malignancy Consortium and the Central Pancreas Consortium. J. Am. Coll. Surg. 2017, 224, 406–413. [Google Scholar] [CrossRef] [PubMed]
- Gerritsen, A.; Molenaar, I.; Bollen, T.; Nio, C.; Dijkgraaf, M.; van Santvoort, H.; Offerhaus, G.; Brosens, L.; Biermann, K.; Sieders, E.; et al. Preoperative Characteristics of Patients with Presumed Pancreatic Cancer but Ultimately Benign Disease: A Multicenter Series of 344 Pancreatoduodenectomies. Ann. Surg. Oncol. 2014, 21, 3999–4006. [Google Scholar] [CrossRef]
- Van Heerde, M.; Buijs, J.; Hansen, B.; de Waart, M.; van Eijck, C.; Kazemier, G.; Pek, C.; Poley, J.; Bruno, M.; Kuipers, E.; et al. Serum Level of Ca 19-9 Increases Ability of Igg4 Test to Distinguish Patients with Autoimmune Pancreatitis from Those with Pancreatic Carcinoma. Dig. Dis. Sci. 2014, 59, 1322–1329. [Google Scholar] [CrossRef] [PubMed]
- Crinò, S.F.; Di Mitri, R.; Nguyen, N.Q.; Tarantino, I.; de Nucci, G.; Deprez, P.H.; Carrara, S.; Kitano, M.; Shami, V.M.; Fernández-Esparrach, G.; et al. Endoscopic Ultrasound-Guided Fine-Needle Biopsy With or without Rapid On-Site Evaluation for Diagnosis of Solid Pancreatic Lesions: A Randomized Controlled Non-Inferiority Trial. Gastroenterology 2021, 161, 899–909.e5. [Google Scholar] [CrossRef] [PubMed]
- Doherty, B.; Nambudiri, V.E.; Palmer, W.C. Update on the Diagnosis and Treatment of Cholangiocarcinoma. Curr. Gastroenterol. Rep. 2017, 19, 2. [Google Scholar] [CrossRef] [PubMed]
- Tsen, A.; Barbara, M.; Rosenkranz, L. Dilemma of Elevated CA 19-9 in Biliary Pathology. Pancreatology 2018, 18, 862–867. [Google Scholar] [CrossRef] [PubMed]
- Bolm, L.; Petrova, E.; Weitz, J.; Rückert, F.; Wittel, U.A.; Makowiec, F.; Lapshyn, H.; Bronsert, P.; Rau, B.M.; Khatkov, I.E.; et al. Prognostic Relevance of Preoperative Bilirubin-Adjusted Serum Carbohydrate Antigen 19-9 in a Multicenter Subset Analysis of 179 Patients with Distal Cholangiocarcinoma. HPB 2019, 21, 1513–1519. [Google Scholar] [CrossRef]
- Tempero, M.A.; Uchida, E.; Takasaki, H.; Burnett, D.A.; Steplewski, Z.; Pour, P.M. Relationship of Carbohydrate Antigen 19-9 and Lewis Antigens in Pancreatic Cancer. Cancer Res. 1987, 47, 5501–5503. [Google Scholar] [PubMed]
- Zhang, Y.; Yang, J.; Li, H.; Wu, Y.; Zhang, H.; Chen, W. Tumor Markers CA19-9, CA242 and CEA in the Diagnosis of Pancreatic Cancer: A Meta-Analysis. Int. J. Clin. Exp. Med. 2015, 8, 11683. [Google Scholar] [PubMed]
- Skulimowski, A.; Durczyński, A.; Strzelczyk, J.; Hogendorf, P. Comparison of Clinical Usefulness of Serum Ca125 and CA19-9 in Pancreatic Adenocarcinoma Diagnosis: Meta-Analysis and Systematic Review of Literature. Biomarkers 2021, 26, 287–295. [Google Scholar] [CrossRef]
- Huang, Z.; Liu, F. Diagnostic Value of Serum Carbohydrate Antigen 19-9 in Pancreatic Cancer: A Meta-Analysis. Tumor Biol. 2014, 35, 7459–7465. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Yan, S.; Tian, H.; Bao, Y. Macrophage Inhibitory Cytokine-1 versus Carbohydrate Antigen 19-9 as a Biomarker for Diagnosis of Pancreatic Cancer: A PRISMA-Compliant Meta-Analysis of Diagnostic Accuracy Studies. Medicine 2018, 97, e9994. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Park, B.; Seo, J.; Choi, J.; Choi, J.; Lee, C.; Chung, J.; Park, Y.; Kim, D. Carbohydrate Antigen 19-9 Elevation Without Evidence Of Malignant Or Pancreatobiliary Diseases. Sci. Rep. 2020, 10, 8820. [Google Scholar] [CrossRef]
- Detecting Cancers Earlier Through Elective Plasma-Based CancerSEEK Testing ClinicalTrials.gov. Available online: https://clinicaltrials.gov/ct2/show/NCT04213326 (accessed on 8 October 2021).
- Le Large, T.Y.; Meijer, L.L.; Paleckyte, R.; Boyd, L.N.; Kok, B.; Wurdinger, T.; Schelfhorst, T.; Piersma, S.R.; Pham, T.V.; van Grieken, N.C.; et al. Combined Expression of Plasma Thrombospondin-2 and CA19-9 for Diagnosis of Pancreatic Cancer and Distal Cholangiocarcinoma: A Proteome Approach. Oncologist 2020, 25, e634–e643. [Google Scholar] [CrossRef] [Green Version]
- Meijer, L.L.; Puik, J.R.; Le Large, T.Y.S.; Heger, M.; Dijk, F.; Funel, N.; Wurdinger, T.; Garajová, I.; van Grieken, N.C.T.; van de Wiel, M.A.; et al. Unravelling the Diagnostic Dilemma: A MicroRNA Panel of Circulating Mir-16 and Mir-877 as a Diagnostic Classifier for Distal Bile Duct Tumors. Cancers 2019, 11, 1181. [Google Scholar] [CrossRef] [Green Version]
- Mantini, G.; Meijer, L.L.; Glogovitis, I.; In ‘t Veld, S.G.; Paleckyte, R.; Capula, M.; Le Large, T.Y.; Morelli, L.; Pham, T.V.; Piersma, S.R.; et al. Omics Analysis of Educated Platelets in Cancer and Benign Disease of the Pancreas. Cancers 2020, 13, 66. [Google Scholar] [CrossRef]
- Kern, S.E. Why Your New Cancer Biomarker May Never Work: Recurrent Patterns and Remarkable Diversity in Biomarker Failures. Cancer Res. 2012, 72, 6097–6101. [Google Scholar] [CrossRef] [Green Version]
- La Greca, G.; Sofia, M.; Lombardo, R.; Latteri, S.; Ricotta, A.; Puleo, S.; Russello, D. Adjusting CA19-9 Values to Predict Malignancy in Obstructive Jaundice: Influence of Bilirubin and C-Reactive Protein. World J. Gastroenterol. 2012, 18, 4150–4155. [Google Scholar] [CrossRef]
- Ong, S.L.; Sachdeva, A.; Garcea, G.; Gravante, G.; Metcalfe, M.S.; Lloyd, D.M.; Berry, D.P.; Dennison, A.R. Elevation of CarboHydrate Antigen 19.9 in Benign Hepatobiliary Conditions and its Correlation with Serum Bilirubin Concentration. Dig. Dis. Sci. 2008, 53, 3213–3217. [Google Scholar] [CrossRef]
- Sullivan, J.I.; Rockey, D.C. Diagnosis and Evaluation of Hyperbilirubinemia. Curr. Opin. Gastroenterol. 2017, 33, 164–170. [Google Scholar] [CrossRef]
- Garcea, G.; Ngu, W.; Neal, C.P.; Dennison, A.R.; Berry, D.P. Bilirubin Levels Predict Malignancy in Patients with Obstructive Jaundice. HPB 2011, 13, 426–430. [Google Scholar] [CrossRef] [Green Version]
- Mann, D.V.; Edwards, R.; Ho, S.; Lau, W.Y.; Glazer, G. Elevated Tumour Marker CA19-9: Clinical Interpretation and Influence of Obstructive Jaundice. Eur. J. Surg. Oncol. 2000, 26, 474–479. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Liu, Q.; Wang, W.; Wang, P.; Chen, J.; Hong, T.; Zhang, N.; Li, B.; Qu, Q.; He, X. Differential Diagnostic Roles of the Serum CA19-9, Total Bilirubin (TBIL) and the Ratio of CA19-9 to TBIL for Benign and Malignant. J. Cancer. 2018, 9, 1804–1812. [Google Scholar] [CrossRef] [Green Version]
- Li, J.; Chen, Q.; Jin, B.; Shi, Y.; Wu, X.; Xu, H.; Zheng, Y.; Wang, Y.; Du, S.; Lu, X.; et al. Preoperative Bilirubin-Adjusted Carbohydrate Antigen 19-9 as a Prognostic Factor for Extrahepatic Cholangiocarcinoma Patients at a Single Center. Cancer Manag. Res. 2020, 12, 411–417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kang, C.M.; Kim, J.Y.; Choi, G.H.; Kim, K.S.; Choi, J.S.; Lee, W.J.; Kim, B.R. The Use of Adjusted Preoperative CA 19-9 to Predict the Recurrence of Resectable Pancreatic Cancer. J. Surg. Res. 2007, 140, 31–35. [Google Scholar] [CrossRef] [PubMed]
- Kronmal, R.A. Spurious Correlation and the Fallacy of the Ratio Standard Revisited. J. R. Stat. Soc. Ser. A 1993, 156, 379–392. [Google Scholar] [CrossRef]
- Austin, P.C.; Steyerberg, E.W. The Integrated Calibration Index (ICI) and Related Metrics for Quantifying the Calibration of Logistic Regression Models. Stat. Med. 2019, 38, 4051–4065. [Google Scholar] [CrossRef] [Green Version]
- Vickers, A.J.; Elkin, E.B. Decision Curve Analysis: A Novel Method for Evaluating Prediction Models. Med. Decis. Mak. 2006, 26, 565–574. [Google Scholar] [CrossRef] [Green Version]
- Fitzgerald, M.; Saville, B.R.; Lewis, R.J. Decision Curve Analysis. JAMA 2015, 313, 409–410. [Google Scholar] [CrossRef]
- Singh, H.; Perez, K.; Wolpin, B.; Aguirre, A. Beyond The Front Line: Emerging Data For Maintenance Therapy In Pancreatic Cancer. J. Clin. Oncol. 2021, 39, 3199–3206. [Google Scholar] [CrossRef]
- Vickers, A.J.; Van Calster, B.; Steyerberg, E. Net Benefit Approaches to the Evaluation of Prediction Models, Molecular Markers, and Diagnostic Tests. BMJ 2016, 352, i6. [Google Scholar] [CrossRef] [Green Version]
- Steyerberg, E.W. Evaluation of Clinical Usefulness. In Clinical Prediction Models; Springer International Publishing: Berlin/Heidelberg, Germany, 2019; pp. 309–328. [Google Scholar]
- Harrell, F.E., Jr. Regression Modeling Strategies: With Applications to Linear Models, Logistic and Ordinal Regression, and Survival Analysis; Springer: Berlin/Heidelberg, Germany, 2015. [Google Scholar]
- Moons, K.; Altman, D.; Reitsma, J.; Ioannidis, J.; Macaskill, P.; Steyerberg, E.; Vickers, A.; Ransohoff, D.; Collins, G. Transparent Reporting Of A Multivariable Prediction Model For Individual Prognosis Or Diagnosis (TRIPOD): Explanation And Elaboration. Ann. Intern. Med. 2015, 162, W1–W73. [Google Scholar] [CrossRef] [Green Version]
- Staal, B.; Liu, Y.; Barnett, D.; Hsueh, P.; He, Z.; Gao, C.; Partyka, K.; Hurd, M.; Singhi, A.; Drake, R.; et al. The Stra Plasma Biomarker: Blinded Validation of Improved Accuracy over CA19-9 in Pancreatic Cancer Diagnosis. Clin. Cancer Res. 2019, 25, 2745–2754. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mayerle, J.; Kalthoff, H.; Reszka, R.; Kamlage, B.; Peter, E.; Schniewind, B.; González Maldonado, S.; Pilarsky, C.; Heidecke, C.; Schatz, P.; et al. Metabolic Biomarker Signature To Differentiate Pancreatic Ductal Adenocarcinoma From Chronic Pancreatitis. Gut 2017, 67, 128–137. [Google Scholar] [CrossRef] [PubMed]
- Caputo, D.; Digiacomo, L.; Cascone, C.; Pozzi, D.; Palchetti, S.; Di Santo, R.; Quagliarini, E.; Coppola, R.; Mahmoudi, M.; Caracciolo, G. Synergistic Analysis Of Protein Corona And Haemoglobin Levels Detects Pancreatic Cancer. Cancers 2020, 13, 93. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Patients ≥ 18 year Informed consent | Patients < 18 year No consent |
| Included tumours: Distal cholangiocarcinoma (dCCA) Pancreatic ductal adenocarcinoma (PDAC) Histopathologically confirmed | Excluded tumours: Hepatocellular carcinoma (HCC) Gallbladder cancer Metastases from other primary malignancies Not histopathologically confirmed |
| Included benign diseases: Cholangitis on basis of choledocholithiasis Chronic pancreatitis Intraductal Papillary Mucinous Neoplasm (IPMN) Pancreatic lipomas Pancreatic cysts Benign CBD stenosis | Excluded benign diseases: Primary Sclerosing Cholangitis (PSC) Hepatitis Liver cirrhosis Neuroendocrine tumours Cholecystitis IgG4 autoimmune pancreatitis |
| Characteristic | PDAC (n = 178) | Distal CCA (n = 34) | Benign Disease (n = 53) | p Value |
|---|---|---|---|---|
| Age, mean (SD)—yr | 68.1 (9.5) | 69.4 (10.0) | 65.3 (12.4) | 0.233 |
| Sex—n (%) | 0.617 | |||
| Female | 84 (47.2) | 15 (44.1) | 21 (39.6) | |
| Male | 94 (52.8) | 19 (55.9) | 32 (60.4) | |
| Tumor stage—n (%) | 0.956 | |||
| Stage I-II | 116 (65.2) | 22 (64.7) | 0 (0) | |
| Stage III-IV | 62 (34.8) | 12 (35.3) | 0 (0) | |
| N/A | 0 (0) | 0 (0) | 53 (100) | |
| CA19-9, median (IQR) - U/mL | 243 (72–963) | 104 (43–292) | 15 (6–39) | <0.0001 |
| CA19-9—n (%) | <0.0001 | |||
| Normal | 29 (16.3) | 27 (79.4) | 39 (73.6) | |
| Elevated | 149 (83.7) | 7 (20.6) | 14 (26.4) | |
| Bilirubin, median (IQR) - μmol/L | 38 (10–156) | 85 (27–169) | 7 (6–13) | <0.0001 |
| Bilirubin—n (%) | <0.0001 | |||
| Normal | 79 (44.4) | 5 (14.7) | 45 (84.9) | |
| Elevated | 99 (55.6) | 29 (85.3) | 8 (15.1) |
| Characteristic | PDAC (n = 161) | Distal CCA (n = 22) | Benign Disease (n = 49) | p Value |
|---|---|---|---|---|
| Age, mean (SD)—yr | 68.8 (9.1) | 69.9 (10.3) | 66.3 (12.1) | 0.384 |
| Sex—n (%) | 0.283 | |||
| Female | 79 (49.1) | 9 (40.9) | 18 (36.7) | |
| Male | 82 (50.9) | 13 (59.1) | 31 (63.3) | |
| Tumor stage—n (%) | 0.979 | |||
| Stage I-II | 102 (63.4) | 14 (63.6) | 0 (0) | |
| Stage III-IV | 59 (36.6) | 8 (36.4) | 0 (0) | |
| N/A | 0 (0) | 0 (0) | 49 (100) | |
| CA19-9, median (IQR) - U/mL | 300 (75–1059) | 80 (32–164) | 15 (6–39) | <0.0001 |
| CA19-9—n (%) | <0.0001 | |||
| Normal | 24 (14.9) | 15 (68.2) | 36 (73.5) | |
| Elevated | 137 (85.1) | 7 (31.8) | 13 (26.5) | |
| Bilirubin, median (IQR) - μmol/L | 38 (10–171) | 78 (22–140) | 7 (6–12) | <0.0001 |
| Bilirubin—n (%) | <0.0001 | |||
| Normal | 71 (44.1) | 4 (18.2) | 42 (85.7) | |
| Elevated | 90 (55.9) | 18 (81.8) | 7 (14.3) |
| Comparison | Model Ratio | Model CA19-9 | Model Bilirubin | Model CA19-9 + Bilirubin |
|---|---|---|---|---|
| PDAC and dCCA vs. benign disease—n = 183 vs. 49 | ||||
| AUC (95% CI) | 0.906 (0.863–0.949) | 0.849 (0.796–0.902) | 0.770 (0.703–0.837) | 0.897 (0.852–0.943) |
| Cut-off | 0.712 | 37 U/mL | 20 μmol/L | 0.508 |
| SEN (95% CI) | 90.0 | 83.1 (77.6–88.5) | 59.0 (51.9–66.1) | 90.0 |
| SPE (95% CI) | 77.6 (65.3–87.8) | 73.5 (61.2–85.7) | 85.7 (75.5–93.9) | 65.3 (53.1–77.6) |
| Accuracy (95% CI) | 87.4 (83.2–91.4) | 81.0 (75.9–86.2) | 64.7 (58.6–70.3) | 84.1 (79.3–88.4) |
| ICI (95% CI) | 0.029 (0.014–0.061) | 0.047 (0.014–0.088) | 0.048 (0.015–0.088) | 0.060 (0.028–0.091) |
| PDAC vs. benign disease—n = 161 vs. 49 | ||||
| AUC (95% CI) | 0.914 (0.874–0.955) | 0.858 (0.806–0.910) | 0.754 (0.684–0.824) | 0.901 (0.856–0.945) |
| Cut-off | 0.629 | 37 U/mL | 20 μmol/L | 0.455 |
| SEN (95% CI) | 90.0 | 85.1 (79.5–90.1) | 55.9 (48.5–63.4) | 90.0 |
| SPE (95% CI) | 80.0 (67.4–89.8) | 73.5 (61.2–85.7) | 85.7 (75.5–93.9) | 65.3 (51.0–77.6) |
| Accuracy (95% CI) | 87.1 (82.4–91.4) | 82.4 (77.1–87.6) | 62.9 (56.7–69.1) | 84.3 (79.5–89.1) |
| ICI (95% CI) | 0.019 (0.016–0.069) | 0.046 (0.022–0.094) | 0.045 (0.024–0.098) | 0.053 (0.029–0.094) |
| PDAC vs. distal CCA—n = 161 vs. 22 | ||||
| AUC (95% CI) | 0.828 (0.740–0.915) | 0.689 (0.581–0.796) | 0.582 (0.486–0.678) | 0.655 (0.549–0.761) |
| Cut-off | 0.900 | 37 U/mL | 20 μmol/L | 0.868 |
| SEN (95% CI) | 64.6 (57.1–72.1) | 85.1 (79.5–90.1) | 44.1 (36.0–51.6) | 52.8 (45.3–60.3) |
| SPE (95% CI) | 90.9 (77.3–100.0) | 31.8 (13.6–50.0) | 81.8 (63.6–95.5) | 81.8 (63.6–95.5) |
| Accuracy (95% CI) | 67.8 (61.2–74.3) | 78.7 (73.2–84.2) | 48.6 (41.5–55.2) | 56.3 (49.2–63.4) |
| ICI (95% CI) | 0.027 (0.014–0.060) | 0.062 (0.016–0.109) | 0.061 (0.029–0.104) | 0.044 (0.012–0.097) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boyd, L.N.C.; Ali, M.; Kam, L.; Puik, J.R.; Rodrigues, S.M.F.; Zwart, E.S.; Daams, F.; Zonderhuis, B.M.; Meijer, L.L.; Le Large, T.Y.S.; et al. The Diagnostic Value of the CA19-9 and Bilirubin Ratio in Patients with Pancreatic Cancer, Distal Bile Duct Cancer and Benign Periampullary Diseases, a Novel Approach. Cancers 2022, 14, 344. https://doi.org/10.3390/cancers14020344
Boyd LNC, Ali M, Kam L, Puik JR, Rodrigues SMF, Zwart ES, Daams F, Zonderhuis BM, Meijer LL, Le Large TYS, et al. The Diagnostic Value of the CA19-9 and Bilirubin Ratio in Patients with Pancreatic Cancer, Distal Bile Duct Cancer and Benign Periampullary Diseases, a Novel Approach. Cancers. 2022; 14(2):344. https://doi.org/10.3390/cancers14020344
Chicago/Turabian StyleBoyd, Lenka N. C., Mahsoem Ali, Laura Kam, Jisce R. Puik, Stephanie M. Fraga Rodrigues, Eline S. Zwart, Freek Daams, Barbara M. Zonderhuis, Laura L. Meijer, Tessa Y. S. Le Large, and et al. 2022. "The Diagnostic Value of the CA19-9 and Bilirubin Ratio in Patients with Pancreatic Cancer, Distal Bile Duct Cancer and Benign Periampullary Diseases, a Novel Approach" Cancers 14, no. 2: 344. https://doi.org/10.3390/cancers14020344