


Development of a Prognostic Model of Overall Survival for Metastatic Hormone-Naïve Prostate Cancer in Japanese Men
 ,
,  , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Collection of Clinical Data
2.3. Statistical Analyses
2.4. Ethical Considerations
3. Results
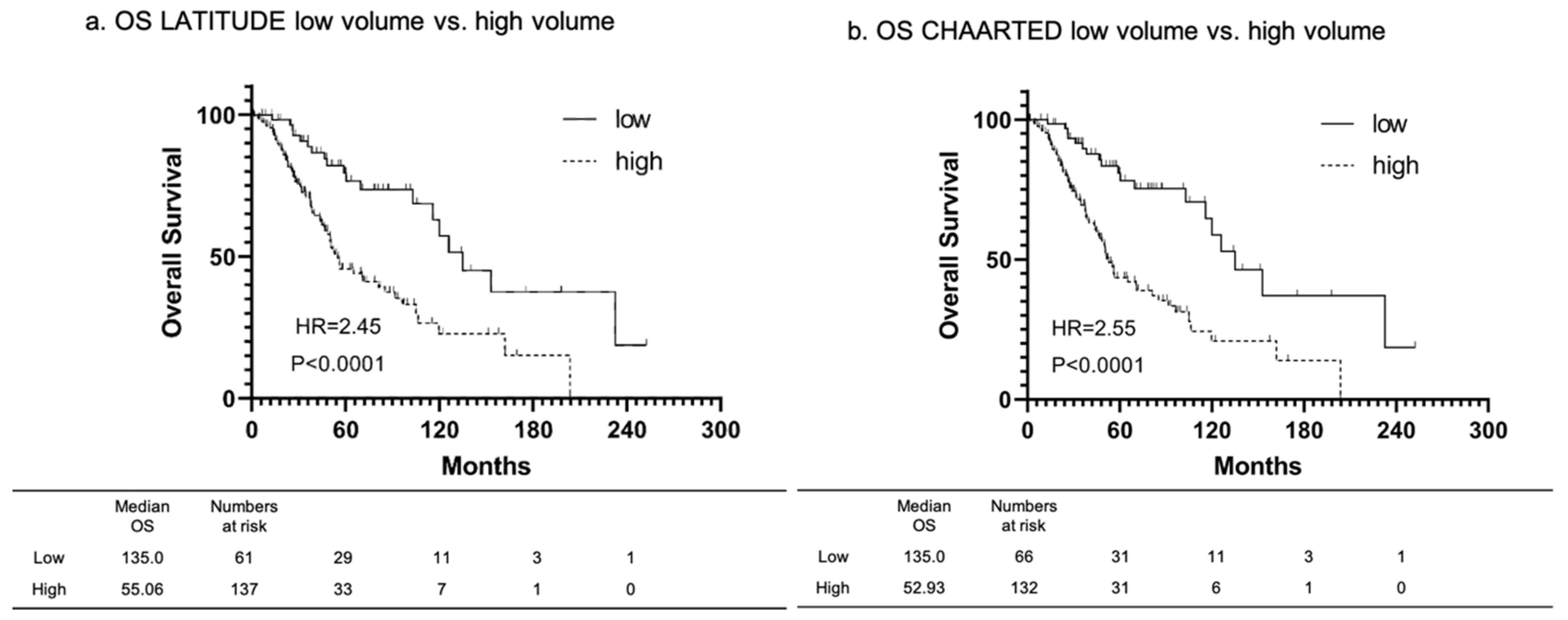
3.1. Overall Survival of Patients Classified by LATITUDE and CHAARTED Criteria
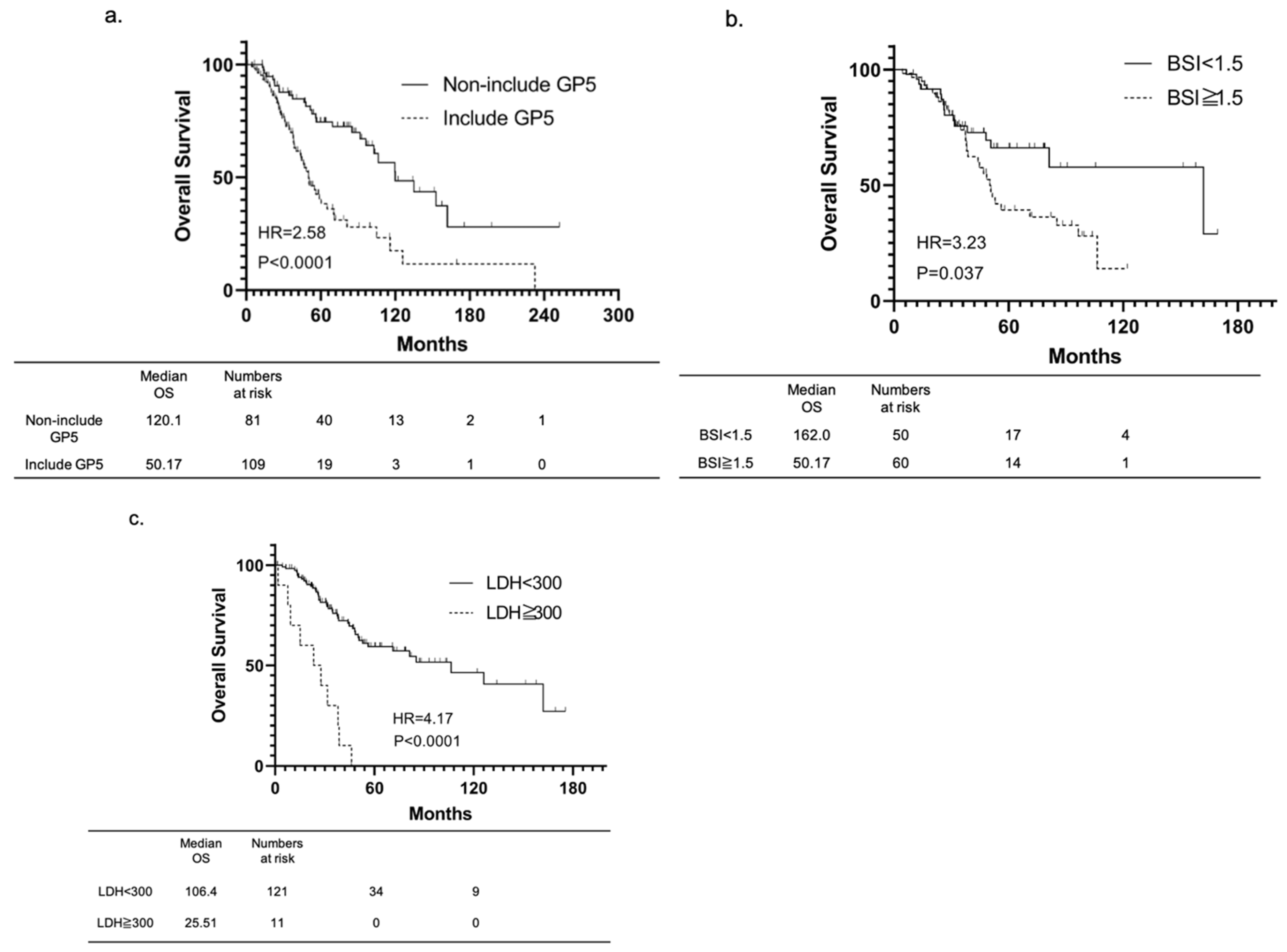
3.2. Identification of Prognostic Factors in Overall Survival
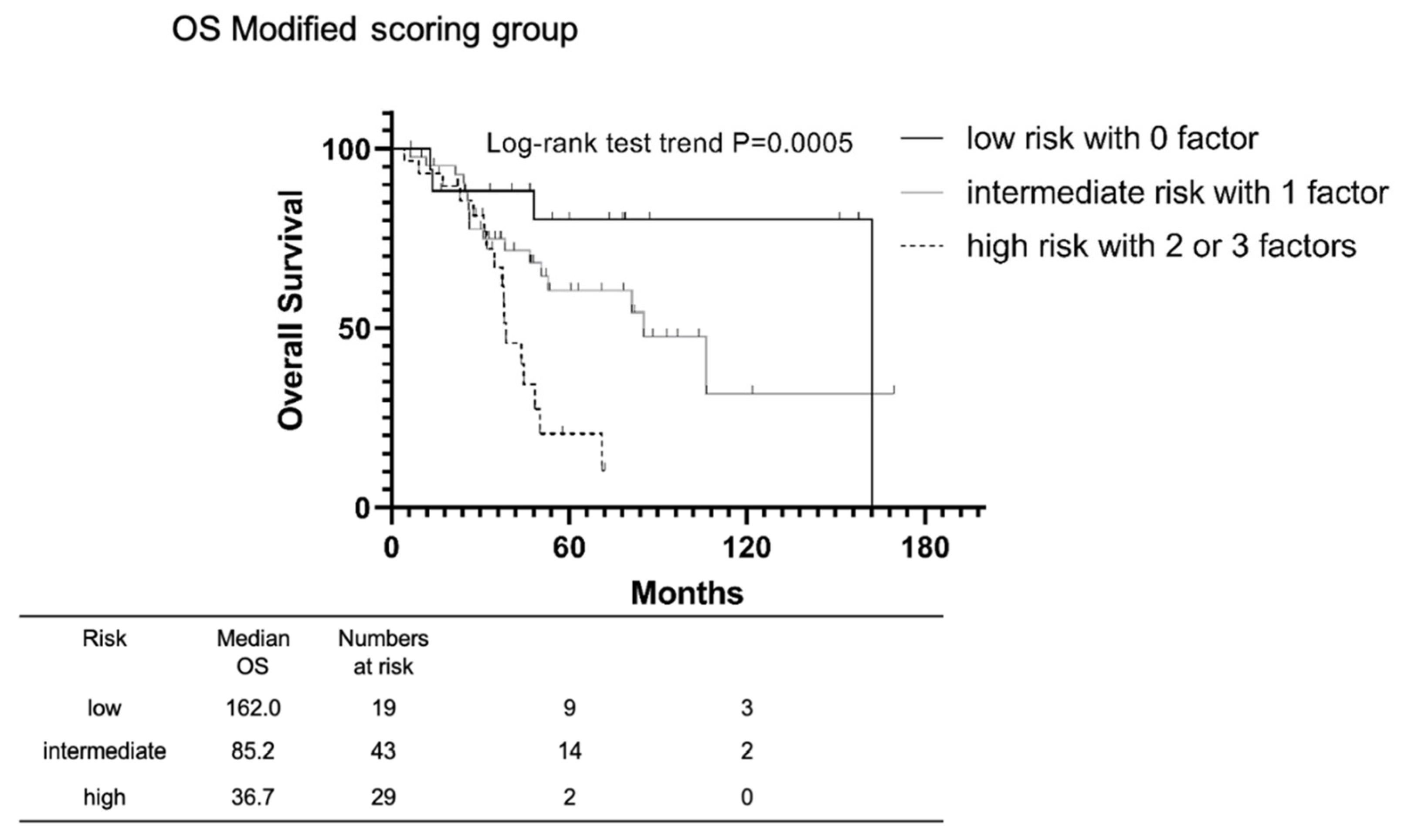
3.3. Development of a Risk Model for Overall Survival
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Ethics Statement
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2019. CA Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yap, T.A.; Zivi, A.; Omlin, A.; de Bono, J.S. The changing therapeutic landscape of castration-resistant prostate cancer. Nat. Rev. Clin. Oncol. 2011, 8, 597–610. [Google Scholar] [CrossRef] [PubMed]
- Huggins, C.; Hodges, C.V. Studies on prostatic cancer: I. The effect of castration, of estrogen and of androgen injection on serum phosphatases in metastatic carcinoma of the prostate. J. Urol. 2002, 168, 9–12. [Google Scholar] [CrossRef]
- Iwamoto, H.; Kano, H.; Shimada, T.; Naito, R.; Makino, T.; Kadamoto, S.; Yaegashi, H.; Shigehara, K.; Izumi, K.; Kadonoa, Y.; et al. Effectiveness of Vintage Hormone Therapy as Alternative Androgen Deprivation Therapy for Non-metastatic Castration-resistant Prostate Cancer. In Vivo 2021, 35, 1247–1252. [Google Scholar] [CrossRef] [PubMed]
- Tannock, I.F.; de Wit, R.; Berry, W.R.; Horti, J.; Pluzanska, A.; Chi, K.N.; Oudard, S.; Théodore, C.; James, N.D.; Turesson, I.; et al. Docetaxel plus prednisone or mitoxantrone plus prednisone for advanced prostate cancer. N. Engl. J. Med. 2004, 351, 1502–1512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iwamoto, H.; Kano, H.; Shimada, T.; Naito, R.; Makino, T.; Kadomoto, S.; Yaegashi, H.; Shigehara, K.; Izumi, K.; Kadono, Y.; et al. Sarcopenia and Visceral Metastasis at Cabazitaxel Initiation Predict Prognosis in Patients With Castration-resistant Prostate Cancer Receiving Cabazitaxel Chemotherapy. In Vivo 2021, 35, 1703–1709. [Google Scholar] [CrossRef] [PubMed]
- Coleman, R. Treatment of Metastatic Bone Disease and the Emerging Role of Radium-223. Semin. Nucl. Med. 2016, 46, 99–104. [Google Scholar] [CrossRef] [PubMed]
- Kyriakopoulos, C.E.; Chen, Y.H.; Carducci, M.A.; Liu, G.; Jarrard, D.F.; Hahn, N.M.; Shevrin, D.H.; Dreicer, R.; Hussain, M.; Eisenberger, M.; et al. Chemohormonal Therapy in Metastatic Hormone-Sensitive Prostate Cancer: Long-Term Survival Analysis of the Randomized Phase III E3805 CHAARTED Trial. J. Clin. Oncol. 2018, 36, 1080–1087. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Armstrong, A.J.; Szmulewitz, R.Z.; Petrylak, D.P.; Holzbeierlein, J.; Villers, A.; Azad, A.; Alcaraz, A.; Alekseev, B.; Iguchi, T.; Shore, N.D.; et al. ARCHES: A Randomized, Phase III Study of Androgen Deprivation Therapy With Enzalutamide or Placebo in Men With Metastatic Hormone-Sensitive Prostate Cancer. J. Clin. Oncol. 2019, 37, 2974–2986. [Google Scholar] [CrossRef] [PubMed]
- Sweeney, C.J.; Chen, Y.H.; Carducci, M.; Liu, G.; Jarrard, D.F.; Eisenberger, M.; Wong, Y.N.; Hahn, N.; Kohli, M.; Cooney, M.M.; et al. Chemohormonal Therapy in Metastatic Hormone-Sensitive Prostate Cancer. N. Engl. J. Med. 2015, 373, 737–746. [Google Scholar] [CrossRef] [PubMed]
- Fizazi, K.; Tran, N.; Fein, L.; Matsubara, N.; Rodriguez-Antolin, A.; Alekseev, B.Y.; Özgüroğlu, M.; Ye, D.; Feyerabend, S.; Protheroe, A.; et al. Abiraterone acetate plus prednisone in patients with newly diagnosed high-risk metastatic castration-sensitive prostate cancer (LATITUDE): Final overall survival analysis of a randomised, double-blind, phase 3 trial. Lancet Oncol. 2019, 20, 686–700. [Google Scholar] [CrossRef]
- Davis, I.D.; Martin, A.J.; Stockler, M.R.; Begbie, S.; Chi, K.N.; Chowdhury, S.; Coskinas, X.; Frydenberg, M.; Hague, W.E.; Horvath, L.G.; et al. Enzalutamide with Standard First-Line Therapy in Metastatic Prostate Cancer. N. Engl. J. Med. 2019, 381, 121–131. [Google Scholar] [CrossRef]
- Chi, K.N.; Agarwal, N.; Bjartell, A.; Chung, B.H.; Pereira de Santana Gomes, A.J.; Given, R.; Juárez Soto, Á.; Merseburger, A.S.; Özgüroğlu, M.; Uemura, H.; et al. Apalutamide for Metastatic, Castration-Sensitive Prostate Cancer. N. Engl. J. Med. 2019, 381, 13–24. [Google Scholar] [CrossRef]
- Smith, M.R.; Hussain, M.; Saad, F.; Fizazi, K.; Sternberg, C.N.; Crawford, E.D.; Kopyltsov, E.; Park, C.H.; Alekseev, B.; Montesa-Pino, Á.; et al. Darolutamide and Survival in Metastatic, Hormone-Sensitive Prostate Cancer. N. Engl. J. Med. 2022, 386, 1132–1142. [Google Scholar] [CrossRef] [PubMed]
- Roy, S.; Sun, Y.; Wallis, C.J.D.; Morgan, S.C.; Grimes, S.; Malone, J.; Kishan, A.U.; Mukherjee, D.; Spratt, D.E.; Saad, F.; et al. Development and validation of a multivariable prognostic model in de novo metastatic castrate sensitive prostate cancer. Prostate Cancer Prostatic Dis. 2022. [Google Scholar] [CrossRef]
- Koizumi, M.; Wagatsuma, K.; Miyaji, N.; Murata, T.; Miwa, K.; Takiguchi, T.; Makino, T.; Koyama, M. Evaluation of a computer-assisted diagnosis system, BONENAVI version 2, for bone scintigraphy in cancer patients in a routine clinical setting. Ann. Nucl. Med. 2015, 29, 138–148. [Google Scholar] [CrossRef]
- Dennis, E.R.; Jia, X.; Mezheritskiy, I.S.; Stephenson, R.D.; Schoder, H.; Fox, J.J.; Heller, G.; Scher, H.I.; Larson, S.M.; Morris, M.J. Bone scan index: A quantitative treatment response biomarker for castration-resistant metastatic prostate cancer. J. Clin. Oncol. 2012, 30, 519–524. [Google Scholar] [CrossRef] [Green Version]
- Soloway, M.S.; Hardeman, S.W.; Hickey, D.; Raymond, J.; Todd, B.; Soloway, S.; Moinuddin, M. Stratification of patients with metastatic prostate cancer based on extent of disease on initial bone scan. Cancer 1988, 61, 195–202. [Google Scholar] [CrossRef]
- Fukagai, T.; Namiki, T.S.; Carlile, R.G.; Yoshida, H.; Namiki, M. Comparison of the clinical outcome after hormonal therapy for prostate cancer between Japanese and Caucasian men. BJU Int. 2006, 97, 1190–1193. [Google Scholar] [CrossRef]
- Fizazi, K.; Tran, N.; Fein, L.; Matsubara, N.; Rodriguez-Antolin, A.; Alekseev, B.Y.; Özgüroğlu, M.; Ye, D.; Feyerabend, S.; Protheroe, A.; et al. Abiraterone plus Prednisone in Metastatic, Castration-Sensitive Prostate Cancer. N. Engl. J. Med. 2017, 377, 352–360. [Google Scholar] [CrossRef]
- Glass, T.R.; Tangen, C.M.; Crawford, E.D.; Thompson, I. Metastatic carcinoma of the prostate: Identifying prognostic groups using recursive partitioning. J. Urol. 2003, 169, 164–169. [Google Scholar] [CrossRef]
- Cooperberg, M.R.; Hinotsu, S.; Namiki, M.; Ito, K.; Broering, J.; Carroll, P.R.; Akaza, H. Risk assessment among prostate cancer patients receiving primary androgen deprivation therapy. J. Clin. Oncol. 2009, 27, 4306–4313. [Google Scholar] [CrossRef] [Green Version]
- Kryvenko, O.N.; Williamson, S.R.; Schwartz, L.E.; Epstein, J.I. Gleason score 5 + 3 = 8 (grade group 4) prostate cancer-a rare occurrence with contemporary grading. Hum. Pathol. 2020, 97, 40–51. [Google Scholar] [CrossRef]
- Tsao, C.K.; Gray, K.P.; Nakabayashi, M.; Evan, C.; Kantoff, P.W.; Huang, J.; Galsky, M.D.; Pomerantz, M.; Oh, W.K. Patients with Biopsy Gleason 9 and 10 Prostate Cancer Have Significantly Worse Outcomes Compared to Patients with Gleason 8 Disease. J. Urol. 2015, 194, 91–97. [Google Scholar] [CrossRef]
- Huynh, M.A.; Chen, M.H.; Wu, J.; Braccioforte, M.H.; Moran, B.J.; D’Amico, A.V. Gleason Score 3 + 5 or 5 + 3 versus 4 + 4 Prostate Cancer: The Risk of Death. Eur. Urol. 2016, 69, 976–979. [Google Scholar] [CrossRef]
- Shiota, M.; Terada, N.; Kitamura, H.; Kojima, T.; Saito, T.; Yokomizo, A.; Kohei, N.; Goto, T.; Kawamura, S.; Hashimoto, Y.; et al. Novel metastatic burden-stratified risk model in de novo metastatic hormone-sensitive prostate cancer. Cancer Sci. 2021, 112, 3616–3626. [Google Scholar] [CrossRef]
- Akamatsu, S.; Kubota, M.; Uozumi, R.; Narita, S.; Takahashi, M.; Mitsuzuka, K.; Hatakeyama, S.; Sakurai, T.; Kawamura, S.; Ishidoya, S.; et al. Development and Validation of a Novel Prognostic Model for Predicting Overall Survival in Treatment-naïve Castration-sensitive Metastatic Prostate Cancer. Eur. Urol. Oncol. 2019, 2, 320–328. [Google Scholar] [CrossRef]
- Nakajima, K.; Edenbrandt, L.; Mizokami, A. Bone scan index: A new biomarker of bone metastasis in patients with prostate cancer. Int. J. Urol. 2017, 24, 668–673. [Google Scholar] [CrossRef] [Green Version]
- Imbriaco, M.; Larson, S.M.; Yeung, H.W.; Mawlawi, O.R.; Erdi, Y.; Venkatraman, E.S.; Scher, H.I. A new parameter for measuring metastatic bone involvement by prostate cancer: The Bone Scan Index. Clin. Cancer Res. 1998, 4, 1765–1772. [Google Scholar]
- Poulsen, M.H.; Rasmussen, J.; Edenbrandt, L.; Høilund-Carlsen, P.F.; Gerke, O.; Johansen, A.; Lund, L. Bone Scan Index predicts outcome in patients with metastatic hormone-sensitive prostate cancer. BJU Int. 2016, 117, 748–753. [Google Scholar] [CrossRef]
- Nakajima, K.; Mizokami, A.; Matsuyama, H.; Ichikawa, T.; Kaneko, G.; Takahashi, S.; Shiina, H.; Horikoshi, H.; Hashine, K.; Sugiyama, Y.; et al. Prognosis of patients with prostate cancer and bone metastasis from the Japanese Prostatic Cancer Registry of Standard Hormonal and Chemotherapy Using Bone Scan Index cohort study. Int. J. Urol. 2021, 28, 955–963. [Google Scholar] [CrossRef]
- Suzuki, K.; Okamura, Y.; Hara, T.; Terakawa, T.; Furukawa, J.; Harada, K.; Hinata, N.; Fujisawa, M. Prognostic impact of bone metastatic volume beyond vertebrae and pelvis in patients with metastatic hormone-sensitive prostate cancer. Int. J. Clin. Oncol. 2021, 26, 1533–1540. [Google Scholar] [CrossRef]
- Mongre, R.K.; Mishra, C.B.; Prakash, A.; Jung, S.; Lee, B.S.; Kumari, S.; Hong, J.T.; Lee, M.S. Novel Carbazole-Piperazine Hybrid Small Molecule Induces Apoptosis by Targeting BCL-2 and Inhibits Tumor Progression in Lung Adenocarcinoma in Vitro and Xenograft Mice Model. Cancers 2019, 11, 1245. [Google Scholar] [CrossRef] [Green Version]
- Narita, S.; Hatakeyama, S.; Takahashi, M.; Sakurai, T.; Kawamura, S.; Hoshi, S.; Ishida, M.; Kawaguchi, T.; Ishidoya, S.; Shimoda, J.; et al. Clinical outcomes and prognostic factors in patients with newly diagnosed metastatic prostate cancer initially treated with androgen deprivation therapy: A retrospective multicenter study in Japan. Int. J. Clin. Oncol. 2020, 25, 912–920. [Google Scholar] [CrossRef]
- Kobayashi, T.; Namitome, R.; Hirata, Y.U.; Shiota, M.; Imada, K.; Kashiwagi, E.; Takeuchi, A.; Inokuchi, J.; Tatsugami, K.; Eto, M. Serum Prognostic Factors of Androgen-deprivation Therapy Among Japanese Men With De Novo Metastatic Prostate Cancer. Anticancer Res. 2019, 39, 3191–3195. [Google Scholar] [CrossRef]
- Kawahara, T.; Yoneyama, S.; Ohno, Y.; Iizuka, J.; Hashimoto, Y.; Tsumura, H.; Tabata, K.I.; Nakagami, Y.; Tanabe, K.; Iwamura, M.; et al. Prognostic Value of the LATITUDE and CHAARTED Risk Criteria for Predicting the Survival of Men with Bone Metastatic Hormone-Naïve Prostate Cancer Treated with Combined Androgen Blockade Therapy: Real-World Data from a Japanese Multi-Institutional Study. Biomed Res. Int. 2020, 2020, 7804932. [Google Scholar] [CrossRef]
- Shiota, M.; Terada, N.; Saito, T.; Yokomizo, A.; Kohei, N.; Goto, T.; Kawamura, S.; Hashimoto, Y.; Takahashi, A.; Kimura, T.; et al. Differential prognostic factors in low- and high-burden de novo metastatic hormone-sensitive prostate cancer patients. Cancer Sci. 2021, 112, 1524–1533. [Google Scholar] [CrossRef]
- Iwamoto, H.; Izumi, K.; Shimada, T.; Kano, H.; Kadomoto, S.; Makino, T.; Naito, R.; Yaegashi, H.; Shigehara, K.; Kadono, Y.; et al. Androgen receptor signaling-targeted therapy and taxane chemotherapy induce visceral metastasis in castration-resistant prostate cancer. Prostate 2021, 81, 72–80. [Google Scholar] [CrossRef]
- Cooperberg, M.R.; Hinotsu, S.; Namiki, M.; Carroll, P.R.; Akaza, H. Trans-Pacific variation in outcomes for men treated with primary androgen-deprivation therapy (ADT) for prostate cancer. BJU Int. 2016, 117, 102–109. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | Entire Cohort (n = 198) |
|---|---|
| Age, median (range) | 71 (65–78) |
| T stage, no (%) | |
| T1-2 | 17 (8.6) |
| T3 | 85 (42.9) |
| T4 | 77 (38.9) |
| Unknown | 19 (9.6) |
| N stage, no (%) | |
| N0 | 79 (39.9) |
| N1 | 115 (58.1) |
| Unknown | 4 (2.0) |
| M stage, no (%) | |
| M1a | 5 (2.5) |
| M1b | 165 (83.3) |
| M1c | 28 (14.1) |
| Site of metastasis, no (%) | |
| Lymph node | 116 (58.6) |
| Bone | 188 (94.9) |
| Lung | 23 (11.6) |
| Liver | 3 (1.5) |
| Adrenal gland | 1 (0.5) |
| Initial PSA level, ng/mL, median (range) | 230.5 (72.7–859.4) |
| Gleason score, no (%) | |
| ≦3 + 4 | 10 (5.1) |
| 4 + 3 | 19 (9.6) |
| 8 | 52 (26.3) |
| ≧9 | 107 (54.0) |
| Unknown | 10 (5.1) |
| Initial treatment, no (%) | |
| CAB | 185 (93.4) |
| LHRH agonist | 3 (1.5) |
| Abiraterone | 1 (0.5) |
| Other | 5 (2.5) |
| Unknown | 4 (2.0) |
| Variables | Univariate | Multivariable | ||||||
|---|---|---|---|---|---|---|---|---|
| 95% CI | 95% CI | |||||||
| p Value | HR | Lower | Upper | p Value | HR | Lower | Upper | |
| Age <70 vs. ≧70 (years) | 0.53 | 1.15 | 0.74 | 1.79 | 0.37 | 1.46 | 0.64 | 3.33 |
| Include GP5 | <0.001 | 2.78 | 1.72 | 4.47 | 0.045 | 2.77 | 1.03 | 7.49 |
| PSA <200 vs. ≧200 (ng/mL) | 0.40 | 1.21 | 0.78 | 1.86 | 0.32 | 0.55 | 0.17 | 1.78 |
| BSI <1.5 vs. ≧1.5 | 0.04 | 1.91 | 1.03 | 3.53 | 0.033 | 3.48 | 1.10 | 11.00 |
| Visceral metastasis | 0.53 | 1.20 | 0.69 | 2.07 | 0.053 | 0.15 | 0.02 | 1.03 |
| CRP <1.0 vs. ≧1.0 (mg/dL) | 0.76 | 1.10 | 0.60 | 2.03 | 0.67 | 0.80 | 0.29 | 2.24 |
| NLR <2.5 vs. ≧2.5 | 0.13 | 1.65 | 0.87 | 3.14 | 0.09 | 2.32 | 0.89 | 6.08 |
| Hb <12 vs. ≧12 (g/dL) | 0.35 | 1.35 | 0.72 | 2.56 | 0.64 | 0.79 | 0.29 | 2.15 |
| ALP <300 vs. ≧300 (IU/L) | 0.31 | 1.34 | 0.76 | 2.37 | 0.32 | 0.55 | 0.17 | 1.79 |
| LDH <300 vs. ≧300 (IU/L) | <0.001 | 6.08 | 2.95 | 12.50 | 0.004 | 8.11 | 1.99 | 33.11 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nakagawa, R.; Iwamoto, H.; Makino, T.; Naito, R.; Kadomoto, S.; Akatani, N.; Yaegashi, H.; Kawaguchi, S.; Nohara, T.; Shigehara, K.; et al. Development of a Prognostic Model of Overall Survival for Metastatic Hormone-Naïve Prostate Cancer in Japanese Men. Cancers 2022, 14, 4822. https://doi.org/10.3390/cancers14194822
Nakagawa R, Iwamoto H, Makino T, Naito R, Kadomoto S, Akatani N, Yaegashi H, Kawaguchi S, Nohara T, Shigehara K, et al. Development of a Prognostic Model of Overall Survival for Metastatic Hormone-Naïve Prostate Cancer in Japanese Men. Cancers. 2022; 14(19):4822. https://doi.org/10.3390/cancers14194822
Chicago/Turabian StyleNakagawa, Ryunosuke, Hiroaki Iwamoto, Tomoyuki Makino, Renato Naito, Suguru Kadomoto, Norihito Akatani, Hiroshi Yaegashi, Shohei Kawaguchi, Takahiro Nohara, Kazuyoshi Shigehara, and et al. 2022. "Development of a Prognostic Model of Overall Survival for Metastatic Hormone-Naïve Prostate Cancer in Japanese Men" Cancers 14, no. 19: 4822. https://doi.org/10.3390/cancers14194822