

Automated Assessment of Breast Positioning Quality in Screening Mammography
 ,
, 
Abstract
:Simple Summary
Abstract
1. Introduction and Related Work
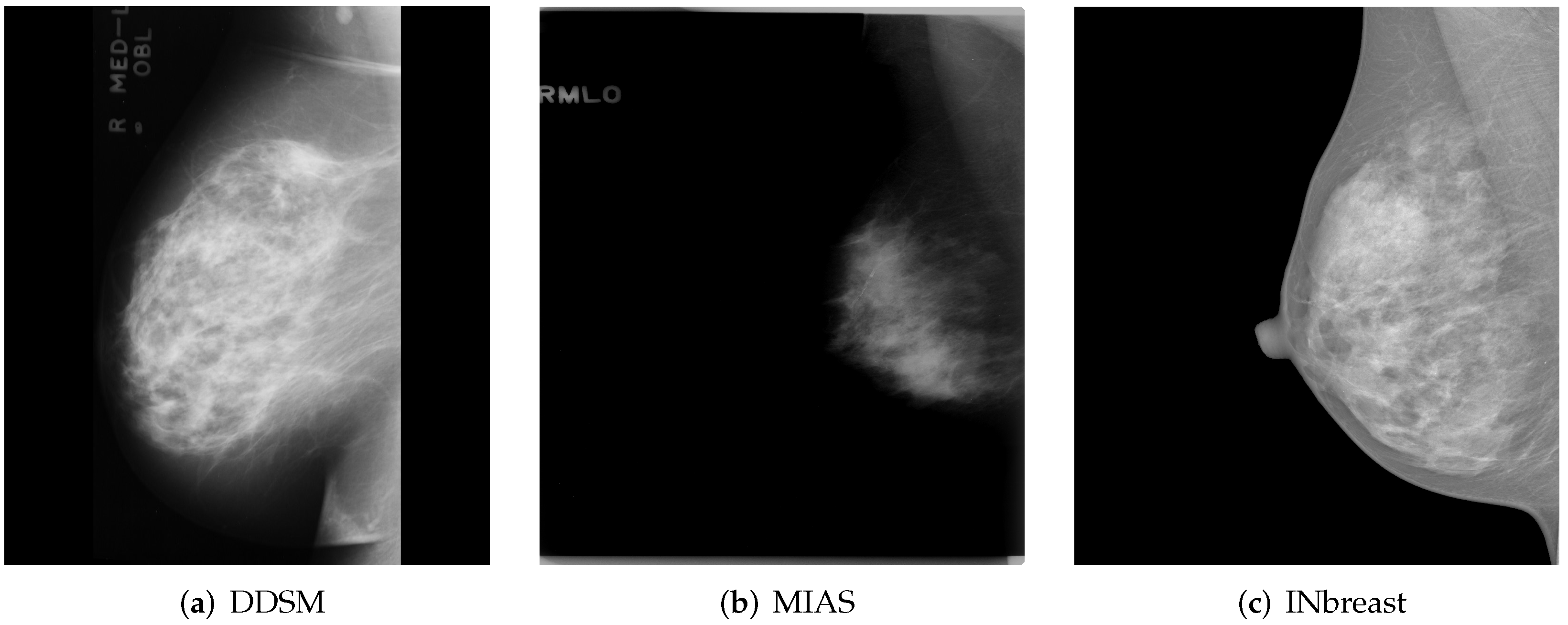
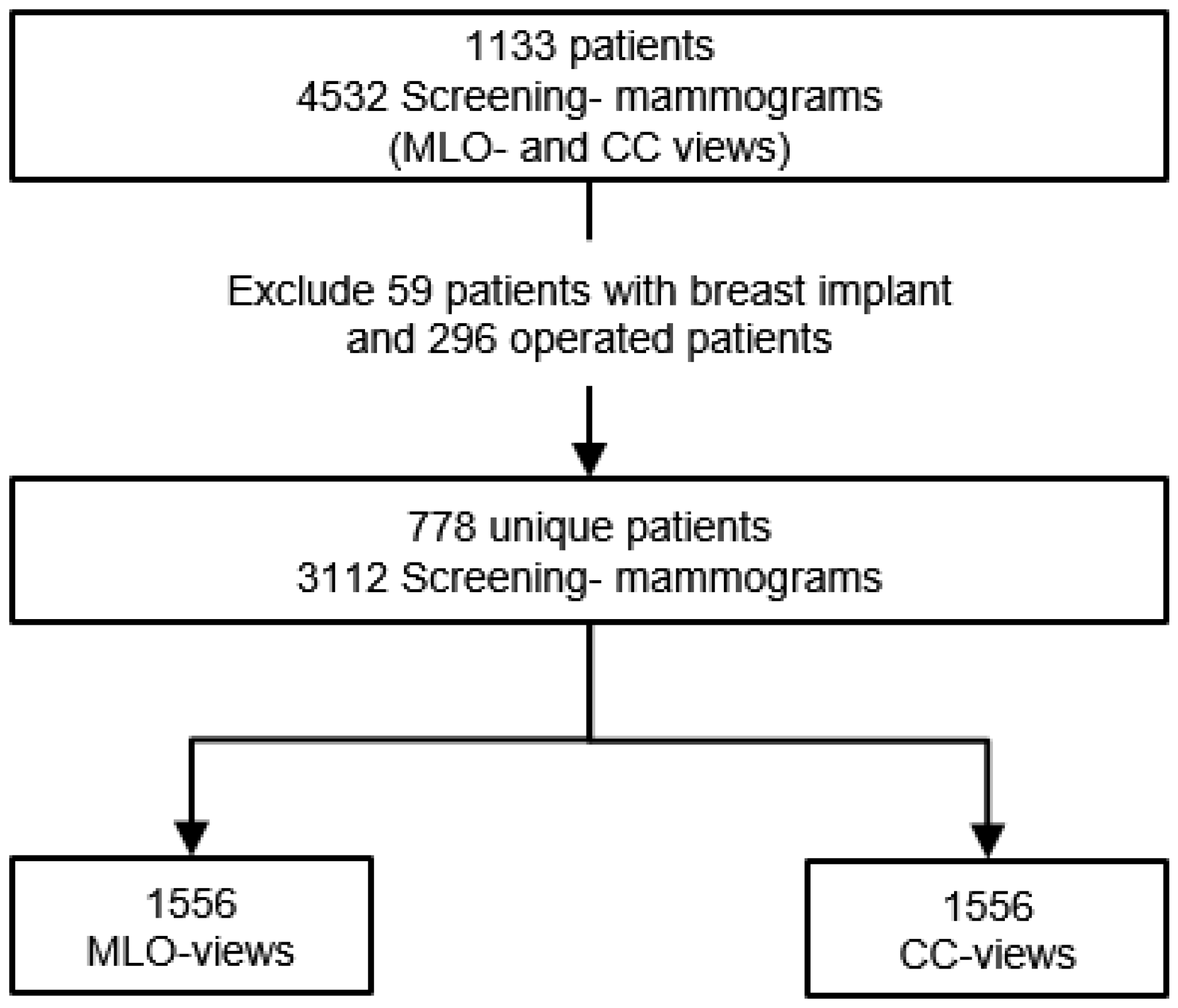
2. Materials and Methods
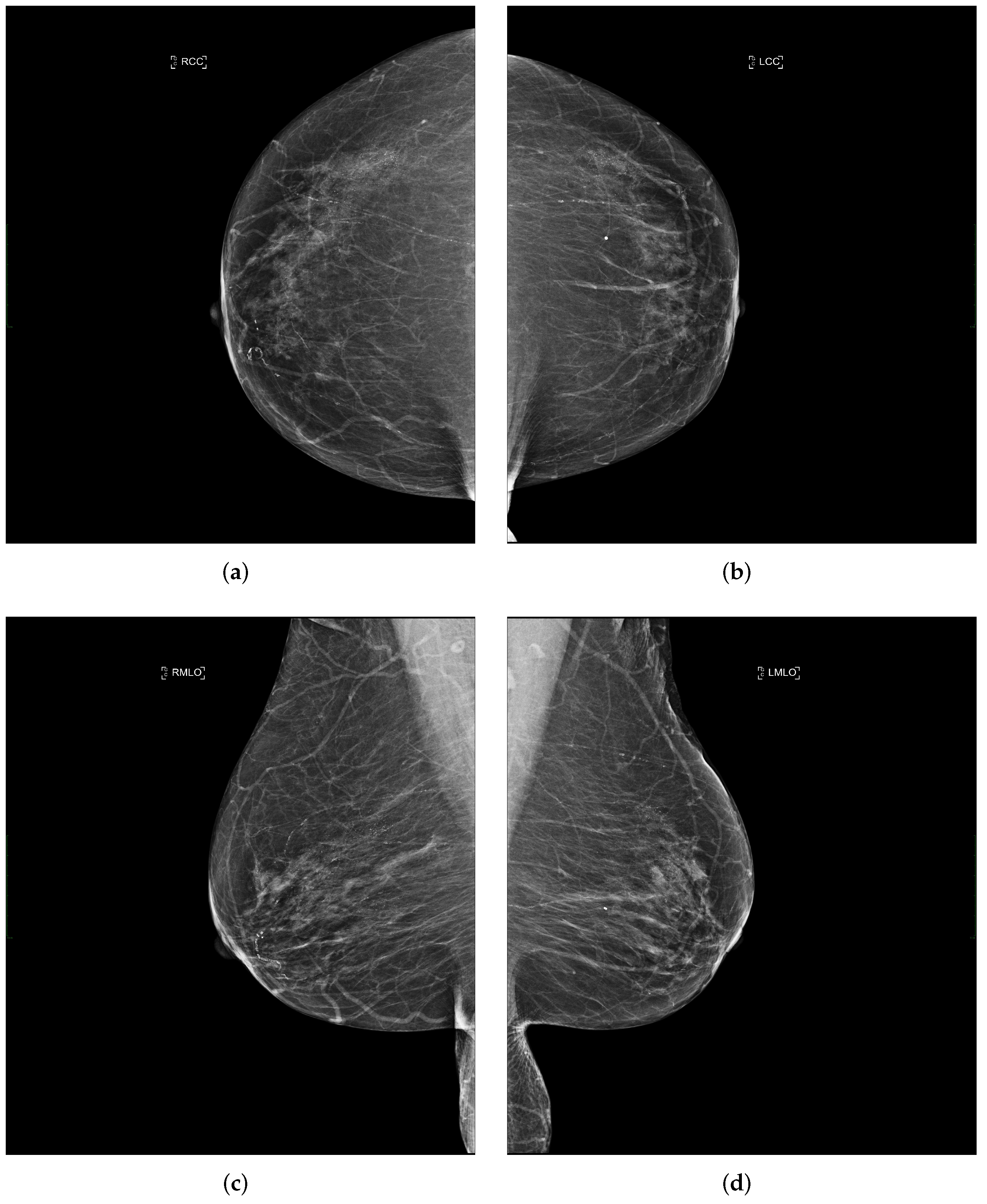
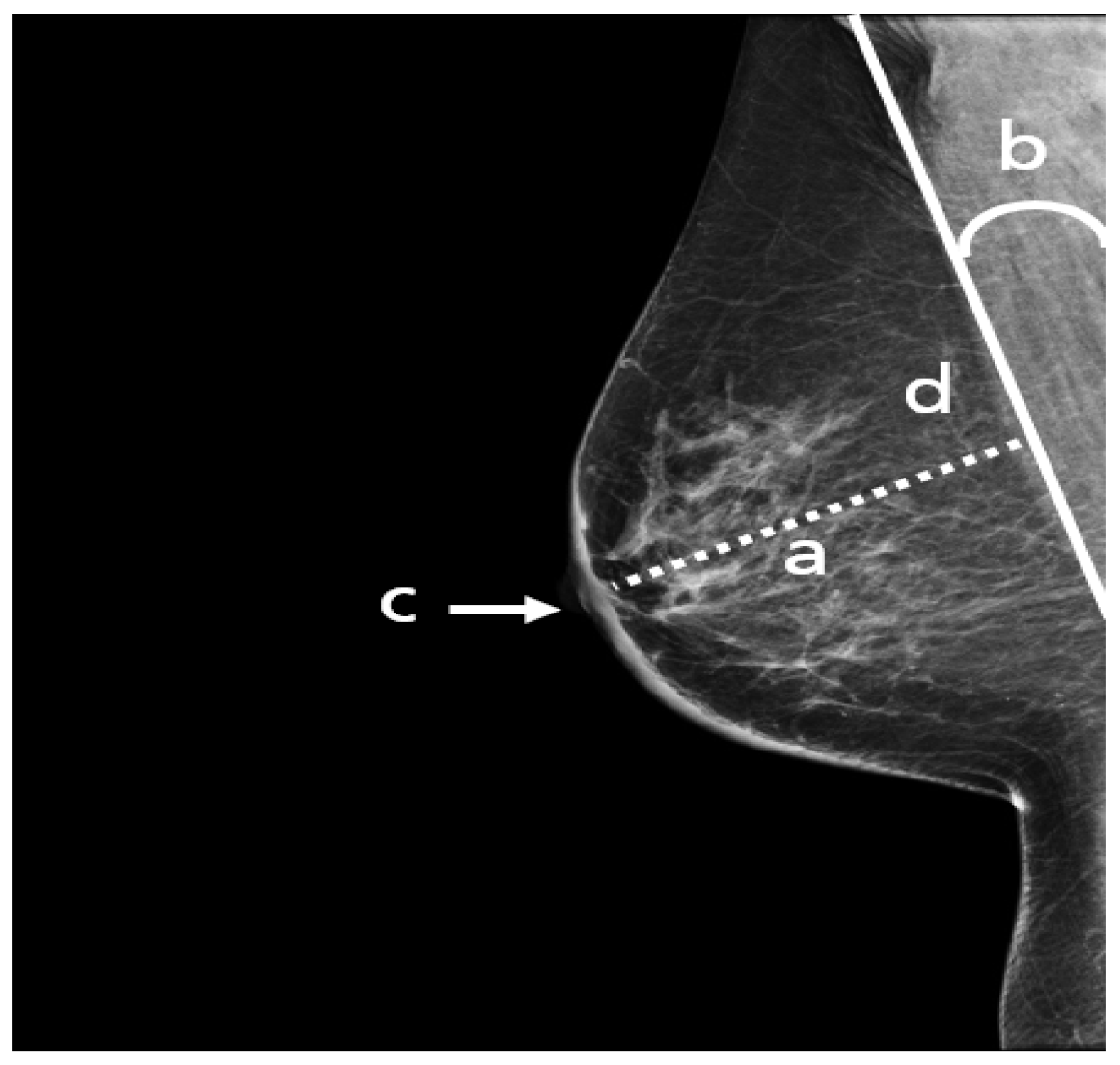
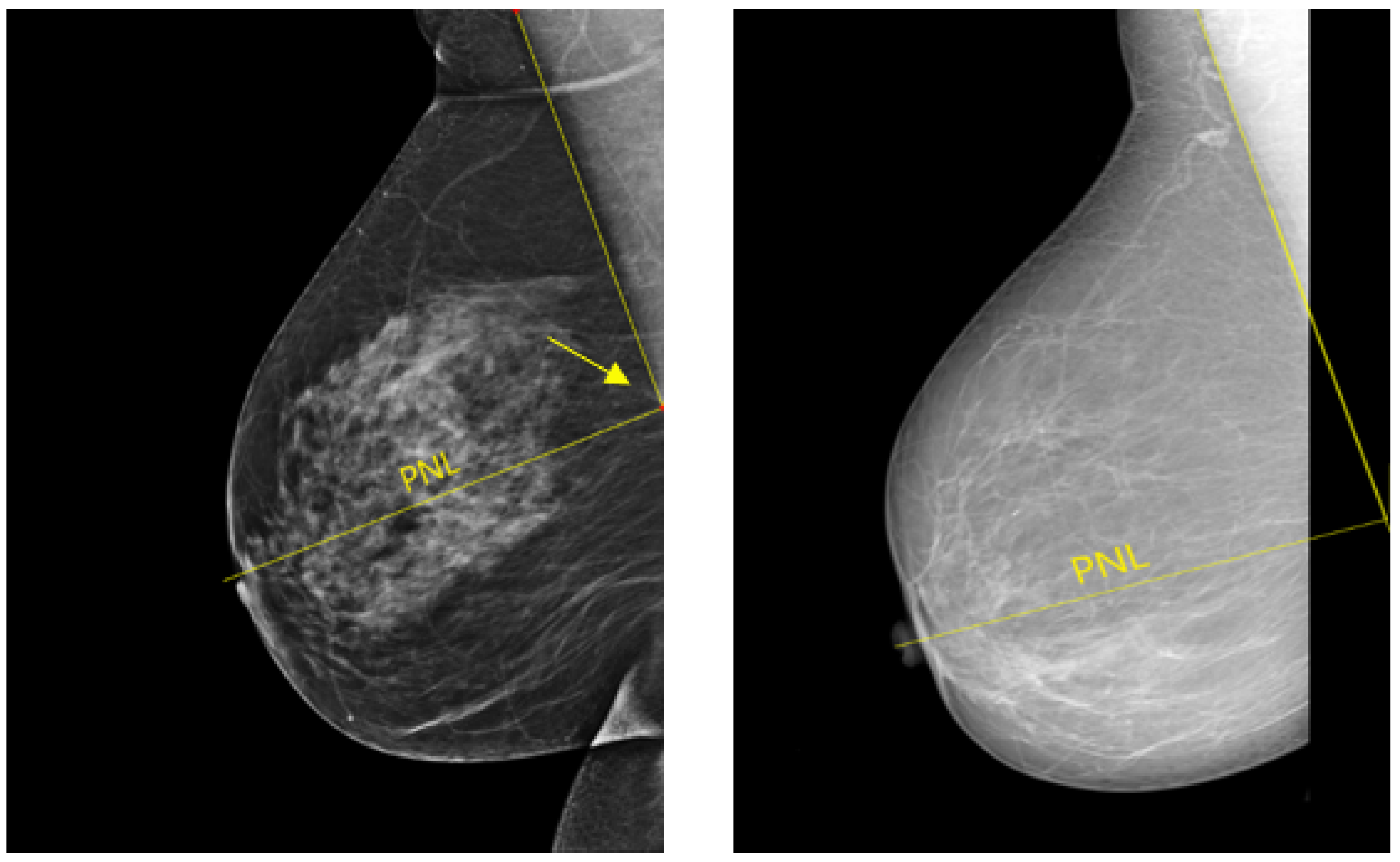
2.1. Mediolateral-Oblique View
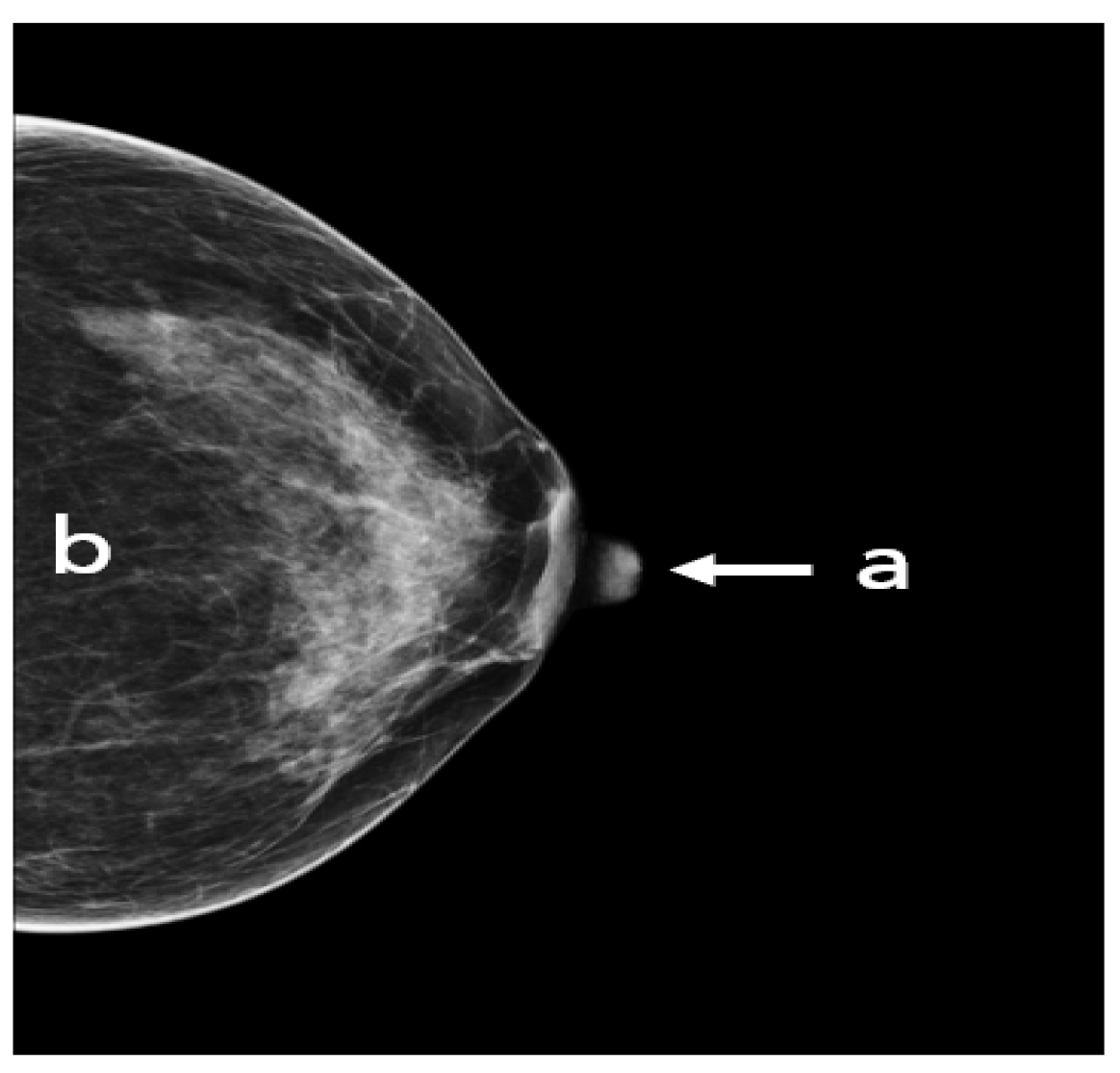
2.2. Cranio-Caudal View
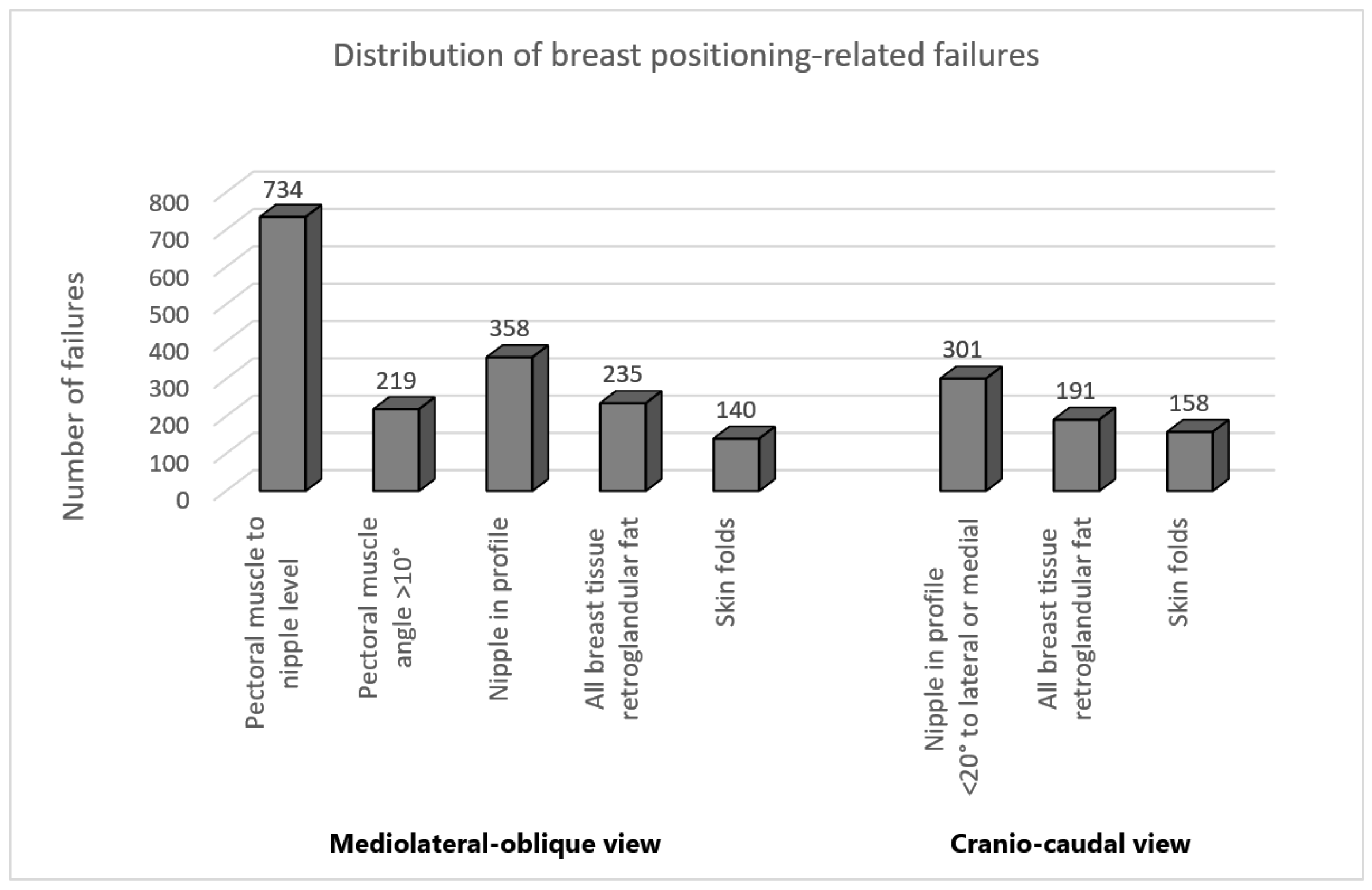
2.3. Data Classification
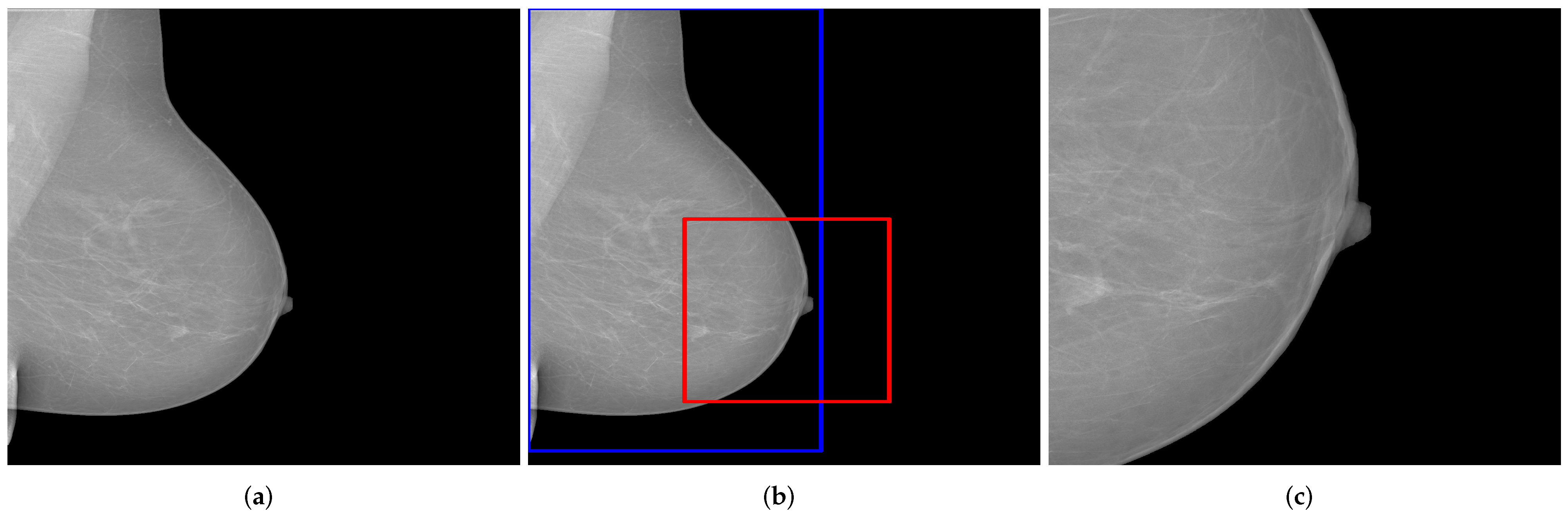
2.4. Data Preprocessing and Augmentation
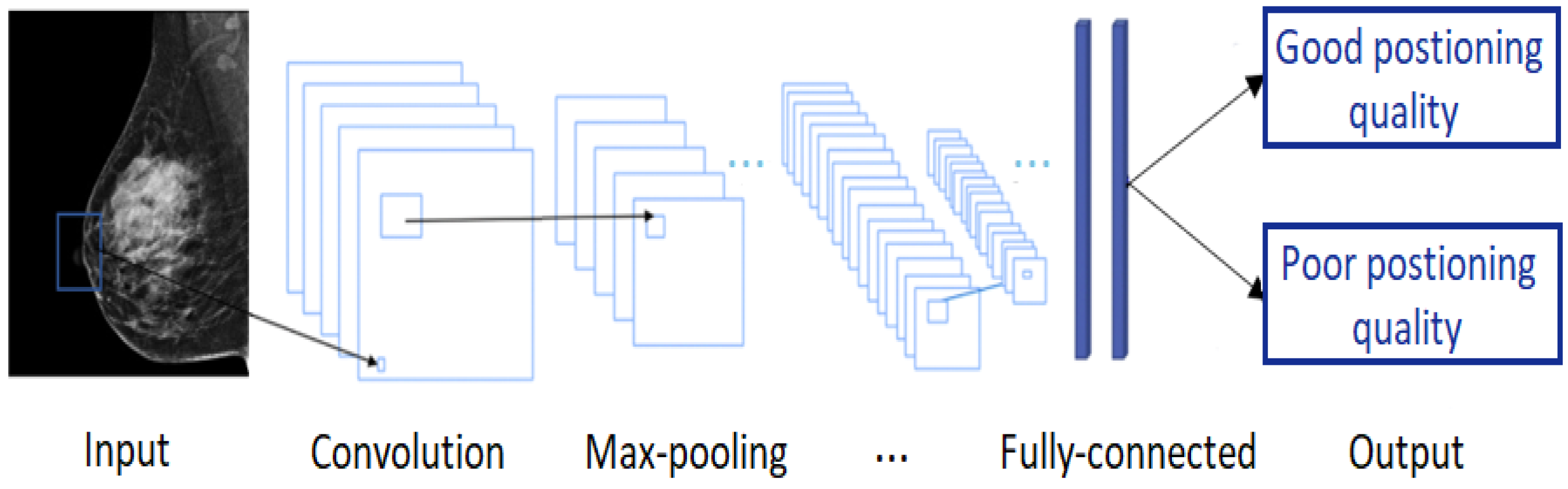
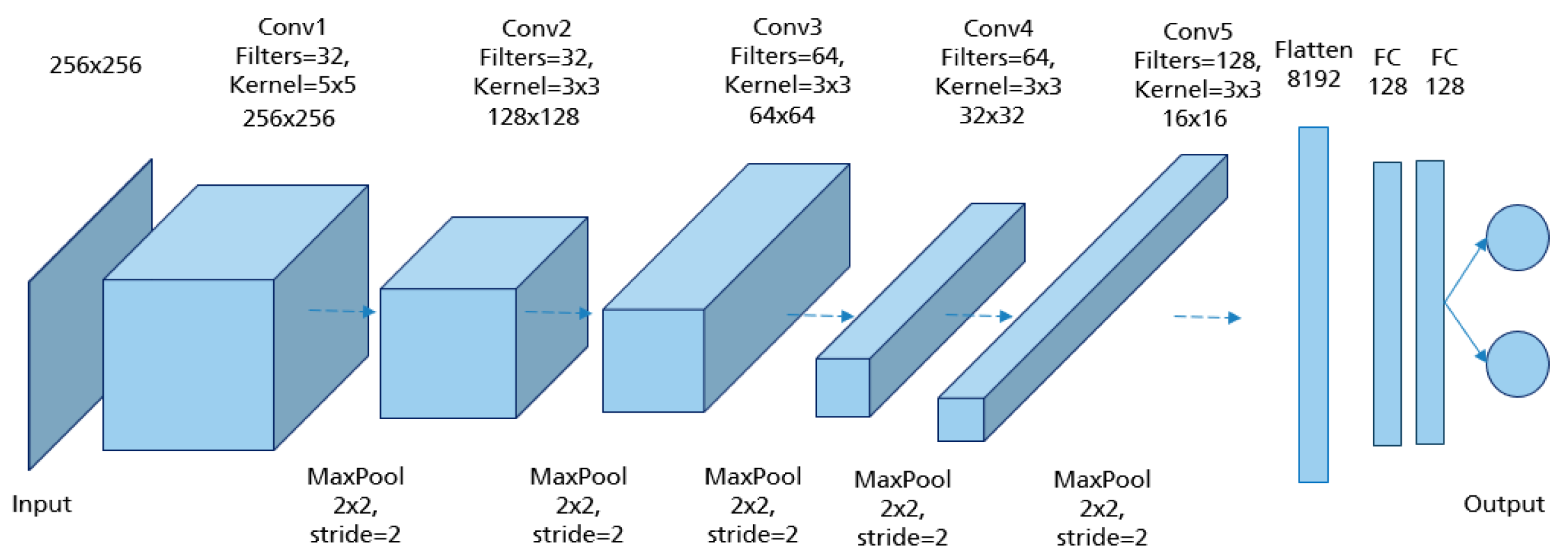
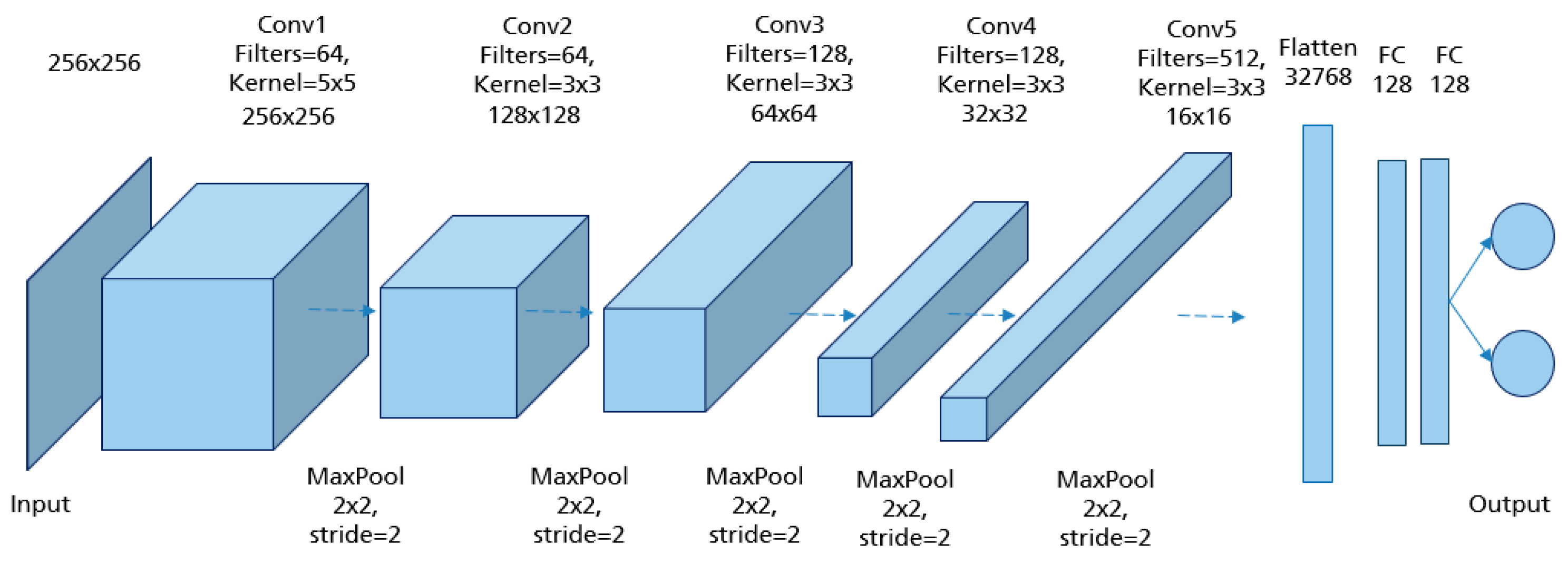
2.5. Convolutional Neural Networks (CNN)
3. Development of the CNN Models
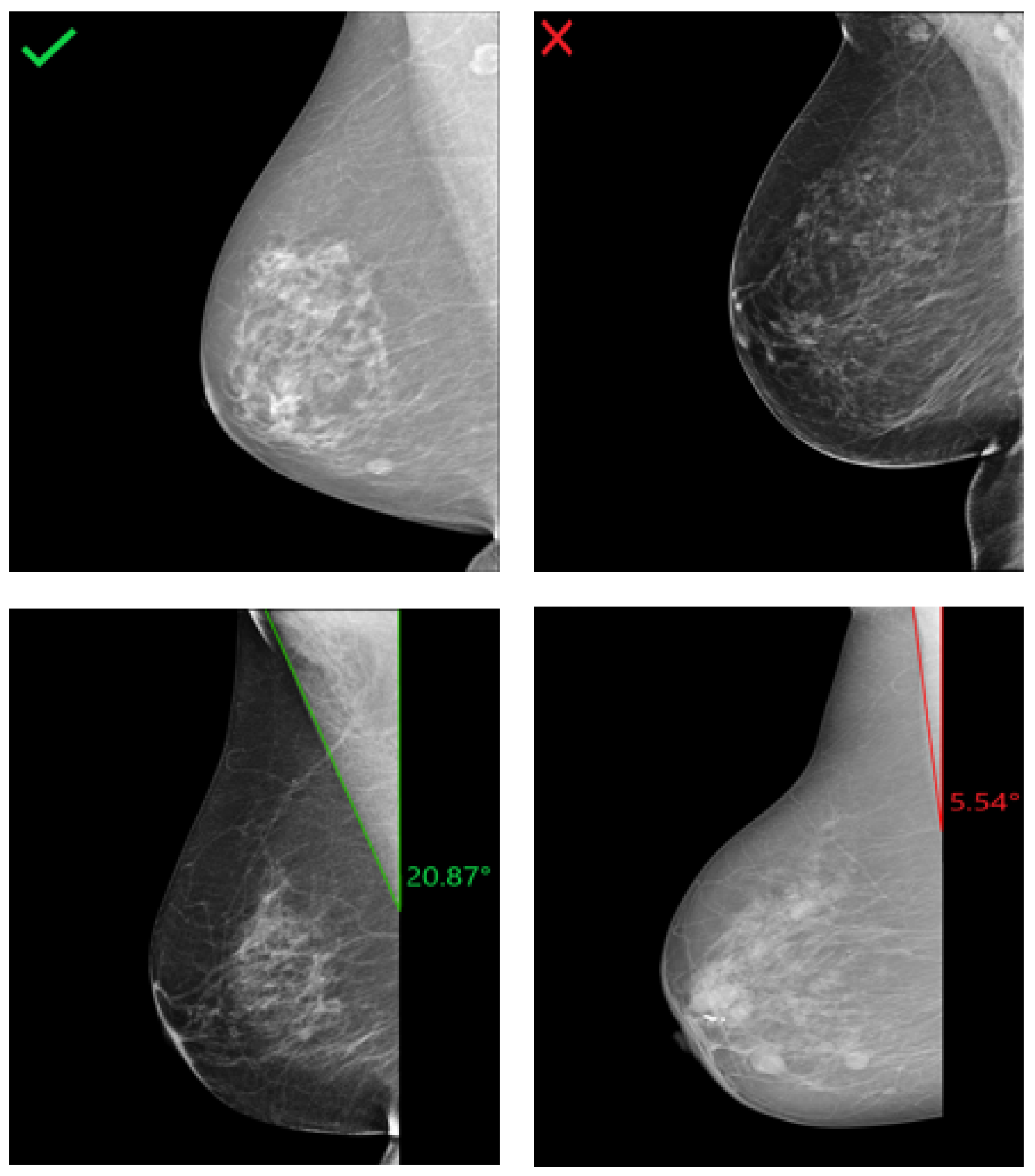
3.1. MLO: Pectoralis Muscle Angle
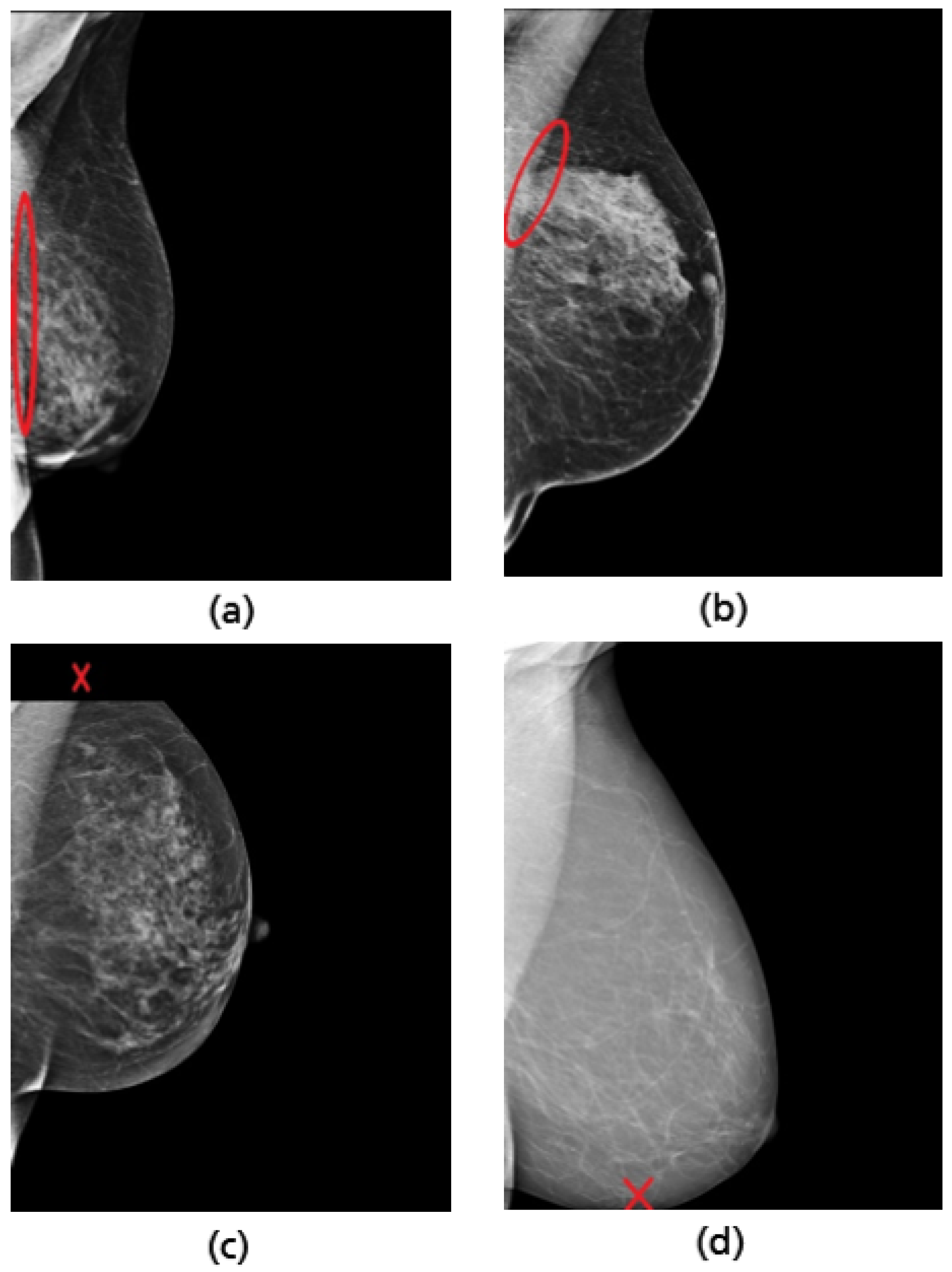
3.2. MLO: Pectoralis Muscle Level
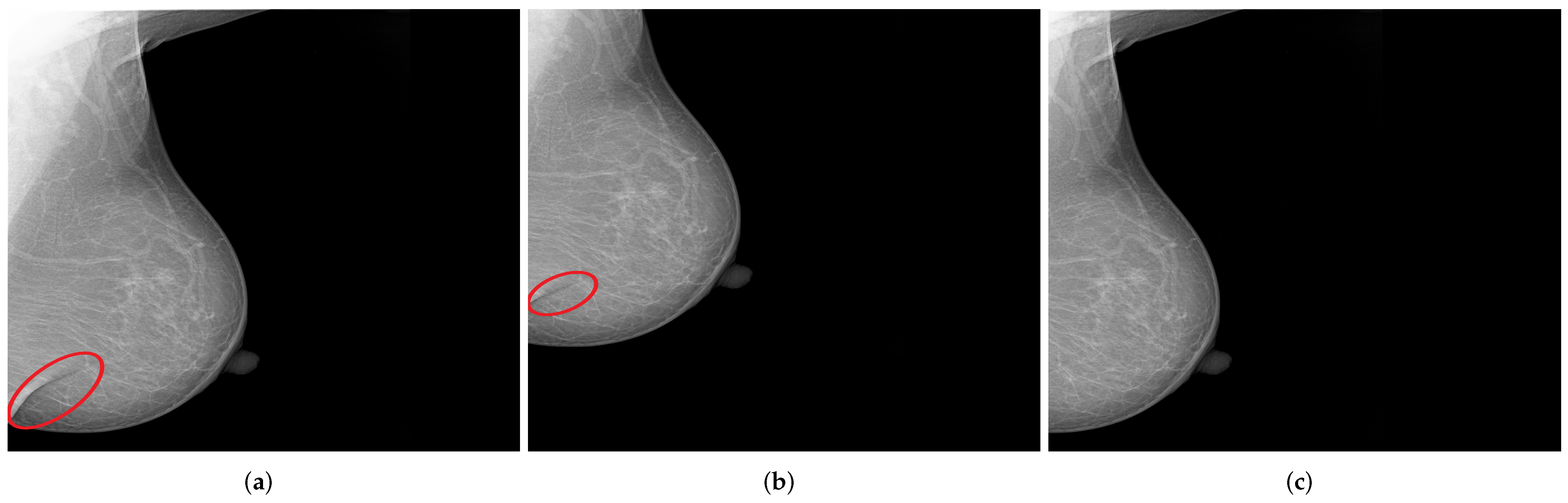
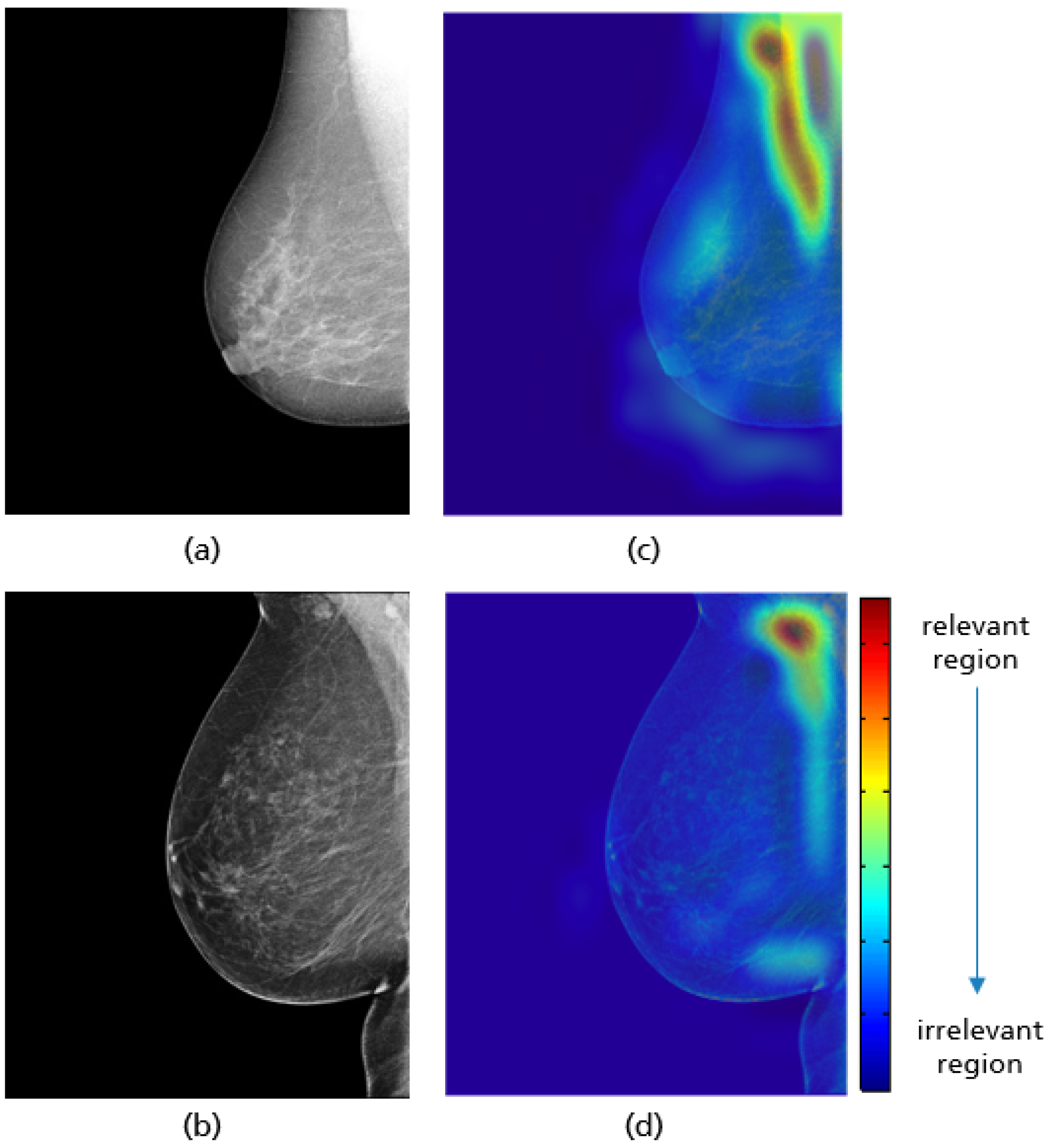
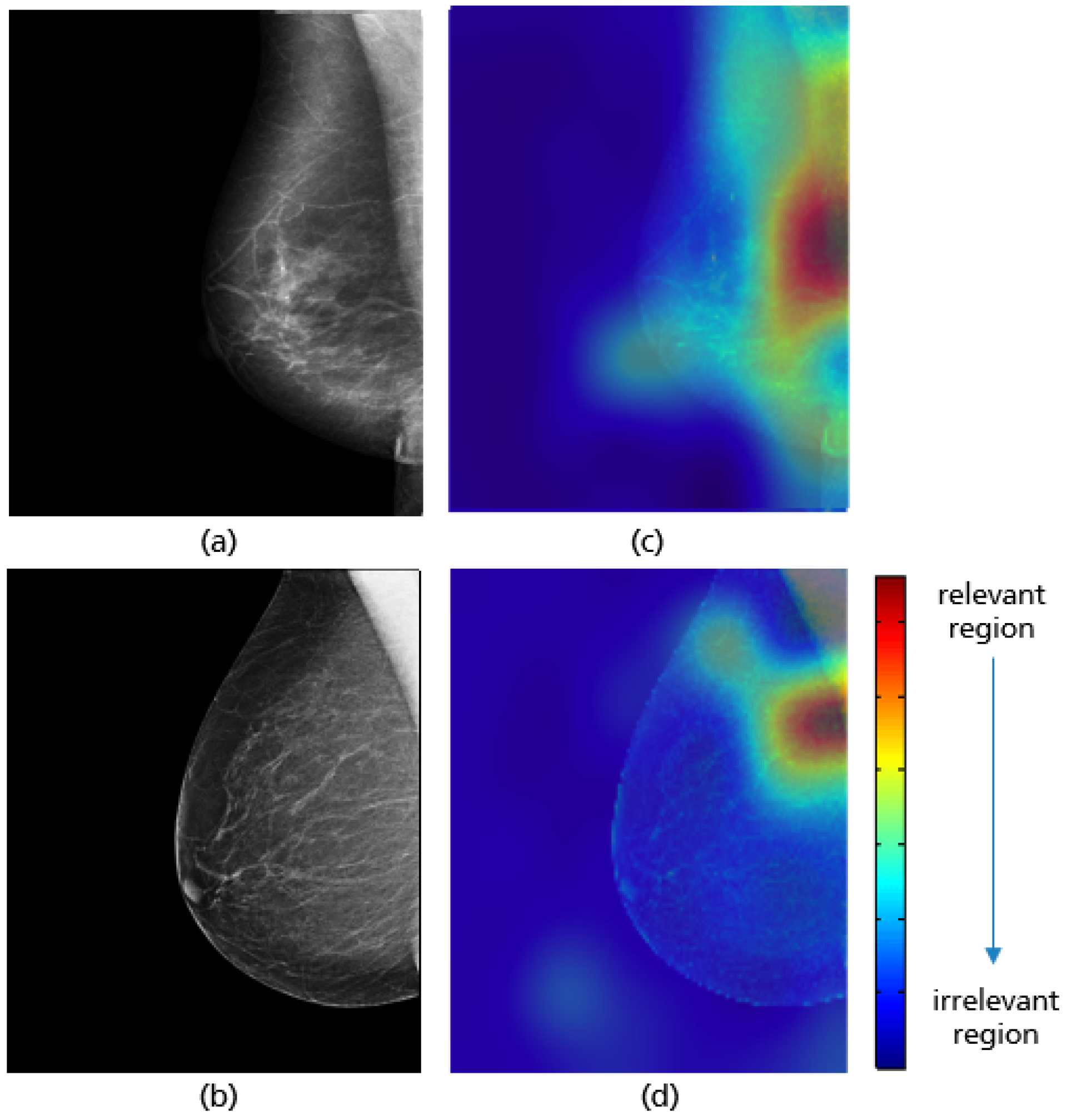
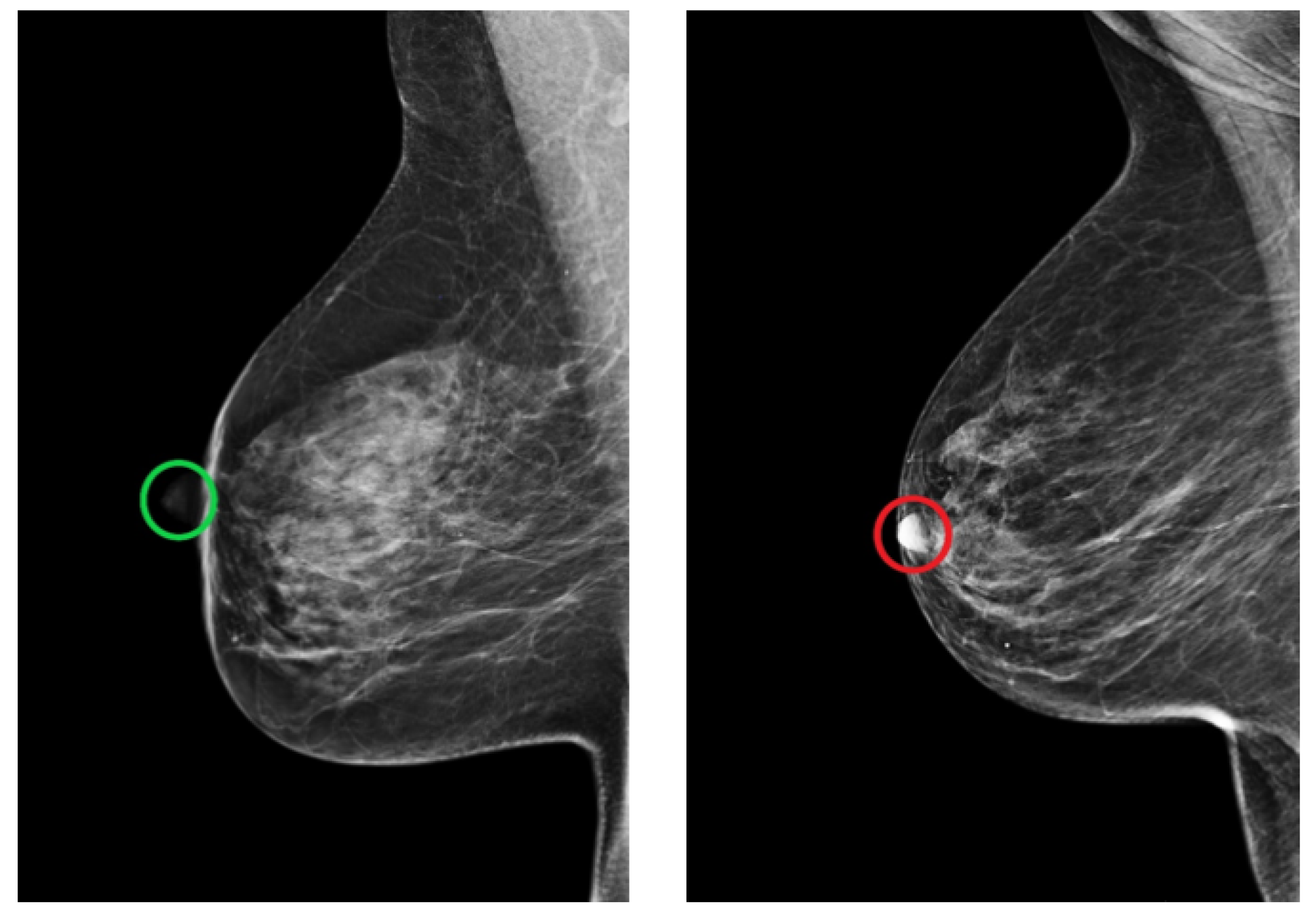
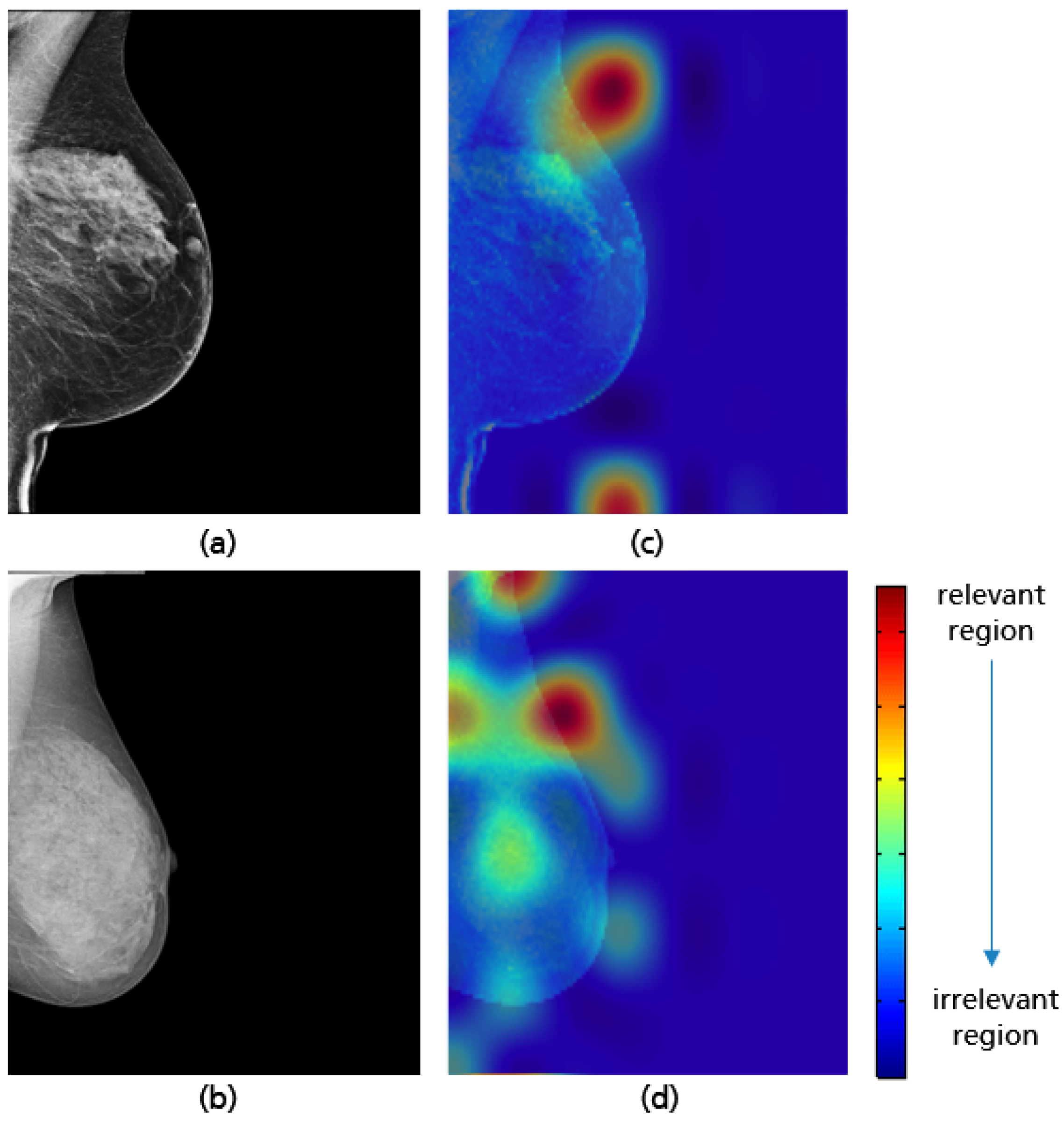
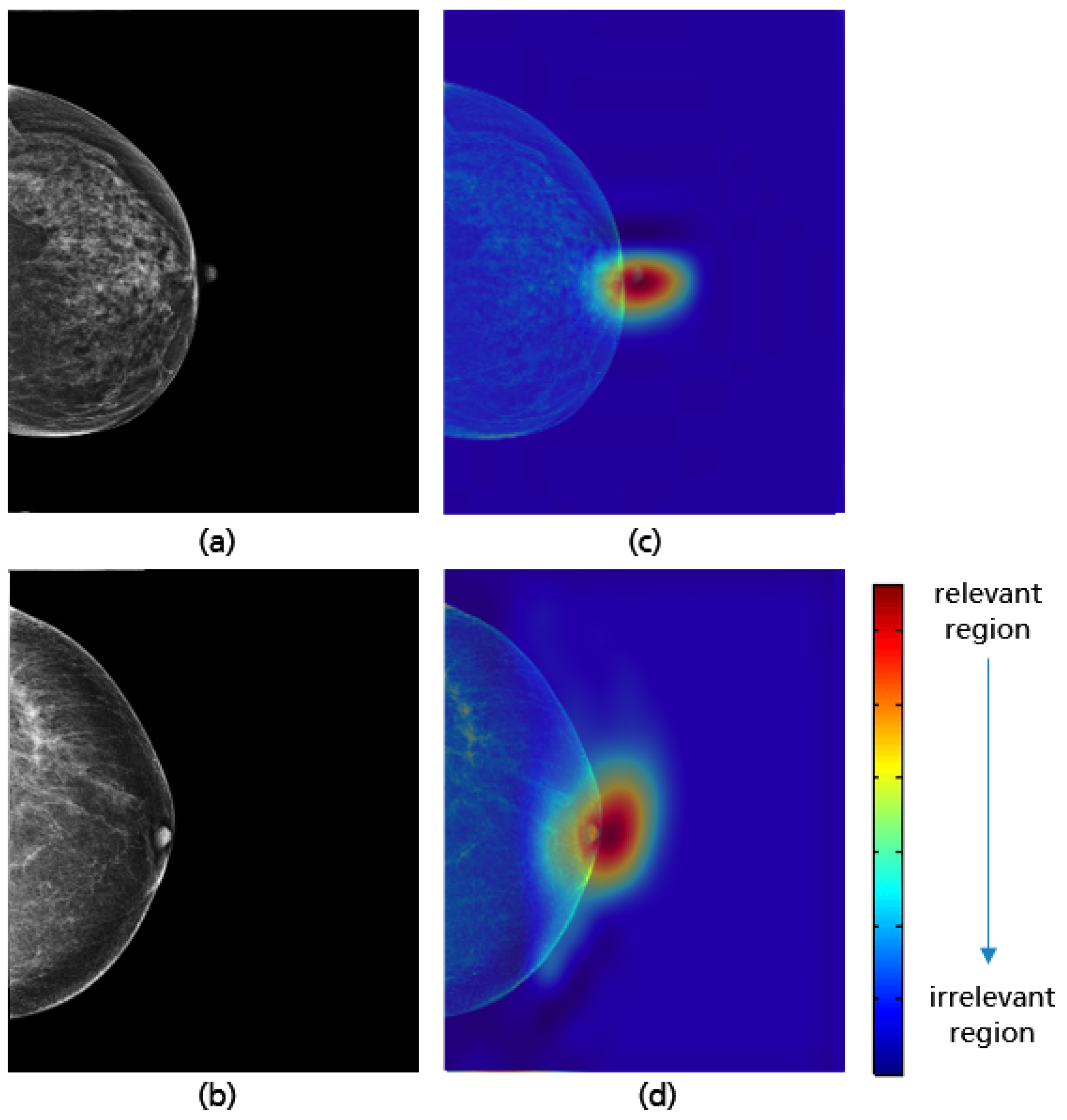
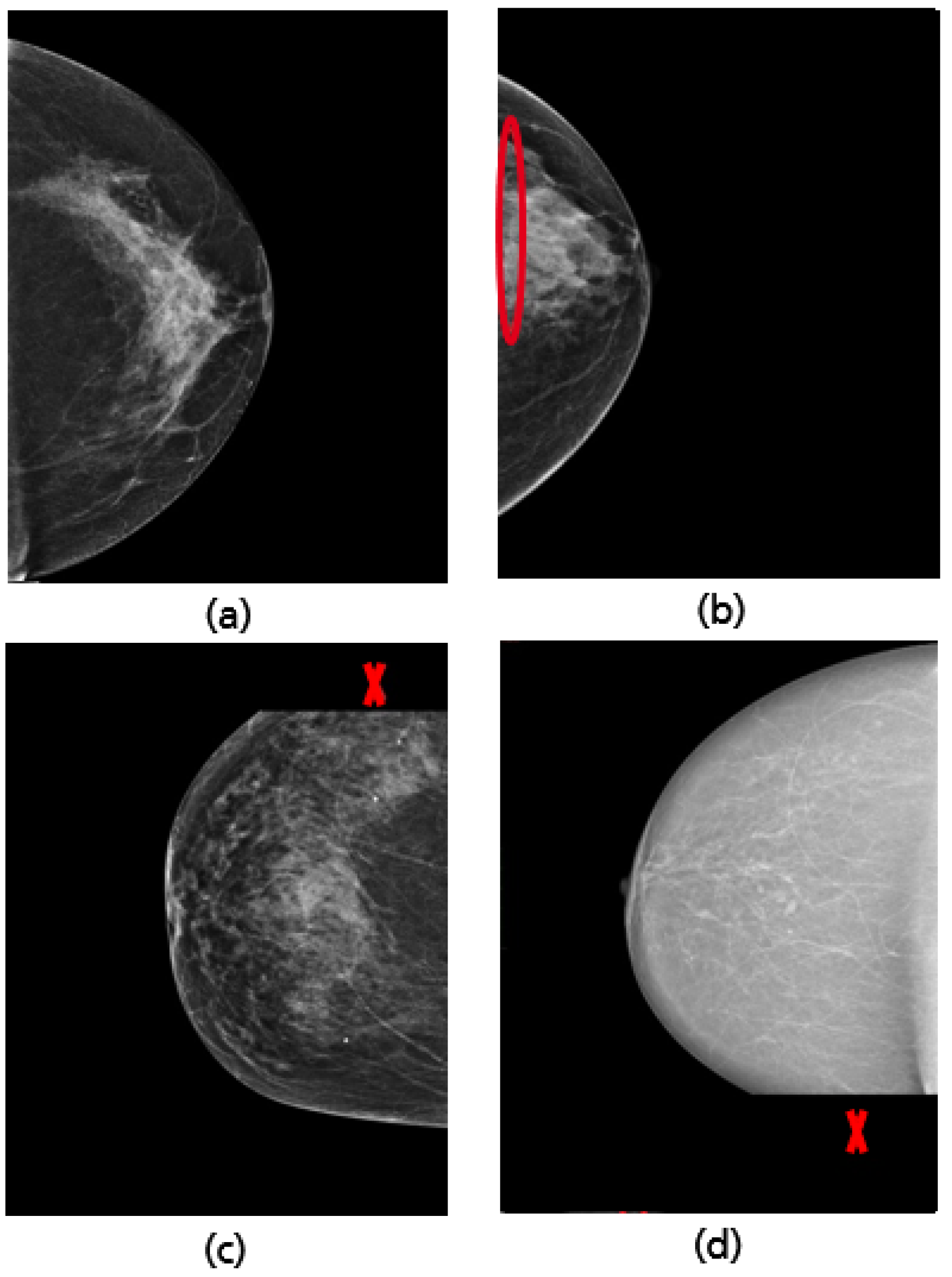
3.3. MLO: Nipple Position
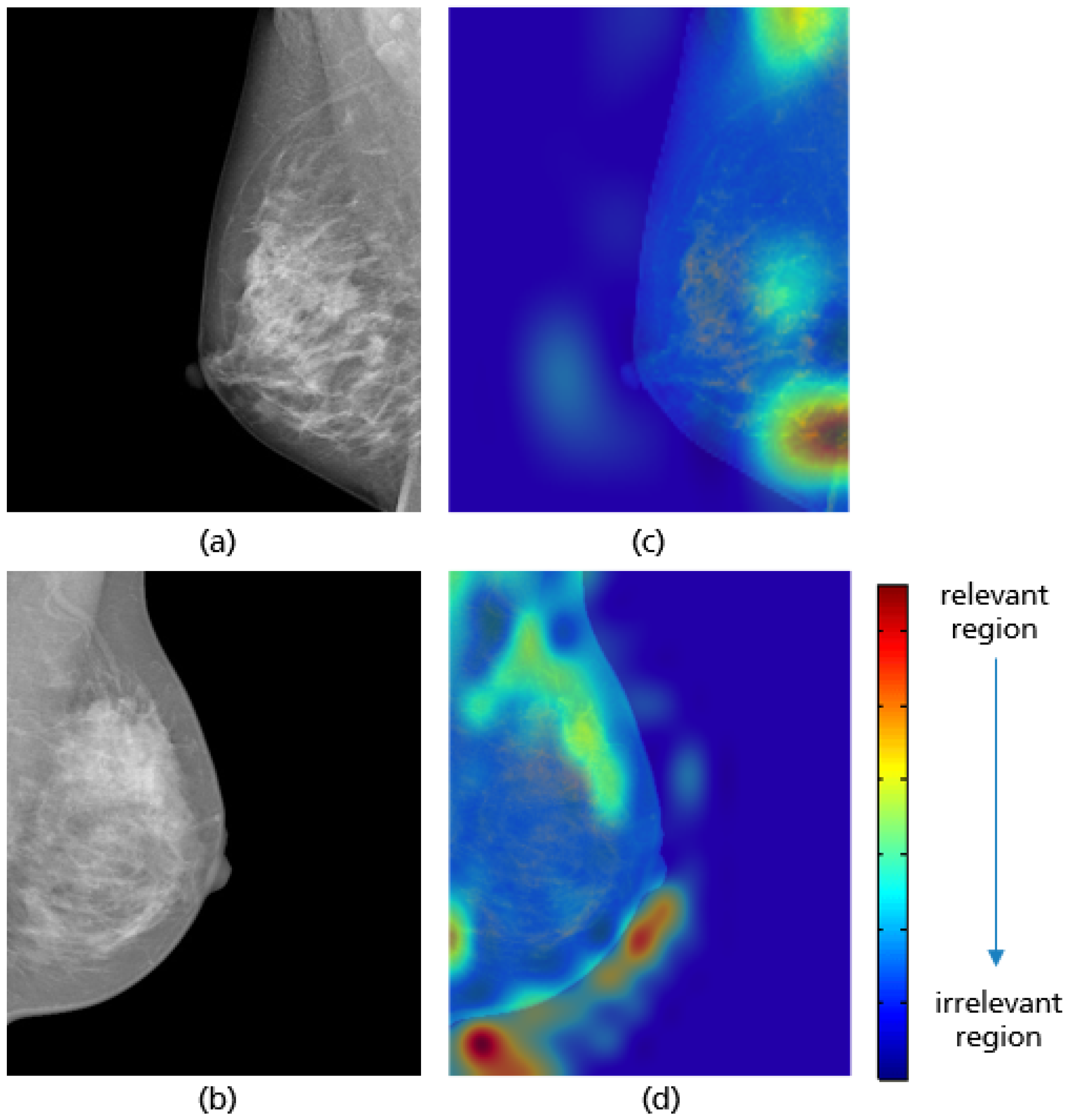
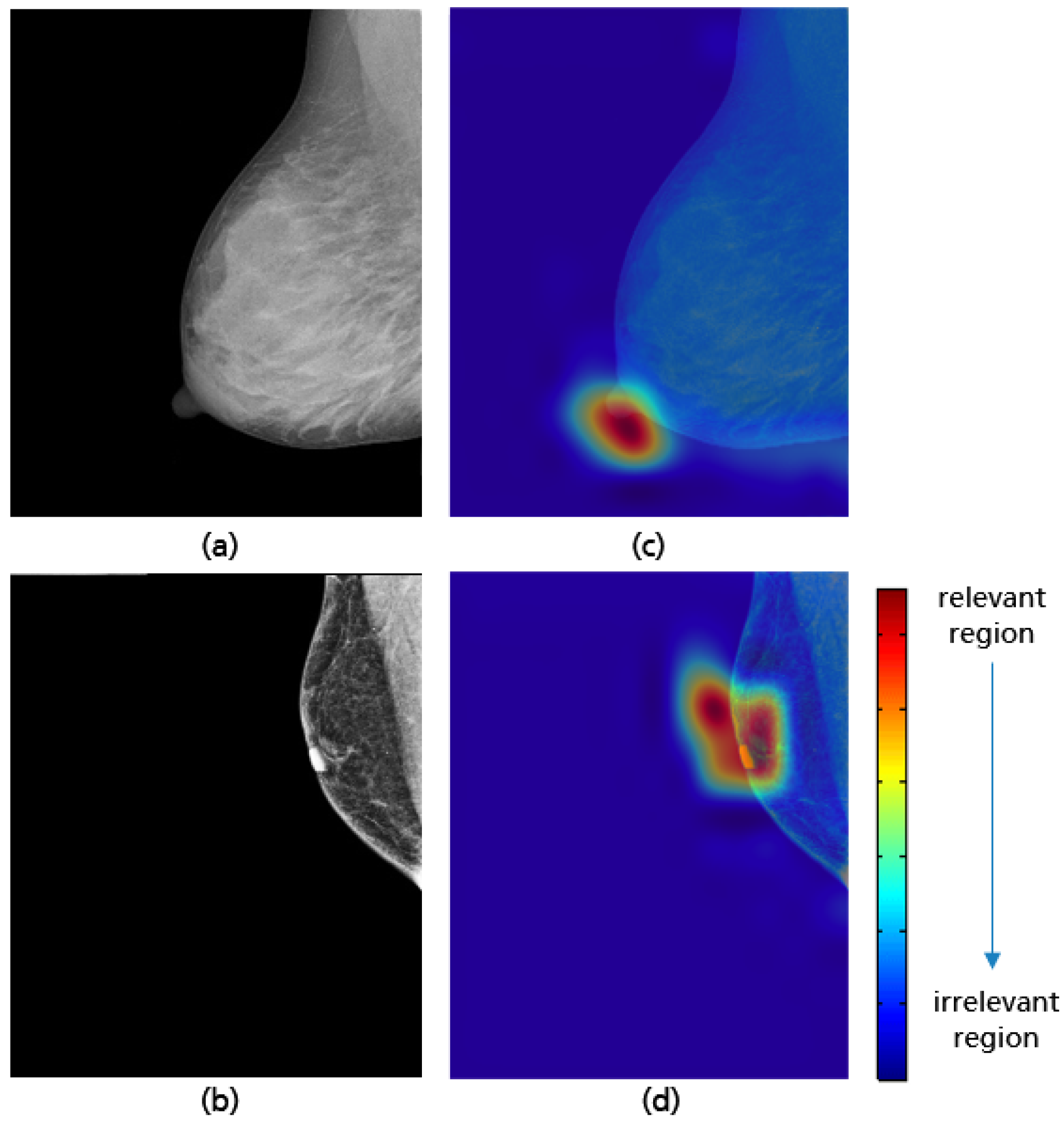
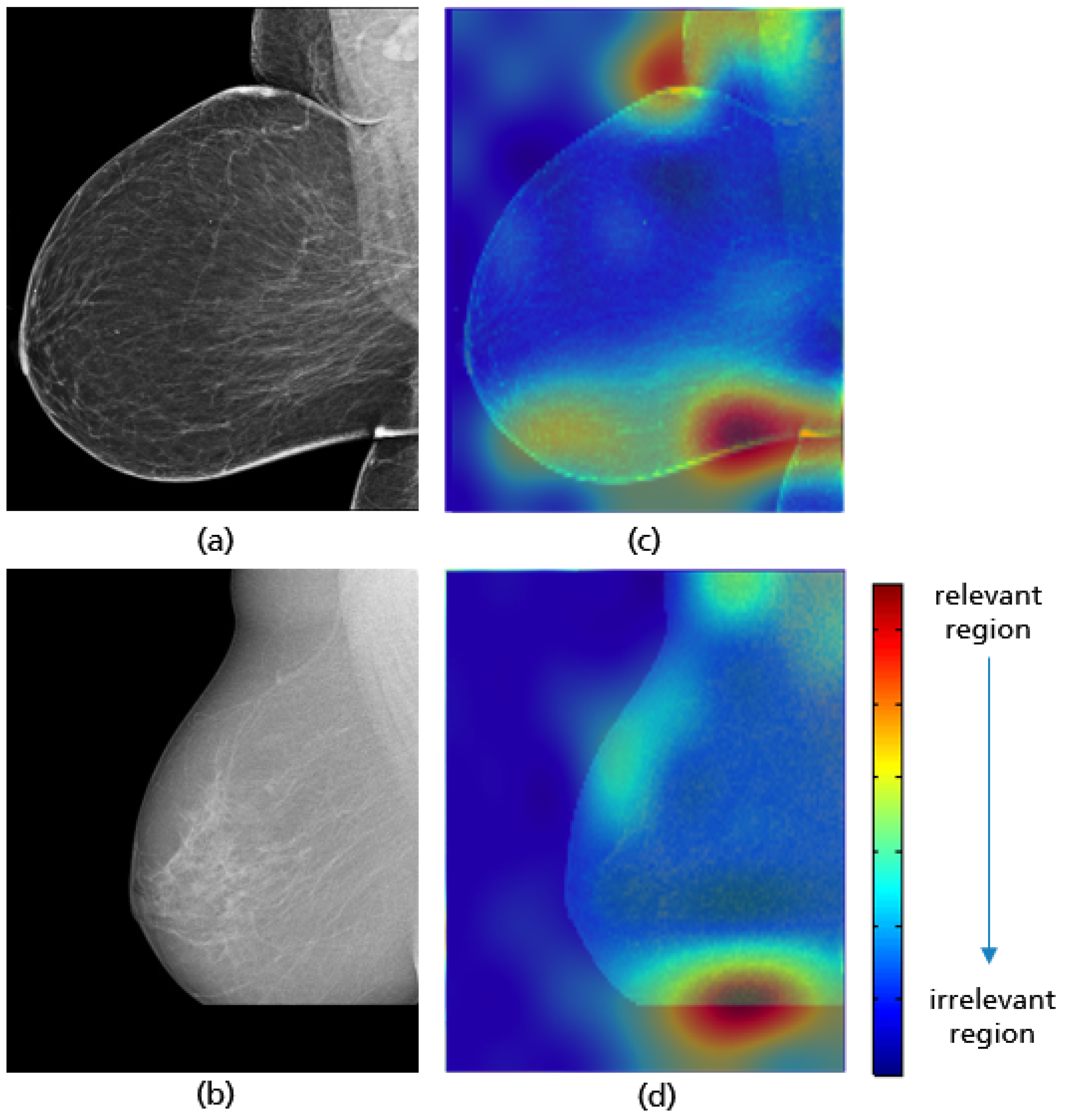
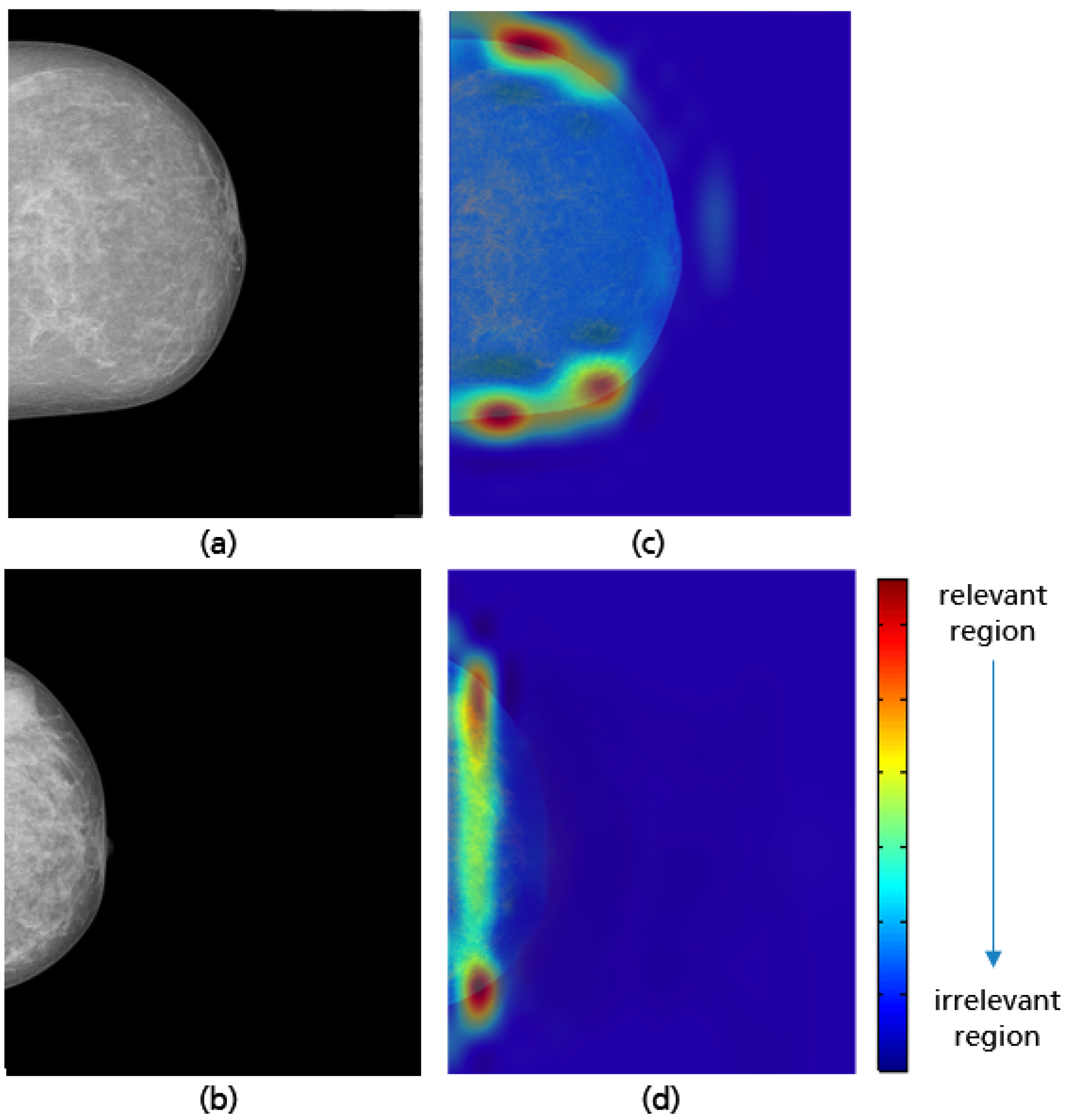
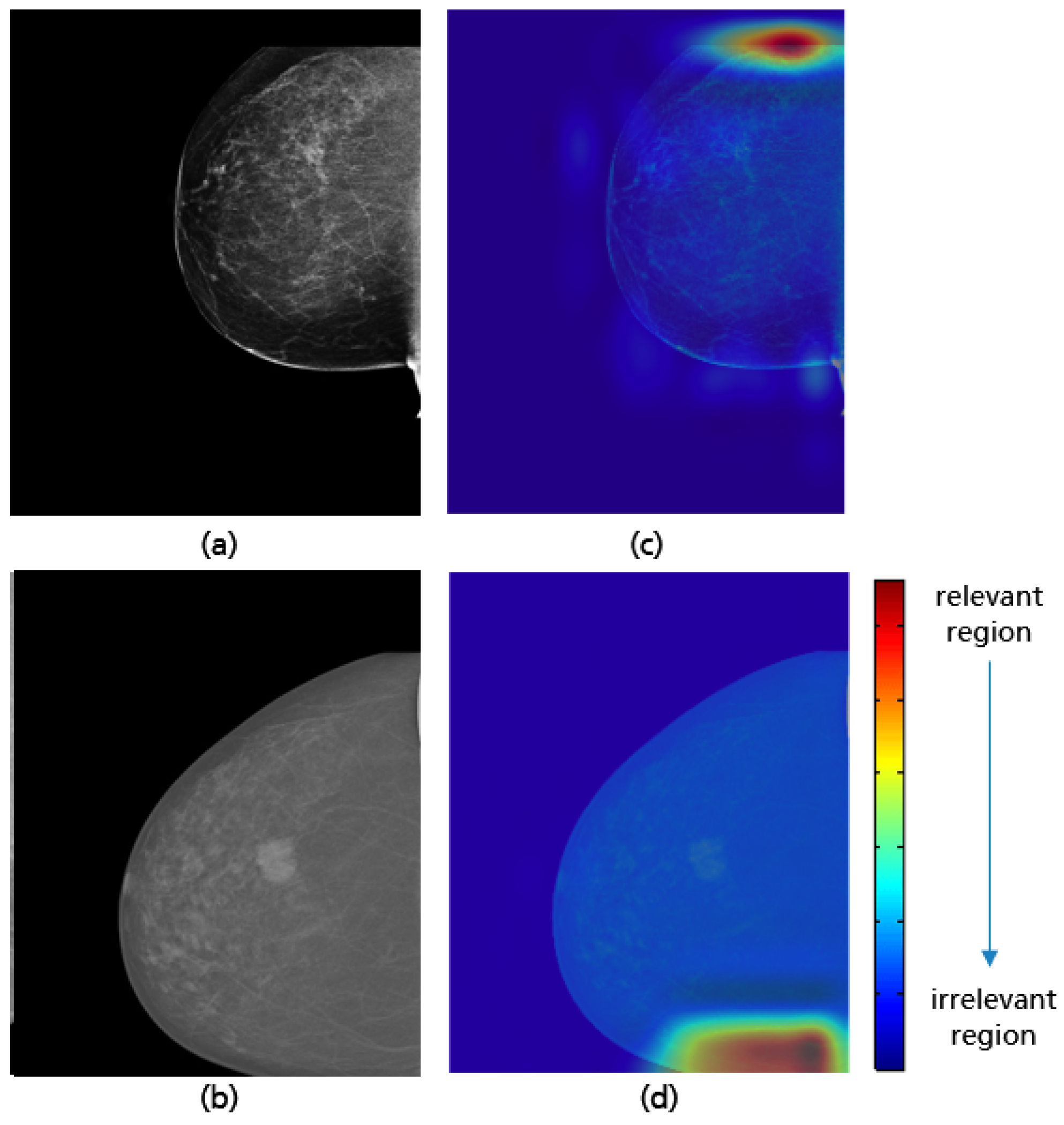
3.4. MLO: Coverage of All Relevant Breast Tissue
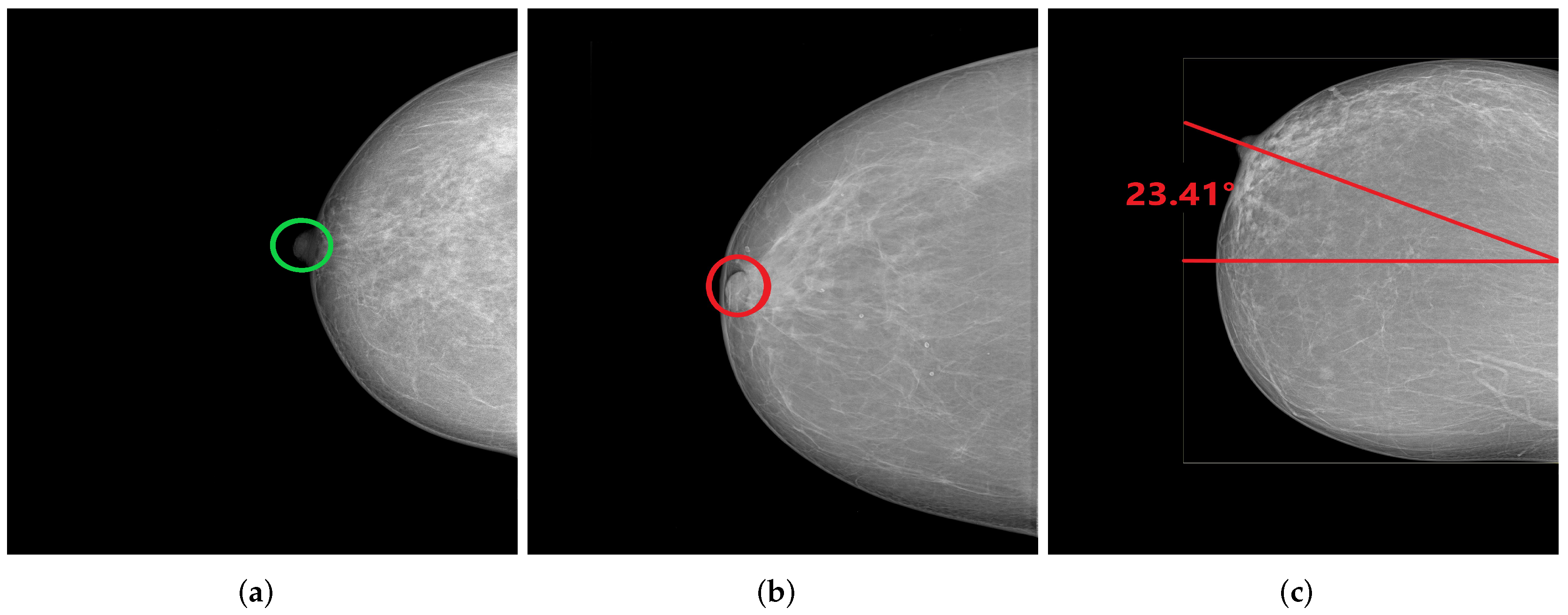
3.5. CC: Nipple Position
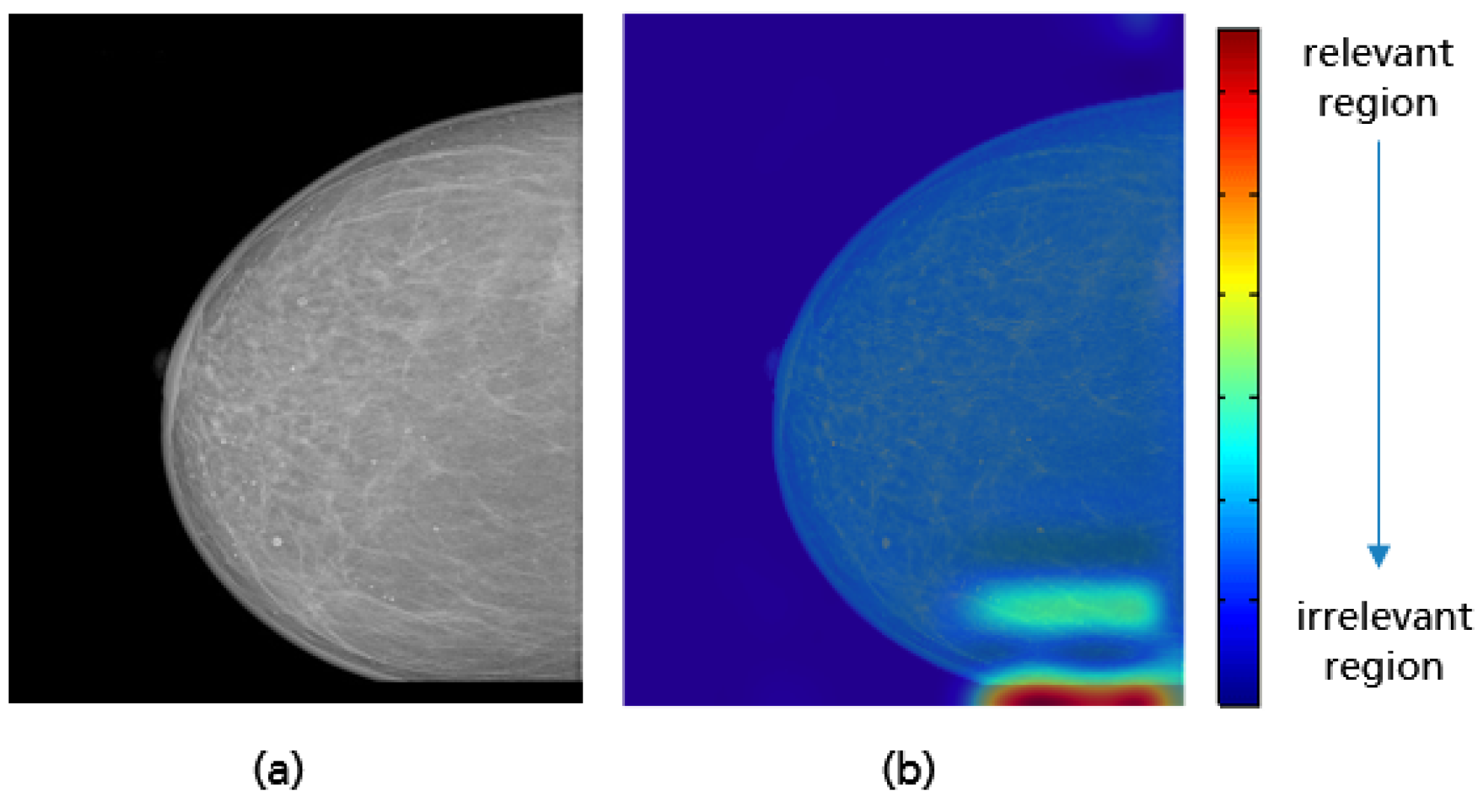
3.6. CC: Coverage of All Relevant Breast Tissue
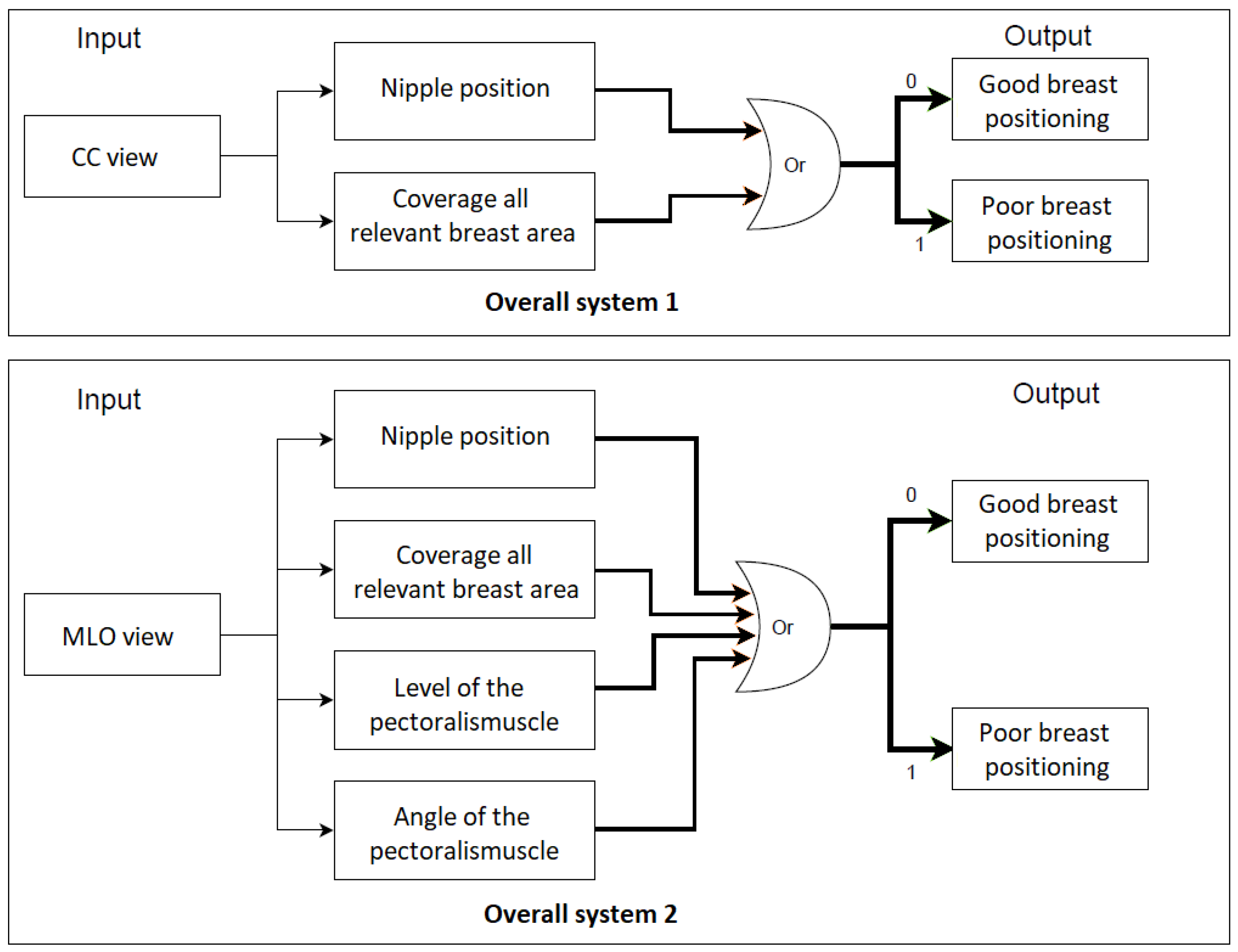
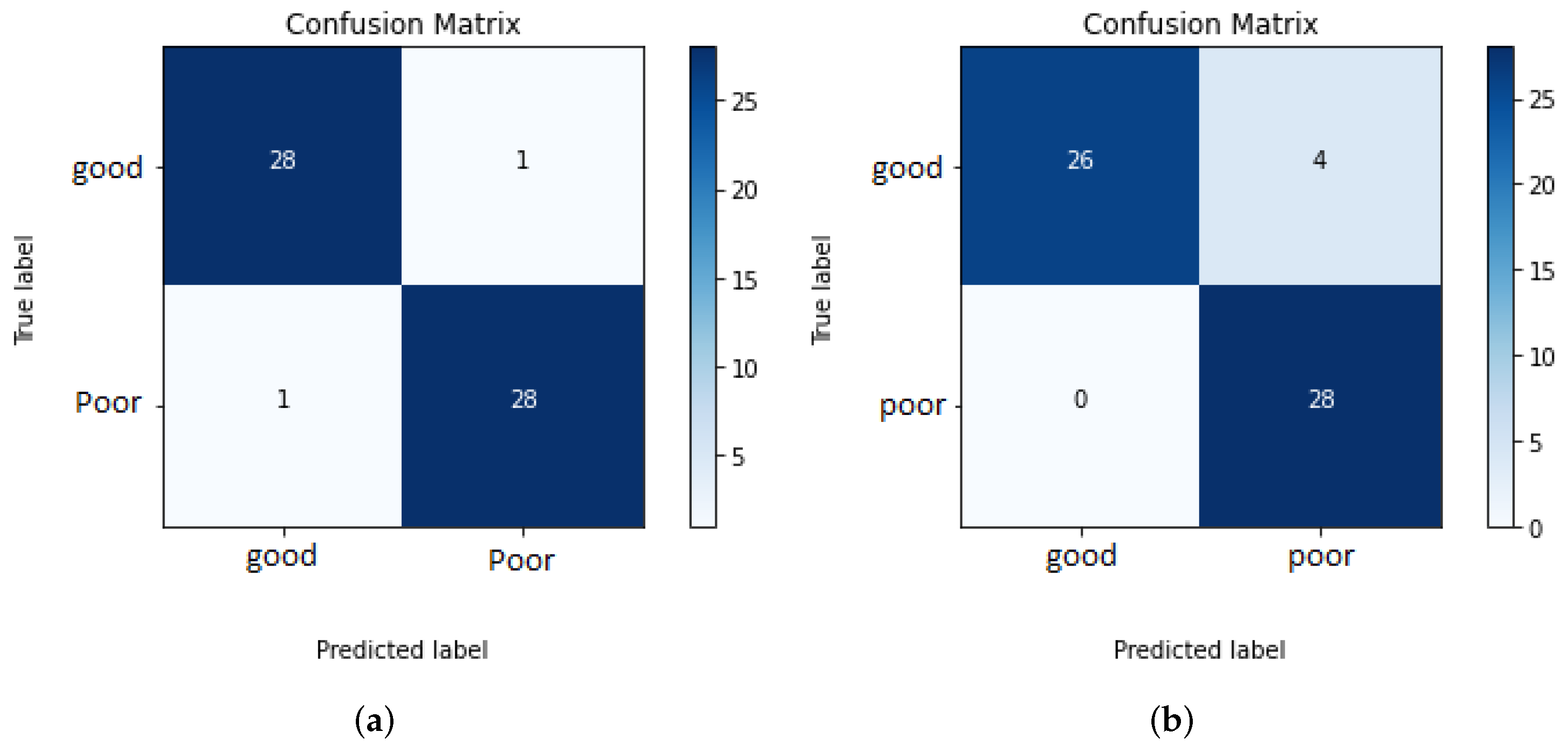
4. Overall Systems and Results
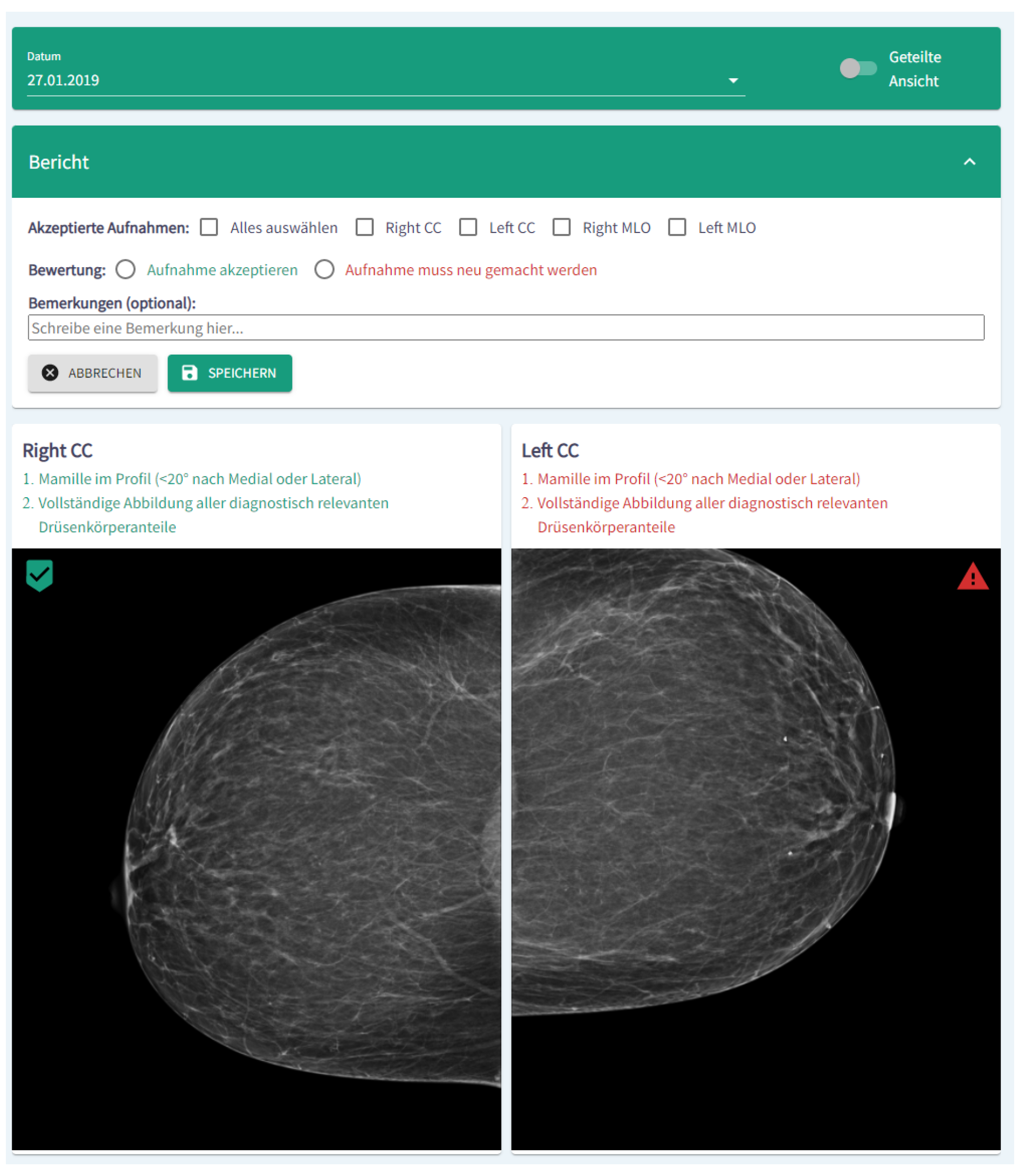
5. Implementation as a Software Module for Clinical Decision Support
6. Discussion
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Shen, L.; Margolies, L.R.; Rothstein, J.H.; Fluder, E.; McBride, R.; Sieh, W. Deep learning to improve breast cancer detection on screening mammography. Sci. Rep. 2019, 9, 12495. [Google Scholar] [CrossRef] [PubMed]
- Duffy, S.W.; Tabár, L.; Chen, H.H.; Holmqvist, M.; Yen, M.F.; Abdsalah, S.; Epstein, B.; Frodis, E.; Ljungberg, E.; Hedborg-Melander, C.; et al. The impact of organized mammography service screening on breast carcinoma mortality in seven Swedish counties. Cancer Interdiscip. Int. J. Am. Cancer Soc. 2002, 95, 458–469. [Google Scholar] [CrossRef] [PubMed]
- Feig, S.A. Image Quality of Screening Mammography: Effect on Clinical Outcome. Am. J. Roentgenol. 2002, 178, 805–807. [Google Scholar] [CrossRef] [PubMed]
- Mackenzie, A.; Warren, L.M.; Wallis, M.G.; Given-Wilson, R.M.; Cooke, J.; Dance, D.R.; Chakraborty, D.P.; Halling-Brown, M.D.; Looney, P.T.; Young, K.C. The relationship between cancer detection in mammography and image quality measurements. Phys. Med. 2016, 32, 568–574. [Google Scholar] [CrossRef] [PubMed]
- US Food and Drug Administration. Poor Positioning Responsible for Most Clinical Image Deficiencies, Failures; US Food and Drug Administration: Silver Spring, MD, USA, 2017.
- Srinivasu, P.N.; SivaSai, J.G.; Ijaz, M.F.; Bhoi, A.K.; Kim, W.; Kang, J.J. Classification of skin disease using deep learning neural networks with MobileNet V2 and LSTM. Sensors 2021, 21, 2852. [Google Scholar] [CrossRef] [PubMed]
- Saha, S.K.; Islam, S.R.; Abdullah-Al-Wadud, M.; Islam, S.; Ali, F.; Park, K.S. Multiomics analysis reveals that GLS and GLS2 differentially modulate the clinical outcomes of cancer. J. Clin. Med. 2019, 8, 355. [Google Scholar] [CrossRef]
- Vulli, A.; Srinivasu, P.N.; Sashank, M.S.K.; Shafi, J.; Choi, J.; Ijaz, M.F. Fine-Tuned DenseNet-169 for Breast Cancer Metastasis Prediction Using FastAI and 1-Cycle Policy. Sensors 2022, 22, 2988. [Google Scholar] [CrossRef]
- KhanID, M.H.M.; Boodoo-Jahangeer, N.; Dullull, W.; Nathire, S.; Gao, X.; Sinha, G.R.; Nagwanshi, K.K. Multi-class classification of breast cancer abnormalities using Deep Convolutional Neural Network (CNN). PLoS ONE 2021, 16, e0256500. [Google Scholar]
- Alanazi, S.A.; Kamruzzaman, M.M.; Sarker, M.N.I.; Alruwaili, M.; Alhwaiti, Y.; Alshammari, N.; Siddiqi, M.H. Boosting Breast Cancer Detection Using Convolutional Neural Network. J. Healthc. Eng. 2021, 2021, 5528622. [Google Scholar] [CrossRef]
- Sechopoulos, I.; Teuwen, J.; Mann, R. Artificial intelligence for breast cancer detection in mammography and digital breast tomosynthesis: State of the art. Semin. Cancer Biol. 2020, 72, 214–225. [Google Scholar] [CrossRef]
- Gupta, V.; Taylor, C.; Bonnet, S.; Prevedello, L.M.; Hawley, J.; White, R.D.; Flores, M.G.; Erdal, B.S. Deep Learning-Based Automatic Detection of Poorly Positioned Mammograms to Minimize Patient Return Visits for Repeat Imaging: A Real-World Application. arXiv 2020, arXiv:2009.13580v1. [Google Scholar]
- Heath, M.; Bowyer, K.; Kopans, D.; Moore, R.; Kegelmeyer, W. The Digital Database for Screening Mammography. In Proceedings of the Fifth International Workshop on Digital Mammography, Toronto, ON, Canada, 11–14 June 2000; pp. 212–218. [Google Scholar]
- Suckling, J.; Astley, S.; Betal, D.; Cerneaz, N.; Dance, D.R.; Kok, S.L.; Parker, J.; Ricketts, I.; Savage, J.; Stamatakis, E.; et al. MIAS: The Mammographic Image Analysis Society. Available online: https://www.repository.cam.ac.uk/handle/1810/250394 (accessed on 2 September 2022).
- Moreira, I.C.; Amaral, I.; Domingues, I.; Cardoso, A.; Cardoso, M.J.; Cardosog, J.S. INbreast: Toward a full-field digital mammographic database. Acad. Radiol. 2012, 19, 236–248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hendrick, R.E. The ACR Mammography Quality Control Manual; American College of Radiology: Reston, VA, USA, 1999. [Google Scholar]
- Bassett, L.W.; Hirbawi, I.A.; DeBruhl, N.; Hayes, M.K. Mammographic positioning: Evaluation from the view box. Radiology 1993, 188, 803–806. [Google Scholar] [CrossRef] [PubMed]
- Bassett, L.W.; Farria, D.M.; Bansal, S.; Farquhar, M.A.; Wilcox, P.A.; Feig, S.A. Reasons for failure of a mammography unit at clinical image review in the American College of Radiology Mammography Accreditation Program. Radiology 2000, 215, 698–702. [Google Scholar] [CrossRef]
- England, P.H. Quality Assurance Guidelines for Mammography Including Radiographic Quality Control; National Health Service Cancer Screening Programmes: Sheffield, UK, 2006. [Google Scholar]
- Amendoeira, I.; Perry, N.; Broeders, M.; de Wolf, C.; Törnberg, S.; Holl, R.; von Karsa, L. European Guidelines for Quality Assurance in Breast Cancer Screening and Diagnosis. In European Reference Organisation for Quality Assured Breast Screening and Diagnostic Services; Office for Official Publications of the European Communities: Luxembourg, 2006. [Google Scholar]
- Ministry of Health. Breast Screen Aotearoa Policy and Quality Standards; Ministry of Health: Wellington, New Zealand, 2016.
- Die Mammographie. DMW-Deutsche Medizinische Wochenschrift 1964, 89, 634–635. [CrossRef]
- Sabino, S.M.P.D.S.; Carvalho, A.; Silva, T.B. Implementation of a Clinical Quality Control Program in a Mammography Screening Service of Brazil. Anticancer. Res. 2014, 34, 5057–5065. [Google Scholar]
- Ute, W.; Rupert, P. Mammographien regelgerecht erstellen: Hinweise zur regelgereichten Erstellung von Aufnahmen. In PraxisWissenSpezial; Kassenaerztliche Bundevereinigung (KBV): Berlin, Germany, 2017. [Google Scholar]
- Kang, Y.J.; Ahn, S.K.; Kim, S.J.; Oh, H.; Han, J.; Ko, E. Relationship between Mammographic Density and Age in the United Arab Emirates Population. J. Oncol. 2019, 2019, 7351350. [Google Scholar] [CrossRef]
- Zhang, C. Medical Image Classification under Class Imbalance; Iowa State University: Ames, IA, USA, 2019. [Google Scholar]
- Ganesan, K.; Acharya, U.R.; Chua, K.C.; Lim, C.M.; Thomas, A.K.; Ng, K.H. Computer-Aided Breast Cancer Detection Using Mammograms: A Review. IEEE Rev. Biomed. Eng. 2012, 6, 77–98. [Google Scholar] [CrossRef]
- Van Engeland, S.; Karssemeijer, N. Combining two mammographic projections in a computer aided mass detection method. Med. Phys. 2007, 34, 898–905. [Google Scholar] [CrossRef]
- Tahmoush, D.; Samet, H. Image Similarity and Asymmetry to Improve Computer-Aided Detection of Breast Cancer. In International Workshop on Digital Mammography; Springer: Berlin/Heidelberg, Germany, 2006; pp. 221–228. [Google Scholar]
- Wang, X.; Li, L.; Xu, W.; Liu, W.; Lederman, D.; Zheng, B. Improving Performance of Computer-aided Detection of Masses by Incorporating Bilateral Mammographic Density Asymmetry: An Assessment. Acad. Radiol. 2012, 19, 303–310. [Google Scholar] [CrossRef]
- Castellino, R.A. Computer aided detection (CAD): An overview. Cancer Imaging 2005, 5, 17–19. [Google Scholar] [CrossRef] [PubMed]
- Kumar, P.; Srivastava, S.; Srivastava, S.; Sai, Y.P. End-to-end improved convolutional neural network model for breast cancer detection using mammographic data. J. Def. Model. Simul. 2020, 8, 1548512920973268. [Google Scholar] [CrossRef]
- O’Shea, K.T.; Nash, R. An Introduction to Convolutional Neural Networks. arXiv 2015, arXiv:1511.08458. [Google Scholar]
- Alzubaidi, L.; Zhang, J.; Humaidi, A.J.; Al-Dujaili, A.; Duan, Y.; Al-Shamma, O.; Santamaría, J.; Fadhel, M.A.; Al-Amidie, M.; Farhan, L. Review of deep learning: Concepts, CNN architectures, challenges, applications, future directions. J. Big Data 2021, 8, 53. [Google Scholar] [CrossRef]
- Malathia, M.; Sinthia, P.; Farzana, F.; Mary, G.A. Breast cancer detection using active contour and classification by deep belief network. Mater. Today Proc. 2021, 45, 2721–2724. [Google Scholar] [CrossRef]
- Zeiler, M.D.; Fergus, R. Visualizing and Understanding Convolutional Networks. In Proceedings of the European Conference on Computer Vision (ECCV), Zurich, Switzerland, 6–12 September 2014; pp. 818–833. [Google Scholar]
- Team, K. Keras Documentation. Developer Guides: The Sequential Model. Available online: https://keras.io/guides/sequential_model (accessed on 15 June 2022).
- Selvaraju, R.R.; Cogswell, M.; Das, A.; Vedantam, R.; Parikh, D.; Batra, D. Grad-CAM: Visual Explanations from Deep Networks via Gradient-based Localization. arXiv 2019, arXiv:1610.02391. [Google Scholar]
- Zhou, B.; Khosla, A.; Lapedriza, A.; Oliva, A.; Torralba, A. Learning Deep Features for Discriminative Localization. arXiv 2015, arXiv:1512.04150. [Google Scholar]
- Pacifici, S. Posterior Nipple Line. Available online: https://radiopaedia.org/articles/posterior-nipple-line?lang=us (accessed on 20 September 2021).
- FHIR Foundation. FHIR Specification v4.0.1 R4. Available online: http://hl7.org/fhir/R4/ (accessed on 30 June 2021).
- Benson, T.; Grieve, G. Principles of Health Interoperability: FHIR, HL7 and SNOMED CT; Springer Nature: Cham, Switzerland, 2021. [Google Scholar]
- Yadav, S.S.; Jadhav, S.M. Deep convolutional neural network based medical image classification for disease diagnosis. J. Big Data 2019, 6, 113. [Google Scholar] [CrossRef] [Green Version]





































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ACR Category | Breast Positioning Quality | |
|---|---|---|
| Good | Poor | |
| ACR1 | 241 | 213 |
| ACR2 | 387 | 291 |
| ACR3 | 113 | 195 |
| ACR4 | 78 | 38 |
| ACR Category | Breast Positioning Quality | |
|---|---|---|
| Good | Poor | |
| ACR1 | 312 | 142 |
| ACR2 | 472 | 206 |
| ACR3 | 206 | 102 |
| ACR4 | 84 | 32 |
| MLO View | ||
|---|---|---|
| Positioning Quality Criteria | Accuracy | F1-Score |
| MLO: Nipple position | 96.2% | 96.3% |
| MLO: Coverage of all relevant breast area | 94.4% | 94.3% |
| MLO: Pectoralismuscle Angle | 94.3% | 94.2% |
| MLO: Pectoralismuscle Level | 96.8% | 96.9% |
| CC View | ||
| Positioning Quality Criteria | Accuracy | F1-Score |
| CC: Nipple position | 98.2% | 98.3% |
| CC: Coverage of all relevant breast area | 97.0% | 97.0% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brahim, M.; Westerkamp, K.; Hempel, L.; Lehmann, R.; Hempel, D.; Philipp, P. Automated Assessment of Breast Positioning Quality in Screening Mammography. Cancers 2022, 14, 4704. https://doi.org/10.3390/cancers14194704
Brahim M, Westerkamp K, Hempel L, Lehmann R, Hempel D, Philipp P. Automated Assessment of Breast Positioning Quality in Screening Mammography. Cancers. 2022; 14(19):4704. https://doi.org/10.3390/cancers14194704
Chicago/Turabian StyleBrahim, Mouna, Kai Westerkamp, Louisa Hempel, Reiner Lehmann, Dirk Hempel, and Patrick Philipp. 2022. "Automated Assessment of Breast Positioning Quality in Screening Mammography" Cancers 14, no. 19: 4704. https://doi.org/10.3390/cancers14194704