
Monitoring of Dabrafenib and Trametinib in Serum and Self-Sampled Capillary Blood in Patients with BRAFV600-Mutant Melanoma
 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Collection of Serum Samples
2.3. Collection of Capillary Blood Samples
2.4. Assessment of Adverse Events
2.5. Quantification of Dabrafenib, Hydroxy-Dabrafenib, and Trametinib in Serum and Capillary Blood
2.6. Data Processing and Statistical Analysis
2.7. Estimation of Pharmacokinetic Parameters Based on Existing Population Pharmacokinetic Models
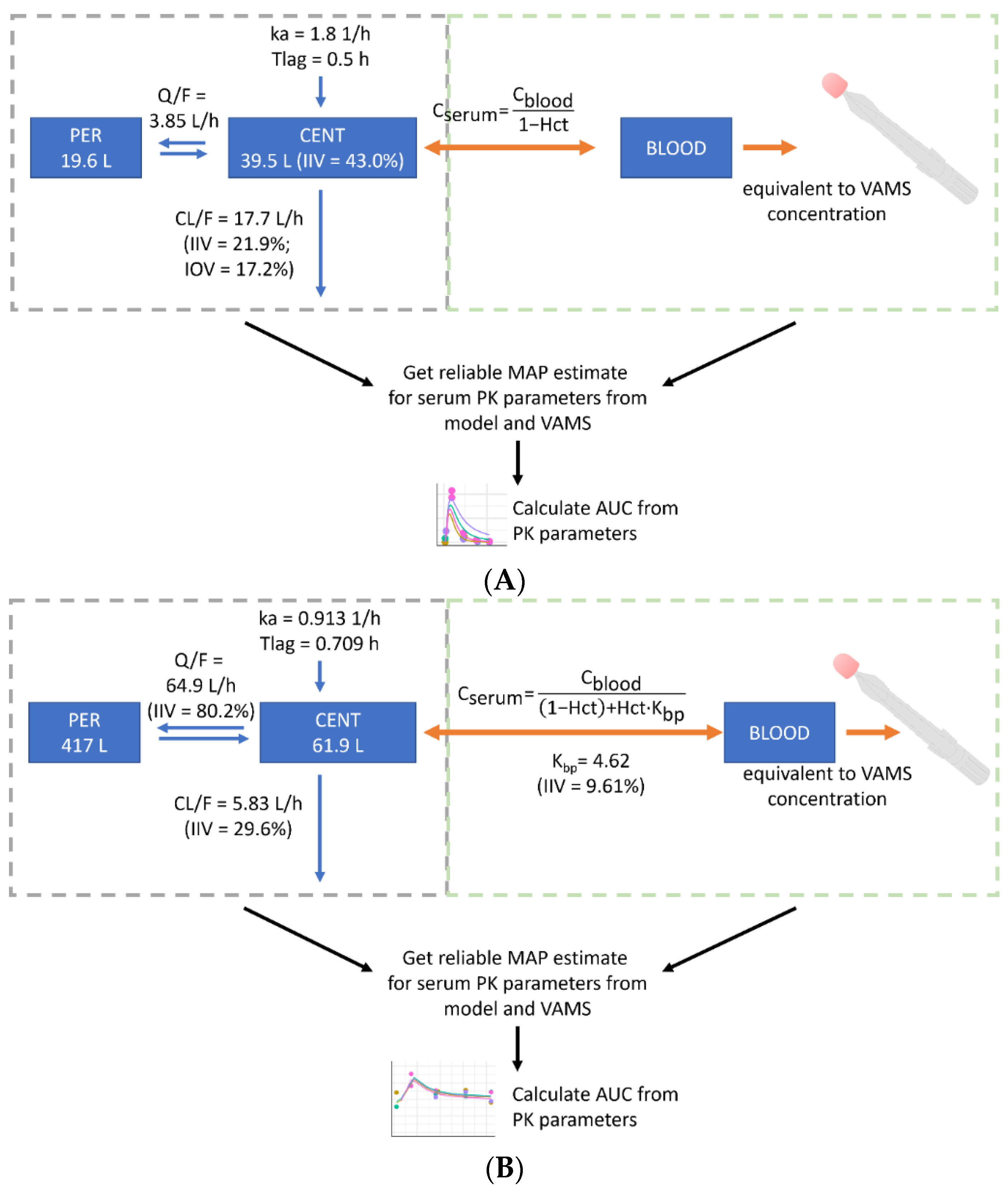
2.8. Development of a New Population Pharmacokinetic Model-Informed VAMS-to-Serum Conversion Model
3. Results
3.1. Patient and Sample Characteristics
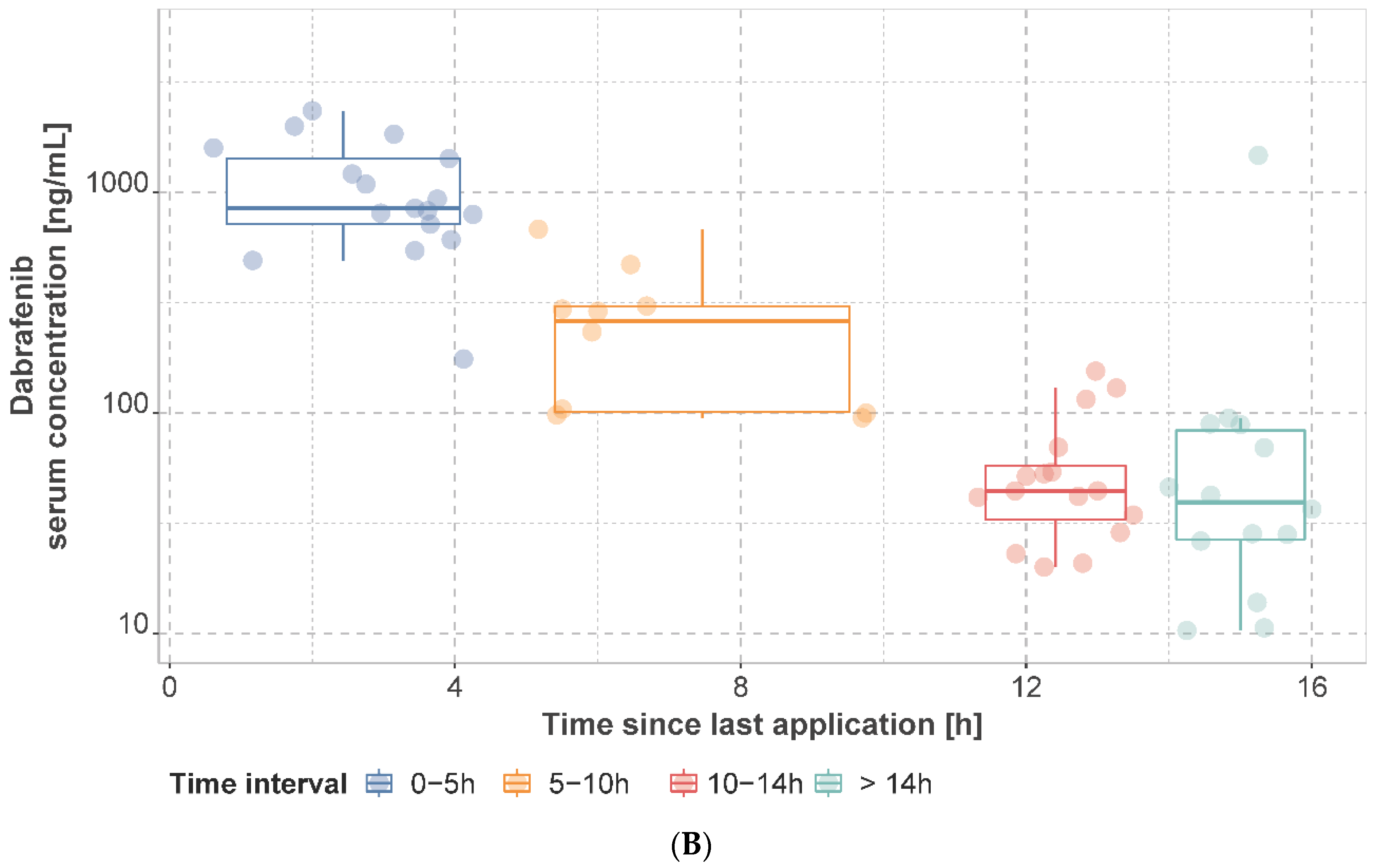
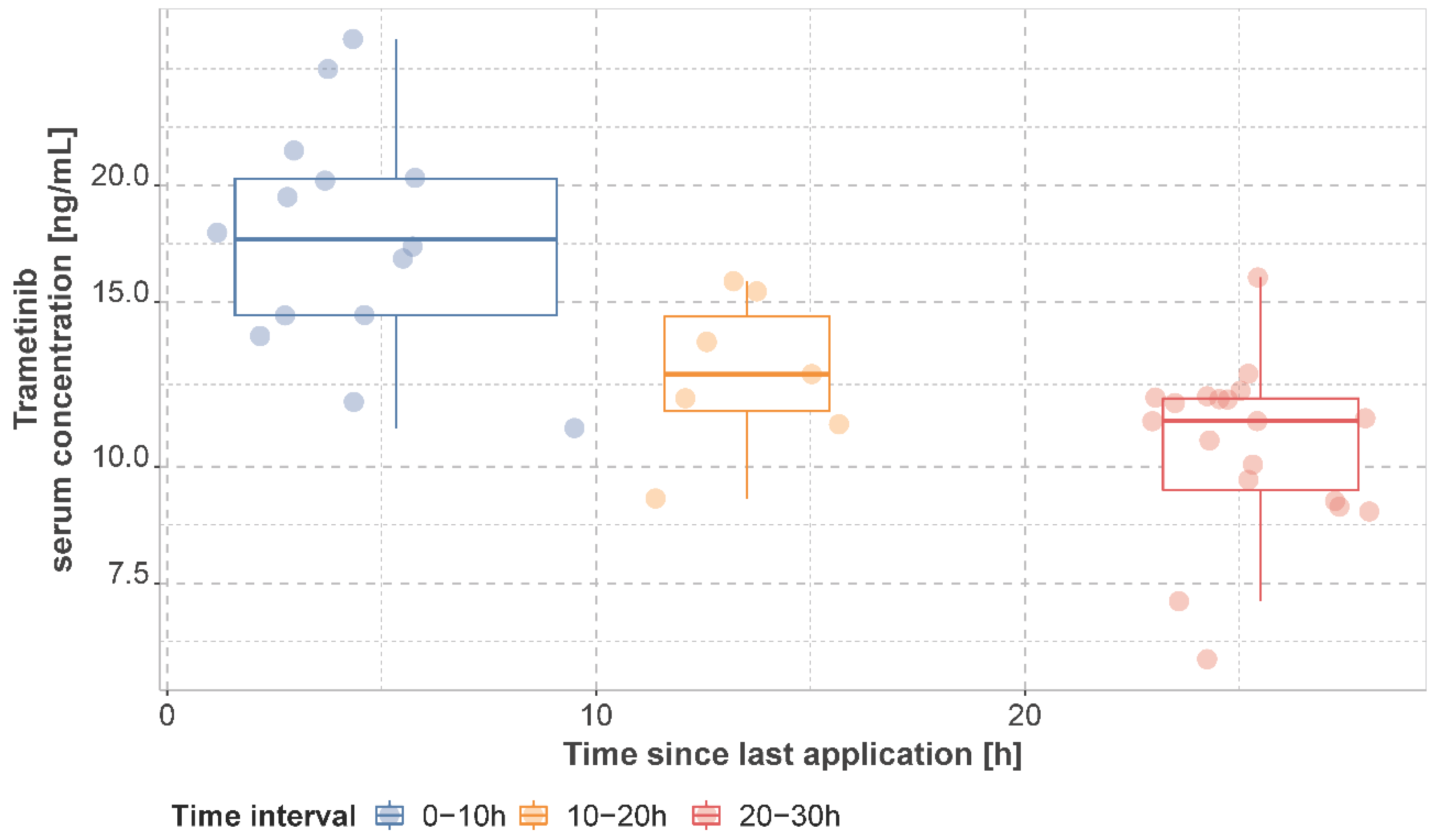
3.2. Observed Dabrafenib, Hydroxy-Dabrafenib, and Trametinib Serum Concentrations
3.3. Estimates for Pharmacokinetic Parameters Based on Existing Population Pharmacokinetic Models
3.4. Adverse Events, Dose Reductions and Treatment Discontinuations
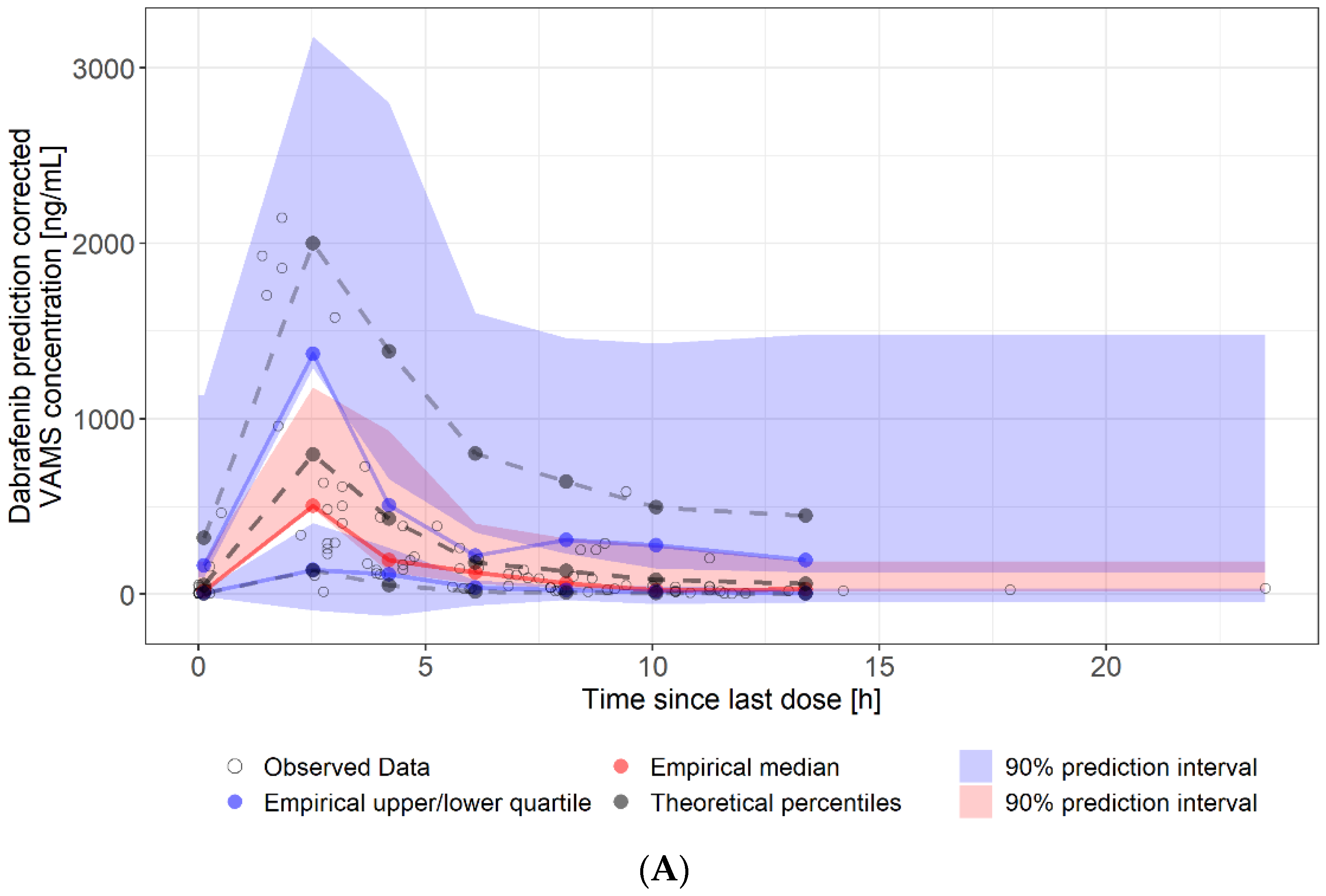
3.5. Estimates for Serum Pharmacokinetic Parameters from Self-Sampled Capillary Blood
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Atkinson, V. Recent Advances in Malignant Melanoma. Intern. Med. J. 2017, 47, 1114–1121. [Google Scholar] [CrossRef] [PubMed]
- U.S. Food and Drug Administration. Highlights of Prescribing Information Tafinlar (Dabrafenib). 2022. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2022/202806s019lbl.pdf (accessed on 29 May 2022).
- U.S. Food and Drug Administration. Highlights of Prescribing Information Mekinist (Trametinib). 2022. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2022/204114s023lbl.pdf (accessed on 29 May 2022).
- Robert, C.; Karaszewska, B.; Schachter, J.; Rutkowski, P.; Mackiewicz, A.; Stroiakovski, D.; Lichinitser, M.; Dummer, R.; Grange, F.; Mortier, L.; et al. Improved Overall Survival in Melanoma with Combined Dabrafenib and Trametinib. N. Engl. J. Med. 2015, 372, 30–39. [Google Scholar] [CrossRef] [PubMed]
- Long, G.V.; Stroyakovskiy, D.; Gogas, H.; Levchenko, E.; de Braud, F.; Larkin, J.; Garbe, C.; Jouary, T.; Hauschild, A.; Grob, J.J.; et al. Combined BRAF and MEK Inhibition versus BRAF Inhibition Alone in Melanoma. N. Engl. J. Med. 2014, 371, 1877–1888. [Google Scholar] [CrossRef] [PubMed]
- Groenland, S.L.; van Eerden, R.a.G.; Westerdijk, K.; Meertens, M.; Koolen, S.L.W.; Moes, D.J.a.R.; de Vries, N.; Rosing, H.; Otten, H.; Vulink, A.J.E.; et al. Therapeutic Drug Monitoring Based Precision Dosing of Oral Targeted Therapies in Oncology: A Prospective Multicentre Study. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2022. online ahead of print. [Google Scholar] [CrossRef]
- Cardoso, E.; Guidi, M.; Blanchet, B.; Schneider, M.P.; Decosterd, L.A.; Buclin, T.; Csajka, C.; Widmer, N. Therapeutic Drug Monitoring of Targeted Anticancer Protein Kinase Inhibitors in Routine Clinical Use: A Critical Review. Ther. Drug Monit. 2020, 42, 33–44. [Google Scholar] [CrossRef] [PubMed]
- Mueller-Schoell, A.; Groenland, S.L.; Scherf-Clavel, O.; van Dyk, M.; Huisinga, W.; Michelet, R.; Jaehde, U.; Steeghs, N.; Huitema, A.D.R.; Kloft, C. Therapeutic Drug Monitoring of Oral Targeted Antineoplastic Drugs. Eur. J. Clin. Pharmacol. 2021, 77, 441–464. [Google Scholar] [CrossRef]
- Rousset, M.; Dutriaux, C.; Bosco-Lévy, P.; Prey, S.; Pham-Ledard, A.; Dousset, L.; Gérard, E.; Bouchet, S.; Canal-Raffin, M.; Titier, K.; et al. Trough Dabrafenib Plasma Concentrations Can Predict Occurrence of Adverse Events Requiring Dose Reduction in Metastatic Melanoma. Clin. Chim. Acta Int. J. Clin. Chem. 2017, 472, 26–29. [Google Scholar] [CrossRef] [PubMed]
- Goldwirt, L.; Louveau, B.; Baroudjian, B.; Allayous, C.; Jouenne, F.; Da Meda, L.; Vu, L.-T.; Sauvageon, H.; Herms, F.; Delyon, J.; et al. Dabrafenib and Trametinib Exposure-Efficacy and Tolerance in Metastatic Melanoma Patients: A Pharmacokinetic-Pharmacodynamic Real-Life Study. Cancer Chemother. Pharmacol. 2021, 88, 427–437. [Google Scholar] [CrossRef]
- Falchook, G.S.; Long, G.V.; Kurzrock, R.; Kim, K.B.; Arkenau, H.-T.; Brown, M.P.; Hamid, O.; Infante, J.R.; Millward, M.; Pavlick, A.; et al. Dose Selection, Pharmacokinetics, and Pharmacodynamics of BRAF Inhibitor Dabrafenib (GSK2118436). Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2014, 20, 4449–4458. [Google Scholar] [CrossRef]
- Balakirouchenane, D.; Guégan, S.; Csajka, C.; Jouinot, A.; Heidelberger, V.; Puszkiel, A.; Zehou, O.; Khoudour, N.; Courlet, P.; Kramkimel, N.; et al. Population Pharmacokinetics/Pharmacodynamics of Dabrafenib Plus Trametinib in Patients with BRAF-Mutated Metastatic Melanoma. Cancers 2020, 12, 931. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Puszkiel, A.; Noé, G.; Bellesoeur, A.; Kramkimel, N.; Paludetto, M.-N.; Thomas-Schoemann, A.; Vidal, M.; Goldwasser, F.; Chatelut, E.; Blanchet, B. Clinical Pharmacokinetics and Pharmacodynamics of Dabrafenib. Clin. Pharmacokinet. 2019, 58, 451–467. [Google Scholar] [CrossRef] [PubMed]
- Zanger, U.M.; Schwab, M. Cytochrome P450 Enzymes in Drug Metabolism: Regulation of Gene Expression, Enzyme Activities, and Impact of Genetic Variation. Pharmacol. Ther. 2013, 138, 103–141. [Google Scholar] [CrossRef] [PubMed]
- Ouellet, D.; Kassir, N.; Chiu, J.; Mouksassi, M.-S.; Leonowens, C.; Cox, D.; DeMarini, D.J.; Gardner, O.; Crist, W.; Patel, K. Population Pharmacokinetics and Exposure-Response of Trametinib, a MEK Inhibitor, in Patients with BRAF V600 Mutation-Positive Melanoma. Cancer Chemother. Pharmacol. 2016, 77, 807–817. [Google Scholar] [CrossRef] [PubMed]
- Mittapalli, R.K.; Vaidhyanathan, S.; Dudek, A.Z.; Elmquist, W.F. Mechanisms Limiting Distribution of the Threonine-Protein Kinase B-RaF(V600E) Inhibitor Dabrafenib to the Brain: Implications for the Treatment of Melanoma Brain Metastases. J. Pharmacol. Exp. Ther. 2013, 344, 655–664. [Google Scholar] [CrossRef] [PubMed]
- Vaidhyanathan, S.; Mittapalli, R.K.; Sarkaria, J.N.; Elmquist, W.F. Factors Influencing the CNS Distribution of a Novel MEK-1/2 Inhibitor: Implications for Combination Therapy for Melanoma Brain Metastases. Drug Metab. Dispos. Biol. Fate Chem. 2014, 42, 1292–1300. [Google Scholar] [CrossRef]
- Ouellet, D.; Gibiansky, E.; Leonowens, C.; O’Hagan, A.; Haney, P.; Switzky, J.; Goodman, V.L. Population Pharmacokinetics of Dabrafenib, a BRAF Inhibitor: Effect of Dose, Time, Covariates, and Relationship with Its Metabolites. J. Clin. Pharmacol. 2014, 54, 696–706. [Google Scholar] [CrossRef]
- Raynal, M.; Alvarez, J.-C.; Saiag, P.; Beauchet, A.; Funck-Brentano, C.; Funck-Brentano, E. Monitoring of Plasma Concentrations of Dabrafenib and Trametinib in Advanced BRAFV600mut Melanoma Patients. Ann. Dermatol. Venereol. 2022, 149, 32–38. [Google Scholar] [CrossRef]
- Kim, K.B.; Kefford, R.; Pavlick, A.C.; Infante, J.R.; Ribas, A.; Sosman, J.A.; Fecher, L.A.; Millward, M.; McArthur, G.A.; Hwu, P.; et al. Phase II Study of the MEK1/MEK2 Inhibitor Trametinib in Patients With Metastatic BRAF-Mutant Cutaneous Melanoma Previously Treated With or Without a BRAF Inhibitor. J. Clin. Oncol. 2013, 31, 482–489. [Google Scholar] [CrossRef]
- Flaherty, K.T.; Robert, C.; Hersey, P.; Nathan, P.; Garbe, C.; Milhem, M.; Demidov, L.V.; Hassel, J.C.; Rutkowski, P.; Mohr, P.; et al. Improved Survival with MEK Inhibition in BRAF-Mutated Melanoma. N. Engl. J. Med. 2012, 367, 107–114. [Google Scholar] [CrossRef]
- Groenland, S.L.; Janssen, J.M.; Nijenhuis, C.; de Vries, N.; Rosing, H.; Wilgenhof, S.; van Thienen, J.V.; Haanen, J.B.a.G.; Blank, C.U.; Beijnen, J.; et al. 567P Exposure-Response Analyses of Dabrafenib and Trametinib in Melanoma Patients. Ann. Oncol. 2020, 31, S486–S487. [Google Scholar] [CrossRef]
- Menzies, A.M.; Ashworth, M.T.; Swann, S.; Kefford, R.F.; Flaherty, K.; Weber, J.; Infante, J.R.; Kim, K.B.; Gonzalez, R.; Hamid, O.; et al. Characteristics of Pyrexia in BRAFV600E/K Metastatic Melanoma Patients Treated with Combined Dabrafenib and Trametinib in a Phase I/II Clinical Trial. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2015, 26, 415–421. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.Y.; Duong, J.K.; Gonzalez, M.; Long, G.V.; Menzies, A.M.; Rizos, H.; Lim, S.Y.; Lee, J.; Boddy, A.V. Pharmacokinetic and Cytokine Profiles of Melanoma Patients with Dabrafenib and Trametinib-Induced Pyrexia. Cancer Chemother. Pharmacol. 2019, 83, 693–704. [Google Scholar] [CrossRef] [PubMed]
- Ette, E.I.; Williams, P.J. Population Pharmacokinetics I: Background, Concepts, and Models. Ann. Pharmacother. 2004, 38, 1702–1706. [Google Scholar] [CrossRef] [PubMed]
- Jelliffe, R.W.; Schumitzky, A.; Van Guilder, M.; Liu, M.; Hu, L.; Maire, P.; Gomis, P.; Barbaut, X.; Tahani, B. Individualizing Drug Dosage Regimens: Roles of Population Pharmacokinetic and Dynamic Models, Bayesian Fitting, and Adaptive Control. Ther. Drug Monit. 1993, 15, 380–393. [Google Scholar] [CrossRef] [PubMed]
- Brocks, D.R.; Hamdy, D.A. Bayesian Estimation of Pharmacokinetic Parameters: An Important Component to Include in the Teaching of Clinical Pharmacokinetics and Therapeutic Drug Monitoring. Res. Pharm. Sci. 2020, 15, 503–514. [Google Scholar] [CrossRef]
- Wakefield, J.; Aarons, L.; Racine-Poon, A. The Bayesian Approach to Population Pharmacokinetic/Pharmacodynamic Modeling. In Proceedings of the Case Studies in Bayesian Statistics; Gatsonis, C., Kass, R.E., Carlin, B., Carriquiry, A., Gelman, A., Verdinelli, I., West, M., Eds.; Springer: New York, NY, USA, 1999; pp. 205–265. [Google Scholar]
- Leil, T.A. A Bayesian Perspective on Estimation of Variability and Uncertainty in Mechanism-Based Models. CPT Pharmacomet. Syst. Pharmacol. 2014, 3, e121. [Google Scholar] [CrossRef] [PubMed]
- Kiang, T.K.L.; Sherwin, C.M.T.; Spigarelli, M.G.; Ensom, M.H.H. Fundamentals of Population Pharmacokinetic Modelling: Modelling and Software. Clin. Pharmacokinet. 2012, 51, 515–525. [Google Scholar] [CrossRef]
- Sulochana, S.P.; Daram, P.; Srinivas, N.R.; Mullangi, R. Review of DBS Methods as a Quantitative Tool for Anticancer Drugs. Biomed. Chromatogr. 2019, 33, e4445. [Google Scholar] [CrossRef]
- Verougstraete, N.; Stove, V.; Verstraete, A.G.; Stove, C.P. Therapeutic Drug Monitoring of Tyrosine Kinase Inhibitors Using Dried Blood Microsamples. Front. Oncol. 2022, 12, 821807. [Google Scholar] [CrossRef]
- Wilhelm, A.J.; den Burger, J.C.G.; Swart, E.L. Therapeutic Drug Monitoring by Dried Blood Spot: Progress to Date and Future Directions. Clin. Pharmacokinet. 2014, 53, 961–973. [Google Scholar] [CrossRef] [Green Version]
- Edelbroek, P.M.; van der Heijden, J.; Stolk, L.M.L. Dried Blood Spot Methods in Therapeutic Drug Monitoring: Methods, Assays, and Pitfalls. Ther. Drug Monit. 2009, 31, 327–336. [Google Scholar] [CrossRef] [PubMed]
- National Cancer Institute. Common Terminology Criteria for Adverse Events (CTCAE) Version 5.0. 2017. Available online: https://ctep.cancer.gov/protocolDevelopment/electronic_applications/docs/CTCAE_v5_Quick_Reference_5x7.pdf (accessed on 21 November 2021).
- Aghai, F.; Zimmermann, S.; Kurlbaum, M.; Jung, P.; Pelzer, T.; Klinker, H.; Isberner, N.; Scherf-Clavel, O. Development and Validation of a Sensitive Liquid Chromatography Tandem Mass Spectrometry Assay for the Simultaneous Determination of Ten Kinase Inhibitors in Human Serum and Plasma. Anal. Bioanal. Chem. 2021, 413, 599–612. [Google Scholar] [CrossRef] [PubMed]
- Balakirouchenane, D.; Khoudour, N.; Guégan, S.; Kramkimel, N.; Franck, N.; Rodier, T.; Goldwasser, F.; Dupin, N.; Aractingi, S.; Vidal, M.; et al. Simultaneous Quantification of Dabrafenib, Hydroxy-Dabrafenib and Trametinib in Human Plasma by Liquid Chromatography-Tandem Mass Spectrometry. J. Pharm. Biomed. Anal. 2021, 193, 113718. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, S.; Aghai, F.; Schilling, B.; Kraus, S.; Grigoleit, G.U.; Kalogirou, C.; Goebeler, M.-E.; Jung, P.; Pelzer, T.; Klinker, H.; et al. Volumetric Absorptive Microsampling (VAMS) for the Quantification of Ten Kinase Inhibitors and Determination of Their in Vitro VAMS-to-Plasma Ratio. J. Pharm. Biomed. Anal. 2022, 211, 114623. [Google Scholar] [CrossRef] [PubMed]
- Iacuzzi, V.; Posocco, B.; Zanchetta, M.; Gagno, S.; Poetto, A.S.; Guardascione, M.; Toffoli, G. Dried Blood Spot Technique Applied in Therapeutic Drug Monitoring of Anticancer Drugs: A Review on Conversion Methods to Correlate Plasma and Dried Blood Spot Concentrations. Pharm. Res. 2021, 38, 759–778. [Google Scholar] [CrossRef]
- European Medicines Agency. Tafinlar: EPAR—Product Information. 2021. Available online: https://www.ema.europa.eu/en/documents/product-information/tafinlar-epar-product-information_en.pdf (accessed on 30 July 2022).
- European Medicines Agency. Mekinist: EPAR—Product Information. 2022. Available online: https://www.ema.europa.eu/en/documents/product-information/mekinist-epar-product-information_en.pdf (accessed on 30 July 2022).







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Characteristic | No. of Patients | % |
|---|---|---|
| Total | 27 | |
| Age, median (range) | 66 (40–76) | |
| Weight (kg), mean (range) | 81.2 (54.4–115) | |
| Height (cm), mean (range) | 174.4 (164–186) a | |
| BMI (kg/m²), median (range), (IQR) | 26.7 (18.3–39.3) a | |
| Gender | ||
| Male | 19 | 70.4 |
| Female | 8 | 29.6 |
| Ethnicity | ||
| Caucasian | 27 | 100 |
| Smoking status | ||
| Smoker | 4 | 14.8 |
| Non-smoker | 22 | 81.5 |
| Unknown | 1 | 3.7 |
| CYP inhibitors | No. of occasions (patients) | |
| Strong CYP2C8 inhibitor | ||
| 1 inhibitor | 265 (27) | 95.3 |
| none | 13 (2) | 4.7 |
| Moderate CYP2C8 inhibitor | ||
| 2 inhibitors | 5 (1) | 1.8 |
| 1 inhibitor | 94 (10) | 33.8 |
| none | 179 (18) | 64.4 |
| Strong or moderate CYP3A4 inhibitor | ||
| 1 inhibitor | 2 b (2) | 0.7 |
| none | 276 (27) | 99.3 |
| P-gp inhibitors | ||
| 3 inhibitors | 19 (3) | 6.9 |
| 2 inhibitors | 41 (5) | 14.7 |
| 1 inhibitor | 89 (9) | 32.0 |
| none | 129 (15) | 46.4 |
| P-gp inducers | ||
| 2 inducers | 6 c (1) | 2.2 |
| 1 inducer | 105 (11) | 37.8 |
| none | 167 (18) | 60.0 |
| Proton pump inhibitor | ||
| Yes | 84 (9) | 30.2 |
| No | 194 (21) | 69.8 |
| AJCC staged | No. of patients | |
| Stage IIIB | 5 | 18.5 |
| Stage IIIC | 6 | 22.2 |
| Stage IIID | 1 | 3.7 |
| Stage IV | 15 | 55.6 |
| Duration of treatment at enrollment (days), median (range) | ||
| Dabrafenib | 146 (11–1494) | |
| Trametinib | 146 (11–1466) | |
| Median time in study (range) | 324 (26–714) |
| ID | Occasion | Dose [mg/12 h] | Ind V1/F [L] | Ind CL/F [L/h] | Simulated AUCτ for 150 mg q12h [ng·h/L] | Average Simulated AUCτ for 150 mg q12h Using at-Home VAMS [ng·h/L] | Average Simulated AUCτ for 150 mg q12h Using Untimed Serum Sampling [ng·h/L] |
|---|---|---|---|---|---|---|---|
| DT002 | 1 | 150 | 30.8 | 13.5 | 11,125 | 9045 | 7809 |
| DT002 | 2 | 150 | 30.8 | 17.2 | 8815 | ||
| DT002 | 3 | 150 | 30.8 | 21.1 | 7195 | ||
| DT005 | 1 | 150 | 24.7 | 20.7 | 7345 | 7345 | 6240 |
| DT010 | 1 | 150 | 14.3 | 18.5 | 8254 | 8443 | 3610 |
| DT010 | 2 | 150 | 14.3 | 33.3 | 4530 | ||
| DT010 | 3 | 150 | 14.3 | 12.1 | 12,544 | ||
| DT014 | 1 | 150 | 30.2 | 30.1 | 5005 | 5005 | 3145 |
| DT018 | 1 | 150 | 82.5 | 24.7 | 6081 | 6259 | 5944 |
| DT018 | 2 | 150 | 82.5 | 14.9 | 10,223 | ||
| DT018 | 3 | 150 | 82.5 | 37.5 | 4046 | ||
| DT018 | 4 | 150 | 82.5 | 32.3 | 4686 | ||
| DT019 | 1 | 150 | 39.5 | 33.1 | 4563 | 8925 | 5709 |
| DT019 | 2 | 150 | 39.5 | 15.8 | 9501 | ||
| DT019 | 3 | 150 | 39.5 | 9.8 | 15,347 | ||
| DT019 | 4 | 150 | 39.5 | 24.2 | 6288 | ||
| DT026 | 1 | 100 | 40.3 | 33.3 | 4530 | 4035 | 4999 |
| DT026 | 2 | 100 | 40.3 | 41.1 | 3674 | ||
| DT026 | 3 | 100 | 40.3 | 38.7 | 3903 | ||
| DT027 | 1 | 150 | 71.5 | 28.6 | 5287 | 5302 | 6350 |
| DT027 | 2 | 150 | 71.5 | 23.2 | 6457 | ||
| DT027 | 3 | 150 | 71.5 | 36.5 | 4164 |
| ID | Dose [mg/24 h] | Ind Q/F [L/h] | Ind CL/F [L/h] | Ind Kbp | Simulated AUCτ for 2 mg q24h Using at-Home VAMS [ng·h/L] | Simulated AUCτ for 2 mg q24h Using Untimed Serum Sampling [ng·h/L] |
|---|---|---|---|---|---|---|
| DT002 | 2 | 97.65 | 6.07 | 4.84 | 326 | 358 |
| DT010 | 2 | 125.55 | 6.63 | 4.98 | 299 | 300 |
| DT014 | 2 | 129.17 | 8.36 | 5.36 | 239 | 326 |
| DT018 | 1 | 185.04 | 3.52 | 3.89 | 527 | 252 |
| DT019 | 1.5 | 77.82 | 3.79 | 3.91 | 496 | 336 |
| DT026 | 2 | 106.5 | 6.25 | 4.38 | 317 | 303 |
| DT027 | 2 | 65.04 | 6.95 | 4.41 | 286 | 304 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Isberner, N.; Gesierich, A.; Balakirouchenane, D.; Schilling, B.; Aghai-Trommeschlaeger, F.; Zimmermann, S.; Kurlbaum, M.; Puszkiel, A.; Blanchet, B.; Klinker, H.; et al. Monitoring of Dabrafenib and Trametinib in Serum and Self-Sampled Capillary Blood in Patients with BRAFV600-Mutant Melanoma. Cancers 2022, 14, 4566. https://doi.org/10.3390/cancers14194566
Isberner N, Gesierich A, Balakirouchenane D, Schilling B, Aghai-Trommeschlaeger F, Zimmermann S, Kurlbaum M, Puszkiel A, Blanchet B, Klinker H, et al. Monitoring of Dabrafenib and Trametinib in Serum and Self-Sampled Capillary Blood in Patients with BRAFV600-Mutant Melanoma. Cancers. 2022; 14(19):4566. https://doi.org/10.3390/cancers14194566
Chicago/Turabian StyleIsberner, Nora, Anja Gesierich, David Balakirouchenane, Bastian Schilling, Fatemeh Aghai-Trommeschlaeger, Sebastian Zimmermann, Max Kurlbaum, Alicja Puszkiel, Benoit Blanchet, Hartwig Klinker, and et al. 2022. "Monitoring of Dabrafenib and Trametinib in Serum and Self-Sampled Capillary Blood in Patients with BRAFV600-Mutant Melanoma" Cancers 14, no. 19: 4566. https://doi.org/10.3390/cancers14194566