
Targeting the Tumor Microenvironment through mTOR Inhibition and Chemotherapy as Induction Therapy for Locally Advanced Head and Neck Squamous Cell Carcinoma: The CAPRA Study
 ,
,  , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Study Design and Treatment
2.3. On-Study Evaluation
2.4. Endpoints and Statistics
2.5. Translational Research
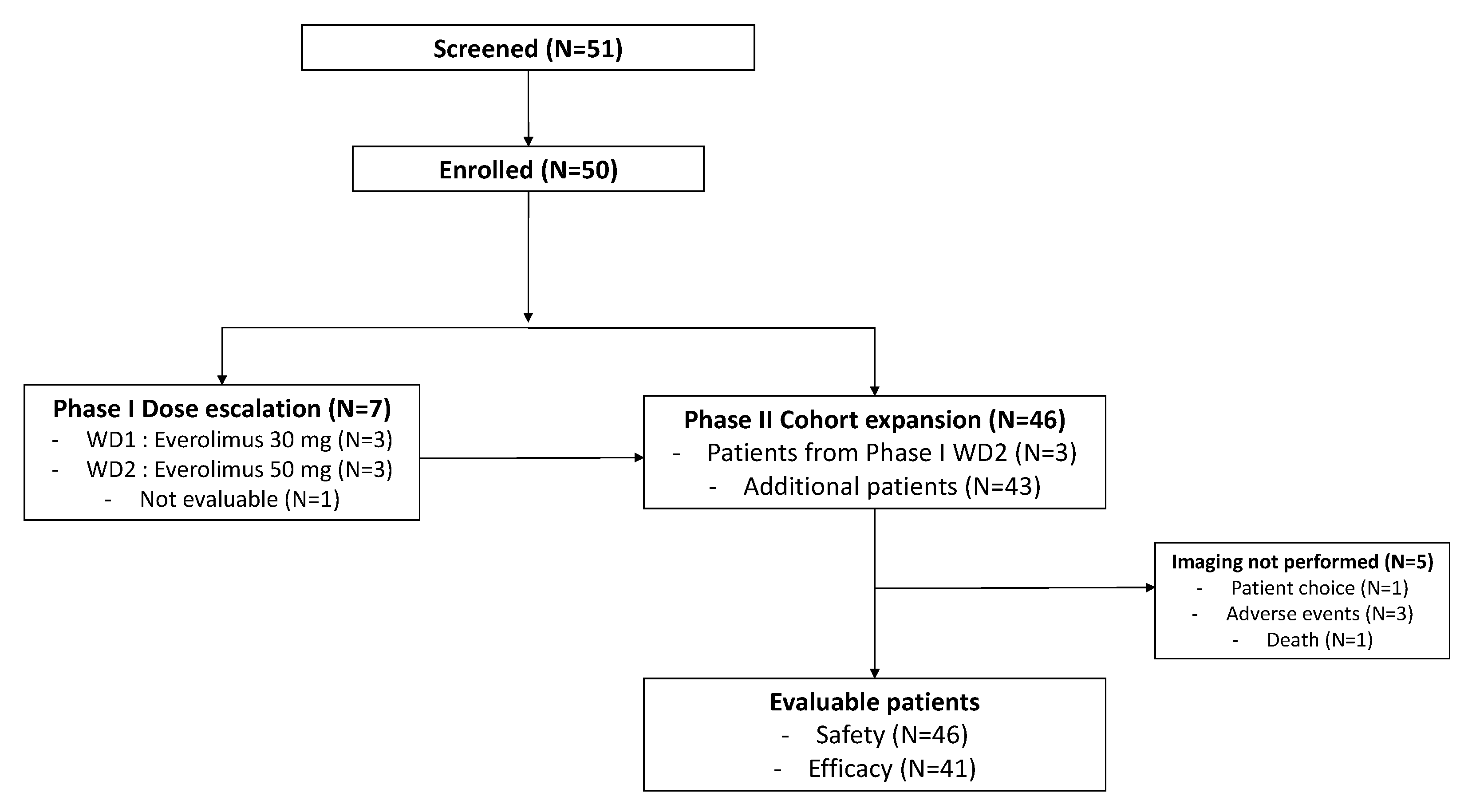
3. Results
3.1. Patient Characteristics
3.2. Dosing and Toxicity
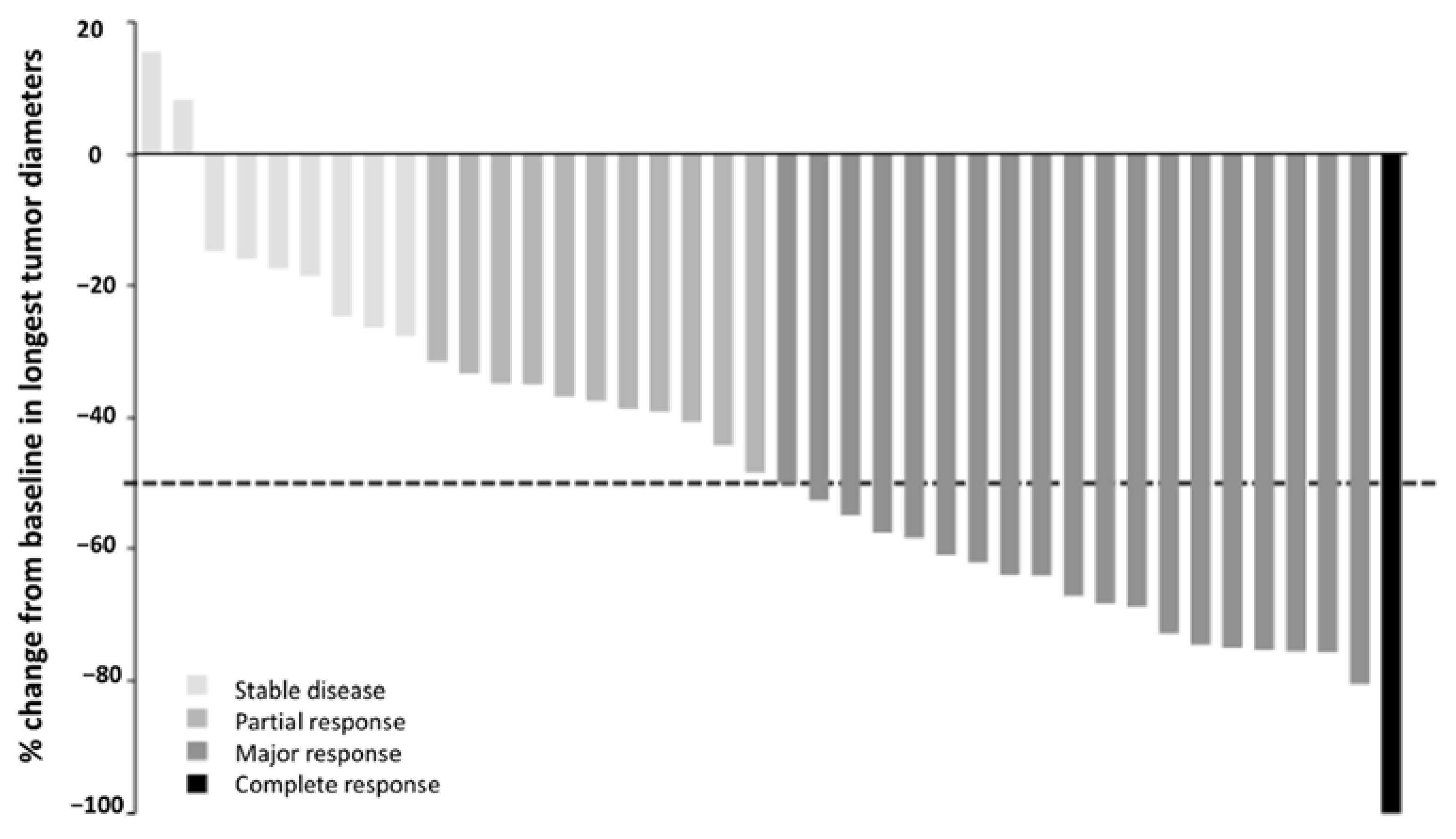
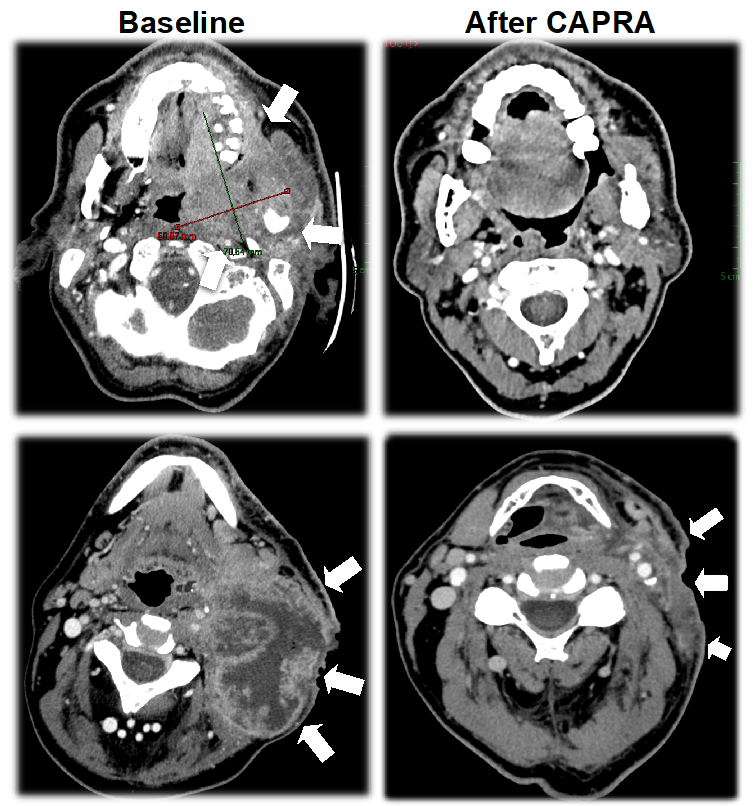
3.3. Activity
3.4. Translational Research
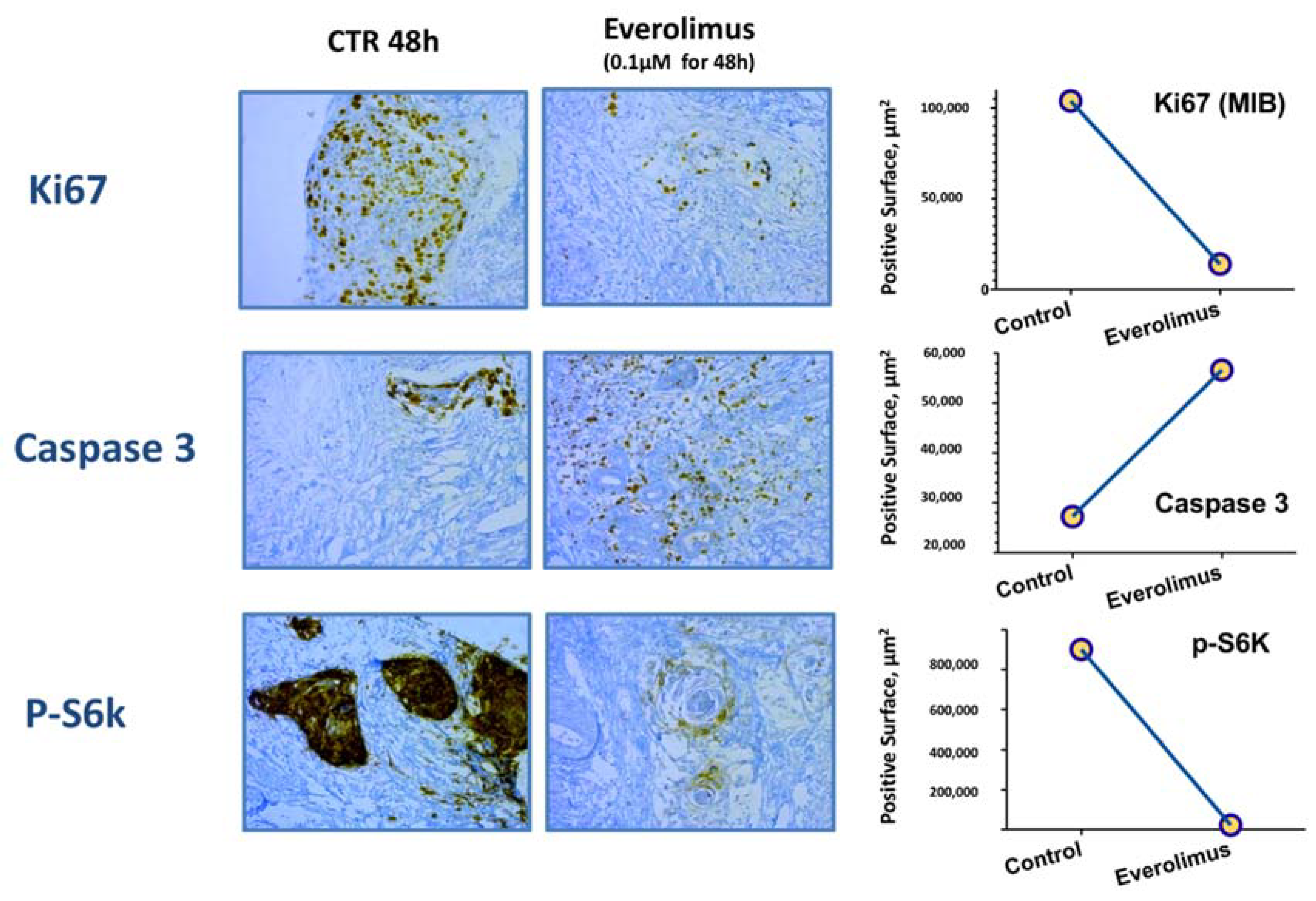
3.4.1. Ex Vivo Pharmacodynamic Study
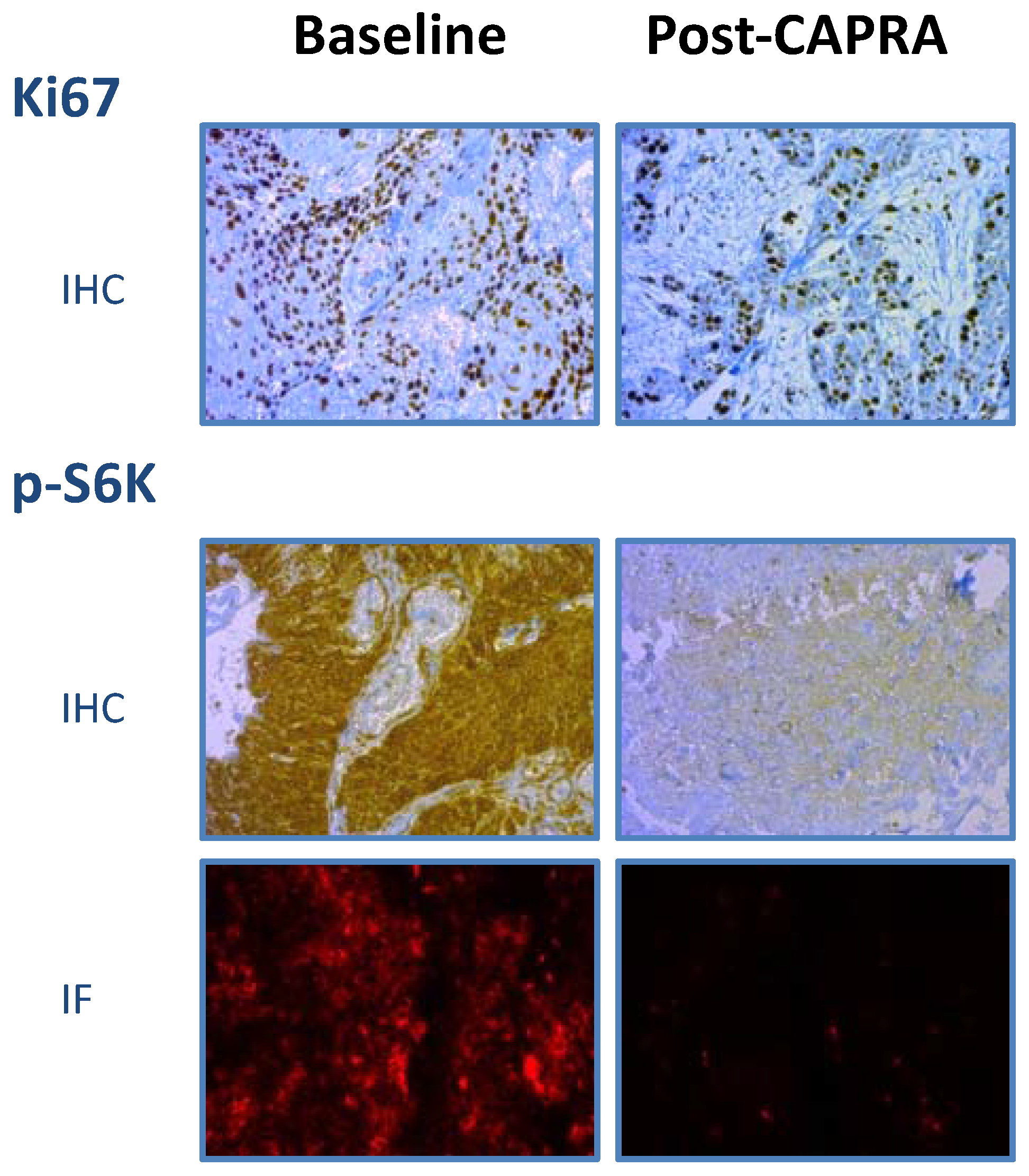
3.4.2. Pharmacodynamic Histological Biomarkers
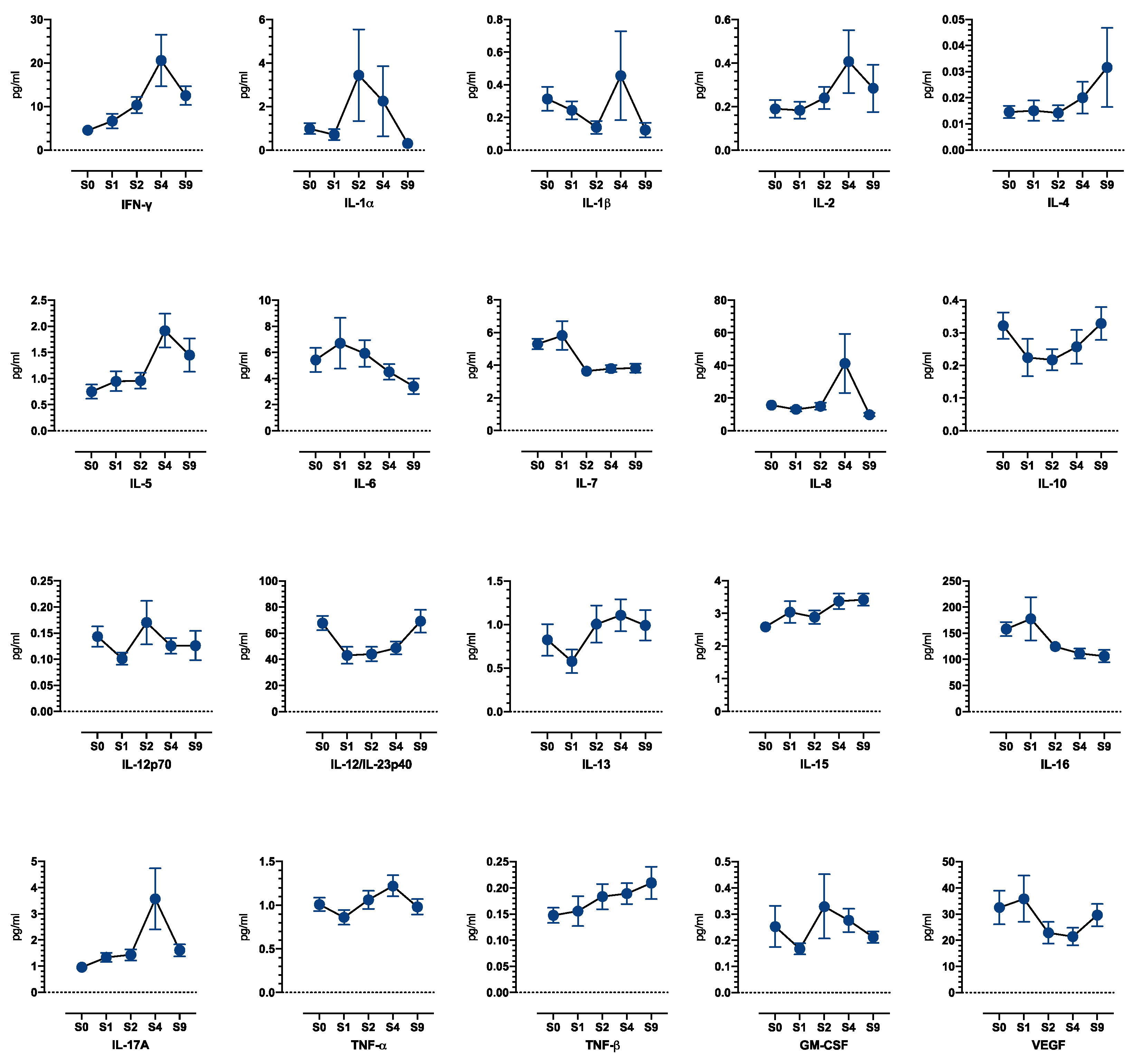
3.4.3. Blood Biomarkers
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Haddad, R.I.; Posner, M.; Hitt, R.; Cohen, E.E.W.; Schulten, J.; Lefebvre, J.-L.; Vermorken, J.B. Induction chemotherapy in locally advanced squamous cell carcinoma of the head and neck: Role, controversy, and future directions. Ann. Oncol. 2018, 29, 1130–1140. [Google Scholar] [CrossRef] [PubMed]
- Vermorken, J.B.; Remenar, E.; van Herpen, C.; Gorlia, T.; Mesia, R.; Degardin, M.; Stewart, J.S.; Jelic, S.; Betka, J.; Preiss, J.H.; et al. Cisplatin, Fluorouracil, and Docetaxel in Unresectable Head and Neck Cancer. Available online: https://www-nejm-org.proxy.insermbiblio.inist.fr/doi/10.1056/NEJMoa071028 (accessed on 20 July 2022).
- Posner, M.R.; Hershock, D.M.; Blajman, C.R.; Mickiewicz, E.; Winquist, E.; Gorbounova, V.; Tjulandin, S.; Shin, D.M.; Cullen, K.; Ervin, T.J.; et al. Cisplatin and Fluorouracil Alone or with Docetaxel in Head and Neck Cancer. Available online: https://www-nejm-org.proxy.insermbiblio.inist.fr/doi/10.1056/NEJMoa070956 (accessed on 28 July 2022).
- Vokes, E.E.; Stenson, K.; Rosen, F.R.; Kies, M.S.; Rademaker, A.W.; Witt, M.E.; Brockstein, B.E.; List, M.A.; Fung, B.B.; Portugal, L.; et al. Weekly Carboplatin and Paclitaxel Followed by Concomitant Paclitaxel, Fluorouracil, and Hydroxyurea Chemoradiotherapy: Curative and Organ-Preserving Therapy for Advanced Head and Neck Cancer. J. Clin. Oncol. 2016, 21, 320–326. [Google Scholar] [CrossRef] [PubMed]
- Ready, N.E.; Rathore, R.; Johnson, T.T.; Nadeem, A.; Chougule, P.; Ruhl, C.; Radie-Keane, K.; Theall, K.; Wanebo, H.J.; Marcello, J.; et al. Weekly Paclitaxel and Carboplatin Induction Chemotherapy Followed by Concurrent Chemoradiotherapy in Locally Advanced Squamous Cell Carcinoma of the Head and Neck. Am. J. Clin. Oncol. 2012, 35, 6–12. [Google Scholar] [CrossRef]
- Hay, N. The Akt-mTOR tango and its relevance to cancer. Cancer Cell 2005, 8, 179–183. [Google Scholar] [CrossRef]
- Faivre, S.; Kroemer, G.; Raymond, E. Current development of mTOR inhibitors as anticancer agents. Nat. Rev. Drug Discov. 2006, 5, 671–688. [Google Scholar] [CrossRef]
- Dong, J.; Peng, J.; Zhang, H.; Mondesire, W.H.; Jian, W.; Mills, G.B.; Hung, M.-C.; Meric-Bernstam, F. Role of Glycogen Synthase Kinase 3β in Rapamycin-Mediated Cell Cycle Regulation and Chemosensitivity. Cancer Res. 2005, 65, 1961–1972. [Google Scholar] [CrossRef]
- Oki, E.; Baba, H.; Tokunaga, E.; Nakamura, T.; Ueda, N.; Futatsugi, M.; Mashino, K.; Yamamoto, M.; Ikebe, M.; Kakeji, Y.; et al. Akt phosphorylation associates with LOH of PTEN and leads to chemoresistance for gastric cancer. Int. J. Cancer 2005, 117, 376–380. [Google Scholar] [CrossRef]
- Aissat, N.; Le Tourneau, C.; Ghoul, A.; Serova, M.; Bieche, I.; Lokiec, F.; Raymond, E.; Faivre, S. Antiproliferative effects of rapamycin as a single agent and in combination with carboplatin and paclitaxel in head and neck cancer cell lines. Cancer Chemother. Pharmacol. 2008, 62, 305–313. [Google Scholar] [CrossRef]
- O’Donnell, J.S.; Massi, D.; Teng, M.W.L.; Mandala, M. PI3K-AKT-mTOR inhibition in cancer immunotherapy, redux. Semin. Cancer Biol. 2018, 48, 91–103. [Google Scholar] [CrossRef] [Green Version]
- Okkenhaug, K.; Turner, M.; Gold, M.R. PI3K Signaling in B Cell and T Cell Biology. Front. Immunol. 2014, 5, 557. [Google Scholar] [CrossRef] [PubMed]
- Dormond, O.; Madsen, J.C.; Briscoe, D.M. The Effects of mTOR-Akt Interactions on Anti-apoptotic Signaling in Vascular Endothelial Cells. J. Biol. Chem. 2007, 282, 23679–23686. [Google Scholar] [CrossRef] [PubMed]
- Lyford-Pike, S.; Peng, S.; Young, G.D.; Taube, J.M.; Westra, W.H.; Akpeng, B.; Bruno, T.C.; Richmon, J.D.; Wang, H.; Bishop, J.A.; et al. Evidence for a role of the PD-1:PD-L1 pathway in immune resistance of HPV-associated head and neck squamous cell carcinoma. Cancer Res. 2013, 73, 1733–1741. [Google Scholar] [CrossRef] [PubMed]
- Vanneman, M.; Dranoff, G. Combining Immunotherapy and Targeted Therapies in Cancer Treatment. Nat. Rev. Cancer 2012, 12, 237–251. [Google Scholar] [CrossRef]
- Chi, H. Regulation and function of mTOR signalling in T cell fate decision. Nat. Rev. Immunol. 2012, 12, 325–338. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, D.; Ghi, M.G.; Franzese, C.; Codecà, C.; Gau, M.; Fayette, J. The Slippery Role of Induction Chemotherapy in Head and Neck Cancer: Myth and Reality. Front. Oncol. 2020, 10, 7. [Google Scholar] [CrossRef]
- Aisner, J.; Sinibaldi, V.; Eisenberger, M. Carboplatin in the treatment of squamous cell head and neck cancers. Semin. Oncol. 1992, 19, 60–65. [Google Scholar]
- Volling, P.; Schröder, M.; Rauschning, W.; Achterrath, W.; Stennert, E. Carboplatin: The Better Platinum in Head and Neck Cancer? Arch. Otolaryngol. Neck Surg. 1989, 115, 695–698. [Google Scholar] [CrossRef]
- Blanchard, P.; Bourhis, J.; Lacas, B.; Posner, M.R.; Vermorken, J.B.; Hernandez, J.J.C.; Bourredjem, A.; Calais, G.; Paccagnella, A.; Hitt, R.; et al. Taxane-Cisplatin-Fluorouracil As Induction Chemotherapy in Locally Advanced Head and Neck Cancers: An Individual Patient Data Meta-Analysis of the Meta-Analysis of Chemotherapy in Head and Neck Cancer Group. J. Clin. Oncol. 2013, 31, 2854–2860. [Google Scholar] [CrossRef]
- Simpson, D.R.; Mell, L.K.; Cohen, E.E. Targeting the PI3K/AKT/mTOR pathway in squamous cell carcinoma of the head and neck. Oral Oncol. 2015, 51, 291–298. [Google Scholar] [CrossRef]
- Iglesias-Bartolome, R.; Martin, D.; Gutkind, J.S. Exploiting the head and neck cancer oncogenome: Widespread PI3K-mTOR pathway alterations and novel molecular targets. Cancer Discov. 2013, 3, 722–725. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lui, V.W.Y.; Hedberg, M.L.; Li, H.; Vangara, B.S.; Pendleton, K.; Zeng, Y.; Lu, Y.; Zhang, Q.; Du, Y.; Gilbert, B.; et al. Frequent mutation of the PI3K pathway in head and neck cancer defines predictive biomarkers. Cancer Discov. 2013, 3, 761–769. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Valera, J.C.; Zhao, X.; Chen, Q.; Silvio Gutkind, J. mTOR co-targeting strategies for head and neck cancer therapy. Cancer Metastasis Rev. 2017, 36, 491–502. [Google Scholar] [CrossRef]
- Costa, L.F.; Balcells, M.; Edelman, E.R.; Nadler, L.M.; Cardoso, A.A. Proangiogenic stimulation of bone marrow endothelium engages mTOR and is inhibited by simultaneous blockade of mTOR and NF-κB. Blood 2006, 107, 285–292. [Google Scholar] [CrossRef] [PubMed]
- Balcarcel, R.R.; Stephanopoulos, G. Rapamycin reduces hybridoma cell death and enhances monoclonal antibody production. Biotechnol. Bioeng. 2001, 76, 1–10. [Google Scholar] [CrossRef]
- Ferris, R.L. Immunology and Immunotherapy of Head and Neck Cancer. J. Clin. Oncol. 2015, 33, 3293–3304. [Google Scholar] [CrossRef] [PubMed]
- Weichhart, T.; Hengstschläger, M.; Linke, M. Regulation of innate immune cell function by mTOR. Nat. Rev. Immunol. 2015, 15, 599–614. [Google Scholar] [CrossRef]
- Beziaud, L.; Mansi, L.; Ravel, P.; Marie-Joseph, E.L.; Laheurte, C.; Rangan, L.; Bonnefoy, F.; Pallandre, J.-R.; Boullerot, L.; Gamonet, C.; et al. Rapalogs Efficacy Relies on the Modulation of Antitumor T-cell Immunity. Cancer Res. 2016, 76, 4100–4112. [Google Scholar] [CrossRef]
- Kondoh, N.; Mizuno-Kamiya, M. The Role of Immune Modulatory Cytokines in the Tumor Microenvironments of Head and Neck Squamous Cell Carcinomas. Cancers 2022, 14, 2884. [Google Scholar] [CrossRef]
- Kuo, C.-S.; Yang, C.-Y.; Lin, C.-K.; Lin, G.-J.; Sytwu, H.-K.; Chen, Y.-W. Triptolide suppresses oral cancer cell PD-L1 expression in the interferon-γ-modulated microenvironment in vitro, in vivo, and in clinical patients. Biomed. Pharmacother. 2021, 133, 111057. [Google Scholar] [CrossRef]
- Ayers, M.; Lunceford, J.; Nebozhyn, M.; Murphy, E.; Loboda, A.; Kaufman, D.R.; Albright, A.; Cheng, J.D.; Kang, S.P.; Shankaran, V.; et al. IFN-γ-related mRNA profile predicts clinical response to PD-1 blockade. J. Clin. Investig. 2017, 127, 2930–2940. [Google Scholar] [CrossRef] [PubMed]
- Moore, E.C.; Cash, H.A.; Caruso, A.M.; Uppaluri, R.; Hodge, J.W.; Van Waes, C.; Allen, C.T. Enhanced tumor control with combination mTOR and PD-L1 inhibition in syngeneic oral cavity cancers. Cancer Immunol. Res. 2016, 4, 611–620. [Google Scholar] [CrossRef] [PubMed] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | |
|---|---|
| Number of patients enrolled | N = 46 |
| Age, median (year); (range) | 58 (39–85) |
| Gender, N (%) | |
| Male | 37 (80.4) |
| Female | 9 (19.6) |
| WHO performance status, n (%) | |
| 0 | 22 (47.8) |
| 1 | 18 (39.1) |
| 2 | 6 (13.0) |
| Disease stage, N (%) | |
| IVa | 30 (65.2) |
| IVb | 16 (34.8) |
| T stage, N (%) | |
| 1 | 2 (4.3) |
| 2 | 6 (13.0) |
| 3 | 2 (4.3) |
| 4a | 31 (67.4) |
| 4b | 4 (8.7) |
| x | 1 (2.2) |
| N stage, N (%) | |
| 1 | 6 (13.0) |
| 2a | 3 (6.5) |
| 2b | 5 (10.9) |
| 2c | 14 (30.4) |
| 3 | 13 (28.3) |
| x | 5 (6.5) |
| Primary site, N (%) | |
| Oropharynx | 24 (52.2) |
| Oral cavity | 13 (28.3) |
| Hypopharynx | 5 (6.5) |
| Larynx | 4 (8.7) |
| Adverse Event | All Grades, N (%) | Grade 1–2, N (%) | Grade 3–4, N (%) |
|---|---|---|---|
| Hematologic toxicity 1 | |||
| Leucopenia | 39 (85) | 26 (57) | 13 (28) |
| Neutropenia | 40 (87) | 16 (35) | 24 (52) |
| Anemia | 43 (93) | 35 (76) | 8 (17) |
| Thrombocytopenia | 37 (80) | 31 (67) | 6 (13) |
| Biologic toxicity 2 | |||
| Hyperglycemia | 38 (83) | 36 (78) | 2 (4) |
| Hypercholesterolemia | 27 (59) | 27 (59) | 0 |
| Clinical toxicity | |||
| Asthenia | 31 (67) | 27 (58) | 4 (9) |
| Nausea | 16 (35) | 16 (35) | 0 |
| Alopecia | 14 (30) | 14 (30) | 0 |
| Mucositis | 13 (28) | 13 (28) | 0 |
| Rash | 12 (26) | 11 (24) | 1 (2) |
| Pruritis | 3 (7) | 2 (4) | 1 (2) |
| Constipation | 11 (24) | 11 (24) | 0 |
| Vomiting | 9 (20) | 9 (20) | 0 |
| Dyspnea | 9 (20) | 8 (17) | 1 (2) |
| Cough | 6 (13) | 6 (13) | 0 |
| Acne | 5 (11) | 5 (11) | 0 |
| Neuropathy | 3 (7) | 3 (7) | 0 |
| Edema | 2 (4) | 2 (4) | 0 |
| Hand–foot syndrome | 2 (4) | 2 (4) | 0 |
| Response | N (%) |
|---|---|
| Objective response | 31 (75.6) |
| Complete response | 1 (2.4) |
| Partial response | 30 (73.2) |
| Stable disease | 9 (22.0) |
| Disease progression | 1 (2.4) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Evrard, D.; Dumont, C.; Gatineau, M.; Delord, J.-P.; Fayette, J.; Dreyer, C.; Tijeras-Raballand, A.; de Gramont, A.; Delattre, J.-F.; Granier, M.; et al. Targeting the Tumor Microenvironment through mTOR Inhibition and Chemotherapy as Induction Therapy for Locally Advanced Head and Neck Squamous Cell Carcinoma: The CAPRA Study. Cancers 2022, 14, 4509. https://doi.org/10.3390/cancers14184509
Evrard D, Dumont C, Gatineau M, Delord J-P, Fayette J, Dreyer C, Tijeras-Raballand A, de Gramont A, Delattre J-F, Granier M, et al. Targeting the Tumor Microenvironment through mTOR Inhibition and Chemotherapy as Induction Therapy for Locally Advanced Head and Neck Squamous Cell Carcinoma: The CAPRA Study. Cancers. 2022; 14(18):4509. https://doi.org/10.3390/cancers14184509
Chicago/Turabian StyleEvrard, Diane, Clément Dumont, Michel Gatineau, Jean-Pierre Delord, Jérôme Fayette, Chantal Dreyer, Annemilaï Tijeras-Raballand, Armand de Gramont, Jean-François Delattre, Muriel Granier, and et al. 2022. "Targeting the Tumor Microenvironment through mTOR Inhibition and Chemotherapy as Induction Therapy for Locally Advanced Head and Neck Squamous Cell Carcinoma: The CAPRA Study" Cancers 14, no. 18: 4509. https://doi.org/10.3390/cancers14184509