

Hemopatch to Prevent Lymphatic Leak after Robotic Prostatectomy and Pelvic Lymph Node Dissection: A Randomized Controlled Trial
 , , , ,
, , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Trial Design
2.2. Participants
- Inclusion criteria
- -
- Aged 18 years and above
- -
- Able to give informed consent
- -
- Suitable for minimally invasive surgery
- Exclusion criteria
- -
- Known allergy or hypersensitivity to any component of Hemopatch
- -
- Known hypersensitivity to bovine proteins or brilliant blue
- -
- Patients with prior pelvic radiotherapy
- -
- Patients with non-correctable coagulopathy
- -
- Patients who are on anticoagulants
- -
- Contraindication to general anaesthesia
- -
- Previous transurethral resection of prostate (TURP) or prostatic surgery
- -
- Untreated active infection
2.3. Randomization and Blinding
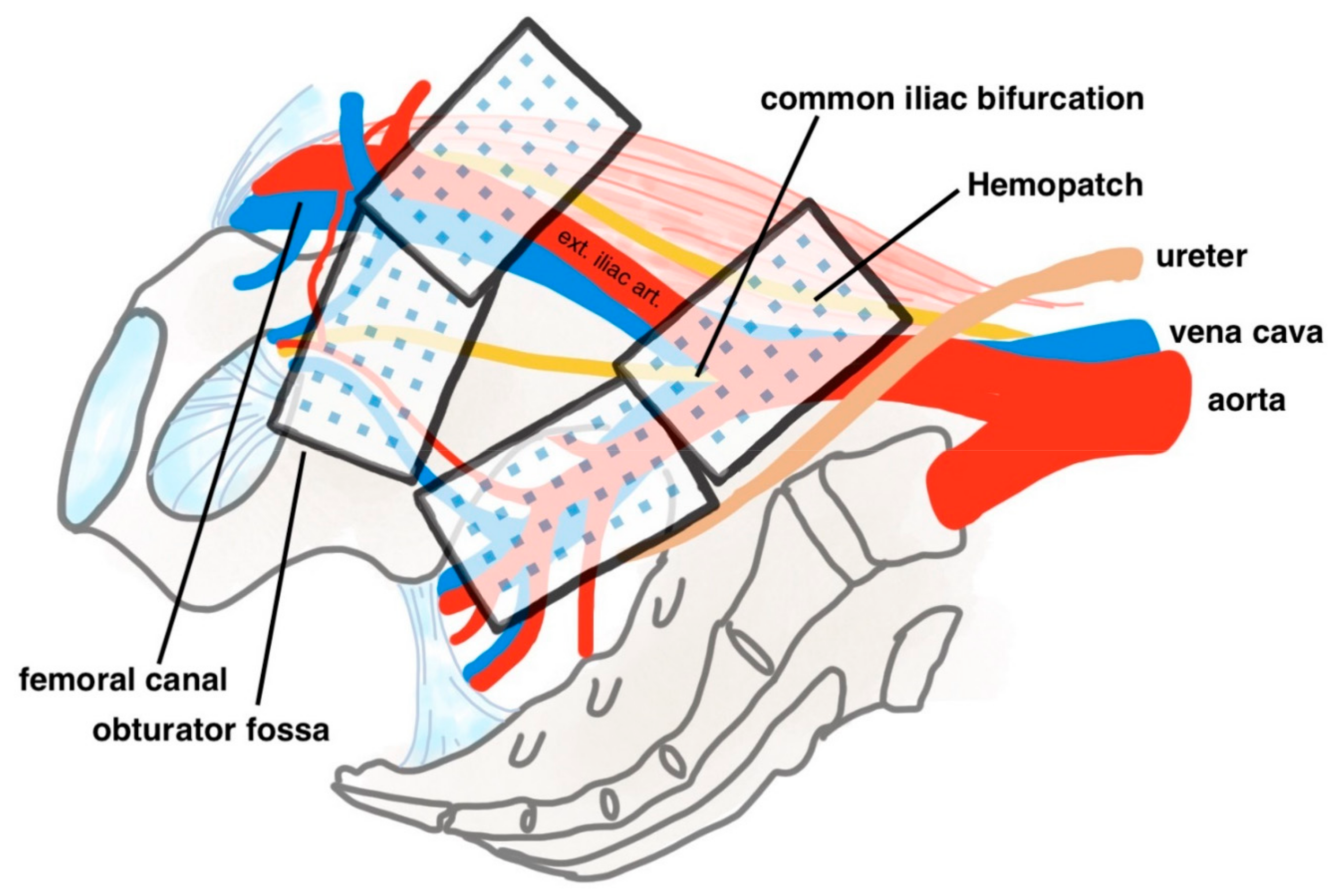
2.4. Interventions
2.5. Post-Operative Management
2.6. Outcome Measures and Data Collection
2.7. Sample Size
2.8. Statistical Methods
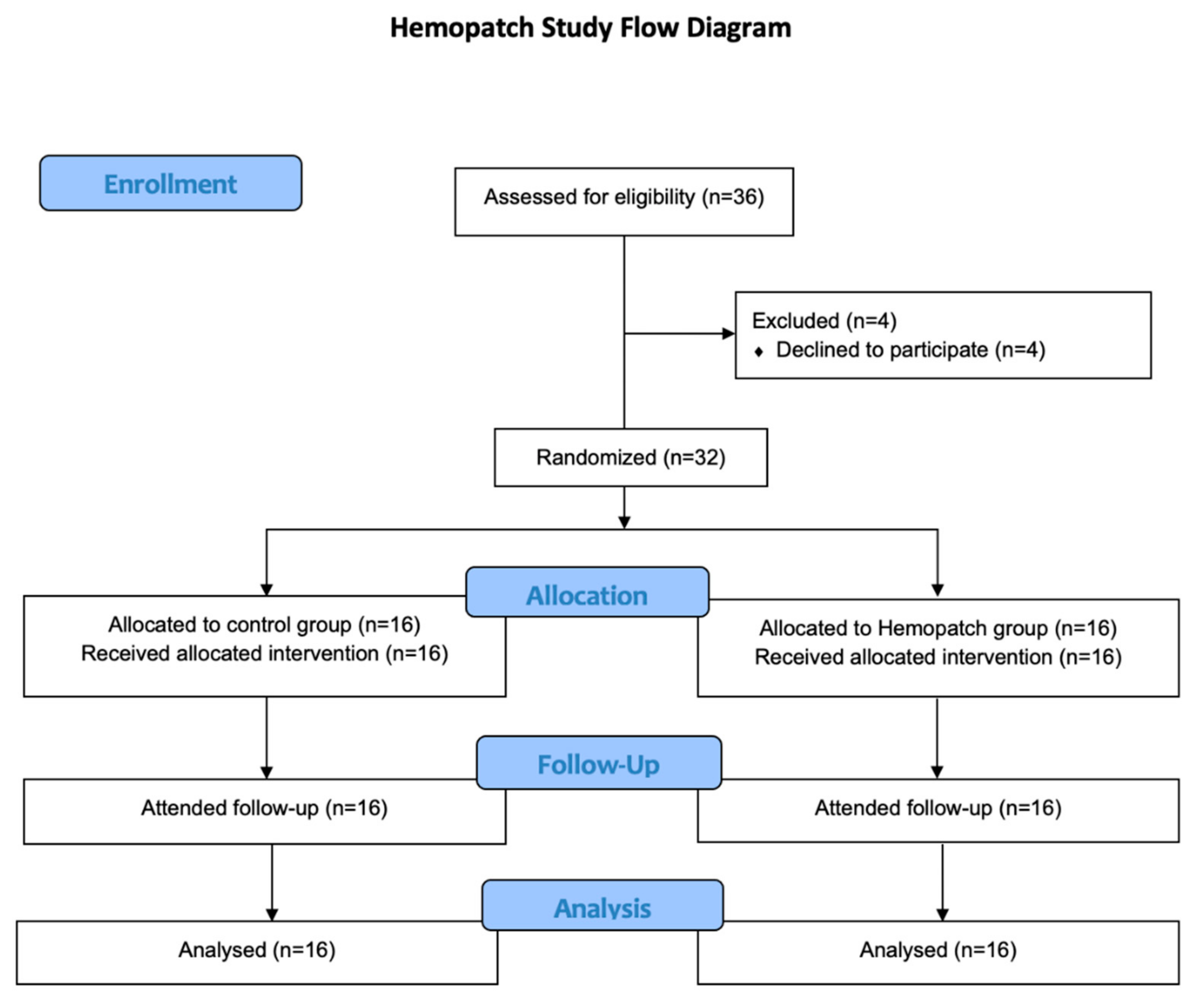
3. Results
3.1. Overview
3.2. Patient and Disease Characteristics
3.3. Study Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mottet, N.; Bellmunt, J.; Bolla, M.; Briers, E.; Cumberbatch, M.G.; De Santis, M.; Fossati, N.; Gross, T.; Henry, A.M.; Joniau, S.; et al. EAU-ESTRO-SIOG Guidelines on Prostate Cancer. Part 1: Screening, Diagnosis, and Local Treatment with Curative Intent. Eur. Urol. 2017, 71, 618–629. [Google Scholar] [CrossRef] [PubMed]
- Fossati, N.; Willemse, P.-P.M.; Van den Broeck, T.; van den Bergh, R.C.; Yuan, C.Y.; Briers, E.; Bellmunt, J.; Bolla, M.; Cornford, P.; De Santis, M.; et al. The Benefits and Harms of Different Extents of Lymph Node Dissection During Radical Prostatectomy for Prostate Cancer: A Systematic Review. Eur. Urol. 2017, 72, 84–109. [Google Scholar] [CrossRef]
- Breslin, J.W.; Yang, Y.; Scallan, J.P.; Sweat, R.S.; Adderley, S.P.; Murfee, W.L. Lymphatic vessel network structure and physiology. Compr. Physiol. 2018, 9, 207–299. [Google Scholar] [PubMed]
- Gilbert, D.R.; Angell, J.; Abaza, R. Evaluation of Absorbable Hemostatic Powder for Prevention of Lymphoceles Following Robotic Prostatectomy with Lymphadenectomy. Urology 2016, 98, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Simonato, A.; Varca, V.; Esposito, M.; Venzano, F.; Carmignani, G. The Use of a Surgical Patch in the Prevention of Lymphoceles after Extraperitoneal Pelvic Lymphadenectomy for Prostate Cancer: A Randomized Prospective Pilot Study. J. Urol. 2009, 182, 2285–2290. [Google Scholar] [CrossRef]
- Keegan, K.A.; Cookson, M.S. Complications of pelvic lymph node dissection for prostate cancer. Curr. Urol. Rep. 2011, 12, 203–208. [Google Scholar] [CrossRef]
- Sihra, N.; Kujawa, M.; Counsell, A.; Brough, R. Post-prostatectomy lymphocoele presenting with renal failure. Urology 2019, 123, e9–e10. [Google Scholar] [CrossRef]
- Gotto, G.T.; Yunis, L.H.; Guillonneau, B.; Touijer, K.; Eastham, J.A.; Scardino, P.T.; Rabbani, F. Predictors of symptomatic lymphocele after radical prostatectomy and bilateral pelvic lymph node dissection. Int. J. Urol. 2011, 18, 291–296. [Google Scholar] [CrossRef]
- Mikami, H.; Ito, K.; Yoshii, H.; Kosaka, T.; Miyajima, A.; Kaji, T.; Asano, T.; Hayakawa, M. Giant lymphocele arising after extraperitoneal laparoscopic radical prostatectomy. Hinyokika Kiyo 2008, 54, 23–27. [Google Scholar]
- Jereczek-Fossa, B.A.; Colangione, S.P.; Fodor, C.I.; Russo, S.; Cambria, R.; Zerini, D.; Bonora, M.; Cecconi, A.; Vischioni, B.; Vavassori, A.; et al. Radiotherapy in prostate cancer patients with pelvic lymphocele after surgery: Clinical and dosimetric data of 30 patients. Clin. Genitourin. Cancer 2015, 13, e223–e228. [Google Scholar] [CrossRef]
- Waldert, M.; Remzi, M.; Klatte, T.; Klingler, H.C. FloSeal reduces the incidence of lymphoceles after lymphadenectomies in laparoscopic and robot-assisted extraperitoneal radical prostatectomy. J. Endourol. 2011, 25, 969–973. [Google Scholar] [CrossRef] [PubMed]
- Lewis, K.M. Control of bleeding in surgical procedures: Critical appraisal of HEMOPATCH. Med. Devices Evid. Res. 2009, 3, 1–10. [Google Scholar] [CrossRef]
- Hueting, T.A.; Cornel, E.B.; Somford, D.M.; Jansen, H.; van Basten, J.-P.A.; Pleijhuis, R.G.; Korthorst, R.A.; van der Palen, J.; Koffijberg, H. External validation of models predicting the probability of lymph node involvement in prostate cancer patients. Eur. Urol. Oncol. 2018, 1, 411–417. [Google Scholar] [CrossRef]
- Briganti, A.; Larcher, A.; Abdollah, F.; Capitanio, U.; Gallina, A.; Suardi, N.; Bianchi, M.; Sun, M.; Freschi, M.; Salonia, A.; et al. Updated nomogram predicting lymph node invasion in patients with prostate cancer undergoing extended pelvic lymph node dissection: The essential importance of percentage of positive cores. Eur. Urol. 2012, 61, 480–487. [Google Scholar] [CrossRef] [PubMed]
- Yip, K.H.S.; Yee, C.-H.; Ng, C.-F.; Lam, N.-Y.; Ho, K.-L.; Ma, W.-K.; Li, C.-M.; Hou, S.-M.; Tam, P.-C.; Yiu, M.-K.; et al. Robot-assisted radical prostatectomy in Hong Kong: A review of 235 cases. J. Endourol. 2012, 26, 258–263. [Google Scholar] [CrossRef]
- Culp, M.B.; Soerjomataram, I.; Efstathiou, J.A.; Bray, F.; Jemal, A. Recent Global Patterns in Prostate Cancer Incidence and Mortality Rates. Eur. Urol. 2020, 77, 38–52. [Google Scholar] [CrossRef] [PubMed]
- Rawla, P. Epidemiology of Prostate Cancer. World J. Oncol. 2019, 10, 63–89. [Google Scholar] [CrossRef]
- Wilt, T.J.; Jones, K.M.; Barry, M.J.; Andriole, G.L.; Culkin, D.; Wheeler, T.; Aronson, W.J.; Brawer, M.K. Follow-up of Prostatectomy versus Observation for Early Prostate Cancer. N. Engl. J. Med. 2017, 377, 132–142. [Google Scholar] [CrossRef]
- Stolzenburg, J.U.; Kyriazis, I.; Liatsikos, E. Postoperative Lymphocele Formation after Pelvic Lymph Node Dissection at the Time of Radical Prostatectomy Should Not Be Considered an Inevitable Consequence of the Approach. Eur. Urol. 2017, 71, 159–160. [Google Scholar] [CrossRef]
- Lebeis, C.; Canes, D.; Sorcini, A.; Moinzadeh, A. Novel Technique Prevents Lymphoceles After Transperitoneal Robotic-assisted Pelvic Lymph Node Dissection: Peritoneal Flap Interposition. Urology 2015, 85, 1505–1509. [Google Scholar] [CrossRef]
- Buelens, S.; Van Praet, C.; Poelaert, F.; Van Huele, A.; Decaestecker, K.; Lumen, N. Prospective Randomized Controlled Trial Exploring the Effect of TachoSil on Lymphocele Formation after Extended Pelvic Lymph Node Dissection in Prostate Cancer. Urology 2018, 118, 134–140. [Google Scholar] [CrossRef] [PubMed]
- Lewis, K.M.; Ikeme, S.; Olubunmi, T.; Kuntze, C.E. Clinical effectiveness and versatility of a sealing hemostatic patch (Hemopatch) in multiple surgical specialties. Expert Rev. Med. Devices 2018, 15, 367–376. [Google Scholar] [CrossRef] [PubMed]
- Imkamp, F.; Von Klot, C.; Wolters, M.; Husmann, S.; Herrmann, T.; Tolkach, Y. The role of Hemopatch in zero ischemia laparoscopic partial nephrectomy. Eur. Urol. Suppl. 2016, 15, e858. [Google Scholar] [CrossRef]
- Imkamp, F.; Tolkach, Y.; Wolters, M.; Jutzi, S.; Kramer, M.; Herrmann, T. Initial experiences with the Hemopatch® as a hemostatic agent in zero-ischemia partial nephrectomy. World J. Urol. 2015, 33, 1527–1534. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Control Group (n = 16) | Hemopatch Group (n = 16) | |
|---|---|---|
| Age (year) | 69 (5) | 65 (6) |
| Weight (kg) | 68.2 (10.0) | 68.4 (10.2) |
| Height (cm) | 170 (7) | 170 (4) |
| ASA group | ||
| ASA 1 | 2 (12.5%) | 1 (6.3%) |
| ASA 2 | 9 (56.3%) | 14 (87.5%) |
| ASA 3 | 5 (31.3%) | 1 (6.3%) |
| ASA 4 | 0 (0%) | 0 (0%) |
| Prostate volume (cm3) | 53.1 (25.8) | 41.0 (22.4) |
| PSA (ng/mL) | 9.0 (6.5) | 10.5 (6.4) |
| ISUP ≥ 3 | 9 (56.3%) | 11 (68.8%) |
| Risk category | ||
| Low-risk disease | 0 (0%) | 0 (0%) |
| Intermediate-risk disease | 6 (37.5%) | 7 (43.8%) |
| High-risk disease | 10 (62.5%) | 9 (56.3%) |
| cT stage | ||
| cT1 | 9 (56.3%) | 12 (75.0%) |
| cT2 | 7 (43.8%) | 4 (25.0%) |
| pT stage | ||
| pT2 | 7 (43.8%) | 7 (43.8%) |
| pT3a | 3 (18.8%) | 6 (37.5%) |
| pT3b | 6 (37.5%) | 3 (18.8%) |
| pN1 | 1 (6.3%) | 0 (0%) |
| Control Group (n = 16) | Hemopatch Group (n = 16) | p-Value | |
|---|---|---|---|
| Primary outcome | |||
| Total drain output (mL) * | 180 (73–558) | 35 (1–190) | 0.022 |
| Secondary outcomes | |||
| Operative time (minute) | 189 (45) | 175 (52) | 0.449 |
| Intra-operative blood loss (mL) | 272 (244) | 209 (156) | 0.395 |
| Number of lymph nodes excised | 13.6 (6.6) | 12.69 (4.4) | 0.663 |
| Duration of drainage (day) * | 2 (1–5) | 1 (1–2) | 0.139 |
| Drain output per post-op day (mL/day) * | 89 (68–139) | 35 (1–117) | 0.038 |
| Hospital stay (day) | 5 (3) | 3 (1) | 0.105 |
| Transfusion | 0 (0%) | 0 (0%) | - |
| 30-day complications | 5 (31.3%) | 3 (18.8%) | 0.685 |
| Control Group (n = 16) | Hemopatch Group (n = 16) * | |
|---|---|---|
| Clavien–Dindo grade 1 | 5 (31.3%)
| 1 (18.8%)
|
| Calvien–Dindo grade 2 | 0 (0%) | 2 (12.5%)
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Teoh, J.Y.-C.; Liu, A.Q.; Yuen, V.W.-F.; Lai, F.P.-T.; Yuen, S.K.-K.; Chan, S.Y.-S.; Wong, J.H.-F.; Li, J.K.-M.; Tam, M.H.-M.; Chiu, P.K.-F.; et al. Hemopatch to Prevent Lymphatic Leak after Robotic Prostatectomy and Pelvic Lymph Node Dissection: A Randomized Controlled Trial. Cancers 2022, 14, 4476. https://doi.org/10.3390/cancers14184476
Teoh JY-C, Liu AQ, Yuen VW-F, Lai FP-T, Yuen SK-K, Chan SY-S, Wong JH-F, Li JK-M, Tam MH-M, Chiu PK-F, et al. Hemopatch to Prevent Lymphatic Leak after Robotic Prostatectomy and Pelvic Lymph Node Dissection: A Randomized Controlled Trial. Cancers. 2022; 14(18):4476. https://doi.org/10.3390/cancers14184476
Chicago/Turabian StyleTeoh, Jeremy Yuen-Chun, Alex Qinyang Liu, Violet Wai-Fan Yuen, Franco Pui-Tak Lai, Steffi Kar-Kei Yuen, Samson Yun-Sang Chan, Julius Ho-Fai Wong, Joseph Kai-Man Li, Mandy Ho-Man Tam, Peter Ka-Fung Chiu, and et al. 2022. "Hemopatch to Prevent Lymphatic Leak after Robotic Prostatectomy and Pelvic Lymph Node Dissection: A Randomized Controlled Trial" Cancers 14, no. 18: 4476. https://doi.org/10.3390/cancers14184476