


Music Therapy as a Form of Nonpharmacologic Pain Modulation in Patients with Cancer: A Systematic Review of the Current Literature


Abstract
:Simple Summary
Abstract
1. Introduction
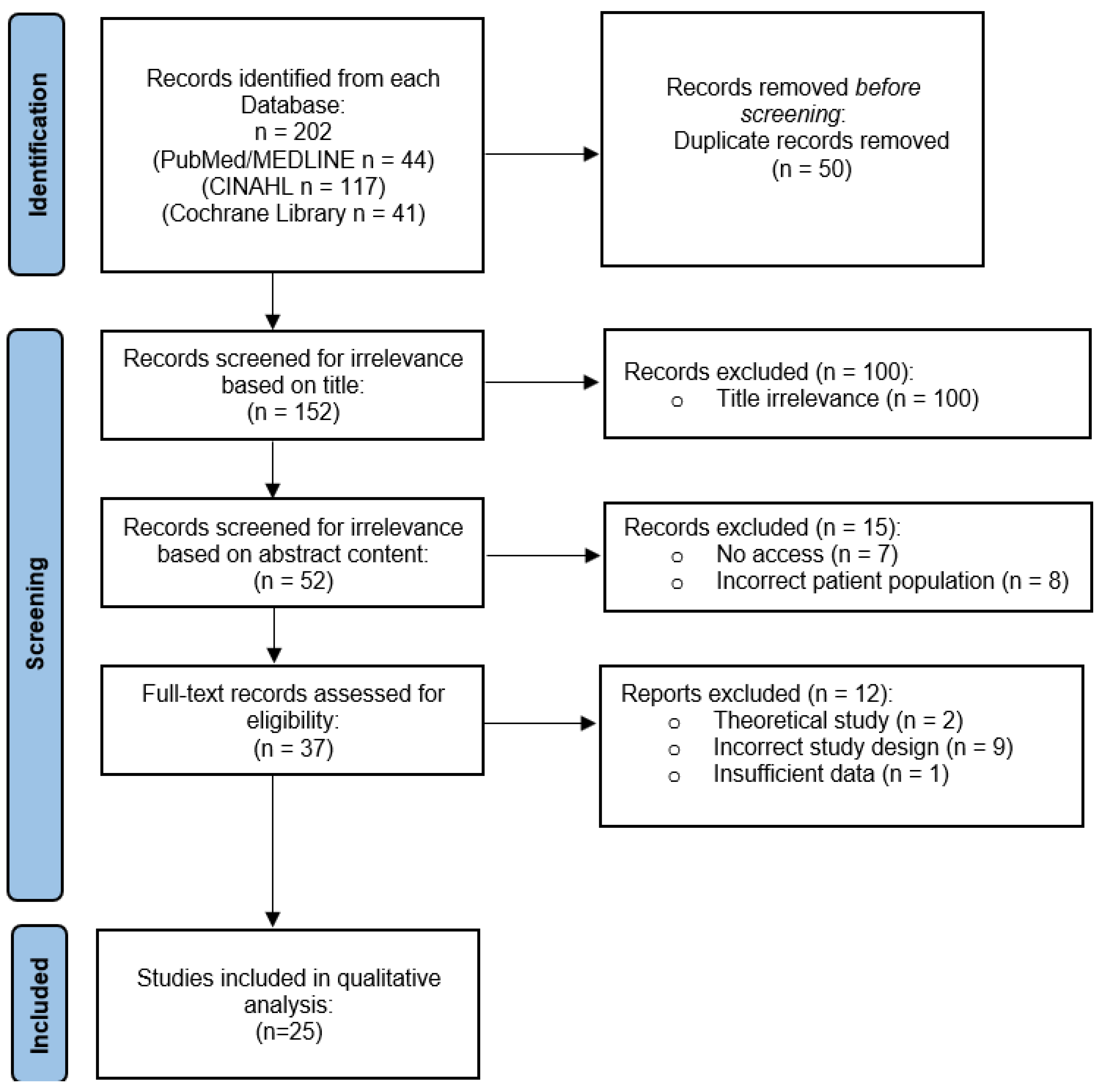
2. Materials and Methods
- P—Patients with cancer
- I—Received music therapy in addition to traditional cancer treatment
- C—Received traditional cancer treatment
- O—Pain, anxiety, quality of life, mood, sleep disorders, fatigue, heart rate (HR), blood pressure (BP), respiratory rate (RR), and oxygen saturation.
- S—Randomized controlled trials (RCTs)
3. Results


{kind=link}
| Study | Year | Country | Study Design | Patients | MT Type and Treatment Methods | Clinical Outcomes Evaluated | Main Results |
|---|---|---|---|---|---|---|---|
| Xiao et al. [24] | 2018 | China | RCT | N = 100 Tx. for breast CA, inpatient | MT and mixed therapy. Record 30 min prior to symptoms, 30 min after symptoms, 4 hours after symptoms | Stress and pain scores. | MT ↓ stress and pain in both tx. groups. |
| Liu et al. [25] | 2019 | China | RCT | N = 91 Tx. for osteo-sarcoma, in-patient | Mixed therapy. 30 min MT, followed by mindfulness-based stress reduction (MSBR), followed by 30 min of listening to any music | Pain, anxiety, and sleep dysfunction. | MT + MBSR ↓ pain, anxiety, and sleep disorders. |
| Nguyen et al. [26] | 2010 | Vietnam | RCT | N = 40 Tx. for leukemia, inpa-tient | MT. Received MT before, during, and after lumbar puncture (LP). | Anxiety, pain, RR, and HR. | MT ↓ anxiety and pain, RR, and HR. |
| Tang et al. [27] | 2021 | China | RCT | N = 100 Tx. for SCLC, inpatient | MT. 6 steps of MT before, during, and after chemotherapy. | Pain, anxiety, and sleep quality. | MT ↓ pain and anxiety, and ↑ sleep quality. |
| Reimnitz et al. [28] | 2020 | USA | RCT | N = 35 Tx. for blood and bone marrow CA, inpatient. | MT. Patient Preferred Live Music (PPLM). | Pain and fatigue. | PPLM MT ↓ pain and fa-tigue. |
| Warth et al. [29] | 2016 | Germany | RCT | N = 84 Tx. for un-known CA, inpatient. | MT. Live MT with pre and post therapy discussion, 30 min total. | Vascular sympathetic tone via stress and pain. | MT ↓ vascular sympathetic tone, stress, and pain |
| Tuinmann et al. [30] | 2016 | Germany | RCT | N = 66 Tx. for un-known CA, inpatient. | MT. Standard adjunct MT. | Pain, toxicity levels, and amount of antiemetics prescribed. | MT ↓ pain, tox-icities, and antiemetic use. |
| Kwekkeboom [31] | 2007 | USA | RCT | N = 60 Tx. for un-known CA, inpatient | MT. MT before and during procedure | Pain and anxiety scores. | MT showed no significant difference |
| Huang et al. [32] | 2010 | Taiwan | RCT | N = 126 Tx. for multiple CA types, inpatient | MT. Patients listened to a chosen recording out of four 60-80 bpm melodic tracks for 30 min. | Pain management compared to analgesic usage. | MT ↑ pain relief. |
| Shabanloei et al. [33] | 2010 | Iran | RCT | N = 100 Tx. for un-known CA, inpatient. | MT. MT during a bone marrow biop-sy/aspiration. | Pain and anxiety scores. | MT ↓ pain and anxiety. |
| Li et al. [34] | 2011 | China | RCT | N = 120 Tx. for breast CA, inpatient | MT. Patient preferred mu-sic via headphones 2x a day. | Short and long-term postoperative pain. | MT ↓ pain following mastec-tomy. |
| Deng et al. [35] | 2021 | China | RCT | N = 160 Tx. for breast CA, inpatient | MT and mixed therapy. MT +/- aroma therapy | Pain, anxiety scores, IL-6, and HMGB-1 levels. | MT +/– aroma therapy improved all out-comes. |
| Bieligmeyer et al. [36] | 2019 | Germany | RCT | N = 48 Tx. for multiple CA types, inpatient | MT. MT via vibroacoustic sound bed. | Emotional and physical well-being. | ↑ Subjective emo-tional experiences and well-being. |
| Bradt et al. [37] | 2015 | USA | RCT | N = 31 Tx. for un-known CA, inpatient | MT and MM. 2 sessions of live music + 2 sessions of recorded music. | Pain and anxiety. | MT and MM ↓ pain and anxiety |
| Hsieh et al. [38] | 2019 | Taiwan | RCT | N = 60 Tx. for breast CA, at home | MT. Five 30 min sessions of HBMI for 24 weeks. | Mental fatigue, and pain intensity. | HBMI ↓ mental fatigue and pain intensity |
| Alam et al. [39] | 2015 | USA | RCT | N = 155 Tx. for skin CA, inpatient | MT. MT 4 days before and during surgery. | Intraoperative pain and anxiety. | MT showed no effect on intraoperative pain or anxiety |
| Hilliard [40] | 2003 | USA | RCT | N = 80 Tx. for multiple CA types, hospice | MT. Regular MT sessions. | Quality of life measures and lifespan. | Quality of life ↑. Lifespan had no change. |
| Bates et al. [41] | 2015 | USA | RCT | N = 108 Tx. for unknown CA, inpatient | MT. Two 30 min sessions 1 day prior and within 5 days of transplant. | Pain scores and amount of morphine required | MT ↓ pain and morphine use. |
| Wang et al. [42] | 2015 | China | RCT | N = 60 Tx. for lung CA, inpatient | MT. IV analgesia +/− MT pre- and post-op | VAS, SAS, BP, HR, analgesia frequency, and analgesic dosage | MT ↓ VAS, SAS, BP, HR, analgesia frequency, and dose |
| Burrai et al. [43] | 2014 | Italy | RCT | N = 52 Tx. for un-known CA, inpatient | MT. 30 minutes of live saxophone MT prior to treatment | Oxygen saturation and patient mood | MT ↑ oxygen saturation and mood |
| Clark et al. [44] | 2006 | USA | RCT | N = 63 Tx. for un-known CA, outpatient | MT. MT with preselected or self-selected music | Stress and anxiety | MT ↓ stress and anxiety |
| Walworth et al. [45] | 2008 | USA | RCT | N = 27 Tx. for brain CA, inpatient | MT. MT preoperatively and each day until discharge | Anxiety, relaxation, stress, and pre-procedure perception | MT ↑ quality of life measures. Length of stay was not affected |
| Bufalini [46] | 2009 | Italy | RCT | N = 39 Tx. for unknown CA, inpatient | MT. MT +/− conscious sedation | Conscious sedation, anxiety, and compliance | MT ↓ anxiety and ↑ compliance |
| Wint et al. [47] | 2002 | USA | RCT | N = 30 Tx. for unknown CA, inpatient | Mixed therapy. Patients undergoing LP were provided virtual reality (VR) glasses that incorporated visuals and music in a distraction therapy | Pain levels | VR glasses (with MT) ↓ pain |
| Ramirez et al. [48] | 2018 | Spain | RCT | N = 40 Tx. for un-known CA, inpatient | MT. One session of MT or company of the music therapist with no MT. EEG was performed for both groups | Emotional state, fatigue, anxiety, perceived ability to breathe, and relaxation | MT ↑ breathing ease and emotional state and ↓ fatigue and anxiety |
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
References
- American Cancer Society. Cancer Facts & Figures 2021; American Cancer Society: Atlanta, GA, USA, 2021; Available online: https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/annual-cancer-facts-and-figures/2021/cancer-facts-and-figures-2021.pdf (accessed on 1 May 2022).
- Emanuel, E.J.; Gudbranson, E.; Van Parys, J.; Gørtz, M.; Helgeland, J.; Skinner, J. Comparing Health Outcomes of Privileged US Citizens With Those of Average Residents of Other Developed Countries. JAMA Intern. Med. 2021, 181, 339–344. [Google Scholar] [CrossRef] [PubMed]
- Rahib, L.; Wehner, M.R.; Matrisian, L.M.; Nead, K.T. Estimated Projection of US Cancer Incidence and Death to 2040. JAMA Netw. Open 2021, 4, e214708. [Google Scholar] [CrossRef] [PubMed]
- Takeshima, H.; Ushijima, T. Accumulation of genetic and epigenetic alterations in normal cells and cancer risk. NPJ Precis. Oncol. 2019, 3, 7. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.; Kruper, L.; Dieli-Conwright, C.M.; Mortimer, J.E. The Impact of Obesity on Breast Cancer Diagnosis and Treatment. Curr. Oncol. Rep. 2019, 21, 41. [Google Scholar] [CrossRef]
- Key, T.J.; Bradbury, K.E.; Perez-Cornago, A.; Sinha, R.; Tsilidis, K.K.; Tsugane, S. Diet, nutrition, and cancer risk: What do we know and what is the way forward? BMJ 2020, 368, m511, Correction in BMJ 2020, 368, m996. [Google Scholar] [CrossRef]
- Yasunaga, J.-I.; Matsuoka, M. Oncogenic spiral by infectious pathogens: Cooperation of multiple factors in cancer development. Cancer Sci. 2017, 109, 24–32. [Google Scholar] [CrossRef]
- Olsson, A.; Kromhout, H. Occupational cancer burden: The contribution of exposure to process-generated substances at the workplace. Mol. Oncol. 2021, 15, 753–763. [Google Scholar] [CrossRef]
- Smith, R.A.; Ba, K.S.A.; Brooks, D.; Fedewa, S.A.; Manassaram-Baptiste, D.; Saslow, D.; Wender, R.C. Cancer screening in the United States, 2019: A review of current American Cancer Society guidelines and current issues in cancer screening. CA A Cancer J. Clin. 2019, 69, 184–210. [Google Scholar] [CrossRef]
- Saito, Y.; Oka, S.; Kawamura, T.; Shimoda, R.; Sekiguchi, M.; Tamai, N.; Hotta, K.; Matsuda, T.; Misawa, M.; Tanaka, S.; et al. Colonoscopy screening and surveillance guidelines. Dig. Endosc. 2021, 33, 486–519. [Google Scholar] [CrossRef]
- Weber, W. Clinical PET/MR. Recent Results Cancer Res. 2020, 216, 747–764. [Google Scholar] [CrossRef]
- Anzai, Y.; Nishizawa, S.; Shinke, T.; Takesono, S.; Asai, T.; Okada, H. Prospective Employer-Initiated Whole-Body Cancer Screening—Costs and Outcomes of a Cancer Screening Program in Japan. J. Am. Coll. Radiol. 2021, 18, 140–147. [Google Scholar] [CrossRef]
- Kitajima, K.; Kaida, H.; Nakatani, K.; Ishibashi, M.; Morita, T.; Nakajo, M.; Tamaki, Y.; Minamimoto, R. Assessment of tumor response to definitive chemoradiotherapy and prognosis prediction in patients with esophageal cancer judged by PET response criteria in solid tumors: Multicenter study in Japan. Nucl. Med. Commun. 2020, 41, 443–451. [Google Scholar] [CrossRef]
- Nitya, K.; Keerthinarayan, V.; Rajprakash, B.; Shanmugam, K.T.; Dhamodhar, M.D.; Mohan, R.; Karthikeyan, M.; Solomon, N. Biopsy—As a Diagnostic Tool. Recent Dev. Med. Med. Res. 2021, 15, 154–166. [Google Scholar] [CrossRef]
- Hahlweg, P.; Kriston, L.; Scholl, I.; Brähler, E.; Faller, H.; Schulz, H.; Weis, J.; Koch, U.; Wegscheider, K.; Mehnert, A.; et al. Cancer patients’ preferred and perceived level of involvement in treatment decision-making: An epidemiological study. Acta Oncol. 2020, 59, 967–974. [Google Scholar] [CrossRef]
- Shariati, M.; Meric-Bernstam, F. Targeting AKT for cancer therapy. Expert Opin. Investig. Drugs 2019, 28, 977–988. [Google Scholar] [CrossRef]
- Cillessen, L.; Johannsen, M.; Speckens, A.E.; Zachariae, R. Mindfulness-based interventions for psychological and physical health outcomes in cancer patients and survivors: A systematic review and meta-analysis of randomized controlled trials. Psycho-Oncology 2019, 28, 2257–2269. [Google Scholar] [CrossRef]
- Dekker, J.; Graves, K.D.; Badger, T.A.; Diefenbach, M.A. Management of Distress in Patients with Cancer—Are We Doing the Right Thing? Ann. Behav. Med. 2020, 54, 978–984. [Google Scholar] [CrossRef]
- Deng, G. Integrative Medicine Therapies for Pain Management in Cancer Patients. Cancer J. 2019, 25, 343–348. [Google Scholar] [CrossRef]
- Stanczyk, M.M. Music therapy in supportive cancer care. Rep. Pr. Oncol. Radiother. 2011, 16, 170–172. [Google Scholar] [CrossRef]
- Palmer, J.B.; Lane, D.; Mayo, D.; Schluchter, M.; Leeming, R. Effects of Music Therapy on Anesthesia Requirements and Anxiety in Women Undergoing Ambulatory Breast Surgery for Cancer Diagnosis and Treatment: A Randomized Controlled Trial. J. Clin. Oncol. 2015, 33, 3162–3168. [Google Scholar] [CrossRef] [Green Version]
- Köhler, F.; Martin, Z.-S.; Hertrampf, R.-S.; Gäbel, C.; Kessler, J.; Ditzen, B.; Warth, M. Music Therapy in the Psychosocial Treatment of Adult Cancer Patients: A Systematic Review and Meta-Analysis. Front. Psychol. 2020, 11, 651. [Google Scholar] [CrossRef]
- Montinari, M.R.; Giardina, S.; Minelli, P.; Minelli, S. History of Music Therapy and Its Contemporary Applications in Cardiovascular Diseases. South. Med. J. 2018, 111, 98–102. [Google Scholar] [CrossRef]
- Xiao, Y.; Li, L.; Xie, Y.; Xu, J.; Liu, Y. Effects of aroma therapy and music intervention on pain and anxious for breast cancer patients in the perioperative period. Zhong Nan Da Xue Xue Bao Yi Xue Ban 2018, 43, 656–661. [Google Scholar] [CrossRef]
- Liu, H.; Gao, X.; Hou, Y. Effects of mindfulness-based stress reduction combined with music therapy on pain, anxiety, and sleep quality in patients with osteosarcoma. Rev. Bras. de Psiquiatr. 2019, 41, 540–545. [Google Scholar] [CrossRef]
- Nguyen, T.N.; Nilsson, S.; Hellström, A.-L.; Bengtson, A. Music Therapy to Reduce Pain and Anxiety in Children With Cancer Undergoing Lumbar Puncture: A Randomized Clinical Trial. J. Pediatr. Oncol. Nurs. 2010, 27, 146–155. [Google Scholar] [CrossRef]
- Tang, H.; Chen, L.; Wang, Y.; Zhang, Y.; Yang, N.; Yang, N. The efficacy of music therapy to relieve pain, anxiety, and promote sleep quality, in patients with small cell lung cancer receiving platinum-based chemotherapy. Support. Care Cancer 2021, 29, 7299–7306. [Google Scholar] [CrossRef]
- Reimnitz, L.; Silverman, M.J. A randomized pilot study of music therapy in the form of patient-preferred live music on fatigue, energy and pain in hospitalized adult oncology patients on a blood and marrow transplant unit. Arts Heal. 2018, 12, 154–168. [Google Scholar] [CrossRef]
- Warth, M.; Kessler, J.; Hillecke, T.K.; Bardenheuer, H.J. Trajectories of Terminally Ill Patients’ Cardiovascular Response to Receptive Music Therapy in Palliative Care. J. Pain Symptom Manag. 2016, 52, 196–204. [Google Scholar] [CrossRef]
- Tuinmann, G.; Preissler, P.; Böhmer, H.; Suling, A.; Bokemeyer, C. The effects of music therapy in patients with high-dose chemotherapy and stem cell support: A randomized pilot study. Psycho-Oncology 2016, 26, 377–384. [Google Scholar] [CrossRef]
- Kwekkeboom, K.L. Music Versus Distraction for Procedural Pain and Anxiety in Patients with Cancer. Oncol. Nurs. Forum 2003, 30, 433–440. [Google Scholar] [CrossRef]
- Huang, S.-T.; Good, M.; Zauszniewski, J.A. The effectiveness of music in relieving pain in cancer patients: A randomized controlled trial. Int. J. Nurs. Stud. 2010, 47, 1354–1362. [Google Scholar] [CrossRef] [PubMed]
- Shabanloei, R.; Golchin, M.; Esfahani, A.; Dolatkhah, R.; Rasoulian, M. Effects of Music Therapy on Pain and Anxiety in Patients Undergoing Bone Marrow Biopsy and Aspiration. AORN J. 2010, 91, 746–751. [Google Scholar] [CrossRef] [PubMed]
- Li, X.-M.; Yan, H.; Zhou, K.-N.; Dang, S.-N.; Wang, D.-L.; Zhang, Y.-P. Effects of music therapy on pain among female breast cancer patients after radical mastectomy: Results from a randomized controlled trial. Breast Cancer Res. Treat. 2011, 128, 411–419. [Google Scholar] [CrossRef] [PubMed]
- Deng, C.; Xie, Y.; Liu, Y.; Li, Y.; Xiao, Y. Aromatherapy Plus Music Therapy Improve Pain Intensity and Anxiety Scores in Patients With Breast Cancer During Perioperative Periods: A Randomized Controlled Trial. Clin. Breast Cancer 2021, 22, 115–120. [Google Scholar] [CrossRef]
- Bieligmeyer, S.; Helmert, E.; Hautzinger, M.; Vagedes, J. Feeling the sound—Short-term effect of a vibroacoustic music interven-tion on well-being and subjectively assessed warmth distribution in cancer patients-A randomized controlled trial. Complement Ther. Med. 2018, 40, 171–178. [Google Scholar] [CrossRef]
- Bradt, J.; Potvin, N.; Kesslick, A.; Shim, M.; Radl, D.; Schriver, E.; Gracely, E.J.; Komarnicky-Kocher, L.T. The impact of music therapy versus music medicine on psychological outcomes and pain in cancer patients: A mixed methods study. Support. Care Cancer 2014, 23, 1261–1271. [Google Scholar] [CrossRef]
- Hsieh, F.; Miao, N.; Tseng, I.; Chiu, H.; Kao, C.; Liu, D.; Chen, R.; Tsai, H.; Chou, K. Effect of home-based music intervention versus ambient music on breast cancer survivors in the community: A feasibility study in Taiwan. Eur. J. Cancer Care 2019, 28, e13064. [Google Scholar] [CrossRef]
- Alam, M.; Roongpisuthipong, W.; Kim, N.A.; Goyal, A.; Swary, J.H.; Brindise, R.T.; Iyengar, S.; Pace, N.; West, D.P.; Polavarapu, M.; et al. Utility of recorded guided imagery and relaxing music in reducing patient pain and anxiety, and surgeon anxiety, during cutaneous surgical procedures: A single-blinded randomized controlled trial. J. Am. Acad. Dermatol. 2016, 75, 585–589. [Google Scholar] [CrossRef]
- Hilliard, R.E. The Effects of Music Therapy on the Quality and Length of Life of People Diagnosed with Terminal Cancer. J. Music Ther. 2003, 40, 113–137. [Google Scholar] [CrossRef]
- Bates, D.; Bolwell, B.; Majhail, N.S.; Rybicki, L.; Yurch, M.; Abounader, D.; Kohuth, J.; Jarancik, S.; Koniarczyk, H.; McLellan, L.; et al. Music Therapy for Symptom Management After Autologous Stem Cell Transplantation: Results From a Randomized Study. Biol. Blood Marrow Transplant. 2017, 23, 1567–1572. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Tang, H.; Guo, Q.; Liu, J.; Liu, X.; Luo, J.; Yang, W. Effects of Intravenous Patient-Controlled Sufentanil Analgesia and Music Therapy on Pain and Hemodynamics After Surgery for Lung Cancer: A Randomized Parallel Study. J. Altern. Complement. Med. 2015, 21, 667–672. [Google Scholar] [CrossRef]
- Burrai, F.; Micheluzzi, V.; Bugani, V. Effects of live sax music on various physiological parameters, pain level, and mood level in cancer patients: A randomized controlled trial. Holist. Nurs. Pr. 2014, 28, 301–311. [Google Scholar] [CrossRef]
- Clark, M.; Isaacks-Downton, G.; Wells, N.; Redlin-Frazier, S.; Eck, C.; Hepworth, J.T.; Chakravarthy, B. Use of Preferred Music to Reduce Emotional Distress and Symptom Activity During Radiation Therapy. J. Music Ther. 2006, 43, 247–265. [Google Scholar] [CrossRef]
- Walworth, D.; Rumana, C.S.; Nguyen, J.; Jarred, J. Effects of Live Music Therapy Sessions on Quality of Life Indicators, Medications Administered and Hospital Length of Stay for Patients Undergoing Elective Surgical Procedures for Brain. J. Music Ther. 2008, 45, 349–359. [Google Scholar] [CrossRef]
- Bufalini, A. Ruolo della musica interattiva nel paziente pediatrico oncologico sottoposto a procedure dolorose [Role of interac-tive music in oncological pediatric patients undergoing painful procedures]. Minerva Pediatr. 2009, 61, 379–389. [Google Scholar]
- Wint, S.S.; Eshelman, D.; Steele, J.; Guzzetta, C.E. Effects of Distraction Using Virtual Reality Glasses During Lumbar Punctures in Adolescents With Cancer. Oncol. Nurs. Forum 2002, 29, E8–E15. [Google Scholar] [CrossRef]
- Ramirez, R.; Planas, J.; Escude, N.; Mercade, J.; Farriols, C. EEG-Based Analysis of the Emotional Effect of Music Therapy on Palliative Care Cancer Patients. Front. Psychol. 2018, 9, 254. [Google Scholar] [CrossRef]
- Donald, D.E.; Pinson, J. Music Therapy in Principle and Practice; Charles C Thomas Publisher: Springfield, IL, USA, 2012. [Google Scholar]
- Bradt, J.; Dileo, C.; Magill, L.; Teague, A. Music interventions for improving psychological and physical outcomes in cancer patients. Cochrane Database Syst. Rev. 2016, 8, CD006911. [Google Scholar] [CrossRef]
- Gramaglia, C.; Gambaro, E.; Vecchi, C.; Licandro, D.; Raina, G.; Pisani, C.; Burgio, V.; Farruggio, S.; Rolla, R.; Deantonio, L.; et al. Outcomes of music therapy interventions in cancer patients-A review of the litera-ture. Crit. Rev. Oncol. Hematol. 2019, 138, 241–254. [Google Scholar] [CrossRef]
- Yang, T.; Wang, S.; Wang, R.; Wei, Y.; Kang, Y.; Liu, Y.; Zhang, C. Effectiveness of five-element music therapy in cancer patients: A systematic review and meta-analysis. Complement. Ther. Clin. Pr. 2021, 44, 101416. [Google Scholar] [CrossRef]
- Cook, T.; Roy, A.R.K.; Welker, K.M. Music as an emotion regulation strategy: An examination of genres of music and their roles in emotion regulation. Psychol. Music 2017, 47, 144–154. [Google Scholar] [CrossRef]
- Ginsberg, J.P.; Raghunathan, K.; Bassi, G.; Ulloa, L. Review of Perioperative Music Medicine: Mechanisms of Pain and Stress Reduction Around Surgery. Front. Med. 2022, 9, 821022. [Google Scholar] [CrossRef]
- Hiller, J.G.; Cole, S.W.; Crone, E.M.; Byrne, D.J.; Shackleford, D.M.; Pang, J.-M.B.; Henderson, M.A.; Nightingale, S.S.; Ho, K.M.; Myles, P.S.; et al. Preoperative β-Blockade with Propranolol Reduces Biomarkers of Metastasis in Breast Cancer: A Phase II Randomized Trial. Clin. Cancer Res. 2020, 26, 1803–1811. [Google Scholar] [CrossRef] [PubMed]
- Ayroldi, E.; Cannarile, L.; Adorisio, S.; Delfino, D.V.; Riccardi, C. Role of Endogenous Glucocorticoids in Cancer in the Elderly. Int. J. Mol. Sci. 2018, 19, 3774. [Google Scholar] [CrossRef] [PubMed]
- Gupta, K.K.; Attri, J.P.; Singh, A.; Kaur, H.; Kaur, G. Basic concepts for sample size calculation: Critical step for any clinical trials! Saudi J. Anaesth. 2016, 10, 328–331. [Google Scholar] [CrossRef] [PubMed]
- Kalan Farmanfarma, K.H.; Mohammadian, M.; Shahabinia, Z.; Hassanipour, S.; Salehiniya, H. Brain cancer in the world: An epidemiological review. World Cancer Res. J. 2019, 6, e1356. [Google Scholar] [CrossRef]
- Hiller, J.; Gardstrom, S.C. The Selection of Music Experiences in Music Therapy. Music Ther. Perspect. 2018, 36, 79–86. [Google Scholar] [CrossRef]
- Tsoi, K.K.; Chan, J.Y.; Ng, Y.-M.; Lee, M.M.; Kwok, T.C.; Wong, S.Y.-S. Receptive Music Therapy Is More Effective than Interactive Music Therapy to Relieve Behavioral and Psychological Symptoms of Dementia: A Systematic Review and Meta-Analysis. J. Am. Med. Dir. Assoc. 2018, 19, 568–576.e3. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rennie, C.; Irvine, D.S.; Huang, E.; Huang, J. Music Therapy as a Form of Nonpharmacologic Pain Modulation in Patients with Cancer: A Systematic Review of the Current Literature. Cancers 2022, 14, 4416. https://doi.org/10.3390/cancers14184416
Rennie C, Irvine DS, Huang E, Huang J. Music Therapy as a Form of Nonpharmacologic Pain Modulation in Patients with Cancer: A Systematic Review of the Current Literature. Cancers. 2022; 14(18):4416. https://doi.org/10.3390/cancers14184416
Chicago/Turabian StyleRennie, Christopher, Dylan S. Irvine, Evan Huang, and Jeffrey Huang. 2022. "Music Therapy as a Form of Nonpharmacologic Pain Modulation in Patients with Cancer: A Systematic Review of the Current Literature" Cancers 14, no. 18: 4416. https://doi.org/10.3390/cancers14184416