
Controversial Link between Cannabis and Anticancer Treatments—Where Are We and Where Are We Going? A Systematic Review of the Literature

 , ,
, , 
Abstract
:Simple Summary
Abstract
1. Introduction
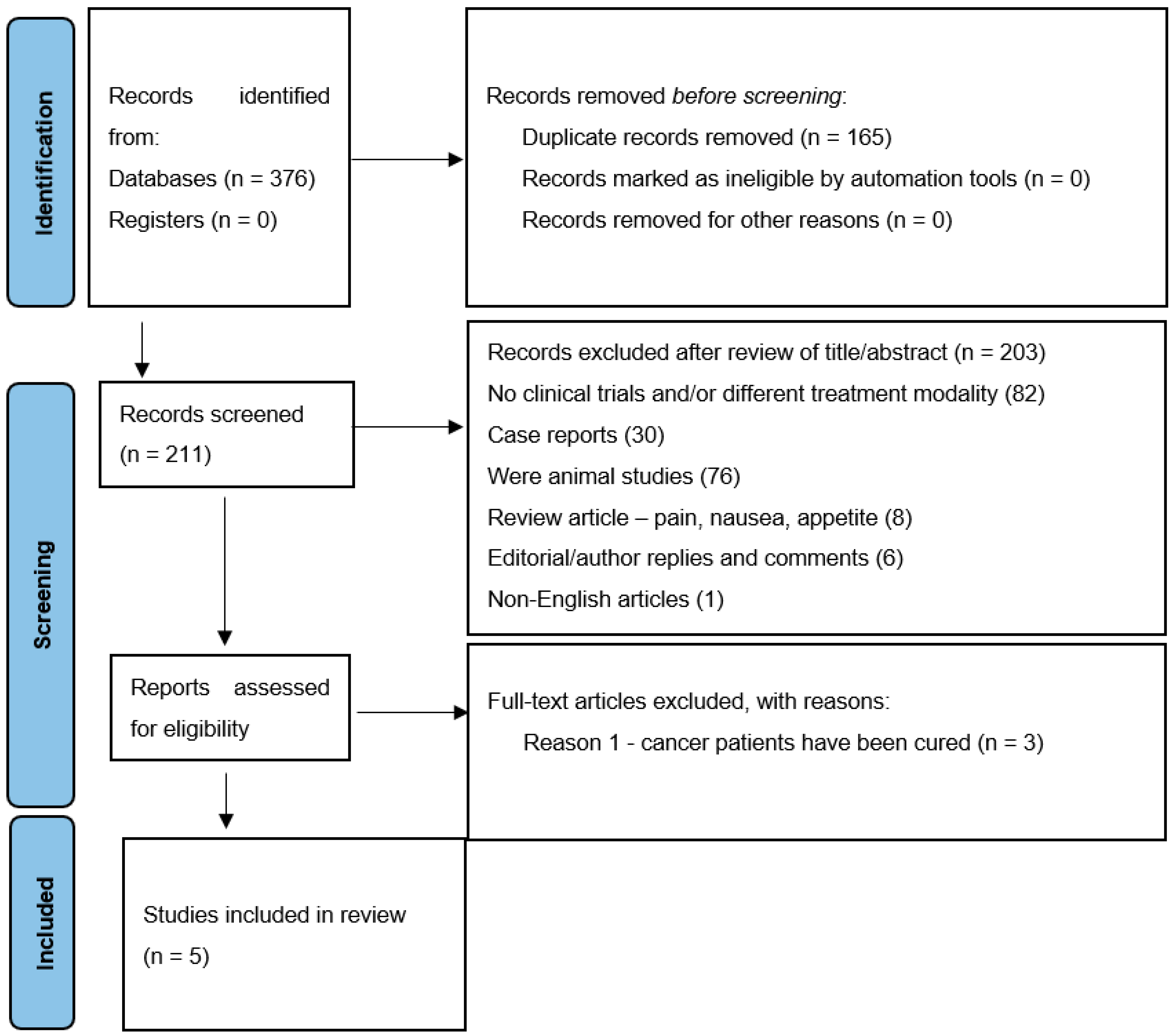
2. Materials and Methods
2.1. Data Collection Process
2.2. Eligibility Criteria
3. Results
3.1. Study Characteristics
3.2. Design of the Studies
3.3. Participants and Regrouping
4. Discussion
5. Conclusions
Limitations
Author Contributions
Funding
Conflicts of Interest
References
- Balhara, Y.P.S.; Mathur, S. Bhang—Beyond the purview of the narcotic drugs and psychotropic substances act. Lung India 2014, 31, 431–432. [Google Scholar] [CrossRef]
- Hall, W.; Solowij, N. Adverse effects of cannabis. Lancet 1998, 352, 1611–1616. [Google Scholar] [CrossRef]
- EMCDDA. European Monitoring Centre for Drugs and Drug Addiction—Annual Report 2012: The State of the Drugs Problem in Europe; Publications Office of the European Union: Luxembourg, 2012. [Google Scholar]
- World Drug Report. United Nations Publication, Sales No. E.19.XI.8. 2019. Available online: https://wdr.unodc.org/wdr2019/prelaunch/WDR19_Booklet_5_CANNABIS_HALLUCINOGENS.pdf (accessed on 5 March 2022).
- Murray, R.M.; Morrison, P.D.; Henquet, C.; Di Forti, M. Cannabis, the mind and society: The hash realities. Nat. Rev. Neurosci. 2007, 8, 885–895. [Google Scholar] [CrossRef] [PubMed]
- Grotenhermen, F.; Müller-Vahl, K. The therapeutic potential of cannabis and cannabinoids. Dtsch. Arztebl. Int. 2012, 109, 495–501. [Google Scholar] [CrossRef] [PubMed]
- UNODC. World Drug Report 2021; United Nations Office on Drugs and Crime: Vienna, Austria, 2021. [Google Scholar]
- Sharma, P.; Murthy, P.; Bharath, M. Chemistry, metabolism, and toxicology of cannabis: Clinical implications. Iran. J. Psychiatry 2012, 7, 149–156. [Google Scholar] [PubMed]
- National Cancer Institute. Cannabis and Cannabinoids (PDQ®)–Health Professional Version. Available online: https://www.cancer.gov/about-cancer/treatment/cam/hp/cannabis-pdq (accessed on 12 May 2022).
- Perez-Reyes, M.; White, W.R.; McDonald, S.A.; Hicks, R.E.; Jeffcoat, A.R.; Cook, C.E. The pharmacologic effects of daily marijuana smoking in humans. Pharmacol. Biochem. Behav. 1991, 40, 691–694. [Google Scholar] [CrossRef]
- Costa, B. On the pharmacological properties of Δ9-tetrahydrocannabinol (THC). Chem. Biodivers. 2007, 4, 1664–1677. [Google Scholar] [CrossRef]
- Zuardi, A.W.; Crippa, J.A.; Hallak, J.E.; Bhattacharyya, S.; Atakan, Z.; Martin-Santos, R.; McGuire, P.K.; Guimarães, F.S. A critical review of the antipsychotic effects of cannabidiol: 30 years of a translational investigation. Curr. Pharm. Des. 2012, 18, 5131–5140. [Google Scholar] [CrossRef] [Green Version]
- Martin-Santos, R.; Crippa, J.A.; Batalla, A.; Bhattacharyya, S.; Atakan, Z.; Borgwardt, S.; Allen, P.; Seal, M.; Langohr, K.; Farré, M.; et al. Acute effects of a single, oral dose of d9-tetrahydrocannabinol (THC) and cannabidiol (CBD) administration in healthy volunteers. Curr. Pharm. Des. 2012, 18, 4966–4979. [Google Scholar] [CrossRef]
- Guindon, J.; Hohmann, A.G. The endocannabinoid system and pain. CNS Neurol. Disord. Drug Targets 2009, 8, 403–421. [Google Scholar] [CrossRef]
- Pertwee, R.G. The diverse CB1 and CB2 receptor pharmacology of three plant cannabinoids: Δ9-tetrahydrocannabinol, cannabidiol and Δ9-tetrahydrocannabivarin. Br. J. Pharmacol. 2008, 153, 199–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lu, H.C.; Mackie, K. An Introduction to the Endogenous Cannabinoid System. Biol. Psychiatry 2016, 79, 516–525. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jain, R.; Balhara, Y.P. Neurobiology of cannabis addiction. Indian J. Physiol. Pharmacol. 2008, 52, 217–232. [Google Scholar]
- Costentin, J. Neuropsychopharmacology of Δ9-tetrahydrocannabinol. Ann. Pharm. Fr. 2008, 66, 219–231. [Google Scholar] [CrossRef] [PubMed]
- Guindon, J.; Hohmann, A.G. Cannabinoid CB2 receptors: A therapeutic target for the treatment of inflammatory and neuropathic pain. Br. J. Pharmacol. 2008, 153, 319–334. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Downer, E.J.; Fogarty, M.P.; Campbell, V.A. Tetrahydrocannabinol-induced neurotoxicity depends on CB1 receptor-mediated c-Jun N-terminal kinase activation in cultured cortical neurons. Br. J. Pharmacol. 2003, 140, 547–557. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rieder, S.A.J.; Chauhan, A.J.; Singh, U.J.; Nagarkatti, M.J.; Nagarkatti, P. Cannabinoid-induced apoptosis in immune cells as a pathway to immunosuppression. Immunobiology 2010, 215, 598–605. [Google Scholar] [CrossRef] [Green Version]
- Blázquez, C.; Salazar, M.; Carracedo, A.; Lorente, M.; Egia, A.; González-Feria, L.; Haro, A.; Velasco, G.; Guzmán, M. Cannabinoids inhibit glioma cell invasion by down-regulating matrix metalloproteinase-2 expression. Cancer Res. 2008, 68, 1945–1952. [Google Scholar] [CrossRef] [Green Version]
- Bahji, A.; Stephenson, C. International Perspectives on the Implications of Cannabis Legalization: A Systematic Review & Thematic Analysis. Int. J. Environ. Res. Public Health 2019, 16, 3095. [Google Scholar] [CrossRef] [Green Version]
- European Monitoring Centre for Drugs and Drug Addiction. Medical Use of Cannabis and Cannabinoids: Questions and Answers for Policymaking; Publications Office of the European Union: Luxembourg, 2018. Available online: https://www.emcdda.europa.eu/system/files/publications/10171/20185584_TD0618186ENN_PDF.pdf (accessed on 15 April 2022).
- Munson, A.E.; Harris, L.S.; Friedman, M.A.; Dewey, W.L.; Carchman, R.A. Antineoplastic activity of cannabinoids. J. Natl. Cancer Inst. 1975, 55, 597–602. [Google Scholar] [CrossRef]
- Zhang, Z.F.; Morgenstern, H.; Spitz, M.R.; Tashkin, D.P.; Yu, G.P.; Marshall, J.R.; Hsu, T.C.; Schantz, S.P. Marijuana use and increased risk of squamous cell carcinoma of the head and neck. Cancer Epidemiol. Biomark. Prev. 1999, 8, 1071–1078. [Google Scholar]
- Hashibe, M.; Ford, D.E.; Zhang, Z.F. Marijuana smoking and head and neck cancer. J. Clin. Pharmacol. 2002, 42, 103S–107S. [Google Scholar] [CrossRef] [PubMed]
- Aldington, S.; Harwood, M.; Cox, B.; Weatherall, M.; Beckert, L.; Hansell, A.; Pritchard, A.; Robinson, G.; Beasley, R. Cannabis use and risk of lung cancer: A case-control study. Eur. Respir. J. 2008, 31, 280–286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Voirin, N.; Berthiller, J.; Benhaim-Luzon, V.; Boniol, M.; Straif, K.; Ayoub, W.B.; Ayed, F.B.; Sasco, A.J. Risk of lung cancer and past use of cannabis in Tunisia. J. Thorac. Oncol. 2006, 1, 577–579. [Google Scholar] [CrossRef] [PubMed]
- Berthiller, J.; Straif, K.; Boniol, M.; Voirin, N.; Benhaim-Luzon, V.; Ayoub, W.B.; Dari, I.; Laouamri, S.; Hamdi-Cherif, M.; Bartal, M.; et al. Cannabis smoking and risk of lung cancer in men: A pooled analysis of three studies in Maghreb. J. Thorac. Oncol. 2008, 3, 1398–1403. [Google Scholar] [CrossRef] [Green Version]
- Sidney, S.; Quesenberry, C.P.; Friedman, G.D.; Tekawa, I.S. Marijuana use and cancer incidence (California, United States). Cancer Causes Control 1997, 8, 722–728. [Google Scholar] [CrossRef]
- Ramos, J.A.; Bianco, F.J. The role of cannabinoids in prostate cancer: Basic science perspective and potential clinical applications. Indian J. Urol. 2012, 28, 9–14. [Google Scholar] [CrossRef]
- Callaghan, R.C.; Allebeck, P.; Akre, O.; McGlynn, K.A.; Sidorchuk, A. Cannabis use and incidence of testicular cancer: A 42-year follow-up of Swedish men between 1970 and 2011. Cancer Epidemiol. Biomark. Prev. 2017, 26, 1644–1652. [Google Scholar] [CrossRef] [Green Version]
- Daling, J.R.; Doody, D.R.; Sun, X.; Trabert, B.L.; Weiss, N.S.; Chen, C.; Biggs, M.L.; Starr, J.R.; Dey, S.K.; Schwartz, S.M. Association of marijuana use and the incidence of testicular germ cell tumors. Cancer 2009, 115, 1215–1223. [Google Scholar] [CrossRef] [Green Version]
- Lacson, J.C.; Carroll, J.D.; Tuazon, E.; Castelao, E.J.; Bernstein, L.; Cortessis, V.K. Population-based case-control study of recreational drug use and testis cancer risk confirms an association between marijuana use and nonseminoma risk. Cancer 2012, 118, 5374–5383. [Google Scholar] [CrossRef] [Green Version]
- Trabert, B.; Sigurdson, A.J.; Sweeney, A.M.; Strom, S.S.; McGlynn, K.A. Marijuana use and testicular germ cell tumors. Cancer 2011, 117, 848–853. [Google Scholar] [CrossRef] [PubMed]
- Luschnig, P.; Schicho, R. Cannabinoids in Gynecological Diseases. Med. Cannabis Cannabinoids 2019, 2, 14–21. [Google Scholar] [CrossRef]
- Efird, J.T.; Friedman, G.D.; Sidney, S.; Klatsky, A.; Habel, L.A.; Udaltsova, N.V.; Van den Eeden, S.; Nelson, L.M. The risk for malignant primary adult-onset glioma in a large, multiethnic, managed-care cohort: Cigarette smoking and other lifestyle behaviors. J. Neurooncol. 2004, 68, 57–69. [Google Scholar] [CrossRef] [PubMed]
- Moiche, B.P.; Atxa de la Presa, M.A.; Cuesta, A.J. Transitional cell carcinoma in a young heavy marihuana smoker. Arch. Esp. Urol. 2001, 54, 165–167. [Google Scholar]
- Chacko, J.A.; Heiner, J.G.; Siu, W.; Macy, M.; Terris, M.K. Association between marijuana use and transitional cell carcinoma. Urology 2006, 67, 100–104. [Google Scholar] [CrossRef] [PubMed]
- Nieder, A.M.; Lipke, M.C.; Madjar, S. Transitional cell carcinoma associated with marijuana: Case report and review of the literature. Urology 2006, 67, 200. [Google Scholar] [CrossRef] [PubMed]
- Bluhm, E.C.; Daniels, J.; Pollock, B.H.; Olshan, A.F. Maternal use of recreational drugs and neuroblastoma in offspring: A report from the Children’s Oncology Group (United States). Cancer Causes Control 2006, 17, 663–669. [Google Scholar] [CrossRef]
- Hashibe, M.; Straif, K.; Tashkin, D.P.; Morgenstern, H.; Greenland, S.; Zhang, Z.F. Epidemiologic review of marijuana use and cancer risk. Alcohol 2005, 35, 265–275. [Google Scholar] [CrossRef]
- Robison, L.L.; Buckley, J.D.; Daigle, A.E.; Wells, R.; Benjamin, D.; Arthur, D.C.; Hammond, G.D. Maternal drug use and risk of childhood nonlymphoblastic leukemia among offspring. An epidemiologic investigation implicating marijuana (a report from the Childrens Cancer Study Group). Cancer 1989, 63, 1904–1911. [Google Scholar] [CrossRef]
- Grobner, S.N.; Worst, B.C.; Weischenfeldt, J.; Buchhalter, I.; Kleinheinz, K.; Rudneva, V.A.; Johann, P.D.; Balasubramanian, G.P.; Segura-Wang, M.; Brabetz, S.; et al. The landscape of genomic alterations across childhood cancers. Nature 2018, 555, 321–327. [Google Scholar] [CrossRef] [Green Version]
- Ma, X.; Liu, Y.; Liu, Y.; Alexandrov, L.B.; Edmonson, M.N.; Gawad, C.; Zhou, X.; Li, Y.; Rusch, M.C.; Easton, J.; et al. Pan-cancer genome and transcriptome analyses of 1699 paediatric leukaemias and solid tumours. Nature 2018, 555, 371–376. [Google Scholar] [CrossRef] [PubMed]
- Kalenderoglou, N.; Macpherson, T.; Wright, W.L. Cannabidiol Reduces Leukemic Cell Size—But Is It Important? Front. Pharmacol. 2017, 8, 144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dando, I.; Donadelli, M.; Costanzo, C.; Dalla Pozza, E.; D’Alessandro, A.; Zolla, L.; Palmieri, M. Cannabinoids inhibit energetic metabolism and induce AMPK-dependent autophagy in pancreatic cancer cells. Cell Death Dis. 2013, 4, e664. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vara, D.; Salazar, M.; Olea-Herrero, N.; Guzmán, M.; Velasco, G.; Díaz-Laviada, I. Anti-tumoral action of cannabinoids on hepatocellular carcinoma: Role of AMPK-dependent activation of autophagy. Cell Death Differ. 2011, 18, 1099–1111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lal, S.; Shekher, A.; Puneet; Narula, A.; Abrahamse, H.; Gupta, S. Cannabis and its constituents for cancer: History, biogenesis, chemistry and pharmacological activities. Pharmacol. Res. 2021, 163, 105302. [Google Scholar] [CrossRef] [PubMed]
- O’Sullivan, S.E. An update on PPAR activation by cannabinoids. Br. J. Pharmacol. 2016, 173, 1899–1910. [Google Scholar] [CrossRef] [Green Version]
- Solinas, M.; Massi, P.; Cinquina, V.; Valenti, M.; Bolognini, D.; Gariboldi, M.; Monti, E.; Rubino, T.; Parolaro, D. Cannabidiol, a non-psychoactive cannabinoid compound, inhibits proliferation and invasion in U87-MG and T98G glioma cells through a multitarget effect. PLoS ONE 2013, 8, e76918. [Google Scholar] [CrossRef] [Green Version]
- Sreevalsan, S.; Joseph, S.; Jutooru, I.; Chadalapaka, G.; Safe, S.H. Induction of apoptosis by cannabinoids in prostate and colon cancer cells is phosphatase dependent. Anticancer Res. 2011, 31, 3799–3807. [Google Scholar]
- Aggarwal, B.B.; Vijayalekshmi, R.V.; Sung, B. Targeting inflammatory pathways for prevention and therapy of cancer: Short-term friend, long-term foe. Clin. Cancer Res. 2009, 15, 425–430. [Google Scholar] [CrossRef] [Green Version]
- Lukhele, S.T.; Motadi, L.R. Cannabidiol rather than Cannabis sativa extracts inhibit cell growth and induce apoptosis in cervical cancer cells. BMC Complement. Altern. Med. 2016, 16, 335. [Google Scholar] [CrossRef] [Green Version]
- Calvaruso, G.; Pellerito, O.; Notaro, A.; Giuliano, M. Cannabinoid-associated cell death mechanisms in tumor models (Review). Int. J. Oncol. 2012, 41, 407–413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galanti, G.; Fisher, T.; Kventsel, I.; Shoham, J.; Gallily, R.; Mechoulam, R.; Lavie, G.; Amariglio, N.; Rechavi, G.; Toren, A. Δ9-tetrahydrocannabinol inhibits cell cycle progression by downregulation of E2F1 in human glioblastoma multiforme cells. Acta Oncol. 2008, 47, 1062–1070. [Google Scholar] [CrossRef] [PubMed]
- Caffarel, M.M.; Sarrió, D.; Palacios, J.; Guzmán, M.; Sánchez, C. Δ9-tetrahydrocannabinol inhibits cell cycle progression in human breast cancer cells through Cdc2 regulation. Cancer Res. 2006, 66, 6615–6621. [Google Scholar] [CrossRef] [Green Version]
- Mangal, N.; Erridge, S.; Habib, N.; Sadanandam, A.; Reebye, V.; Sodergren, M.H. Cannabinoids in the landscape of cancer. J. Cancer Res. Clin. Oncol. 2021, 147, 2507–2534. [Google Scholar] [CrossRef] [PubMed]
- Nagarkatti, P.; Pandey, R.; Rieder, S.A.; Hegde, V.L.; Nagarkatti, M. Cannabinoids as novel anti-inflammatory drugs. Future Med. Chem. 2009, 1, 1333–1349. [Google Scholar] [CrossRef] [Green Version]
- Bifulco, M.; Laezza, C.; Pisanti, S.; Gazzerro, P. Cannabinoids and cancer: Pros and cons of an antitumour strategy. Br. J. Pharmacol. 2006, 148, 123–135. [Google Scholar] [CrossRef]
- Fogaca, M.V.; Campos, A.C.; Coelho, L.D.; Duman, R.S.; Guimarães, F.S. The anxiolytic effects of cannabidiol in chronically stressed mice are mediated by the endocannabinoid system: Role of neurogenesis and dendritic remodeling. Neuropharmacology 2018, 135, 22–33. [Google Scholar] [CrossRef]
- Johnson, J.R.; Lossignol, D.; Burnell-Nugent, M.; Fallon, M.T. An open-label extension study to investigate the long-term safety and tolerability of THC/CBD oromucosal spray and oromucosal THC spray in patients with terminal cancer-related pain refractory to strong opioid analgesics. J. Pain Symptom Manag. 2013, 46, 207–218. [Google Scholar] [CrossRef]
- Klein, T.W.; Lane, B.; Newton, C.A.; Friedman, H. The cannabinoid system and cytokine network. Proc. Soc. Exp. Biol. Med. 2000, 225, 1–8. [Google Scholar] [CrossRef]
- Jeong, S.; Jo, M.J.; Yun, H.K.; Kim, D.Y.; Kim, B.R.; Kim, J.L.; Park, S.H.; Na, Y.J.; Jeong, Y.A.; Kim, B.G.; et al. Cannabidiol promotes apoptosis via regulation of XIAP/Smac in gastric cancer. Cell Death Dis. 2019, 10, 846. [Google Scholar] [CrossRef] [Green Version]
- Sawtelle, L.; Holle, L.M. Use of Cannabis and Cannabinoids in Patients with Cancer. Ann. Pharmacother. 2021, 55, 870–890. [Google Scholar] [CrossRef] [PubMed]
- Zaiachuk, M.; Pryimak, N.; Kovalchuk, O.; Kovalchuk, I. Cannabinoids, Medical Cannabis, and Colorectal Cancer Immunotherapy. Front. Med. 2021, 8, 713153. [Google Scholar] [CrossRef] [PubMed]
- Mazuz, M.; Tiroler, A.; Moyal, L.; Hodak, E.; Nadarajan, S.; Vinayaka, A.C.; Gorovitz-Haris, B.; Lubin, I.; Drori, A.; Drori, G.; et al. Synergistic cytotoxic activity of cannabinoids from Cannabis sativa against cutaneous T-cell lymphoma (CTCL) in-vitro and ex-vivo. Oncotarget 2020, 11, 1141–1156. [Google Scholar] [CrossRef] [Green Version]
- Meng, H.; Dai, T.; Hanlon, J.G.; Downar, J.; Alibhai, S.M.H.; Clarke, H. Cannabis and cannabinoids in cancer pain management. Curr. Opin. Support. Palliat. Care. 2020, 14, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Pergam, S.A.; Woodfield, M.C.; Lee, C.M.; Cheng, G.S.; Baker, K.K.; Marquis, S.R.; Fann, J.R. Cannabis use among patients at a comprehensive cancer center in a state with legalized medicinal and recreational use. Cancer 2017, 123, 4488–4497. [Google Scholar] [CrossRef] [Green Version]
- Braun, I.M.; Wright, A.; Peteet, J.; Meyer, F.L.; Yuppa, D.P.; Bolcic-Jankovic, D.; LeBlanc, J.; Chang, Y.; Yu, L.; Nayak, M.M.; et al. Medical oncologists’ beliefs, practices, and knowledge regarding marijuana used thera-peutically: A nationally representative survey study. J. Clin. Oncol. 2018, 36, 1957–1962. [Google Scholar] [CrossRef] [PubMed]
- Zylla, D.; Steele, G.; Eklund, J.; Mettner, J.; Arneson, T. Oncology clinicians and the Minnesota medical cannabis program: A survey on medical cannabis practice patterns, barriers to enrollment, and educational needs. Cannabis Cannabinoid Res. 2018, 3, 195–202. [Google Scholar] [CrossRef] [Green Version]
- Shi, S.; Brant, A.R.; Sabolch, A.; Pollom, E. False news of a cannabis cancer cure. Cureus 2019, 11, e3918. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guggisberg, J.; Schumacher, M.; Gilmore, G.; Zylla, D.M. Cannabis as an anticancer agent: A review of clinical data and assessment of case reports. Cannabis Cannabinoid Res. 2022, 7, 24–33. [Google Scholar] [CrossRef]
- Available online: www.catasurvey.com (accessed on 22 June 2022).
- Twelves, C.J.; Sabel, M.J.; Checketts, D.J.; Miller, S.J.; Tayo, B.J.; Jove, M.J.; Brazil, L.J.; Short, S.C. A phase 1b randomised, placebo-controlled trial of nabiximols cannabinoid oromucosal spray with temozolomide in patients with recurrent glioblastoma. Br. J. Cancer 2021, 124, 1379–1387. [Google Scholar] [CrossRef]
- Bar-Sela, G.; Cohen, I.; Campisi-Pinto, S.; Lewitus, G.M.; Oz-Ari, L.; Jehassi, A.; Peer, A.; Turgeman, I.; Vernicova, O.; Berman, P.; et al. Cannabis Consumption Used by Cancer Patients during Immunotherapy Correlates with Poor Clinical Outcome. Cancers 2020, 12, 2447. [Google Scholar] [CrossRef] [PubMed]
- Taha, T.; Meiri, D.; Talhamy, S.; Wollner, M.; Peer, A.; Bar-Sela, G. Cannabis Impacts Tumor Response Rate to Nivolumab in Patients with Advanced Malignancies. Oncologist 2019, 24, 549–554. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guzmán, M.; Duarte, M.J.; Blázquez, C.; Ravina, J.; Rosa, M.C.; Galve-Roperh, I.; Sánchez, C.; Velasco, G.; González-Feria, L. A pilot clinical study of Δ9-tetrahydrocannabinol in patients with recurrent glioblastoma multiforme. Br. J. Cancer 2006, 95, 197–203. [Google Scholar] [CrossRef]
- Schloss, J.; Lacey, J.; Sinclair, J.; Steel, A.; Sughrue, M.; Sibbritt, D.; Teo, C.A. Phase 2 Randomised Clinical Trial Assessing the Tolerability of Two Different Ratios of Medicinal Cannabis in Patients with High Grade Gliomas. Front. Oncol. 2021, 11, 649555. [Google Scholar] [CrossRef] [PubMed]
- Verkhratsky, A.; Butt, A. Glial Neurobiology: A Textbook; John Wiley & Sons: Hoboken, NJ, USA, 2007. [Google Scholar]
- Boland, E.G.; Bennett, M.I.; Allgar, V.; Boland, J.W. Cannabinoids for adult cancer related pain: Systematic review and meta-analysis. BMJ Support. Palliat. Care 2020, 10, 14–24. [Google Scholar] [CrossRef] [Green Version]
- Dinitto, D.M.; Choi, N.G. Marijuana use among older adults in the U.S.A.: User characteristics, patterns of use, and implications for intervention. Int. Psychogeriatr. 2011, 23, 732–741. [Google Scholar] [CrossRef]
- Williamson, E.M.; Evans, F.J. Cannabinoids in clinical practice. Drugs 2000, 60, 1303–1314. [Google Scholar] [CrossRef]
- Zehra, A.; Burns, J.; Liu, C.K.; Manza, P.; Wiers, C.E.; Volkow, N.D.; Wang, G.J. Cannabis Addiction and the Brain: A Review. J. Neuroimmune Pharmacol. 2018, 13, 438–452. [Google Scholar] [CrossRef] [Green Version]
- Pearson, N.T.; Berry, J.H. Cannabis and Psychosis Through the Lens of DSM-5. Int. J. Environ. Res. Public Health 2019, 16, 4149. [Google Scholar] [CrossRef] [Green Version]
- Batalla, A.; Janssen, H.; Gangadin, S.S.; Bossong, M.G. The Potential of Cannabidiol as a Treatment for Psychosis and Addiction: Who Benefits Most? A Systematic Review. J. Clin. Med. 2019, 8, 1058. [Google Scholar] [CrossRef] [Green Version]
- Sexton, M.; Garcia, J.M.; Jatoi, A.; Clark, C.S.; Wallace, M.S. The management of cancer symptoms and treatment-induced side effects with cannabis or cannabinoids. JNCI Monogr. 2021, 2021, 86–98. [Google Scholar] [CrossRef] [PubMed]
- Guan, X. Cancer metastases: Challenges and opportunities. Acta Pharm. Sin. B 2015, 5, 402–418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Available online: https://clinicaltrials.gov/ct2/results?term=cannabis&cond=Cancer&Search=Apply&recrs=a&age_v=&gndr=&type=&rslt= (accessed on 22 June 2022).


{kind=link}
| Author | Country | Study Type | Number | Intervention | Administration | Daily Dose | Dosing Schedule | Duration | Outcome Measures | Primary Outcomes | Strengths and Limitations | Link |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Twelves et al., 2021 [76] | United Kingdom [UK] | Phase 1b randomized, double-blind, placebo-controlled clinical trial | 21 (12 in the active arm, 9 in placebo) | Sativex® (Nabiximols spray) | Oromucosal spray | Up to 12 sprays or 30 mg CBD/32.4 mg THC | Controlled | 24.9 weeks for the Sativex ® group and 23.6 weeks for the placebo group | Magnetic resonance (MRI) | Co-administration of the Sativex® in cancer patients treated with temozolomide demonstrated that, in the Sativex® group, the overall survival benefit was 21.8 months compared with 12.1 months for the placebo group. One-year survival in favor of nabiximols was statistically significant (p = 0.042). | Strengths
| https://www.nature.com/articles/s41416-021-01259-3(accessed on 5 January 2022) |
| Bar-Sela et al., 2020 [77] | Israel | Prospective observatory study | 102 (68 immunotherapy and 34 immunotherapy (anti-PD-1 (Pembrolizumab or Nivolumab; IPIlimumab and Nivolumab) and anti-PD-L1 (Durvalumab or Atezolizumab)) plus cannabis) | Cannabis oil, combined oil and flowers | The use of cannabis had been started nine months to two weeks before the first immunotherapy treatment. The patients had permission to change cannabis products monthly. | Up to 40 g per month of cannabis | Uncontrolled | 11–14 weeks of treatment | Panel of serum endocannabinoids (eCBs) and eCB-like lipids | Initiating immunotherapy with cannabis use negatively affects OS and time to tumor progression of cancer patients treated with immunotherapy. The median survival was 6.4 months in those using cannabis and 28.5 months in those who were not. The patient group using cannabis (34 patients) were found to have a statistically significant reduction in the rate of response to immunotherapy agents and also a significantly shorter time to progression (p = 0.0025) and reduced overall survival (p = 0.00094) when compared to the group of non-cannabis users (68 patients). The cannabis user group also experienced fewer treatment-related adverse events when compared to the non-using patients (p = 0.057). | Strengths
| https://www.mdpi.com/2072-6694/12/9/2447(accessed on 5 January 2022) |
| Taha et al., 2019 [78] | Israel | Retrospective observational study | 140 patients (89 nivolumab alone, 51 nivolumab plus cannabis) with stage IV non-small cell lung cancer (NSCLC) or clear cell renal cell carcinoma (RCC) or advanced melanoma | Cannabidiol, tetrahydrocannabinol | Smoked or inhaled (cannabis flowers only), prepared cannabis oil, or combined use | Up to 30 g per month of cannabis | Uncontrolled | 1 year | The response rate was evaluated using RECIST criteria based on imaging assessments carried out every 11–14 weeks. | Cannabis users showed a less favorable prognosis in terms of response rate (RR), which was reduced in the nivolumab–cannabis group compared to the nivolumab group (p = 0.016). Cannabis use did not significantly influence the progression-free survival (PFS) or the overall survival (OS). Cannabis composition had no influence on the results. | Strengths
| https://pubmed.ncbi.nlm.nih.gov/30670598/(accessed on 5 January 2022) |
| Guzmán et al., 2006 [79] | Spain | Pilot phase I controlled clinical trial | 9 patients with glioblastoma | Δ9-Tetrahydrocannabinol (THC) | Intratumorally | Daily intracranial administration of delta-9 THC | Total doses ranging from 0.8 mg to 3.29 mg | Range of 10–64 days | Biopsies of the treated tumors, MRI | Δ9-Tetrahydrocannabinol inhibited tumor-cell proliferation in vitro and decreased tumor-cell Ki67 immunostaining when administered to two patients. Median survival rate from the surgical operation of tumor relapse was 24 weeks. Two of the patients (3 and 8) survived for approximately 1 year. | Strengths
| https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2360617/.(accessed on 5 January 2022) |
| Schloss et al., 2021 [80] | Australia | Phase 2 randomized, double-blind clinical trial | 88 patients with high-grade glioma | THC and cannabidiol (CBD) | Oil ingested orally | 1:1 THC 4.6 mg/mL: cannabidiol (CBD) 4.8 mg/mL and 4:1 THC 15 mg/mL: CBD 3.8 mg/mL | Controlled | 12 weeks | The Functional Assessment of Cancer Therapy—Brain (FACT-Br), participant diary and MRI results imaging assessments | Physical and functional domains of quality of life and sleep were improved in the group with a THC:CBD ratio of 1:1 compared with the group with a ratio of 4:1. Although the primary objective was to assess tolerability of the two ratios, MRI scans were performed in 53 participants at baseline and after 12 weeks because disease status was a secondary outcome. After 12 weeks, disease had regressed in 11%, was stable in 34%, had T2 flair and mild enhancement in 16%, and had progressed in 10%. No differences in treatment outcomes were observed between groups. | Strengths
| https://www.frontiersin.org/articles/10.3389/fonc.2021.649555/full(accessed on 5 January 2022) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hanganu, B.; Lazar, D.E.; Manoilescu, I.S.; Mocanu, V.; Butcovan, D.; Buhas, C.L.; Szalontay, A.S.; Ioan, B.G. Controversial Link between Cannabis and Anticancer Treatments—Where Are We and Where Are We Going? A Systematic Review of the Literature. Cancers 2022, 14, 4057. https://doi.org/10.3390/cancers14164057
Hanganu B, Lazar DE, Manoilescu IS, Mocanu V, Butcovan D, Buhas CL, Szalontay AS, Ioan BG. Controversial Link between Cannabis and Anticancer Treatments—Where Are We and Where Are We Going? A Systematic Review of the Literature. Cancers. 2022; 14(16):4057. https://doi.org/10.3390/cancers14164057
Chicago/Turabian StyleHanganu, Bianca, Diana Elena Lazar, Irina Smaranda Manoilescu, Veronica Mocanu, Doina Butcovan, Camelia Liana Buhas, Andreea Silvana Szalontay, and Beatrice Gabriela Ioan. 2022. "Controversial Link between Cannabis and Anticancer Treatments—Where Are We and Where Are We Going? A Systematic Review of the Literature" Cancers 14, no. 16: 4057. https://doi.org/10.3390/cancers14164057