
Opioid-Induced Sexual Dysfunction in Cancer Patients



Abstract
:Simple Summary
Abstract
1. Introduction
2. Etiology and Pathophysiology
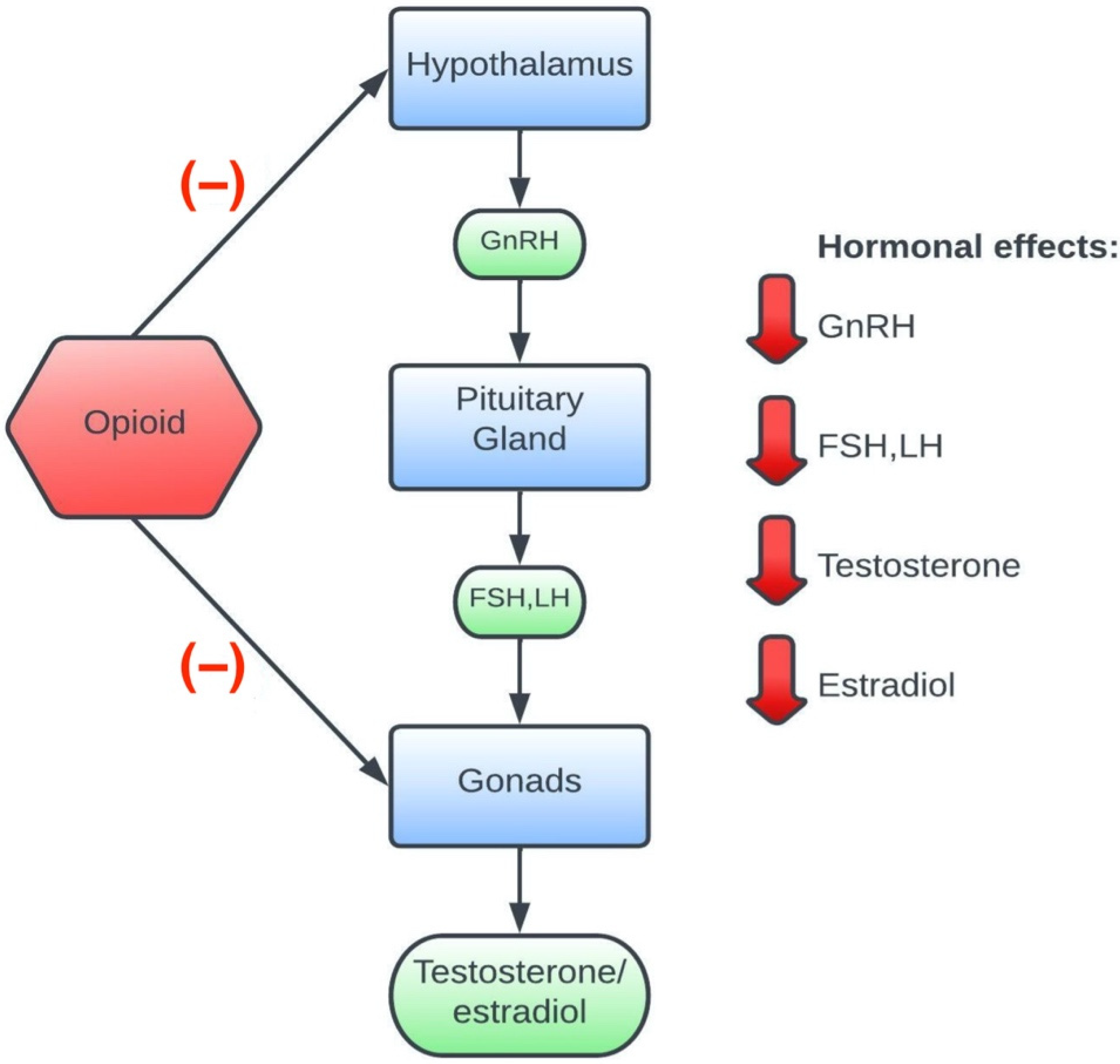
2.1. The Role of Hormones
2.2. Sexual Desire
2.3. Erection
2.4. Orgasm
3. Diagnostic Tools
3.1. Female Sexual Function Index (FSFI)
3.2. International Index of Erectile Function (IIEF)
4. Epidemiology
4.1. Sexual Disorders in Cancer Patients
4.2. Sexual Dysfunction in Patients Taking Opioids
4.2.1. Tramadol
4.2.2. Morphine
4.2.3. Methadone and Buprenorphine
4.2.4. Tapentadol
5. Treatment of Opioid-Induced Sexual Dysfunction
5.1. Testosterone Replacement Ttherapy
5.2. Bupropion and Trazodone
5.3. Opioid Receptor Antagonists
5.4. Plant-Derived Medicines
5.5. Non-Pharmacological Methods
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Rosales, A.R.; Byrne, D.; Burnham, C.; Watts, L.; Clifford, K.; Zuckerman, D.S.; Beck, T. Comprehensive Survivorship Care with Cost and Revenue Analysis. J. Oncol. Pract. 2013, 10, e81–e85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schover, L.R.; van der Kaaij, M.; van Dorst, E.; Creutzberg, C.; Huyghe, E.; Kiserud, C.E. Sexual Dysfunction and Infertility as Late Effects of Cancer Treatment. Eur. J. Cancer Suppl. 2014, 12, 41–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lemieux, L.; Kaiser, S.; Pereira, J.; Meadows, L.M. Sexuality in Palliative Care: Patient Perspectives. Palliat. Med. 2004, 18, 630–637. [Google Scholar] [CrossRef]
- Ussher, J.M.; Perz, J.; Gilbert, E. Perceived Causes and Consequences of Sexual Changes after Cancer for Women and Men: A Mixed Method Study. BMC Cancer 2015, 15, 268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shell, J.A. Sexual Issues in the Palliative Care Population. Semin. Oncol. Nurs. 2008, 24, 131–134. [Google Scholar] [CrossRef]
- Bond, C.B.; Jensen, P.T.; Groenvold, M.; Johnsen, A.T. Prevalence and Possible Predictors of Sexual Dysfunction and Self-Reported Needs Related to the Sexual Life of Advanced Cancer Patients. Acta Oncol. 2019, 58, 769–775. [Google Scholar] [CrossRef] [PubMed]
- ICD-11 for Mortality and Morbidity Statistics. Available online: https://icd.who.int/browse11/l-m/en (accessed on 22 May 2022).
- Schover, L.R. Sexual Quality of Life in Men and Women after Cancer. Climacteric 2019, 22, 553–557. [Google Scholar] [CrossRef]
- Gannon, J.R.; Walsh, T.J. Testosterone and Sexual Function. Urol. Clin. N. Am. 2016, 43, 217–222. [Google Scholar] [CrossRef]
- Basson, R.; Brotto, L.A.; Petkau, A.J.; Labrie, F. Role of Androgens in Women’s Sexual Dysfunction. Menopause 2010, 17, 962–971. [Google Scholar] [CrossRef]
- Davis, S.R.; Wahlin-Jacobsen, S. Testosterone in Women-the Clinical Significance. Lancet Diabetes Endocrinol. 2015, 3, 980–992. [Google Scholar] [CrossRef]
- Traish, A.M.; Paco Kang, H.; Saad, F.; Guay, A.T. Dehydroepiandrosterone (DHEA)—A Precursor Steroid or an Active Hormone in Human Physiology. J. Sex. Med. 2011, 8, 2960–2982. [Google Scholar] [CrossRef] [PubMed]
- Krüger, T.H.C.; Haake, P.; Hartmann, U.; Schedlowski, M.; Exton, M.S. Orgasm-Induced Prolactin Secretion: Feedback Control of Sexual Drive? Neurosci. Biobehav. Rev. 2002, 26, 31–44. [Google Scholar] [CrossRef]
- Stuckey, B.G.A. Female Sexual Function and Dysfunction in the Reproductive Years: The Influence of Endogenous and Exogenous Sex Hormones. J. Sex. Med. 2008, 5, 2282–2290. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.J.; Macbeth, A.H.; Pagani, J.H.; Scott Young, W. Oxytocin: The Great Facilitator of Life. Prog. Neurobiol. 2009, 88, 127–151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bedos, M.; Antaramian, A.; Gonzalez-Gallardo, A.; Paredes, R.G. Paced Mating Increases the Expression of μ Opioid Receptors in the Ventromedial Hypothalamus of Male Rats. Behav. Brain Res. 2019, 359, 401–407. [Google Scholar] [CrossRef]
- Carretero, J.; Bodego, P.; Rodríguez, R.E.; Rubio, M.; Blanco, E.; Burks, D.J. Expression of the μ-Opioid Receptor in the Anterior Pituitary Gland Is Influenced by Age and Sex. Neuropeptides 2004, 38, 63–68. [Google Scholar] [CrossRef]
- Estomba, H.; Muñoa-Hoyos, I.; Gianzo, M.; Urizar-Arenaza, I.; Casis, L.; Irazusta, J.; Subirán, N. Expression and Localization of Opioid Receptors in Male Germ Cells and the Implication for Mouse Spermatogenesis. PLoS ONE 2016, 11, e0152162. [Google Scholar] [CrossRef] [Green Version]
- Kaminski, T. The Involvement of Protein Kinases in Signalling of Opioid Agonist FK 33-824 in Porcine Granulosa Cells. Anim. Reprod. Sci. 2006, 91, 107–122. [Google Scholar] [CrossRef]
- Katz, N.; Mazer, N.A. The Impact of Opioids on the Endocrine System. Clin. J. Pain 2009, 25, 170–175. [Google Scholar] [CrossRef]
- Aloisi, A.M.; Ceccarelli, I.; Fiorenzani, P.; Maddalena, M.; Rossi, A.; Tomei, V.; Sorda, G.; Danielli, B.; Rovini, M.; Cappelli, A.; et al. Aromatase and 5-Alpha Reductase Gene Expression: Modulation by Pain and Morphine Treatment in Male Rats. Mol. Pain 2010, 6, 69. [Google Scholar] [CrossRef] [Green Version]
- Nimbi, F.M.; Tripodi, F.; Rossi, R.; Navarro-Cremades, F.; Simonelli, C. Male Sexual Desire: An Overview of Biological, Psychological, Sexual, Relational, and Cultural Factors Influencing Desire. Sex. Med. Rev. 2020, 8, 59–91. [Google Scholar] [CrossRef] [PubMed]
- Dosch, A.; Rochat, L.; Ghisletta, P.; Favez, N.; van der Linden, M. Psychological Factors Involved in Sexual Desire, Sexual Activity, and Sexual Satisfaction: A Multi-Factorial Perspective. Arch. Sex. Behav. 2016, 45, 2029–2045. [Google Scholar] [CrossRef] [PubMed]
- Kingsberg, S.A.; Clayton, A.H.; Pfaus, J.G. The Female Sexual Response: Current Models, Neurobiological Underpinnings and Agents Currently Approved or under Investigation for the Treatment of Hypoactive Sexual Desire Disorder. CNS Drugs 2015, 29, 915–933. [Google Scholar] [CrossRef] [PubMed]
- McCabe, M.P.; Sharlip, I.D.; Atalla, E.; Balon, R.; Fisher, A.D.; Laumann, E.; Lee, S.W.; Lewis, R.; Segraves, R.T. Definitions of Sexual Dysfunctions in Women and Men: A Consensus Statement from the Fourth International Consultation on Sexual Medicine. J. Sex. Med. 2016, 13, 135–143. [Google Scholar] [CrossRef]
- Jung, J.; Jo, H.W.; Kwon, H.; Jeong, N.Y. Clinical Neuroanatomy and Neurotransmitter-Mediated Regulation of Penile Erection. Int. Neurourol. J. 2014, 18, 58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andersson, K.-E. Mechanisms of Penile Erection and Basis for Pharmacological Treatment of Erectile Dysfunction. Pharmacol. Rev. 2011, 63, 811–859. [Google Scholar] [CrossRef]
- Andersson, K.-E. Erectile Physiological and Pathophysiological Pathways Involved in Erectile Dysfunction. J. Urol. 2003, 170, S6–S14. [Google Scholar] [CrossRef]
- Mckinlay, J. The Worldwide Prevalence and Epidemiology of Erectile Dysfunction. Int. J. Impot. Res. 2000, 12, S6–S11. [Google Scholar] [CrossRef] [Green Version]
- Chew, K.K. Prevalence of Erectile Dysfunction in Community-Based Studies. Int. J. Impot. Res. 2004, 16, 201–202. [Google Scholar] [CrossRef] [Green Version]
- Grover, S.A.; Lowensteyn, I.; Kaouache, M.; Marchand, S.; Coupal, L.; DeCarolis, E.; Zoccoli, J.; Defoy, I. The Prevalence of Erectile Dysfunction in the Primary Care Setting: Importance of Risk Factors for Diabetes and Vascular Disease. Arch. Intern. Med. 2006, 166, 213–219. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, H.M.T.; Gabrielson, A.T.; Hellstrom, W.J.G. Erectile Dysfunction in Young Men—A Review of the Prevalence and Risk Factors. Sex. Med. Rev. 2017, 5, 508–520. [Google Scholar] [CrossRef] [PubMed]
- Pizzol, D.; Xiao, T.; Smith, L.; Sanchez, G.F.L.; Garolla, A.; Parris, C.; Barnett, Y.; Ilie, P.C.; Soysal, P.; Shin, J.I.; et al. Prevalence of Erectile Dysfunction in Male Survivors of Cancer: A Systematic Review and Meta-Analysis of Cross-Sectional Studies. Br. J. Gen. Pract. 2021, 71, e372. [Google Scholar] [CrossRef] [PubMed]
- Toda, N.; Kishioka, S.; Hatano, Y.; Toda, H. Interactions between Morphine and Nitric Oxide in Various Organs. J. Anesth. 2009, 23, 554–568. [Google Scholar] [CrossRef]
- Agmo, A.; Rojas, J.; Vazquez, P. Inhibitory Effect of Opiates on Male Rat Sexual Behavior May Be Mediated by Opiate Receptors Outside the Central Nervous System. Psychopharmacol. Berl. 1992, 107, 89–96. [Google Scholar] [CrossRef] [PubMed]
- Meston, C.M.; Hull, E.; Levin, R.J.; Sipski, M. Disorders of Orgasm in Women. J. Sex. Med. 2004, 1, 66–68. [Google Scholar] [CrossRef]
- Rowland, D.; McMahon, C.G.; Abdo, C.; Chen, J.; Jannini, E.; Waldinger, M.D.; Ahn, T.Y. Disorders of Orgasm and Ejaculation in Men. J. Sex. Med. 2010, 7, 1668–1686. [Google Scholar] [CrossRef]
- Alwaal, A.; Breyer, B.N.; Lue, T.F. Normal Male Sexual Function: Emphasis on Orgasm and Ejaculation. Fertil Steril 2015, 104, 1051. [Google Scholar] [CrossRef] [Green Version]
- Meston, C.M.; Freihart, B.K.; Handy, A.B.; Kilimnik, C.D.; Rosen, R.C. Scoring and Interpretation of the FSFI: What Can Be Learned From 20 Years of Use? J. Sex. Med. 2020, 17, 17–25. [Google Scholar] [CrossRef]
- Baser, R.E.; Li, Y.; Carter, J. Psychometric Validation of the Female Sexual Function Index (FSFI) in Cancer Survivors. Cancer 2012, 118, 4606–4618. [Google Scholar] [CrossRef]
- Jeffery, D.D.; Tzeng, J.P.; Keefe, F.J.; Porter, L.S.; Hahn, E.A.; Flynn, K.E.; Reeve, B.B.; Weinfurt, K.P. Initial Report of the Cancer Patient-Reported Outcomes Measurement Information System (PROMIS) Sexual Function Committee: Review of Sexual Function Measures and Domains Used in Oncology. Cancer 2009, 115, 1142–1153. [Google Scholar] [CrossRef] [Green Version]
- Denlinger, C.S.; Carlson, R.W.; Are, M.; Baker, K.S.; Davis, E.; Edge, S.B.; Friedman, D.L.; Goldman, M.; Jones, L.; King, A.; et al. Survivorship: Sexual Dysfunction (Female), Version 1.2013: Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2014, 12, 184. [Google Scholar] [CrossRef] [Green Version]
- Rosen, R.C.; Riley, A.; Wagner, G.; Osterloh, I.H.; Kirkpatrick, J.; Mishra, A. The International Index of Erectile Function (IIEF): A Multidimensional Scale For Assesment of Erectile Dysfunction. J. Sex. Med. 1997, 49, 822–830. [Google Scholar] [CrossRef] [Green Version]
- Rosen, R.; Cappelleri, J.; Lipsky, J.; Pen, Ä.B. Development and Evaluation of an Abridged, 5-Item Version of the International Index of Erectile Function (IIEF-5) as a Diagnostic Tool for Erectile Dysfunction. Nature 1999, 11, 319–326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Litwin, M.S.M.M.; Hays, R.D.P.; Fink, A.P.; Ganz, P.A.M.; Leake, B.P.; Brook, R.H.M.S. The UCLA Prostate Cancer Index: Development, Reliability, and Validity of a Health-Related Quality of Life Measure. Med. Care 1998, 36, 1002–1012. [Google Scholar] [CrossRef] [PubMed]
- Jensen, P.T.; Klee, M.C.; Thranov, I.; Groenvold, M. Validation of a Questionnaire for Self-Assessment of Sexual Function and Vaginal Changes after Gynaecological Cancer. Psycho-Oncology 2004, 13, 577–592. [Google Scholar] [CrossRef] [PubMed]
- Bartula, I.; Sherman, K.A. Development and Validation of the Female Sexual Function Index Adaptation for Breast Cancer Patients (FSFI-BC). Breast Cancer Res. Treat. 2015, 152, 477–488. [Google Scholar] [CrossRef] [PubMed]
- Maiorino, M.I.; Chiodini, P.; Bellastella, G.; Giugliano, D.; Esposito, K. Sexual Dysfunction in Women with Cancer: A Systematic Review with Meta-Analysis of Studies Using the Female Sexual Function Index. Endocrine 2016, 54, 329–341. [Google Scholar] [CrossRef]
- Bruner, D.W.; Calvano, T. The Sexual Impact of Cancer and Cancer Treatments in Men. Nurs. Clin. N. Am. 2007, 42, 555–580. [Google Scholar] [CrossRef]
- Rajagopal, A.; Vassilopoulou-Sellin, R.; Palmer, J.L.; Kaur, G.; Bruera, E. Symptomatic Hypogonadism in Male Survivors of Cancer with Chronic Exposure to Opioids. Cancer 2004, 100, 851–858. [Google Scholar] [CrossRef]
- Venkatesh, K.; Mattoo, S.K.; Grover, S. Sexual Dysfunction in Men Seeking Treatment for Opioid Dependence: A Study from India. J. Sex. Med. 2014, 11, 2055–2064. [Google Scholar] [CrossRef]
- Zhao, S.; Deng, T.; Luo, L.; Wang, J.; Li, E.; Liu, L.; Li, F.; Luo, J.; Zhao, Z. Association Between Opioid Use and Risk of Erectile Dysfunction: A Systematic Review and Meta-Analysis. J. Sex. Med. 2017, 14, 1209–1219. [Google Scholar] [CrossRef] [PubMed]
- Deyo, R.A.; Smith, D.H.M.; Johnson, E.S.; Tillotson, C.J.; Donovan, M.; Yang, X.; Petrik, A.; Morasco, B.J.; Dobscha, S.K. Prescription Opioids for Back Pain and Use of Medications for Erectile Dysfunction. Spine Phila Pa 1976 2013, 38, 909–915. [Google Scholar] [CrossRef] [PubMed]
- Ajo, R.; Segura, A.; Inda, M.-D.-M.; Margarit, C.; Ballester, P.; Martínez, E.; Ferrández, G.; Sánchez-Barbie, Á.; Peiró, A.M. Erectile Dysfunction in Patients with Chronic Pain Treated with Opioids. Med. Clín. 2017, 149, 49–54. [Google Scholar] [CrossRef]
- Rubinstein, A.L.; Carpenter, D.M.; Minkoff, J.R. Hypogonadism in Men With Chronic Pain Linked to the Use of Long-Acting Rather Than Short-Acting Opioids. Clin. J. Pain 2013, 29, 840–845. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hashim, M.A.; el Rasheed, A.H.; Ismail, G.A.W.; Awaad, M.I.; el Habiby, M.M.; Mohsen Ibrahim, N.M.; Abdeen, M.S. Sexual Dysfunction in Tramadol Hydrochloride Use Disorder Male Patients: A Case-Control Study. Int. Clin. Psychopharmacol. 2020, 35, 42–48. [Google Scholar] [CrossRef] [PubMed]
- Kabbash, A.; el Kelany, R.; Oreby, M.; el Gameel, D. Effect of Tramadol Dependence on Male Sexual Dysfunction. Interdiscip. Toxicol. 2019, 12, 157. [Google Scholar] [CrossRef]
- Kozyrev, N.; Coolen, L.M. Activation of Mu or Delta Opioid Receptors in the Lumbosacral Spinal Cord Is Essential for Ejaculatory Reflexes in Male Rats. PLoS ONE 2015, 10, e0121130. [Google Scholar] [CrossRef] [Green Version]
- Martyn-St James, M.; Cooper, K.; Kaltenthaler, E.; Dickinson, K.; Cantrell, A.; Wylie, K.; Frodsham, L.; Hood, C. Tramadol for Premature Ejaculation: A Systematic Review and Meta-Analysis. BMC Urol. 2015, 15, 6. [Google Scholar] [CrossRef] [Green Version]
- Gomez-Marrero, J.; Feria, M.; Mas, M. Stimulation of Opioid Receptors Suppresses Penile Erectile Reflexes and Seminal Emission in Rats. Pharmacol. Biochem. Behav. 1988, 31, 393–396. [Google Scholar] [CrossRef]
- Yee, A.; Loh, H.S.; Maria, H.; Hashim, H.; Ng, C.G. The Prevalence of Sexual Dysfunction among Male Patients on Methadone and Buprenorphine Treatments: A Meta-Analysis Study. J. Sex. Med. 2013, 11, 22–32. [Google Scholar] [CrossRef]
- Yee, A.; Loh, H.S.; Loh, H.H.; Riahi, S.; Ng, C.G.; Sulaiman, A.H. bin A Comparison of Sexual Desire in Opiate-Dependent Men Receiving Methadone and Buprenorphine Maintenance Treatment. Ann. Gen. Psychiatry 2019, 18, 25. [Google Scholar] [CrossRef] [PubMed]
- Hallinan, R.; Byrne, A.; Agho, K.; McMahon, C.; Tynan, P.; Attia, J. Erectile Dysfunction in Men Receiving Methadone and Buprenorphine Maintenance Treatment. J. Sex. Med. 2007, 5, 684–692. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zamboni, L.; Franceschini, A.; Portoghese, I.; Morbioli, L.; Lugoboni, F. Sexual Functioning and Opioid Maintenance Treatment in Women. Results from a Large Multicentre Study. Front. Behav. Neurosci. 2019, 13, 97. [Google Scholar] [CrossRef] [Green Version]
- Varma, A.; Sapra, M.; Iranmanesh, A. Impact of Opioid Therapy on Gonadal Hormones: Focus on Buprenorphine. Horm. Mol. Biol. Clin. Investig. 2018, 36, 20170080. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baron, R.; Jansen, J.P.; Binder, A.; Pombo-Suarez, M.; Kennes, L.; Müller, M.; Falke, D.; Steigerwald, I. Tolerability, Safety, and Quality of Life with Tapentadol Prolonged Release (PR) Compared with Oxycodone/Naloxone PR in Patients with Severe Chronic Low Back Pain with a Neuropathic Component: A Randomized, Controlled, Open-Label, Phase 3b/4 Trial. Pain Pract. 2016, 16, 600–619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- AminiLari, M.; Manjoo, P.; Craigie, S.; Couban, R.; Wang, L.; Busse, J.W. Hormone Replacement Therapy and Opioid Tapering for Opioid-Induced Hypogonadism among Patients with Chronic Noncancer Pain: A Systematic Review. Pain Med. 2019, 20, 301–313. [Google Scholar] [CrossRef]
- Yee, A.; Loh, H.S.; Ong, T.A.; Guan Ng, C.; Sulaiman, A.H. Randomized, Double-Blind, Parallel-Group, Placebo-Controlled Trial of Bupropion as Treatment for Methadone-Emergent Sexual Dysfunction in Men. Am. J. Men Health 2018, 12, 1705–1718. [Google Scholar] [CrossRef] [Green Version]
- Tatari, F.; Farnia, V.; Nasiri, R.F.; Najafi, F. Trazodone in Methandone Induced Erectile Dysfunction. Iran. J. Psychiatry 2010, 5, 164. [Google Scholar]
- van Ahlen, H.; Piechota, H.J.; Kiasa, H.J.; Brennemann’, W.; Klingmiillerb, D. Opiate Antagonists in Erectile Dysfunction: A Possible New Treatment Option? Results of a Pilot Study with Naltrexone. Eur. Urol. 1995, 28, 246–250. [Google Scholar] [CrossRef]
- Billington, C.J.; Shafer, R.B.; Morley, J.E. Effects of Opioid Blockade with Nalmefene in Older Impotent Men. Life Sci. 1990, 47, 799–805. [Google Scholar] [CrossRef]
- Ramdurg, S.; Ambekar, A.; Lal, R. Sexual Dysfunction among Male Patients Receiving Buprenorphine and Naltrexone Maintenance Therapy for Opioid Dependence. J. Sex. Med. 2012, 9, 3198–3204. [Google Scholar] [CrossRef] [PubMed]
- Farnia, V.; Tatari, F.; Alikhani, M.; Yazdchi, K.; Taghizadeh, M.; Sadeghi Bahmani, D.; Karbasizadeh, H.; Holsboer-Trachsler, E.; Brand, S. Rosa Damascena Oil Improved Methadone-Related Sexual Dysfunction in Females with Opioid Use Disorder under Methadone Maintenance Therapy—Results from a Double-Blind, Randomized, and Placebo-Controlled Trial. J. Psychiatr. Res. 2017, 95, 260–268. [Google Scholar] [CrossRef] [PubMed]
- Farnia, V.; Alikhani, M.; Ebrahimi, A.; Golshani, S.; Sadeghi Bahmani, D.; Brand, S. Ginseng Treatment Improves the Sexual Side Effects of Methadone Maintenance Treatment. Psychiatry Res. 2019, 276, 142–150. [Google Scholar] [CrossRef] [PubMed]
- Basson, R.; Wierman, M.E.; van Lankveld, J.; Brotto, L. Summary of the Recommendations on Sexual Dysfunctions in Women. J. Sex. Med. 2010, 7, 314–326. [Google Scholar] [CrossRef]
- McCarthy, B.; McDonald, D. Assessment, Treatment, and Relapse Prevention: Male Hypoactive Sexual Desire Disorder. J. Sex Marital. Ther. 2009, 35, 58–67. [Google Scholar] [CrossRef]
- Stein, A.; Sauder, S.K.; Reale, J. The Role of Physical Therapy in Sexual Health in Men and Women: Evaluation and Treatment. Sex. Med. Rev. 2019, 7, 46–56. [Google Scholar] [CrossRef]
- Schroder, M.A.; Mell, L.K.; Hurteau, J.A.; Collins, Y.C.; Rotmensch, J.; Waggoner, S.E.; Yamada, S.D.; Small, W.; Mundt, A.J. Clitoral Therapy Device for Treatment of Sexual Dysfunction in Irradiated Cervical Cancer Patients. Int. J. Radiat. Oncol. Biol. Phys. 2005, 61, 1078–1086. [Google Scholar] [CrossRef]
- Wassersug, R.; Wibowo, E. Non-Pharmacological and Non-Surgical Strategies to Promote Sexual Recovery for Men with Erectile Dysfunction. Transl. Androl. Urol. 2017, 6, S776–S794. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| 17 Conditions Related to Sexual Health |
|---|
| Sexual dysfunctions |
| HA00 Hypoactive sexual desire dysfunction |
| HA01 Sexual arousal dysfunctions |
| HA02 Orgasmic dysfunctions |
| HA03 Ejaculatory dysfunctions |
| HA0Y Other specified sexual dysfunctions |
| HA0Z Sexual dysfunctions, unspecified |
| Sexual pain disorders |
| HA20 Sexual pain-penetration disorder |
| HA2Y Other specified sexual pain disorders |
| HA2Z Sexual pain disorders, unspecified |
| HA40 Aetiological considerations in sexual dysfunctions and sexual pain disorders |
| HA40.2 Associated with use of psychoactive substance or medication |
| Female Sexual Function Index (FSFI) | International Index of Erectile Function (IIEF) |
|---|---|
| Desire Arousal Lubrication Orgasm Sexual satisfaction Pain | Erectile function Orgasmic function Sexual desire Intercourse satisfaction Overall satisfaction |
| Pharmacological Treatment Options |
|---|
| Testosterone Replacement Therapy Bupropion |
| Trazodone |
| Opioid antagonist (naltrexone, nalmefene) |
| Phosphodiesterase type 5 inhibitors |
| Plant-derived medicines (damask rose oil, ginseng) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salata, B.; Kluczna, A.; Dzierżanowski, T. Opioid-Induced Sexual Dysfunction in Cancer Patients. Cancers 2022, 14, 4046. https://doi.org/10.3390/cancers14164046
Salata B, Kluczna A, Dzierżanowski T. Opioid-Induced Sexual Dysfunction in Cancer Patients. Cancers. 2022; 14(16):4046. https://doi.org/10.3390/cancers14164046
Chicago/Turabian StyleSalata, Bartłomiej, Agnieszka Kluczna, and Tomasz Dzierżanowski. 2022. "Opioid-Induced Sexual Dysfunction in Cancer Patients" Cancers 14, no. 16: 4046. https://doi.org/10.3390/cancers14164046