
PSMA Radioligand Uptake as a Biomarker of Neoangiogenesis in Solid Tumours: Diagnostic or Theragnostic Factor?

 , , , ,
, , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
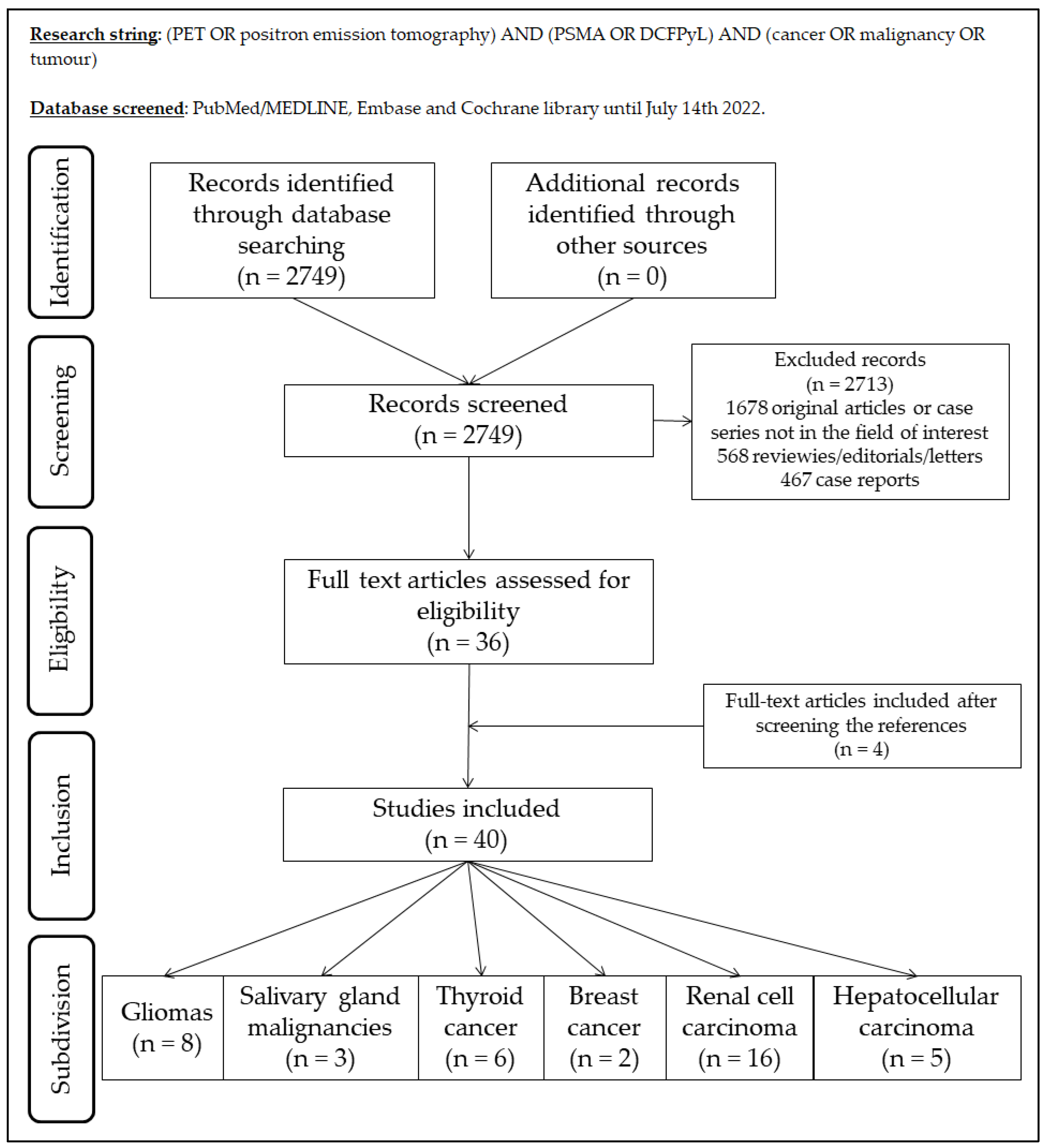
2.1. Search Strategy
2.2. Data Extraction
3. Results
3.1. Gliomas
3.2. Salivary Glands Malignances
3.3. Thyroid Cancer
3.4. Breast Cancer
3.5. Renal Cell Carcinoma
3.6. Hepatocellular Carcinoma
4. Main Findings and Discussion
4.1. General
4.2. Gliomas
4.3. Salivary Gland Malignancies
4.4. Thyroid Cancer
4.5. Breast Cancer
4.6. Renal Cell Carcinoma
4.7. Hepatocellular Carcinoma
4.8. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Farolfi, A.; Calderoni, L.; Mattana, F.; Mei, R.; Telo, S.; Fanti, S.; Castellucci, P. Current and Emerging Clinical Applications of PSMA PET Diagnostic Imaging for Prostate Cancer. J. Nucl. Med. 2021, 62, 596–604. [Google Scholar] [CrossRef] [PubMed]
- Wester, H.-J.; Schottelius, M. PSMA-Targeted Radiopharmaceuticals for Imaging and Therapy. Semin. Nucl. Med. 2019, 49, 302–312. [Google Scholar] [CrossRef] [PubMed]
- Horoszewicz, J.S.; Kawinski, E.; Murphy, G.P. Monoclonal antibodies to a new antigenic marker in epithelial prostatic cells and serum of prostatic cancer patients. Anticancer Res. 1987, 7, 927–935. [Google Scholar] [PubMed]
- Israeli, R.S.; Powell, C.T.; Fair, W.R.; Heston, W.D. Molecular cloning of a complementary DNA encoding a prostate-specific membrane antigen. Cancer Res. 1993, 53, 227–230. [Google Scholar]
- Silver, D.A.; Pellicer, I.; Fair, W.R.; Heston, W.D.; Cordon-Cardo, C. Prostate-specific membrane antigen expression in normal and malignant human tissues. Clin. Cancer Res. 1997, 3, 81–85. [Google Scholar] [PubMed]
- Chang, S.S.; O’Keefe, D.S.; Bacich, D.J.; Reuter, V.E.; Heston, W.D.; Gaudin, P.B. Prostate-specific membrane antigen is pro-duced in tumor-associated neovasculature. Clin. Cancer Res. 1999, 5, 2674–2681. [Google Scholar]
- Conway, R.E.; Petrovic, N.; Li, Z.; Heston, W.; Wu, D.; Shapiro, L.H. Prostate-Specific Membrane Antigen Regulates Angiogenesis by Modulating Integrin Signal Transduction. Mol. Cell. Biol. 2006, 26, 5310–5324. [Google Scholar] [CrossRef] [Green Version]
- Conway, R.E.; Rojas, C.; Alt, J.; Nováková, Z.; Richardson, S.M.; Rodrick, T.C.; Fuentes, J.L.; Richardson, N.; Attalla, J.; Stewart, S.; et al. Prostate-specific membrane antigen (PSMA)-mediated laminin proteolysis generates a pro-angiogenic peptide. Angiogenesis 2016, 19, 487–500. [Google Scholar] [CrossRef]
- Kozikowski, A.P.; Nan, F.; Conti, P.; Zhang, J.; Ramadan, E.; Bzdega, T.; Wroblewska, B.; Neale, J.H.; Pshenichkin, S.; Wroblewski, J.T. Design of Remarkably Simple, Yet Potent Urea-Based Inhibitors of Glutamate Carboxypeptidase II (NAALADase). J. Med. Chem. 2001, 44, 298–301. [Google Scholar] [CrossRef]
- Eder, M.; Schäfer, M.; Bauder-Wüst, U.; Hull, W.-E.; Wängler, C.; Mier, W.; Haberkorn, U.; Eisenhut, M. 68Ga-Complex Lipophilicity and the Targeting Property of a Urea-Based PSMA Inhibitor for PET Imaging. Bioconjug. Chem. 2012, 23, 688–697. [Google Scholar] [CrossRef]
- Afshar-Oromieh, A.; Haberkorn, U.; Eder, M.; Eisenhut, M.; Zechmann, C.M. [68Ga]Gallium-labelled PSMA ligand as superior PET tracer for the diagnosis of prostate cancer: Comparison with 18F-FECH. Eur. J. Pediatr. 2012, 39, 1085–1086. [Google Scholar] [CrossRef] [PubMed]
- Afshar-Oromieh, A.; Malcher, A.; Eder, M.; Eisenhut, M.; Linhart, H.G.; Hadaschik, B.A.; Holland-Letz, T.; Giesel, F.L.; Kratochwil, C.; Haufe, S.; et al. PET imaging with a [68Ga]gallium-labelled PSMA ligand for the diagnosis of prostate cancer: Biodistribution in humans and first evaluation of tumour lesions. Eur. J. Pediatr. 2013, 40, 486–495. [Google Scholar] [CrossRef] [PubMed]
- Rathke, H.; Flechsig, P.; Mier, W.; Bronzel, M.; Mavriopoulou, E.; Hohenfellner, M.; Giesel, F.L.; Haberkorn, U.L.; Kratochwil, C.; Roehrich, M. Dosimetry Estimate and Initial Clinical Experience with 90Y-PSMA-617. J. Nucl. Med. 2019, 60, 806–811. [Google Scholar] [CrossRef] [Green Version]
- Wang, Z.; Jacobson, O.; Tian, R.; Mease, R.C.; Kiesewetter, D.O.; Niu, G.; Pomper, M.G.; Chen, X. Radioligand Therapy of Prostate Cancer with a Long-Lasting Prostate-Specific Membrane Antigen Targeting Agent 90Y-DOTA-EB-MCG. Bioconjug. Chem. 2018, 29, 2309–2315. [Google Scholar] [CrossRef]
- Kratochwil, C.; Bruchertseifer, F.; Giesel, F.L.; Weis, M.; Verburg, F.A.; Mottaghy, F.; Kopka, K.; Apostolidis, C.; Haberkorn, U.; Morgenstern, A. 225Ac-PSMA-617 for PSMA-Targeted α-Radiation Therapy of Metastatic Castration-Resistant Prostate Cancer. J. Nucl. Med. 2016, 57, 1941–1944. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kratochwil, C.; Bruchertseifer, F.; Rathke, H.; Bronzel, M.; Apostolidis, C.; Weichert, W.; Haberkorn, U.; Giesel, F.L.; Morgenstern, A. Targeted α-Therapy of Metastatic Castration-Resistant Prostate Cancer with 225Ac-PSMA-617: Dosimetry Estimate and Empiric Dose Finding. J. Nucl. Med. 2017, 58, 1624–1631. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.; Pullambhatla, M.; Foss, C.A.; Byun, Y.; Nimmagadda, S.; Senthamizhchelvan, S.; Sgouros, G.; Mease, R.C.; Pomper, M.G. 2-(3-{1-Carboxy-5-[(6-[18F]Fluoro-Pyridine-3-Carbonyl)-Amino]-Pentyl}-Ureido)-Pentanedioic Acid, [18F]DCFPyL, a PSMA-Based PET Imaging Agent for Prostate Cancer. Clin. Cancer Res. 2011, 17, 7645–7653. [Google Scholar] [CrossRef] [Green Version]
- Cardinale, J.; Schäfer, M.; Benešová, M.; Bauder-Wüst, U.; Leotta, K.; Eder, M.; Neels, O.C.; Haberkorn, U.; Giesel, F.L.; Kopka, K. Preclinical Evaluation of 18F-PSMA-1007, a New Prostate-Specific Membrane Antigen Ligand for Prostate Cancer Imaging. J. Nucl. Med. 2017, 58, 425–431. [Google Scholar] [CrossRef] [Green Version]
- Giesel, F.L.; Will, L.; Lawal, I.; Lengana, T.; Kratochwil, C.; Vorster, M.; Neels, O.; Reyneke, F.; Haberkon, U.; Kopka, K.; et al. Intraindividual Comparison of 18F-PSMA-1007 and 18F-DCFPyL PET/CT in the Prospective Evaluation of Patients with Newly Diagnosed Prostate Carcinoma: A Pilot Study. J. Nucl. Med. 2018, 59, 1076–1080. [Google Scholar] [CrossRef] [Green Version]
- FDA. FDA Approves First PSMA-Targeted PET Drug. J. Nucl. Med. 2021, 62, 11N. [Google Scholar]
- FDA. FDA Approves 18F-DCFPyL PET Agent in Prostate Cancer. J. Nucl. Med. 2021, 62, 11N. [Google Scholar]
- Sartor, O.; de Bono, J.; Chi, K.N.; Fizazi, K.; Herrmann, K.; Rahbar, K.; Tagawa, S.T.; Nordquist, L.T.; Vaishampayan, N.; El-Haddad, G.; et al. Lutetium-177–PSMA-617 for Metastatic Castration-Resistant Prostate Cancer. N. Engl. J. Med. 2021, 385, 1091–1103. [Google Scholar] [CrossRef] [PubMed]
- FDA. FDA Approves Pluvicto/Locametz for Metastatic Castration-Resistant Prostate Cancer. J. Nucl. Med. 2022, 63, 13N. [Google Scholar]
- Alsultan, A.A.; Barentsz, M.W.; Smits, M.L.; Koopman, M.; Lam, M.G.; Rosenbaum, C.E. Angiogenesis in 90Y-Radioembolization of Colorectal Liver Metastases. Semin. Nucl. Med. 2019, 49, 204–210. [Google Scholar] [CrossRef] [PubMed]
- Folkman, J. Tumor angiogenesis: Therapeutic implications. N. Engl. J. Med. 1971, 285, 1182–1186. [Google Scholar] [CrossRef]
- Ronca, R.; Benkheil, M.; Mitola, S.; Struyf, S.; Liekens, S. Tumor angiogenesis revisited: Regulators and clinical implications. Med. Res. Rev. 2017, 37, 1231–1274. [Google Scholar] [CrossRef] [Green Version]
- Jain, R.K. Antiangiogenesis Strategies Revisited: From Starving Tumors to Alleviating Hypoxia. Cancer Cell 2014, 26, 605–622. [Google Scholar] [CrossRef] [Green Version]
- Carmeliet, P.; Jain, R.K. Principles and mechanisms of vessel normalization for cancer and other angiogenic diseases. Nat. Rev. Drug Discov. 2011, 10, 417–427. [Google Scholar] [CrossRef]
- Sasikumar, A.; Joy, A.; Pillai, M.R.A.; Nanabala, R.; Jayaprakash, P.G.; Madhavan, J.; Nair, S. Diagnostic Value of 68Ga PSMA-11 PET/CT Imaging of Brain Tumors—Preliminary Analysis. Clin. Nucl. Med. 2017, 42, e41–e48. [Google Scholar] [CrossRef]
- Sasikumar, A.; Kashyap, R.; Joy, A.; Patro, K.C.; Bhattacharya, P.; Pilaka, V.K.R.; Oommen, K.E.; Pillai, M.R.A. Utility of 68Ga-PSMA-11 PET/CT in Imaging of Glioma—A Pilot Study. Clin. Nucl. Med. 2018, 43, e304–e309. [Google Scholar] [CrossRef]
- Verma, P.; Malhotra, G.; Goel, A.; Rakshit, S.; Chandak, A.; Chedda, R.; Banerjee, S.; Asopa, R.V. Differential Uptake of 68Ga-PSMA-HBED-CC (PSMA-11) in Low-Grade Versus High-Grade Gliomas in Treatment-Naive Patients. Clin. Nucl. Med. 2019, 44, e318–e322. [Google Scholar] [CrossRef] [PubMed]
- Akgun, E.; Akgun, M.Y.; Selçuk, H.H.; Uzan, M.; Sayman, H.B. 68Ga PSMA PET/MR in the differentiation of low and high grade gliomas: Is 68Ga PSMA PET/MRI useful to detect brain gliomas? Eur. J. Radiol. 2020, 130, 109199. [Google Scholar] [CrossRef] [PubMed]
- Kunikowska, J.; Kuliński, R.; Muylle, K.; Koziara, H.; Królicki, L. 68Ga-Prostate-Specific Membrane Antigen-11 PET/CT: A New Imaging Option for Recurrent Glioblastoma Multiforme? Clin. Nucl. Med. 2020, 45, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; ArunRaj, S.T.; Bhullar, K.; Haresh, K.P.; Gupta, S.; Ballal, S.; Yadav, M.; Singh, M.; Damle, N.A.; Garg, A.; et al. Ga-68 PSMA PET/CT in recurrent high-grade gliomas: Evaluating PSMA expression in vivo. Neuroradiology 2022, 64, 969–979. [Google Scholar] [CrossRef]
- Liu, D.; Cheng, G.; Ma, X.; Wang, S.; Zhao, X.; Zhang, W.; Yang, W.; Wang, J. PET/CT using 68Ga-PSMA-617 versus 18F-fluorodeoxyglucose to differentiate low- and high-grade gliomas. J. Neuroimaging 2021, 31, 733–742. [Google Scholar] [CrossRef]
- Kunikowska, J.; Czepczyński, R.; Pawlak, D.; Koziara, H.; Pełka, K.; Królicki, L. Expression of glutamate carboxypeptidase II in the glial tumor recurrence evaluated in vivo using radionuclide imaging. Sci. Rep. 2022, 12, 652. [Google Scholar] [CrossRef]
- Nulent, T.J.W.K.; Van Es, R.J.J.; Krijger, G.C.; De Bree, R.; Willems, S.M.; de Keizer, B. Prostate-specific membrane antigen PET imaging and immunohistochemistry in adenoid cystic carcinoma—A preliminary analysis. Eur. J. Pediatr. 2017, 44, 1614–1621. [Google Scholar] [CrossRef]
- van Boxtel, W.; Lütje, S.; Grunsven, I.C.V.E.-V.; Verhaegh, G.W.; Schalken, J.A.; Jonker, M.A.; Nagarajah, J.; Gotthardt, M.; van Herpen, C.M. 68Ga-PSMA-HBED-CC PET/CT imaging for adenoid cystic carcinoma and salivary duct carcinoma: A phase 2 imaging study. Theranostics 2020, 10, 2273–2283. [Google Scholar] [CrossRef]
- Nulent, T.J.W.K.; van Es, R.J.J.; Willems, S.M.; Braat, A.J.A.T.; Devriese, L.A.; de Bree, R.; de Keizer, B. First experiences with 177Lu-PSMA-617 therapy for recurrent or metastatic salivary gland cancer. EJNMMI Res. 2021, 11, 126. [Google Scholar] [CrossRef]
- Lütje, S.; Gomez, B.; Cohnen, J.; Umutlu, L.; Gotthardt, M.; Poeppel, T.D.; Bockisch, A.; Rosenbaum-Krumme, S. Imaging of Prostate-Specific Membrane Antigen Expression in Metastatic Differentiated Thyroid Cancer Using 68Ga-HBED-CC-PSMA PET/CT. Clin. Nucl. Med. 2017, 42, 20–25. [Google Scholar] [CrossRef]
- De Vries, L.H.; Lodewijk, L.; Braat, A.J.A.T.; Krijger, G.C.; Valk, G.D.; Lam, M.G.E.H.; Rinkes, I.H.M.B.; Vriens, M.R.; De Keizer, B. 68Ga-PSMA PET/CT in radioactive iodine-refractory differentiated thyroid cancer and first treatment results with 177Lu-PSMA-617. EJNMMI Res. 2020, 10, 18. [Google Scholar] [CrossRef] [PubMed]
- Lawhn-Heath, C.; Yom, S.S.; Liu, C.; Villanueva-Meyer, J.E.; Aslam, M.; Smith, R.; Narwal, M.; Juarez, R.; Behr, S.C.; Pampaloni, M.H.; et al. Gallium-68 prostate-specific membrane antigen ([68Ga]Ga-PSMA-11) PET for imaging of thyroid cancer: A feasibility study. EJNMMI Res. 2020, 10, 128. [Google Scholar] [CrossRef] [PubMed]
- Verma, P.; Malhotra, G.; Meshram, V.; Chandak, A.; Sonavane, S.; Lila, A.R.; Bandgar, T.R.; Asopa, R.V. Prostate-Specific Membrane Antigen Expression in Patients With Differentiated Thyroid Cancer With Thyroglobulin Elevation and Negative Iodine Scintigraphy Using 68Ga-PSMA-HBED-CC PET/CT. Clin. Nucl. Med. 2021, 46, e406–e409. [Google Scholar] [CrossRef] [PubMed]
- Pitalua-Cortes, Q.; García-Perez, F.O.; Vargas-Ahumada, J.; Gonzalez-Rueda, S.; Gomez-Argumosa, E.; Ignacio-Alvarez, E.; Soldevilla-Gallardo, I.; Torres-Agredo, L. Head-to-Head Comparison of 68Ga-PSMA-11 and 131I in the Follow-Up of Well-Differentiated Metastatic Thyroid Cancer: A New Potential Theragnostic Agent. Front. Endocrinol. 2021, 12, 794759. [Google Scholar] [CrossRef]
- Santhanam, P.; Russell, J.; Rooper, L.M.; Ladenson, P.W.; Pomper, M.G.; Rowe, S.P. The prostate-specific membrane antigen (PSMA)-targeted radiotracer 18F-DCFPyL detects tumor neovasculature in metastatic, advanced, radioiodine-refractory, differentiated thyroid cancer. Med. Oncol. 2020, 37, 98. [Google Scholar] [CrossRef] [PubMed]
- Sathekge, M.; Lengana, T.; Modiselle, M.; Vorster, M.; Zeevaart, J.; Maes, A.; Ebenhan, T.; Van De Wiele, C. 68Ga-PSMA-HBED-CC PET imaging in breast carcinoma patients. Eur. J. Pediatr. 2017, 44, 689–694. [Google Scholar] [CrossRef]
- Medina-Ornelas, S.; García-Perez, F.; Estrada-Lobato, E.; Ochoa-Carrillo, F. 68Ga-PSMA PET/CT in the Evaluation of Locally Advanced and Metastatic Breast Cancer, a Single Center Experience. Am. J. Nucl. Med. Mol. Imaging 2020, 10, 135–142. [Google Scholar]
- Rowe, S.P.; Gorin, M.A.; Hammers, H.J.; Javadi, M.S.; Hawasli, H.; Szabo, Z.; Cho, S.Y.; Pomper, M.G.; Allaf, M.E. Imaging of metastatic clear cell renal cell carcinoma with PSMA-targeted 18F-DCFPyL PET/CT. Ann. Nucl. Med. 2015, 29, 877–882. [Google Scholar] [CrossRef] [Green Version]
- Rhee, H.; Blazak, J.; Tham, C.M.; Ng, K.L.; Shepherd, B.; Lawson, M.; Preston, J.; Vela, I.; Thomas, P.; Wood, S. Pilot study: Use of gallium-68 PSMA PET for detection of metastatic lesions in patients with renal tumour. EJNMMI Res. 2016, 6, 76. [Google Scholar] [CrossRef]
- Sawicki, L.M.; Buchbender, C.; Boos, J.; Giessing, M.; Ermert, J.; Antke, C.; Antoch, G.; Hautzel, H. Diagnostic potential of PET/CT using a 68Ga-labelled prostate-specific membrane antigen ligand in whole-body staging of renal cell carcinoma: Initial experience. Eur. J. Pediatr. 2017, 44, 102–107. [Google Scholar] [CrossRef]
- Siva, S.; Callahan, J.; Pryor, D.; Martin, J.; Lawrentschuk, N.; Hofman, M.S. Utility of 68Ga prostate specific membrane antigen—Positron emission tomography in diagnosis and response assessment of recurrent renal cell carcinoma. J. Med. Imaging Radiat. Oncol. 2017, 61, 372–378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yin, Y.; Campbell, S.P.; Markowski, M.C.; Pierorazio, P.M.; Pomper, M.G.; Allaf, M.E.; Rowe, S.P.; Gorin, M.A. Inconsistent Detection of Sites of Metastatic Non-Clear Cell Renal Cell Carcinoma with PSMA-Targeted [18F]DCFPyL PET/CT. Mol. Imaging Biol. 2019, 21, 567–573. [Google Scholar] [CrossRef] [PubMed]
- Meyer, A.R.; Carducci, M.A.; Denmeade, S.R.; Markowski, M.C.; Pomper, M.G.; Pierorazio, P.M.; Allaf, M.E.; Rowe, S.P.; Gorin, M.A. Improved identification of patients with oligometastatic clear cell renal cell carcinoma with PSMA-targeted 18F-DCFPyL PET/CT. Ann. Nucl. Med. 2019, 33, 617–623. [Google Scholar] [CrossRef] [PubMed]
- Raveenthiran, S.; Esler, R.; Yaxley, J.; Kyle, S. The use of 68Ga-PET/CT PSMA in the staging of primary and suspected recurrent renal cell carcinoma. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 2280–2288. [Google Scholar] [CrossRef] [PubMed]
- Gao, J.; Xu, Q.; Fu, Y.; He, K.; Zhang, C.; Zhang, Q.; Shi, J.; Zhao, X.; Wang, F.; Guo, H. Comprehensive evaluation of 68Ga-PSMA-11 PET/CT parameters for discriminating pathological characteristics in primary clear-cell renal cell carcinoma. Eur. J. Pediatr. 2021, 48, 561–569. [Google Scholar] [CrossRef]
- Liu, Y.; Wang, G.; Yu, H.; Wu, Y.; Lin, M.; Gao, J.; Xu, B. Comparison of 18F-DCFPyL and 18F-FDG PET/computed tomography for the restaging of clear cell renal cell carcinoma: Preliminary results of 15 patients. Nucl. Med. Commun. 2020, 41, 1299–1305. [Google Scholar] [CrossRef]
- Gühne, F.; Seifert, P.; Theis, B.; Steinert, M.; Freesmeyer, M.; Drescher, R. PSMA-PET/CT in Patients with Recurrent Clear Cell Renal Cell Carcinoma: Histopathological Correlations of Imaging Findings. Diagnostics 2021, 11, 1142. [Google Scholar] [CrossRef]
- Mittlmeier, L.M.; Unterrainer, M.; Rodler, S.; Todica, A.; Albert, N.L.; Burgard, C.; Cyran, C.C.; Kunz, W.G.; Ricke, J.; Bartenstein, P.; et al. 18F-PSMA-1007 PET/CT for response assessment in patients with metastatic renal cell carcinoma undergoing tyrosine kinase or checkpoint inhibitor therapy: Preliminary results. Eur. J. Pediatr. 2021, 48, 2031–2037. [Google Scholar] [CrossRef]
- Golan, S.; Aviv, T.; Groshar, D.; Yakimov, M.; Zohar, Y.; Prokocimer, Y.; Nadu, A.; Baniel, J.; Domachevsky, L.; Bernstine, H. Dynamic 68Ga-PSMA-11 PET/CT for the Primary Evaluation of Localized Renal Mass: A Prospective Study. J. Nucl. Med. 2021, 62, 773–778. [Google Scholar] [CrossRef]
- Gao, J.; Meng, L.; Xu, Q.; Zhao, X.; Deng, Y.; Fu, Y.; Guo, S.; He, K.; Shi, J.; Wang, F.; et al. 68Ga-PSMA-11 PET/CT Parameter Correlates with Pathological VEGFR-2/PDGFR-β Expression in Renal Cell Carcinoma Patients. Mol. Imaging Biol. 2022. [Google Scholar] [CrossRef]
- Li, Y.; Zheng, R.; Zhang, Y.; Huang, C.; Tian, L.; Liu, R.; Liu, Y.; Zhang, Z.; Han, H.; Zhou, F.; et al. Special issue “the advance of solid tumor research in China”: 68Ga-PSMA-11 PET/CT for evaluating primary and metastatic lesions in different histological subtypes of renal cell carcinoma. Int. J. Cancer 2022, ijc.34189. [Google Scholar] [CrossRef] [PubMed]
- Meng, L.; Zhang, S.; Gao, J.; Xu, Q.; Fu, Y.; Zhou, Y.-H.; Wang, F.; Guo, H. [68Ga]Ga-PSMA-11 PET/CT has potential application in predicting tumor HIF-2α expression and therapeutic response to HIF-2α antagonists in patients with RCC. Eur. Radiol. 2022, 32, 6545–6553. [Google Scholar] [CrossRef] [PubMed]
- Tariq, A.; Kwok, M.; Pearce, A.; Rhee, H.; Kyle, S.; Marsh, P.; Raveenthiran, S.; Wong, D.; McBean, R.; Westera, J.; et al. The role of dual tracer PSMA and FDG PET/CT in renal cell carcinoma (RCC) compared to conventional imaging: A multi-institutional case series with intra-individual comparison. Urol. Oncol. Semin. Orig. Investig. 2021, 40, 66.e1–66.e9. [Google Scholar] [CrossRef]
- Kesler, M.; Levine, C.; Hershkovitz, D.; Mishani, E.; Menachem, Y.; Lerman, H.; Zohar, Y.; Shibolet, O.; Even-Sapir, E. 68Ga-Labeled Prostate-Specific Membrane Antigen Is a Novel PET/CT Tracer for Imaging of Hepatocellular Carcinoma: A Prospective Pilot Study. J. Nucl. Med. 2019, 60, 185–191. [Google Scholar] [CrossRef] [Green Version]
- Kunikowska, J.; Cieślak, B.; Gierej, B.; Patkowski, W.; Kraj, L.; Kotulski, M.; Zieniewicz, K.; Królicki, L. [68Ga]Ga-Prostate-Specific Membrane Antigen PET/CT: A novel method for imaging patients with hepatocellular carcinoma. Eur. J. Pediatr. 2021, 48, 883–892. [Google Scholar] [CrossRef]
- Gündoğan, C.; Ergül, N.; Çakır, M.S.; Kılıçkesmez, Ö.; Gürsu, R.U.; Aksoy, T.; Çermik, T.F. 68Ga-PSMA PET/CT Versus 18F-FDG PET/CT for Imaging of Hepatocellular Carcinoma. Mol. Imaging Radionucl. Ther. 2021, 30, 79–85. [Google Scholar] [CrossRef] [PubMed]
- Hirmas, N.; Leyh, C.; Sraieb, M.; Barbato, F.; Schaarschmidt, B.M.; Umutlu, L.; Nader, M.; Wedemeyer, H.; Ferdinandus, J.; Rischpler, C.; et al. 68Ga-PSMA-11 PET/CT Improves Tumor Detection and Impacts Management in Patients with Hepatocellular Carcinoma. J. Nucl. Med. 2021, 62, 1235–1241. [Google Scholar] [CrossRef]
- Thompson, S.M.; Suman, G.; Torbenson, M.S.; Chen, Z.E.; Jondal, D.E.; Patra, A.; Ehman, E.C.; Andrews, J.C.; Fleming, C.J.; Welch, B.T.; et al. PSMA as a Theranostic Target in Hepatocellular Carcinoma: Immunohistochemistry and 68Ga-PSMA-11 PET Using Cyclotron-Produced 68Ga. Hepatol. Commun. 2021, 6, 1172–1185. [Google Scholar] [CrossRef]
- Li, T.; Kang, G.; Wang, T.; Huang, H. Tumor angiogenesis and anti-angiogenic gene therapy for cancer (Review). Oncol. Lett. 2018, 16, 687–702. [Google Scholar] [CrossRef] [Green Version]
- Evangelista, L.; Maurer, T.; van der Poel, H.; Alongi, F.; Kunikowska, J.; Laudicella, R.; Fanti, S.; Hofman, M.S. [68Ga]Ga-PSMA Versus [18F]PSMA Positron Emission Tomography/Computed Tomography in the Staging of Primary and Recurrent Prostate Cancer. A Systematic Review of the Literature. Eur. Urol. Oncol. 2022, 5, 273–282. [Google Scholar] [CrossRef]
- Giesel, F.L.; Hadaschik, B.; Cardinale, J.; Radtke, J.; Vinsensia, M.; Lehnert, W.; Kesch, C.; Tolstov, Y.; Singer, S.; Grabe, N.; et al. F-18 labelled PSMA-1007: Biodistribution, radiation dosimetry and histopathological validation of tumor lesions in prostate cancer patients. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 678–688. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vollnberg, B.; Alberts, I.; Genitsch, V.; Rominger, A.; Afshar-Oromieh, A. Assessment of malignancy and PSMA expression of uncertain bone foci in [18F]PSMA-1007 PET/CT for prostate cancer—A single-centre experience of PET-guided biopsies. Eur. J. Pediatr. 2022. [Google Scholar] [CrossRef]
- Alberts, I.; Bütikofer, L.; Rominger, A.; Afshar-Oromieh, A. A randomised, prospective and head-to-head comparison of [68Ga]Ga-PSMA-11 and [18F]PSMA-1007 for the detection of recurrent prostate cancer in PSMA-ligand PET/CT—Protocol design and rationale. PLoS ONE 2022, 17, e0270269. [Google Scholar] [CrossRef] [PubMed]
- Francis, S.S.; Ostrom, Q.T.; Cote, D.J.; Smith, T.R.; Claus, E.; Barnholtz-Sloan, J.S. The Epidemiology of Central Nervous System Tumors. Hematol. Clin. N. Am. 2022, 36, 23–42. [Google Scholar] [CrossRef] [PubMed]
- Weller, M.; van den Bent, M.; Preusser, M.; Le Rhun, E.; Tonn, J.C.; Minniti, G.; Bendszus, M.; Balana, C.; Chinot, O.; Dirven, L.; et al. EANO guidelines on the diagnosis and treatment of diffuse gliomas of adulthood. Nat. Rev. Clin. Oncol. 2020, 18, 170–186. [Google Scholar] [CrossRef]
- Komori, T. Grading of adult diffuse gliomas according to the 2021 WHO Classification of Tumors of the Central Nervous System. Lab. Investig. 2022, 102, 126–133. [Google Scholar] [CrossRef]
- Zhou, Q.; Xue, C.; Ke, X.; Zhou, J. Treatment Response and Prognosis Evaluation in High-Grade Glioma: An Imaging Review Based on MRI. J. Magn. Reson. Imaging 2022, 56, 325–340. [Google Scholar] [CrossRef]
- Treglia, G.; Muoio, B.; Trevisi, G.; Mattoli, M.V.; Albano, D.; Bertagna, F.; Giovanella, L. Diagnostic Performance and Prognostic Value of PET/CT with Different Tracers for Brain Tumors: A Systematic Review of Published Meta-Analyses. Int. J. Mol. Sci. 2019, 20, 4669. [Google Scholar] [CrossRef] [Green Version]
- Traub-Weidinger, T.; Poetsch, N.; Woehrer, A.; Klebermass, E.-M.; Bachnik, T.; Preusser, M.; Mischkulnig, M.; Kiesel, B.; Widhalm, G.; Mitterhauser, M.; et al. PSMA Expression in 122 Treatment Naive Glioma Patients Related to Tumor Metabolism in 11C-Methionine PET and Survival. J. Pers. Med. 2021, 11, 624. [Google Scholar] [CrossRef]
- Coca-Pelaz, A.; Rodrigo, J.P.; Bradley, P.J.; Poorten, V.V.; Triantafyllou, A.; Hunt, J.L.; Strojan, P.; Rinaldo, A.; Haigentz, M.; Takes, R.P.; et al. Adenoid cystic carcinoma of the head and neck—An update. Oral Oncol. 2015, 51, 652–661. [Google Scholar] [CrossRef]
- Bjørndal, K.; Krogdahl, A.; Therkildsen, M.H.; Overgaard, J.; Johansen, J.; Kristensen, C.A.; Homøe, P.; Sørensen, C.H.; Andersen, E.; Bundgaard, T.; et al. Salivary gland carcinoma in Denmark 1990–2005: A national study of incidence, site and histology. Results of the Danish Head and Neck Cancer Group (DAHANCA). Oral Oncol. 2011, 47, 677–682. [Google Scholar] [CrossRef]
- Laurie, S.A.; Ho, A.L.; Fury, M.G.; Sherman, E.; Pfister, D.G. Systemic therapy in the management of metastatic or locally recurrent adenoid cystic carcinoma of the salivary glands: A systematic review. Lancet Oncol. 2011, 12, 815–824. [Google Scholar] [CrossRef]
- Alfieri, S.; Granata, R.; Bergamini, C.; Resteghini, C.; Bossi, P.; Licitra, L.; Locati, L.D. Systemic therapy in metastatic salivary gland carcinomas: A pathology-driven paradigm? Oral Oncol. 2017, 66, 58–63. [Google Scholar] [CrossRef]
- Freling, N.; Crippa, F.; Maroldi, R. Staging and follow-up of high-grade malignant salivary gland tumours: The role of traditional versus functional imaging approaches—A review. Oral Oncol. 2016, 60, 157–166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prasad, V.; Steffen, I.G.; Diederichs, G.; Makowski, M.R.; Wust, P.; Brenner, W. Biodistribution of [(68)Ga]PSMA-HBED-CC in Patients with Prostate Cancer: Characterization of Uptake in Normal Organs and Tumour Lesions. Mol. Imaging Biol. 2016, 18, 428–436. [Google Scholar] [CrossRef]
- Rupp, N.J.; Umbricht, C.A.; Pizzuto, D.A.; Lenggenhager, D.; Töpfer, A.; Müller, J.; Muehlematter, U.J.; Ferraro, D.A.; Messerli, M.; Morand, G.B.; et al. First Clinicopathologic Evidence of a Non-PSMA-Related Uptake Mechanism for 68Ga-PSMA-11 in Salivary Glands. J. Nucl. Med. 2019, 60, 1270–1276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tönnesmann, R.; Meyer, P.T.; Eder, M.; Baranski, A.-C. [177Lu]Lu-PSMA-617 Salivary Gland Uptake Characterized by Quantitative In Vitro Autoradiography. Pharmaceuticals 2019, 12, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pandit-Taskar, N.; O’Donoghue, J.A.; Morris, M.J.; Wills, E.A.; Schwartz, L.H.; Gonen, M.; Scher, H.I.; Larson, S.M.; Divgi, C.R. Antibody Mass Escalation Study in Patients with Castration-Resistant Prostate Cancer Using 111In-J591: Lesion Detectability and Dosimetric Projections for 90Y Radioimmunotherapy. J. Nucl. Med. 2008, 49, 1066–1074. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haugen, B.R.; Alexander, E.K.; Bible, K.C.; Doherty, G.M.; Mandel, S.J.; Nikiforov, Y.E.; Pacini, F.; Randolph, G.W.; Sawka, A.M.; Schlumberger, M.; et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 2016, 26, 1–133. [Google Scholar] [CrossRef] [Green Version]
- Salvatori, M.; Biondi, B.; Rufini, V. Imaging in Endocrinology: 2-[18F]-fluoro-2-deoxy-D-glucose positron emission tomography/computed tomography in differentiated thyroid carcinoma: Clinical indications and controversies in diagnosis and follow-up. Eur. J. Endocrinol. 2015, 173, R115–R130. [Google Scholar] [CrossRef] [Green Version]
- Rizzo, A.; Perotti, G.; Zagaria, L.; Lanni, V.; Racca, M.; Palestini, N.; Salvatori, M. 18F-FDG PET/CT concurrent with first radioiodine post-therapeutic scan in high risk differentiated thyroid cancer: A useful tool or just an expensive diversion? Q. J. Nucl. Med. Mol. Imaging 2022. [Google Scholar] [CrossRef] [PubMed]
- Moore, M.; Panjwani, S.; Mathew, R.; Crowley, M.; Liu, Y.-F.; Aronova, A.; Finnerty, B.; Zarnegar, R.; Fahey, T.J.; Scognamiglio, T. Well-Differentiated Thyroid Cancer Neovasculature Expresses Prostate-Specific Membrane Antigen—A Possible Novel Therapeutic Target. Endocr. Pathol. 2017, 28, 339–344. [Google Scholar] [CrossRef] [PubMed]
- Sollini, M.; Di Tommaso, L.; Kirienko, M.; Piombo, C.; Erreni, M.; Lania, A.G.; Erba, P.A.; Antunovic, L.; Chiti, A. PSMA expression level predicts differentiated thyroid cancer aggressiveness and patient outcome. EJNMMI Res. 2019, 9, 93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schlumberger, M.; Tahara, M.; Wirth, L.J.; Robinson, B.; Brose, M.S.; Elisei, R.; Habra, M.A.; Newbold, K.; Shah, M.H.; Hoff, A.O.; et al. Lenvatinib versus Placebo in Radioiodine-Refractory Thyroid Cancer. N. Engl. J. Med. 2015, 372, 621–630. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Perou, C.M.; Sørlie, T.; Eisen, M.B.; Van De Rijn, M.; Jeffrey, S.S.; Rees, C.A.; Pollack, J.R.; Ross, D.T.; Johnsen, H.; Akslen, L.A.; et al. Molecular portraits of human breast tumours. Nature 2000, 406, 747–752. [Google Scholar] [CrossRef]
- Loibl, S.; Gianni, L. HER2-positive breast cancer. Lancet 2016, 389, 2415–2429. [Google Scholar] [CrossRef]
- Burguin, A.; Diorio, C.; Durocher, F. Breast Cancer Treatments: Updates and New Challenges. J. Pers. Med. 2021, 11, 808. [Google Scholar] [CrossRef]
- Paydary, K.; Seraj, S.M.; Zadeh, M.Z.; Emamzadehfard, S.; Shamchi, S.P.; Gholami, S.; Werner, T.J.; Alavi, A. The Evolving Role of FDG-PET/CT in the Diagnosis, Staging, and Treatment of Breast Cancer. Mol. Imaging Biol. 2019, 21, 1–10. [Google Scholar] [CrossRef]
- Tolkach, Y.; Gevensleben, H.; Bundschuh, R.; Koyun, A.; Huber, D.; Kehrer, C.; Hecking, T.; Keyver-Paik, M.-D.; Kaiser, C.; Ahmadzadehfar, H.; et al. Prostate-specific membrane antigen in breast cancer: A comprehensive evaluation of expression and a case report of radionuclide therapy. Breast Cancer Res. Treat. 2018, 169, 447–455. [Google Scholar] [CrossRef]
- Capitanio, U.; Bensalah, K.; Bex, A.; Boorjian, S.A.; Bray, F.; Coleman, J.; Gore, J.L.; Sun, M.; Wood, C.; Russo, P. Epidemiology of Renal Cell Carcinoma. Eur. Urol. 2019, 75, 74–84. [Google Scholar] [CrossRef] [PubMed]
- Tung, I.; Sahu, A. Immune Checkpoint Inhibitor in First-Line Treatment of Metastatic Renal Cell Carcinoma: A Review of Current Evidence and Future Directions. Front. Oncol. 2021, 11, 707214. [Google Scholar] [CrossRef] [PubMed]
- Urso, L.; Castello, A.; Rocca, G.C.; Lancia, F.; Panareo, S.; Cittanti, C.; Uccelli, L.; Florimonte, L.; Castellani, M.; Ippolito, C.; et al. Role of PSMA-ligands imaging in Renal Cell Carcinoma management: Current status and future perspectives. J. Cancer Res. Clin. Oncol. 2022, 148, 1299–1311. [Google Scholar] [CrossRef] [PubMed]
- Park, J.W.; Jo, M.K.; Lee, H.M. Significance of 18F-fluorodeoxyglucose positron-emission tomography/computed tomography for the postoperative surveillance of advanced renal cell carcinoma. Br. J. Urol. 2009, 103, 615–619. [Google Scholar] [CrossRef]
- Baccala, A.; Sercia, L.; Li, J.; Heston, W.; Zhou, M. Expression of Prostate-Specific Membrane Antigen in Tumor-Associated Neovasculature of Renal Neoplasms. Urology 2007, 70, 385–390. [Google Scholar] [CrossRef]
- Ristau, B.T.; O’Keefe, D.S.; Bacich, D.J. The prostate-specific membrane antigen: Lessons and current clinical implications from 20 years of research. Urol. Oncol. 2014, 32, 272–279. [Google Scholar] [CrossRef] [Green Version]
- Al-Ahmadie, H.A.; Olgac, S.; Gregor, P.D.; Tickoo, S.K.; Fine, S.W.; Kondagunta, G.V.; Scher, H.I.; Morris, M.J.; Russo, P.; Motzer, R.J.; et al. Expression of prostate-specific membrane antigen in renal cortical tumors. Mod. Pathol. 2008, 21, 727–732. [Google Scholar] [CrossRef] [Green Version]
- Chang, S.S.; Reuter, V.E.; Heston, W.D.W.; Gaudin, P.B. Metastatic renal cell carcinoma neovasculature expresses prostate-specific membrane antigen. Urology 2001, 57, 801–805. [Google Scholar] [CrossRef]
- Kulik, L.; El-Serag, H.B. Epidemiology and Management of Hepatocellular Carcinoma. Gastroenterology 2019, 156, 477–491.e1. [Google Scholar] [CrossRef]
- El-Serag, H.B.; Marrero, J.A.; Rudolph, L.; Reddy, K.R. Diagnosis and Treatment of Hepatocellular Carcinoma. Gastroenterology 2008, 134, 1752–1763. [Google Scholar] [CrossRef] [Green Version]
- Kanmaniraja, D.; Dellacerra, G.; Holder, J.; Erlichman, D.; Chernyak, V. Liver Imaging Reporting and Data System (LI-RADS) v2018: Review of the CT/MRI Diagnostic Categories. Can. Assoc. Radiol. J. 2021, 72, 142–149. [Google Scholar] [CrossRef] [PubMed]
- Asman, Y.; Evenson, A.R.; Even-Sapir, E.; Shibolet, O. [18F]fludeoxyglucose positron emission tomography and computed tomography as a prognostic tool before liver transplantation, resection, and loco-ablative therapies for hepatocellular carcinoma. Liver Transpl. 2015, 21, 572–580. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiao, D.; Li, Y.; Yang, F.; Han, D.; Wu, J.; Shi, S.; Tian, F.; Guo, Z.; Xi, W.; Li, G.; et al. Expression of Prostate-Specific Membrane Antigen in Tumor-Associated Vasculature Predicts Poor Prognosis in Hepatocellular Carcinoma. Clin. Transl. Gastroenterol. 2019, 10, 1–7. [Google Scholar] [CrossRef]
- Tolkach, Y.; Goltz, D.; Kremer, A.; Ahmadzadehfar, H.; Bergheim, D.; Essler, M.; Lam, M.; de Keizer, B.; Fischer, H.-P.; Kristiansen, G. Prostate-specific membrane antigen expression in hepatocellular carcinoma: Potential use for prognosis and diagnostic imaging. Oncotarget 2019, 10, 4149–4160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Llovet, J.M.; Kelley, R.K.; Villanueva, A.; Singal, A.G.; Pikarsky, E.; Roayaie, S.; Lencioni, R.; Koike, K.; Zucman-Rossi, J.; Finn, R.S. Hepatocellular carcinoma. Nat. Rev. Dis. Primers 2021, 7, 6. [Google Scholar] [CrossRef] [PubMed]
- Uijen, M.J.M.; Derks, Y.H.W.; Merkx, R.I.J.; Schilham, M.G.M.; Roosen, J.; Privé, B.M.; van Lith, S.A.M.; van Herpen, C.M.L.; Gotthardt, M.; Heskamp, S.; et al. PSMA radioligand therapy for solid tumors other than prostate cancer: Background, opportunities, challenges, and first clinical reports. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 4350–4368. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| First Author and Year | Type | Country | N. Patients | Tracer | Histopathological Subtype (N. Patients) | Clinical Setting (N. Patients) | Analysed Lesions | Comparator |
|---|---|---|---|---|---|---|---|---|
| Sasikumar 2017 [29] | Not reported | India | 6 | 68Ga-PSMA-11 (I) | 6 high-grade | Initial diagnosis or restaging | 6 | MRI 18F-FDG PET/CT |
| Sasikumar 2018 [30] | Prospective | India | 15 | 68Ga-PSMA-11 (I) | 1 low-grade; 14 high-grade | Initial diagnosis or restaging | 15 | MRI |
| Verma 2019 [31] | Not reported | India | 10 | 68Ga-PSMA-11 (I) | 3 low-grade; 7 high-grade | Initial diagnosis | 10 | MRI 18F-FDG PET/CT |
| Akgun 2020 [32] | Prospective | Turkey | 35 | 68Ga-PSMA-11 (I) | 14 low-grade; 21 high-grade | Initial diagnosis | 35 | MRI |
| Kunikowska 2020 [33] | Not reported | Poland | 15 | 68Ga-PSMA-11 (I) | 15 high-grade | Restaging | 15 | MRI |
| Kumar 2021 [34] | Prospective | India | 33 | 68Ga-PSMA-11 (I) | 33 high-grade | Restaging | 33 | MRI |
| Liu 2021 [35] | Retrospective | China | 30 | 68Ga-PSMA-617(I) | 14 low-grade; 16 high-grade | Initial diagnosis | 30 | MRI 18F-FDG PET/CT |
| Kunikowska 2022 [36] | Not reported | Poland | 34 | 68Ga-PSMA-11 (I) | 34 high-grade | Restaging | 34 | MRI |
| First Author and Year | Type | Country | N. Patients | Tracer | Histopathological Subtype (N. Patients) | Clinical Setting (N. Patients) | Comparator |
|---|---|---|---|---|---|---|---|
| Klein Nulent 2017 [37] | Retrospective | Netherlands | 9 | 68Ga-PSMA-11 (I) | AdCC | Restaging | 18F-FDG PET/CT CT |
| Van Boxtel 2020 [38] | Prospective | Netherlands | 25 | 68Ga-PSMA-11 (I) | 15 AdCC 10 SDC | Restaging | CT |
| Klein Nulent 2021 [39] | Retrospective | Netherlands | 6 | 68Ga-PSMA-11 (I) 177Lu-PSMA-617 (T) | 4 AdCC 1 unclassified adenocarcoma 1 acinic cell carcinoma | Palliative RLT | / |
| First Author and Year | Type | Country | N. Patients | Tracer | Histopathological Subtype (N. Patients) | Clinical Setting | Analysed Lesions | Comparator |
|---|---|---|---|---|---|---|---|---|
| Lütje 2017 [40] | Prospective | Germany | 6 | 68Ga- PSMA-11 (I) | 2 papillary 4 follicular | Radioiodine refractory TC | 42 | 18F-FDG PET/CT |
| De Vries 2020 [41] | Retrospective | Netherlands | 5 | 68Ga-PSMA-11 (I) 177Lu-PSMA-617 (T) | 4 papillary 1 follicular variant | Radioiodine refractory TC | / | / |
| Lawhn-Heath 2020 [42] | Prospective | USA | 11 | 68Ga- PSMA-11 (I) | 3 papillary 2 follicular 2 Hurthle cell 2 poorly differentiated 2 anaplastic | TC with abnormal uptake on 18F-FDG PET and/or 123I /131I scan | 43 | 18F-FDG PET/CT 123I /131I scan |
| Verma 2021 [43] | Prospective | India | 9 | 68Ga-PSMA-11 (I) | 7 papillary 2 follicular variant | Radioiodine refractory TC | 14 | 18F-FDG PET/CT |
| Pitalua-Cortes 2021 [44] | Retrospective | Mexico | 10 | 68Ga- PSMA-11 (I) | 7 papillary 3 follicular | Radioiodine refractory TC | 64 | 131I scan |
| Santhanam 2021 [45] | Prospective | USA | 2 | 18F-DCFPyl (I) | 1 papillary 1 follicular | Radioiodine refractory TC | 2 | 18F-FDG PET/CT 123I scan |
| First Author and Year | Type | Country | N. Patients | Tracer | Histopathological SubType (N. Patients) | Clinical Setting (N. Patients) | Analysed Lesions | Comparator |
|---|---|---|---|---|---|---|---|---|
| Sathekge 2017 [46] | Prospective | South Africa | 19 | 68Ga-PSMA-11 (I) | 13 ductal 2 lobular 1 neuroendocrine differentiation 3 unknown | 9 staging 5 restaging for local recurrence 5 restaging for distant metastases | 81 | CT bone scan 18F-FDG PET/CT |
| Medina-Ornelas 2020 [47] | Retrospective | Mexico | 21 | 68Ga-PSMA-11 (I) | 4 luminal A 4 luminal B Her2+ 2 luminal B Her2- 5 triple negative | Staging of locally advanced and metastatic BC | 127 | 18F-FDG PET/CT |
| First Author and Year | Type | Country | N. Patients | Tracer | Histopathological Subtype (N. Patients) | Clinical Setting (N. Patients) | Analysed Lesions | Comparator |
|---|---|---|---|---|---|---|---|---|
| Rowe 2015 [48] | Prospective | USA | 5 | 18F-DCFPyL (I) | 5 clear cell | Restaging in metastatic patients naive to systemic therapies | 29 | CT and MRI |
| Rhee 2016 [49] | Prospective | Australia | 10 | 68Ga-PSMA-11 (I) | 8 clear cell 1 papillary 1 unclassified | Staging in metastatic patients | 86 | CT |
| Sawicki 2016 [50] | Retrospective | Germany | 6 | 68Ga-PSMA-11 (I) | 4 clear cell 1 papillary 1 chromophobe | Staging in metastatic patients | 22 | / |
| Siva 2017 [51] | Retrospective | Australia | 8 | 68Ga-PSMA-11 (I) | 7clear cell 1 papillary | 2 staging 5 restaging for suspect recurrence 2 staging and restaging after therapy | 18F-FDG PET/CT | |
| Yin 2018 [52] | Prospective | USA | 8 | 18F-DCFPyL (I) | 3 papillary 2 chromophobe 2 unclassified 1 xp11 translocation | Restaging in metastatic patients previously treated with multiple lines of systemic therapy | 73 | CT MRI |
| Meyer 2019 [53] | Prospective | USA | 14 | 18F-DCFPyL (I) | 14 clear cell | Staging in oligometastatic patients | 47 | CT MRI |
| Raveenthiran 2019 [54] | Retrospective | Australia | 38 | 68Ga-PSMA-11 (I) | 28 clear cell 1 oncocytoma 1 papillary 1 chromophobe 1 TCC 6 unknown | 16 primary staging 32 restaging of suspected recurrent disease | 51 | / |
| Gao 2020 [55] | Retrospective | China | 36 | 68Ga-PSMA-11 (I) | 36 clear cell | Untreated primary renal cell carcinoma | / | / |
| Liu 2020 [56] | Retrospective | China | 15 | 18F-DCFPyL (I) | 15 clear cell | Post-operative restaging | 42 | 18F-FDG PET/CT |
| Gühne 2021 [57] | Prospective | Germany | 8 | 68Ga-PSMA-11 (I) | 8 clear cell | Post-operative restaging | 12 | CT |
| Mittlemeier 2021 [58] | Retrospective | Germany | 11 | 18F-PSMA-1007 (I) | 8 clear cell 2 papillary 1 undifferentiated | Response assessment after therapy | / | CT |
| Golan 2021 [59] | Prospective | Israel | 29 | 68Ga-PSMA-11 (I) | 18 clear cell 4 papillary 2 chromophobe 2 oncocytoma 2 angiomyolipoma 1 mixed epithelial and stromal tumour | Dynamic PET/CT in the evaluation of localized renal masses. | 29 | / |
| Gao 2022 [60] | Retrospective | China | 48 | 68Ga-PSMA-11 (I) | 37 clear cell 4 papillary 3 chromophobe 4 unclassified | Staging and comparison between PET parameters with VEGFR-2/PDGFR-β expression | 48 | / |
| Li 2022 [61] | Retrospective | China | 31 | 68Ga-PSMA-11 (I) | 40 clear cell 3 papillary 1 chromophobe 1 mucinous 1 poorly differentiated 4 Others | Staging in metastatic patients | 94 | CT MRI |
| Meng 2022 [62] | Retrospective | China | 53 | 68Ga-PSMA-11 (I) | 40 clear cell 5 papillary 4 chromophobe 4 other | Staging | 53 | / |
| Tariq 2022 [63] | Retrospective | Australia | 11 | 68Ga-PSMA-11 (I) 18F-PSMA-1007 (I) | 10 clear cell 1 unclassified | 4 staging 7 restaging | / | CT MRI |
| First Author and Year | Type | Country | N. Patients | Tracer | Clinical Setting (N. Patients) | Analysed Lesions | Comparator |
|---|---|---|---|---|---|---|---|
| Kesler 2019 [64] | Prospective | Israel | 7 | 68Ga-PSMA-11 (I) | 6 staging 1 restaging after TACE | 37 | 18F-FDG PET/CT CT MRI |
| Kunikowska 2021 [65] | Prospective | Poland | 15 | 68Ga-PSMA-11 (I) | 10 staging, 4 restaging after TACE, 1 restaging after hemiepatectomy and TACE | 44 | CT MRI |
| Gündoğan 2021 [66] | Prospective | Turkey | 14 | 68Ga-PSMA-11 (I) | 12 staging 1 restaging after TACE, 1 restaging after radiofrequency ablation + TACE. | 61 | 18F-FDG PET/CT MRI |
| Hirmas 2021 [67] | Retrospective | Germany | 40 | 68Ga-PSMA-11 (I) | 27 Staging 13 restaging after local or systemic treatment. | 142 | CT |
| Thompson 2022 [68] | Prospective | USA | 31 | 68Ga-PSMA-11 (I) | Staging | 39 | MRI |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rizzo, A.; Dall’Armellina, S.; Pizzuto, D.A.; Perotti, G.; Zagaria, L.; Lanni, V.; Treglia, G.; Racca, M.; Annunziata, S. PSMA Radioligand Uptake as a Biomarker of Neoangiogenesis in Solid Tumours: Diagnostic or Theragnostic Factor? Cancers 2022, 14, 4039. https://doi.org/10.3390/cancers14164039
Rizzo A, Dall’Armellina S, Pizzuto DA, Perotti G, Zagaria L, Lanni V, Treglia G, Racca M, Annunziata S. PSMA Radioligand Uptake as a Biomarker of Neoangiogenesis in Solid Tumours: Diagnostic or Theragnostic Factor? Cancers. 2022; 14(16):4039. https://doi.org/10.3390/cancers14164039
Chicago/Turabian StyleRizzo, Alessio, Sara Dall’Armellina, Daniele Antonio Pizzuto, Germano Perotti, Luca Zagaria, Valerio Lanni, Giorgio Treglia, Manuela Racca, and Salvatore Annunziata. 2022. "PSMA Radioligand Uptake as a Biomarker of Neoangiogenesis in Solid Tumours: Diagnostic or Theragnostic Factor?" Cancers 14, no. 16: 4039. https://doi.org/10.3390/cancers14164039