
Sequential Hypofractionated versus Concurrent Twice-Daily Radiotherapy for Limited-Stage Small-Cell Lung Cancer: A Propensity Score-Matched Analysis

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Radiotherapy
2.3. Acute and Late Toxicities
2.4. Propensity Score Matching
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics and Treatment
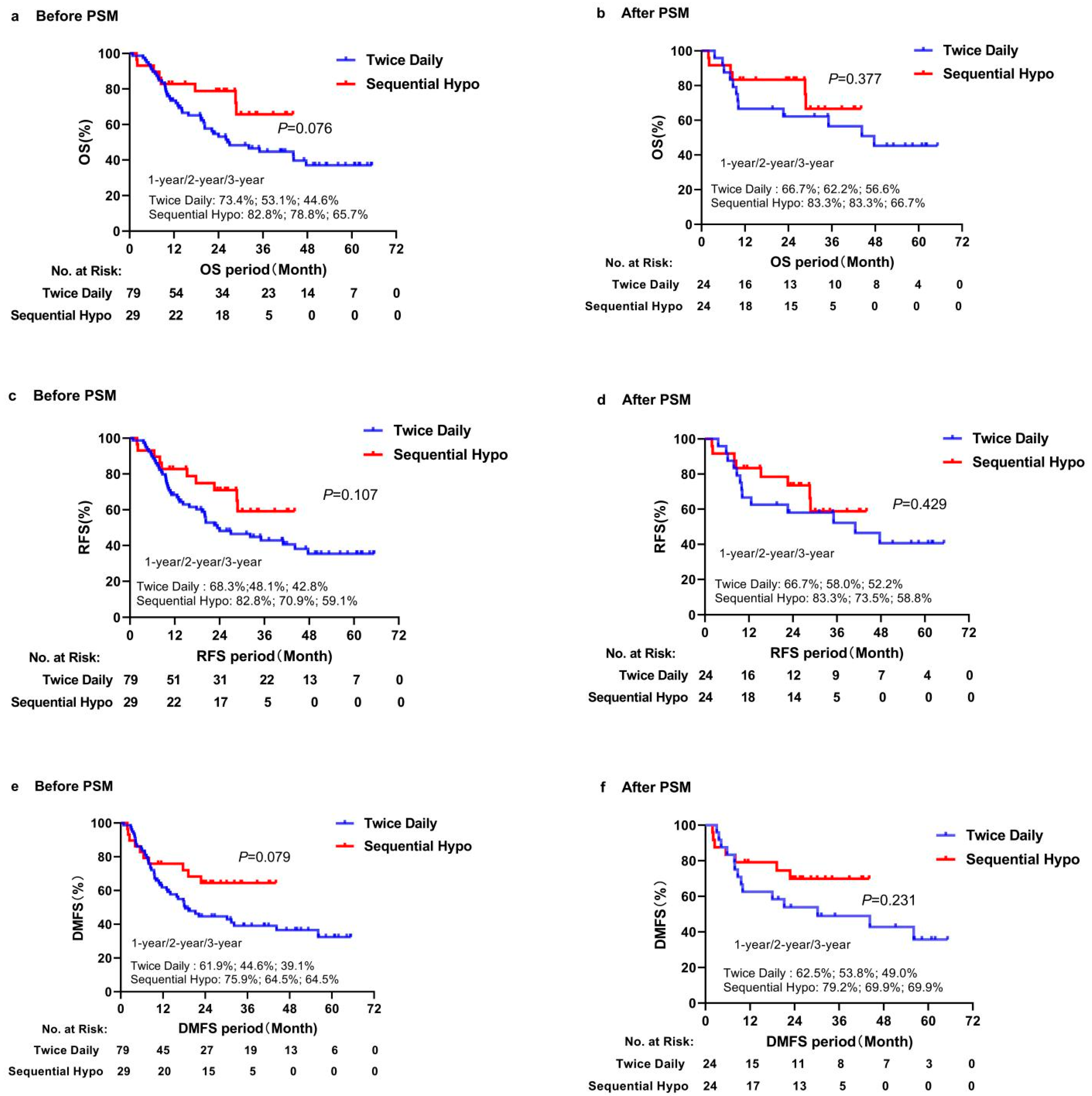
3.2. Survival and Prognostic Factors
3.3. Survival and Prognostic Factors for Matched Patients
3.4. Failure Pattern
3.5. Toxicities
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Herbst, R.S.; Heymach, J.V.; Lippman, S.M. Lung cancer. N. Engl. J. Med. 2008, 359, 1367–1380. [Google Scholar] [CrossRef] [PubMed]
- Govindan, R.; Page, N.; Morgensztern, D.; Read, W.; Tierney, R.; Vlahiotis, A.; Spitznagel, E.L.; Piccirillo, J. Changing epidemiology of small-cell lung cancer in the United States over the last 30 years: Analysis of the surveillance, epidemiologic, and end results database. J. Clin. Oncol. 2006, 24, 4539–4544. [Google Scholar] [CrossRef] [PubMed]
- Almquist, D.; Mosalpuria, K.; Ganti, A.K. Multimodality Therapy for Limited-Stage Small-Cell Lung Cancer. J. Oncol. Pract. 2016, 12, 111–117. [Google Scholar] [CrossRef] [PubMed]
- van Meerbeeck, J.P.; Fennell, D.A.; De Ruysscher, D.K. Small-cell lung cancer. Lancet 2011, 378, 1741–1755. [Google Scholar] [CrossRef]
- Byers, L.A.; Rudin, C.M. Small cell lung cancer: Where do we go from here? Cancer 2015, 121, 664–672. [Google Scholar] [CrossRef] [PubMed]
- Turrisi, A.T.; Kim, K.; Blum, R.; Sause, W.T.; Livingston, R.B.; Komaki, R.; Wagner, H.; Aisner, S.; Johnson, D.H. Twice-daily compared with once-daily thoracic radiotherapy in limited small-cell lung cancer treated concurrently with cisplatin and etoposide. N. Engl. J. Med. 1999, 340, 265–271. [Google Scholar] [CrossRef] [PubMed]
- Rudin, C.M.; Ismaila, N.; Hann, C.L.; Malhotra, N.; Movsas, B.; Norris, K.; Pietanza, M.C.; Ramalingam, S.S.; Turrisi, A.T.; Giaccone, G. Treatment of Small-Cell Lung Cancer: American Society of Clinical Oncology Endorsement of the American College of Chest Physicians Guideline. J. Clin. Oncol. 2015, 33, 4106–4111. [Google Scholar] [CrossRef]
- Früh, M.; De Ruysscher, D.; Popat, S.; Crinò, L.; Peters, S.; Felip, E. Small-cell lung cancer (SCLC): ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2013, 24, 99–105. [Google Scholar] [CrossRef]
- Simone, C.B., II; Bogart, J.A.; Cabrera, A.R.; Daly, M.E.; DeNunzio, N.J.; Detterbeck, F.; Faivre-Finn, C.; Gatschet, N.; Gore, E.; Jabbour, S.K.; et al. Radiation Therapy for Small Cell Lung Cancer: An ASTRO Clinical Practice Guideline. Pract. Radiat. Oncol. 2020, 10, 158–173. [Google Scholar] [CrossRef]
- Faivre-Finn, C.; Snee, M.; Ashcroft, L.; Appel, W.; Barlesi, F.; Bhatnagar, A.; Bezjak, A.; Cardenal, F.; Fournel, P.; Harden, S.; et al. Concurrent once-daily versus twice-daily chemoradiotherapy in patients with limited-stage small-cell lung cancer (CONVERT): An open-label, phase 3, randomised, superiority trial. Lancet Oncol. 2017, 18, S1470–S2045. [Google Scholar] [CrossRef]
- Zhang, J.; Fan, M.; Liu, D.; Zhao, K.L.; Wu, K.L.; Zhao, W.X.; Zhu, Z.F.; Fu, X.L. Hypo- or conventionally fractionated radiotherapy combined with chemotherapy in patients with limited stage small cell lung cancer. Radiat. Oncol. 2017, 12, 51. [Google Scholar] [CrossRef] [PubMed]
- Grønberg, B.H.; Halvorsen, T.O.; Fløtten, Ø.; Brustugun, O.T.; Brunsvig, P.F.; Aasebø, U.; Bremnes, R.M.; Tollåli, T.; Hornslien, K.; Aksnessæther, B.Y. Randomized phase II trial comparing twice daily hyperfractionated with once daily hypofractionated thoracic radiotherapy in limited disease small cell lung cancer. Acta Oncol. 2016, 55, 591–597. [Google Scholar] [CrossRef] [PubMed]
- Qiu, B.; Li, Q.; Liu, J.; Huang, Y.; Pang, Q.; Zhu, Z.; Yang, X.; Wang, B.; Chen, L.; Fang, J. Moderately Hypofractionated Once-Daily Compared with Twice-Daily Thoracic Radiation Therapy Concurrently with Etoposide and Cisplatin in Limited-Stage Small Cell Lung Cancer: A Multicenter, Phase II, Randomized Trial. Int. J. Radiat. Oncol. Biol. Phys. 2021, 111, 424–435. [Google Scholar] [CrossRef] [PubMed]
- Yan, M.; Sigurdson, S.; Greifer, N.; Kennedy, T.A.; Toh, T.S.; Lindsay, P.E.; Weiss, J.; Hueniken, K.; Yeung, C.; Sugumar, V. A Comparison of Hypofractionated and Twice-Daily Thoracic Irradiation in Limited-Stage Small-Cell Lung Cancer: An Overlap-Weighted Analysis. Cancers 2021, 13, 2895. [Google Scholar] [CrossRef]
- Micke, P.; Faldum, A.; Metz, T.; Beeh, K.M.; Bittinger, F.; Hengstler, J.G.; Buhl, R. Staging small cell lung cancer: Veterans Administration Lung Study Group versus International Association for the Study of Lung Cancer—What limits limited disease? Lung Cancer 2002, 37, 271–276. [Google Scholar] [CrossRef]
- Goldstraw, P.; Chansky, K.; Crowley, J.; Rami-Porta, R.; Asamura, H.; Eberhardt, W.E.; Nicholson, A.G.; Groome, P.; Mitchell, A.; Bolejack, V. The IASLC Lung Cancer Staging Project: Proposals for Revision of the TNM Stage Groupings in the Forthcoming (Eighth) Edition of the TNM Classification for Lung Cancer. J. Thorac. Oncol. 2016, 11, 39–51. [Google Scholar] [CrossRef]
- Huang, F.; Sun, M.; Ning, B.; Luo, Y.; An, S. Propensity score matching in SPSS. J. South. Med. Univ. 2015, 35, 1597–1601. [Google Scholar]
- Austin, P.C.; Grootendorst, P.; Anderson, G.M. A comparison of the ability of different propensity score models to balance measured variables between treated and untreated subjects: A Monte Carlo study. Stat. Med. 2007, 26, 734–753. [Google Scholar] [CrossRef]
- Farrell, M.J.; Yahya, J.B.; Degnin, C.; Chen, Y.; Holland, J.M.; Henderson, M.A.; Jaboin, J.J.; Harkenrider, M.M.; Thomas, C.R., Jr.; Mitin, T. Radiation Dose and Fractionation for Limited-stage Small-cell Lung Cancer: Survey of US Radiation Oncologists on Practice Patterns. Clin. Lung Cancer 2019, 20, 13–19. [Google Scholar] [CrossRef]
- Pezzi, T.A.; Schwartz, D.L.; Mohamed, A.S.; Welsh, J.W.; Komaki, R.U.; Hahn, S.M.; Sepesi, B.; Pezzi, C.M.; Fuller, C.D.; Chun, S.G. Barriers to Combined-Modality Therapy for Limited-Stage Small Cell Lung Cancer. JAMA Oncol. 2018, 4, e174504. [Google Scholar] [CrossRef]
- Xia, B.; Hong, L.Z.; Cai, X.W.; Zhu, Z.F.; Liu, Q.; Zhao, K.L.; Fan, M.; Mao, J.F.; Yang, H.J.; Wu, K.L. Phase 2 study of accelerated hypofractionated thoracic radiation therapy and concurrent chemotherapy in patients with limited-stage small-cell lung cancer. Int. J. Radiat. Oncol. Biol. Phys. 2015, 91, 517–523. [Google Scholar] [CrossRef] [PubMed]
- Turgeon, G.A.; Souhami, L.; Kopek, N.; Hirsh, V.; Ofiara, L.; Faria, S.L. Thoracic irradiation in 3weeks for limited-stage small cell lung cancer: Is twice a day fractionation really needed? Cancer Radiother. 2017, 21, 89–98. [Google Scholar] [CrossRef] [PubMed]
- Zayed, S.; Chen, H.; Ali, E.; Rodrigues, G.B.; Warner, A.; Palma, D.A.; Louie, A.V. Is There a Role for Hypofractionated Thoracic Radiation Therapy in Limited-Stage Small Cell Lung Cancer? A Propensity Score Matched Analysis. Int. J. Radiat. Oncol. Biol. Phys. 2020, 108, 575–586. [Google Scholar] [CrossRef] [PubMed]
- Socha, J.; Guzowska, A.; Tyc-Szczepaniak, D.; Wierzchowski, M.; Sprawka, A.; Szczesna, A.; Kepka, L. Accelerated hypofractionated thoracic radiotherapy in limited disease small cell lung cancer: Comparison with the results of conventionally fractionated radiotherapy. J. BUON 2015, 20, 146–157. [Google Scholar] [PubMed]
- Li, Q.W.; Qiu, B.; Wang, B.; Zhang, J.; Chen, L.; Zhou, Y.; Qin, J.K.; Guo, S.P.; Xie, W.H.; Hui, Z.G. Comparison of hyper- and hypofractionated radiation schemes with IMRT technique in small cell lung cancer: Clinical outcomes and the introduction of extended LQ and TCP models. Radiother. Oncol. 2019, 136, 98–105. [Google Scholar] [CrossRef]
- Ohara, S.; Kanda, S.; Okuma, H.; Goto, Y.; Horinouchi, H.; Fujiwara, Y.; Nokihara, H.; Ito, Y.; Yamamoto, N.; Usui, K.; et al. Effect of sequential chemoradiotherapy in patients with limited-disease small-cell lung cancer who were ineligible for concurrent therapy: A retrospective study at two institutions. Jpn. J. Clin. Oncol. 2018, 48, 82–88. [Google Scholar] [CrossRef]
- Qiu, B.; Xiong, M.; Luo, Y.; Li, Q.; Chen, N.; Chen, L.; Guo, S.; Wang, B.; Huang, X.; Lin, M. Hypofractionated Intensity Modulated Radiation Therapy with Concurrent Chemotherapy in Locally Advanced Non-Small Cell Lung Cancer: A Phase II Prospective Clinical Trial (GASTO1011). Pract. Radiat. Oncol. 2021, 11, 374–383. [Google Scholar] [CrossRef]
- De Ruysscher, D.; Pijls-Johannesma, M.; Bentzen, S.M.; Minken, A.; Wanders, R.; Lutgens, L.; Hochstenbag, M.; Boersma, L.; Wouters, B.; Lammering, G.; et al. Time between the first day of chemotherapy and the last day of chest radiation is the most important predictor of survival in limited-disease small-cell lung cancer. J. Clin. Oncol. 2006, 24, 1057–1063. [Google Scholar] [CrossRef]
- Jeong, J.U.; Jeon, W.; Ahn, S.J.; Kim, Y.C.; Oh, I.J.; Park, C.K.; Yoon, M.S.; Song, J.Y.; Nam, T.K.; Chung, W.K. Treatment time to the end of thoracic radiotherapy has more predictive power for survival than radiation dose intensity in patients with limited-stage small-cell lung cancer receiving concurrent chemoradiation of more than 45 Gy. Oncol. Lett. 2020, 19, 239–246. [Google Scholar] [CrossRef]
- Hu, X.; Xia, B.; Bao, Y.; Xu, Y.J.; Wang, J.; Ma, H.L.; Peng, F.; Jin, Y.; Fang, M.; Tang, H.R. Correction to: Timing of thoracic radiotherapy is more important than dose intensification in patients with limited-stage small cell lung cancer: A parallel comparison of two prospective studies. Strahlenther. Onkol. 2020, 196, 405. [Google Scholar] [CrossRef]
- Zhao, S.; Zhou, T.; Ma, S.; Zhao, Y.; Zhan, J.; Fang, W.; Yang, Y.; Hou, X.; Zhang, Z.; Chen, G.; et al. Effects of thoracic radiotherapy timing and duration on progression-free survival in limited-stage small cell lung cancer. Cancer Med. 2018, 7, 4208–4216. [Google Scholar] [CrossRef] [PubMed]
- Hasan, S.; White, R.; Renz, P.; Abel, S.; Otaibi, Z.; Monga, D.; Colonias, A.; Wegner, R.E. Optimal timing of thoracic radiotherapy in limited stage small cell lung cancer (SCLC) with daily fractionation: A brief report. Radiother. Oncol. 2019, 132, 23–26. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.J.; Lee, E.J.; Hur, G.Y.; Lee, S.Y.; Kim, J.H.; Shin, C.; Shim, J.J.; In, K.H.; Kang, K.H.; Yoo, S.H. The start of chemotherapy until the end of radiotherapy in patients with limited-stage small cell lung cancer. Korean J. Intern. Med. 2013, 28, 449–455. [Google Scholar] [CrossRef]
- Xiao, X.G.; Wang, S.J.; Hu, L.Y.; Chu, Q.; Wei, Y.; Li, Y.; Mei, Q.; Chen, Y. Relationship between the SER treatment period and prognosis of patients with small cell lung cancer. Asian Pac. J. Cancer Prev. 2014, 15, 6415–6419. [Google Scholar] [CrossRef] [PubMed]
- Fried, D.B.; Morris, D.E.; Poole, C.; Rosenman, J.G.; Halle, J.S.; Detterbeck, F.C.; Hensing, T.A.; Socinski, M.A. Systematic review evaluating the timing of thoracic radiation therapy in combined modality therapy for limited-stage small-cell lung cancer. J. Clin. Oncol. 2004, 22, 4837–4845. [Google Scholar] [CrossRef]
- Liu, L.; Wei, J.; Teng, F.; Zhu, Y.; Xing, P.; Zhang, J.; Guo, Y.; Dong, J.; Ying, J.; Li, J. Clinicopathological features and prognostic analysis of 247 small cell lung cancer with limited-stage after surgery. Hum. Pathol. 2021, 108, 84–92. [Google Scholar] [CrossRef]
- SchnÖller, L.; Kaesmann, L.; Taugner, J.; Abdo, R.; Eze, C.; Manapov, F. Prognostic Role of Lung Immune Scores for Prediction of Survival in Limited-stage Small Cell Lung Cancer. In Vivo 2021, 35, 929–935. [Google Scholar] [CrossRef]
- Bettington, C.S.; Tripcony, L.; Bryant, G.; Hickey, B.; Pratt, G.; Fay, M. A retrospective analysis of survival outcomes for two different radiotherapy fractionation schedules given in the same overall time for limited stage small cell lung cancer. J. Med. Imaging Radiat. Oncol. 2013, 57, 105–112. [Google Scholar] [CrossRef]


{kind=link}
| Variables | Before PSM (n = 108) | After PSM (n = 48) | ||||||
|---|---|---|---|---|---|---|---|---|
| Total | Twice-Daily (n = 79) | Sequential Hypo (n = 29) | p | Total | Twice-Daily (n = 24) | Sequential Hypo (n = 24) | p | |
| Age (years) | 58.0 (49.0, 64.0) | 57.0 (49.0, 63.0) | 61.0 (52.0, 65.0) | 0.171 | 58.5 (48.3, 64.0) | 56.5 (48.3, 65.5) | 59.5 (48.8, 64.0) | 0.718 |
| SER (days) | 105.5 (75.3, 147.8) | 96.0 (70.0, 125.0) | 140.0 (106.0, 177.5) | 0.002 | 128.5 (94.3, 173.8) | 109.0 (77.8, 138.0) | 154.5 (117.0, 195.3) | 0.006 |
| Total chemotherapy cycles | 4.0 (3.0, 5.0) | 4.0 (3.0, 5.0) | 4.0 (3.5, 5.5) | 0.433 | 4.0 (3.0, 5.8) | 4.0 (3.0, 5.0) | 4.0 (4.0, 6.0) | 0.118 |
| Chemotherapy cycles before radiotherapy | 3.0 (2.0, 4.0) | 3.0 (2.0, 4.0) | 4.0 (3.0, 5.5) | 0.003 | 4.0 (3.0, 5.0) | 3.0 (2.0, 4.0) | 4.0 (4.0, 6.0) | 0.004 |
| Total radiotherapy time (days) | 21.0 (20.0, 25.0) | 21.0 (20.0, 23.0) | 24.0 (22.5, 27.5) | <0.001 | 21.0 (20.0, 25.8) | 21.0 (20.0, 21.0) | 23.5 (21.3, 27.0) | 0.002 |
| Sex | 0.153 | 0.131 | ||||||
| Male | 78 (72.2) | 60 (75.9) | 18 (62.1) | 31 (64.6) | 18 (75.0) | 13 (54.2) | ||
| Female | 30 (27.8) | 19 (24.1) | 11 (37.9) | 17 (35.4) | 6 (25.0) | 11 (45.8) | ||
| ECOG PS | 0.147 | 1.000 | ||||||
| 0–1 | 91 (84.3) | 69 (87.3) | 22 (75.9) | 42 (87.5) | 21 (87.5) | 21 (85.5) | ||
| 2–3 | 17 (15.7) | 10 (12.7) | 7 (24.1) | 6 (12.5) | 3 (12.5) | 3)12.5) | ||
| Smoking status | 0.121 | 0.500 | ||||||
| Never smoker | 21 (19.4) | 14 (17.7) | 7 (24.1) | 9 (18.8) | 5 (20.8) | 4 (16.7) | ||
| Former smoker | 36 (33.3) | 23 (29.1) | 13 (44.8) | 20 (41.7) | 8 (33.3) | 12 (50.0) | ||
| Current smoker | 51 (47.2) | 42 (53.2) | 9 (31.0) | 19 (39.6) | 11 (45.8) | 8 (33.3) | ||
| PCI | 0.007 | 0.755 | ||||||
| No | 28 (25.9) | 15 (19.0) | 13 (44.8) | 15 (31.3) | 7 (29.2) | 8 (33.3) | ||
| Yes | 80 (74.1) | 64 (81.0) | 16 (55.2) | 33 (68.8) | 17 (70.8) | 16 (66.7) | ||
| Introduction chemotherapy | 0.061 | 1.000 | ||||||
| No | 7 (6.5) | 3 (3.8) | 4 (13.8) | 4 (8.3) | 2 (8.3) | 2 (8.3) | ||
| Yes | 101 (93.5) | 76 (96.2) | 25 (86.2) | 44 (91.7) | 22 (91.7) | 22 (91.7) | ||
| SER (day) | 0.009 | 0.027 | ||||||
| <90 | 36 (33.3) | 32 (40.5) | 4 (13.8) | 9 (18.8) | 8 (33.3) | 1 (4.2) | ||
| ≥90 | 72 (66.7) | 47 (59.5) | 25 (86.2) | 39 (81.3) | 16 (66.7) | 23 (95.8) | ||
| Total radiotherapy time (days) | 0.001 | 0.035 | ||||||
| <24 | 74 (68.5) | 61 (77.2) | 13 (44.8) | 31 (64.6) | 19 (79.2) | 12 (50) | ||
| ≥24 | 34 (31.5) | 18 (22.8) | 16 (55.2) | 17 (35.4) | 5 (20.8) | 12 (50) | ||
| Total chemotherapy cycles (times) | 0.319 | 0.051 | ||||||
| <4 | 34 (31.5) | 27 (34.2) | 7 (24.1) | 13 (27.1) | 10 (41.7) | 3 (12.5) | ||
| ≥4 | 74 (68.5) | 52 (65.8) | 22 (75.9) | 35 (72.9) | 14 (58.3) | 21 (87.5) | ||
| Chemo cycles before radiotherapy (times) | 0.519 | |||||||
| <2 | 15 (13.9) | 12 (15.2) | 3 (10.3) | 3 (6.3) | 3 (12.5) | 0 (0) | 0.233 | |
| ≥2 | 93 (86.1) | 67 (84.8) | 26 (89.7) | 45 (93.7) | 21 (87.5) | 24 (100) | ||
| T stage | 0.035 | 0.149 | ||||||
| 1–2 | 86 (79.6) | 59 (74.7) | 27 (93.2) | 46 (95.8) | 24 (100.0) | 22 (91.7) | ||
| 3–4 | 22 (20.4) | 20 (25.3) | 2 (6.8) | 2 (4.2) | 0 (0) | 2 (8.4) | ||
| N stage | 0.304 | 0.712 | ||||||
| 0–1 | 22 (20.4) | 18 (22.8) | 4 (13.8) | 9 (18.8) | 5 (20.8) | 4 (16.7) | ||
| 2–3 | 86 (79.6) | 61 (77.2) | 25 (86.2) | 39 (81.2) | 19 (79.2) | 20 (83.3) | ||
| AJCC stage | 0.389 | 0.466 | ||||||
| I | 2 (1.9) | 1 (1.3) | 1 (3.4) | 1 (2.1) | 0 (0) | 1 (4.2) | ||
| II | 19 (17.6) | 16 (20.2) | 3 (10.3) | 8 (16.7) | 5 (20.8) | 3 (12.5) | ||
| III | 87 (80.5) | 62 (78.5) | 25 (86.2) | 39 (81.2) | 19 (79.2) | 20 (83.3) | ||
| Comorbidity | 0.091 | 0.477 | ||||||
| No | 83 (76.8) | 64 (81.0) | 19 (65.5) | 38 (79.2) | 20 (83.3) | 18 (75.0) | ||
| Yes | 25 (23.2) | 15 (19.0) | 10 (34.5) | 10 (20.8) | 4 (16.7) | 6 (25.0) | ||
| Dose and Fractionation (Gy/F) | - | - | ||||||
| 54/18(QD) | 18 (16.7) | - | 18 (62.1) | 14 (29.2) | - | 14 (58.3) | ||
| 45/15(QD) | 6 (5.5) | - | 6 (20.6) | 5 (10.4) | - | 5 (20.9) | ||
| 60/20(QD) | 5 (4.6) | - | 5 (17.2) | 5 (10.4) | - | 5 (20.8) | ||
| 45/30(BID) | 79 (73.1) | 79 (100.0) | - | 24 (50.0) | 24 (100.0) | - | ||
| Variables | OS | RFS | DMFS | |||
|---|---|---|---|---|---|---|
| HR (95%CI) | p | HR (95%CI) | p | HR (95%CI) | p | |
| Age (years) | 1.032 (0.987–1.079) | 0.163 | 1.038 (0.996–1.081) | 0.079 | 1.022 (0.981–1.064) | 0.303 |
| SER (days) | 1.001 (0.997–1.006) | 0.564 | 1.001 (0.996–1.006) | 0.670 | 0.999 (0.994–1.004) | 0.754 |
| Total chemotherapy cycles (times) | 1.084 (0.805–1.460) | 0.595 | 1.148 (0.863–1.527) | 0.344 | 1.029 (0.782–1.354) | 0.839 |
| Chemotherapy cycles before radiotherapy (times) | 1.237 (0.893–1.713) | 0.200 | 1.218 (0.906–1.638) | 0.192 | 1.051 (0.789–1.401) | 0.735 |
| Total radiotherapy time (days) | 1.034 (0.978–1.092) | 0.239 | 1.027 (0.973–1.084) | 0.331 | 1.030 (0.971–1.093) | 0.331 |
| Group | ||||||
| Twice-daily | 1.000 | 1.000 | 1.000 | |||
| Sequential hypo | 0.632 (0.228–1.748) | 0.377 | 0.697 (0.283–1.715) | 0.432 | 0.569 (0.223–1.449) | 0.237 |
| Age (years) | ||||||
| <65 | 1.000 | 1.000 | 1.000 | |||
| ≥65 | 4.483 (1.713–11.729) | 0.002 | 3.528 (1.408–8.842) | 0.007 | 3.383 (1.348–8.493) | 0.009 |
| Sex | ||||||
| Male | 1.000 | 1.000 | 1.000 | |||
| Female | 0.783 (0.275–2.233) | 0.648 | 0.766 (0.294–1.994) | 0.585 | 0.567 (0.206–1.559) | 0.272 |
| ECOG PS | ||||||
| 0–1 | 1.000 | 1.000 | 1.000 | |||
| 2–3 | 1.192 (0.454–3.129) | 0.722 | 1.403 (0.185–10.636) | 0.743 | 0.879 (0.117–6.602) | 0.900 |
| Smoking status | ||||||
| Never smoker | 1.000 | 1.000 | 1.000 | |||
| Former smoker | 1.055 (0.262–4.244) | 0.940 | 1.333 (0.352–5.050) | 0.672 | 0.929 (0.269–3.211) | 0.908 |
| Current smoker | 1.853 (0.498–6.898) | 0.358 | 2.062 (0.565–7.525) | 0.273 | 1.555 (0.486–4.974) | 0.457 |
| PCI | ||||||
| No | 1.000 | 1.000 | 1.000 | |||
| Yes | 1.151 (0.408–3.247) | 0.790 | 1.078 (0.417–2.788) | 0.877 | 0.839 (0.366–2.092) | 0.706 |
| Introduction chemotherapy | ||||||
| No | 1.000 | 1.000 | 1.000 | |||
| Yes | 23.292 (0.018–30,250.428) | 0.389 | 2.047 (0.274–15.290) | 0.485 | 23.925 (0.050–11,441.100) | 0.313 |
| SER (day) | ||||||
| <110 | 1.000 | 1.000 | 1.000 | |||
| ≥110 | 3.124 (1.003–9.733) | 0.049 | 2.586 (0.937–7.141) | 0.067 | 1.589 (0.629–4.016) | 0.327 |
| Total radiotherapy time (days) | ||||||
| <24 | 1.000 | 1.000 | 1.000 | |||
| ≥24 | 2.848 (1.105–7.344) | 0.030 | 2.478 (1.039–5.908) | 0.041 | 1.990 (0.808–4.901) | 0.135 |
| Total chemotherapy cycles (times) | ||||||
| <6 | 1.000 | 1.000 | 1.000 | |||
| ≥6 | 0.598 (0.173–2.071) | 0.417 | 0.915 (0.334–2.509) | 0.863 | 0.720 (0.241–2.149) | 0.556 |
| Chemotherapy cycles before radiotherapy (times) | ||||||
| <4 | 1.000 | 1.000 | 1.000 | |||
| ≥4 | 2.033 (0.709–5.831) | 0.187 | 1.736 (0.669–4.507) | 0.257 | 1.135 (0.461–2.793) | 0.782 |
| T stage | ||||||
| 1–2 | 1.000 | 1.000 | 1.000 | |||
| 3–4 | 0.046 (0–4612.460) | 0.601 | 1.465 (0.193–11.110) | 0.712 | 0.046 (0–898.256) | 0.542 |
| N stage | ||||||
| 0–1 | 1.000 | 1.000 | 1.000 | |||
| 2–3 | 2.024 (0.465–8.814) | 0.348 | 2.576 (0.599–11.077) | 0.204 | 2.488 (0.579–10.701) | 0.221 |
| AJCC stage | ||||||
| I–II | 1.000 | 1.000 | 1.000 | |||
| III | 2.024 (0.465–8.814) | 0.348 | 2.576 (0.599–11.077) | 0.204 | 2.488 (0.579–10.701) | 0.221 |
| Comorbidity | ||||||
| No | 1.000 | 1.000 | 1.000 | |||
| Yes | 1.274 (0.453–3.579) | 0.646 | 0.988 (0.362–2.701) | 0.982 | 1.234 (0.477–3.193) | 0.665 |
| Variables | OS | RFS | DMFS | |||
|---|---|---|---|---|---|---|
| HR (95%CI) | p | HR (95%CI) | p | HR (95%CI) | p | |
| Age (years) | ||||||
| <65 | 1.000 | 1.000 | 1.000 | |||
| ≥65 | 4.222 (1.601–11.134) | 0.004 | 3.371 (1.337–8.498) | 0.010 | 3.383 (1.348–8.493) | 0.009 |
| Total radiotherapy time (days) | ||||||
| <24 | 1.000 | 1.000 | ||||
| ≥24 | 2.671 (1.018–7.009) | 0.046 | 2.370 (0.984–5.707) | 0.054 | ||
| Site | Before PSM (n = 108) | After PSM (n = 48) | ||||
|---|---|---|---|---|---|---|
| Twice-Daily (n = 79) | Sequential Hypo (n = 29) | p | Twice-Daily (n = 24) | Sequential Hypo (n = 24) | p | |
| Local and/or regional | ||||||
| Local only | 4 (5.1) | 2 (6.9) | 1.000 | 2 (8.3) | 2 (8.3) | 1.000 |
| Local and regional | 2 (2.5) | 0 (0) | 0.952 | 0 (0) | 0 (0) | 1.000 |
| Local and distant | 5 (6.3) | 2 (6.9) | 1.000 | 1 (4.2) | 1 (4.2) | 1.000 |
| Local, regional and distant | 1 (1.3) | 0 (0) | 1.000 | 0 (0) | 0 (0) | 1.000 |
| Regional only | 3 (3.8) | 0 (0) | 0.686 | 0 (0) | 0 (0) | 1.000 |
| Regional and distant | 2 (2.5) | 1 (3.5) | 1.000 | 0 (0) | 1 (4.2) | 1.000 |
| Distant | ||||||
| Bone only | 4 (5.1) | 0 (0) | 0.509 | 1 (4.2) | 1 (4.2) | 1.000 |
| Liver only | 1 (1.3) | 1 (3.5) | 1.000 | 1 (4.2) | 1 (4.2) | 1.000 |
| Lung only | 2 (2.5) | 1 (3.5) | 1.000 | 1 (4.2) | 1 (4.2) | 1.000 |
| Brain only | 13 (16.5) | 1 (3.5) | 0.144 | 3 (12.5) | 0 (0) | 0.233 |
| Multiple location a | 4 (5.1) | 1 (3.5) | 1.000 | 3 (12.5) | 1 (4.2) | 0.602 |
| Other location b | 5 (6.3) | 2 (6.9) | 1.000 | 1 (4.2) | 3 (12.5) | 0.602 |
| Total locoregional failure | 14 (17.7) | 5 (17.2) | 0.954 | 3 (12.5) | 3 (12.5) | 1.000 |
| Total distant failure | 32 (40.5) | 5 (17.2) | 0.024 | 9 (37.5) | 6 (25.0) | 0.350 |
| Toxicities | Before PSM | p | After PSM | p | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Twice-Daily (n = 79) | Sequential Hypo (n = 29) | Twice-Daily (n = 24) | Sequential Hypo (n = 24) | |||||||
| Grade 1–2 | Grade 3–4 | Grade 1–2 | Grade 3–4 | Grade 1–2 | Grade 3–4 | Grade 1–2 | Grade 3–4 | |||
| Acute | ||||||||||
| esophagitis | 71 (89.9) | 0 (0) | 23 (79.3) | 0 (0) | 0.261 | 22 (91.7) | 0 (0) | 19 (79.2) | 0 (0) | 0.001 |
| Hematotoxicity | 30 (38.0) | 20 (25.3) | 11 (37.9) | 1 (3.4) | 0.022 | 11 (45.8) | 6 (25.0) | 10 (41.7) | 1 (4.2) | 0.062 |
| Gastrointestinal | 5 (6.3) | 0 (0) | 0 (0) | 0 (0) | - | 1 (4.2) | 0 (0) | 0 (0) | 0 (0) | - |
| Late | ||||||||||
| pneumonitis | 3 (3.8) | 0 (0) | 1 (3.4) | 0 (0) | 1.000 | 1 (4.2) | 0 (0) | 1 (4.2) | 0 (0) | 1.000 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhou, W.; Wang, P.; Ti, X.; Yin, Y.; Huang, S.; Yang, Z.; Li, J.; Chai, G.; Lyu, B.; Li, Z.; et al. Sequential Hypofractionated versus Concurrent Twice-Daily Radiotherapy for Limited-Stage Small-Cell Lung Cancer: A Propensity Score-Matched Analysis. Cancers 2022, 14, 3920. https://doi.org/10.3390/cancers14163920
Zhou W, Wang P, Ti X, Yin Y, Huang S, Yang Z, Li J, Chai G, Lyu B, Li Z, et al. Sequential Hypofractionated versus Concurrent Twice-Daily Radiotherapy for Limited-Stage Small-Cell Lung Cancer: A Propensity Score-Matched Analysis. Cancers. 2022; 14(16):3920. https://doi.org/10.3390/cancers14163920
Chicago/Turabian StyleZhou, Wei, Pang Wang, Xinyu Ti, Yutian Yin, Shigao Huang, Zhi Yang, Jie Li, Guangjin Chai, Bo Lyu, Zhaohui Li, and et al. 2022. "Sequential Hypofractionated versus Concurrent Twice-Daily Radiotherapy for Limited-Stage Small-Cell Lung Cancer: A Propensity Score-Matched Analysis" Cancers 14, no. 16: 3920. https://doi.org/10.3390/cancers14163920