
Clinical Post-SARS-CoV-2 Infection Scenarios in Vaccinated and Non-Vaccinated Cancer Patients in Three German Cancer Centers: A Retrospective Analysis

 ,
,  , , , , ,
, , , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Methods
2.3. Definitions
2.4. Analyzed Data
2.5. Statistics
3. Results
3.1. Characteristics of Non-Vaccinated and Vaccinated Cancer Patients with Positive Test for SARS-CoV-2
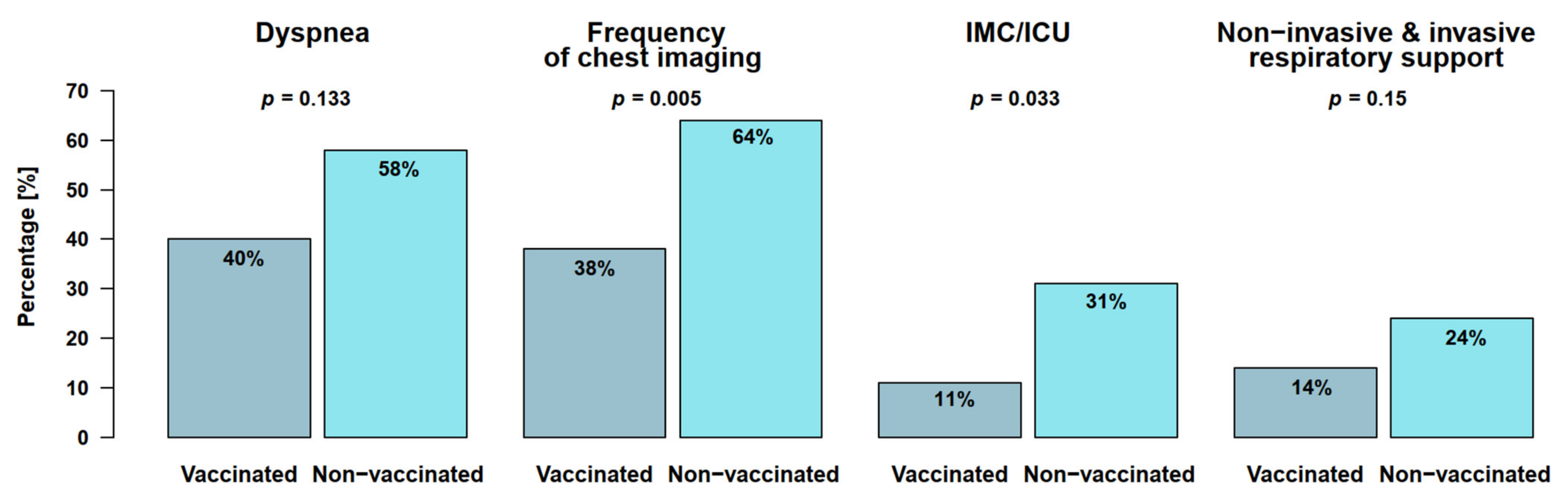
3.2. Clinical, Laboratory, and Imaging Findings in 133 Cancer Patients with SARS-CoV-2
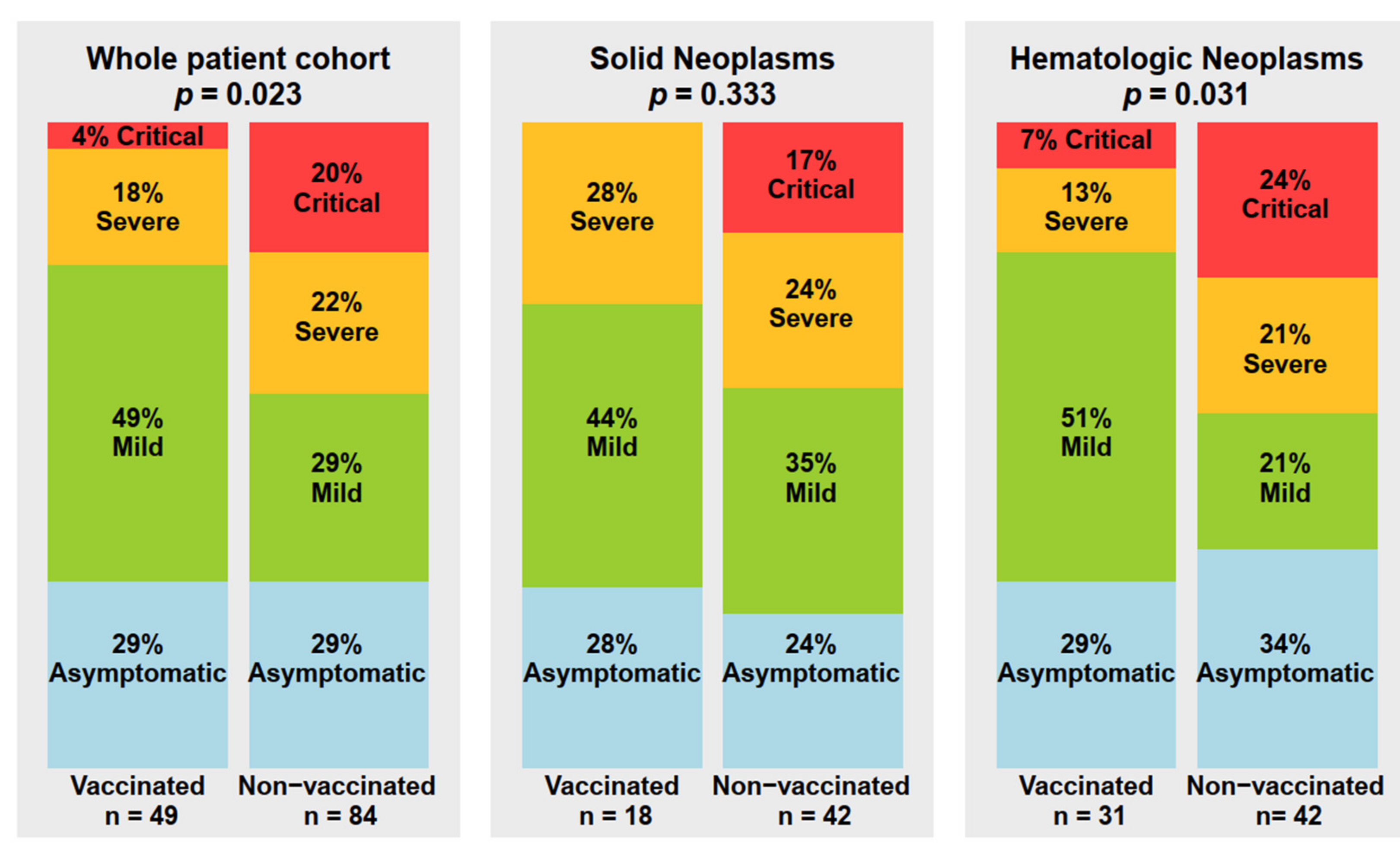
3.3. SARS-CoV-2 Infection Course
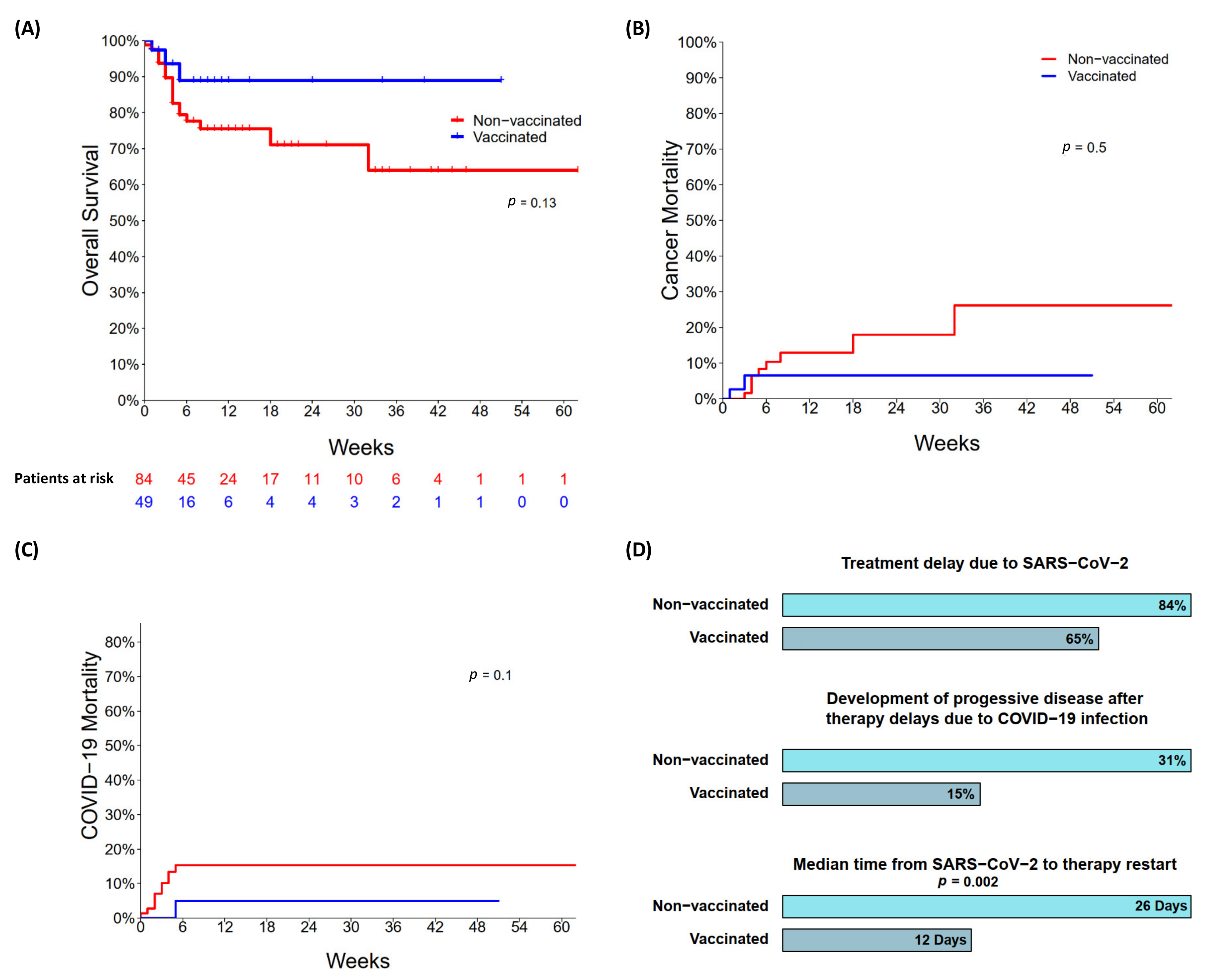
3.4. Outcomes of SARS-CoV-2 Infection with Impact on Cancer Course
4. Discussion
5. Conclusions
- (1)
- The likelihood of a milder COVID-19 course is much greater in vaccinated than in non-vaccinated cancer patients.
- (2)
- COVID-19 vaccines reduce the number of admissions to intermediate/intensive care units, reduce the need for non- and invasive respiratory support, and shorten the length of in-hospital stay following COVID-19 in cancer patients.
- (3)
- COVID-19 vaccines enable significantly earlier resumption of cancer therapies after SARS-CoV-2 infection
- (4)
- Despite vaccination, up to 20% of all cancer patients remain at high risk for a severe or critical COVID-19 course, which mandates a further urgent improvement in pre- and post-SARS-CoV-2 exposure strategies.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Saini, K.S.; Tagliamento, M.; Lambertini, M.; McNally, R.; Romano, M.; Leone, M.; Curigliano, G.; de Azambuja, E. Mortality in patients with cancer and coronavirus disease 2019: A systematic review and pooled analysis of 52 studies. Eur. J. Cancer 2020, 139, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Lee, L.Y.W.; Cazier, J.-B.; Angelis, V.; Arnold, R.; Bisht, V.; Campton, N.A.; Chackathayil, J.; Cheng, V.W.T.; Curley, H.M.; Fittall, M.W.; et al. COVID-19 mortality in patients with cancer on chemotherapy or other anticancer treatments: A prospective cohort study. Lancet 2020, 395, 1919–1926. [Google Scholar] [CrossRef]
- Pinato, D.J.; Zambelli, A.; Aguilar-Company, J.; Bower, M.; Sng, C.C.T.; Salazar, R.; Bertuzzi, A.; Brunet, J.; Mesia, R.; Seguí, E.; et al. Clinical Portrait of the SARS-CoV-2 Epidemic in European Patients with Cancer. Cancer Discov. 2020, 10, 1465–1474. [Google Scholar] [CrossRef]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- El Sahly, H.M.; Baden, L.R.; Essink, B.; Doblecki-Lewis, S.; Martin, J.M.; Anderson, E.J.; Campbell, T.B.; Clark, J.; Jackson, L.A.; Fichtenbaum, C.J.; et al. Efficacy of the mRNA-1273 SARS-CoV-2 Vaccine at Completion of Blinded Phase. N. Engl. J. Med. 2021, 385, 1774–1785. [Google Scholar] [CrossRef]
- Sadoff, J.; Gray, G.; Vandebosch, A.; Cárdenas, V.; Shukarev, G.; Grinsztejn, B.; Goepfert, P.A.; Truyers, C.; Fennema, H.; Spiessens, B.; et al. Safety and Efficacy of Single-Dose Ad26.COV2.S Vaccine against Covid-19. N. Engl. J. Med. 2021, 384, 2187–2201. [Google Scholar] [CrossRef] [PubMed]
- Cavaleri, M.; Enzmann, H.; Straus, S.; Cooke, E. The European Medicines Agency’s EU conditional marketing authorisations for COVID-19 vaccines. Lancet 2021, 397, 355–357. [Google Scholar] [CrossRef]
- Voysey, M.; Clemens, S.A.C.; Madhi, S.A.; Weckx, L.Y.; Folegatti, P.M.; Aley, P.K.; Angus, B.; Baillie, V.L.; Barnabas, S.L.; Bhorat, Q.E.; et al. Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: An interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet 2021, 397, 99–111. [Google Scholar] [CrossRef]
- Ligumsky, H.; Safadi, E.; Etan, T.; Vaknin, N.; Waller, M.; Croll, A.; Nikolaevski-Berlin, A.; Greenberg, I.; Halperin, T.; Wasserman, A.; et al. Immunogenicity and Safety of the BNT162b2 mRNA COVID-19 Vaccine Among Actively Treated Cancer Patients. JNCI J. Natl. Cancer Inst. 2021, 114, 203–209. [Google Scholar] [CrossRef]
- Massarweh, A.; Eliakim-Raz, N.; Stemmer, A.; Levy-Barda, A.; Yust-Katz, S.; Zer, A.; Benouaich-Amiel, A.; Ben-Zvi, H.; Moskovits, N.; Brenner, B.; et al. Evaluation of Seropositivity Following BNT162b2 Messenger RNA Vaccination for SARS-CoV-2 in Patients Undergoing Treatment for Cancer. JAMA Oncol. 2021, 7, 1133–1140. [Google Scholar] [CrossRef]
- Herishanu, Y.; Avivi, I.; Aharon, A.; Shefer, G.; Levi, S.; Bronstein, Y.; Morales, M.; Ziv, T.; Shorer Arbel, Y.; Scarfò, L.; et al. Efficacy of the BNT162b2 mRNA COVID-19 vaccine in patients with chronic lymphocytic leukemia. Blood 2021, 137, 3165–3173. [Google Scholar] [CrossRef] [PubMed]
- Thakkar, A.; Gonzalez-Lugo, J.D.; Goradia, N.; Gali, R.; Shapiro, L.C.; Pradhan, K.; Rahman, S.; Kim, S.Y.; Ko, B.; Sica, R.A.; et al. Seroconversion rates following COVID-19 vaccination among patients with cancer. Cancer Cell 2021, 39, 1081–1090.e1082. [Google Scholar] [CrossRef] [PubMed]
- Greenberger, L.M.; Saltzman, L.A.; Senefeld, J.W.; Johnson, P.W.; DeGennaro, L.J.; Nichols, G.L. Antibody response to SARS-CoV-2 vaccines in patients with hematologic malignancies. Cancer Cell 2021, 39, 1031–1033. [Google Scholar] [CrossRef] [PubMed]
- Beigel, J.H.; Tomashek, K.M.; Dodd, L.E.; Mehta, A.K.; Zingman, B.S.; Kalil, A.C.; Hohmann, E.; Chu, H.Y.; Luetkemeyer, A.; Kline, S.; et al. Remdesivir for the Treatment of COVID-19—Final Report. N. Engl. J. Med. 2020, 383, 1813–1826. [Google Scholar] [CrossRef] [PubMed]
- Mahase, E. Covid-19: UK approves monoclonal antibody sotrovimab for over 12s at high risk. Bmj 2021, 375, n2990. [Google Scholar] [CrossRef]
- Weinreich, D.M.; Sivapalasingam, S.; Norton, T.; Ali, S.; Gao, H.; Bhore, R.; Xiao, J.; Hooper, A.T.; Hamilton, J.D.; Musser, B.J.; et al. REGEN-COV Antibody Combination and Outcomes in Outpatients with Covid-19. N. Engl. J. Med. 2021, 385, e81. [Google Scholar] [CrossRef] [PubMed]
- Shumilov, E.; Hoffknecht, P.; Koch, R.; Peceny, R.; Voigt, S.; Schmidt, N.; Peeck, M.; Bacher, U.; Scheithauer, S.; Trümper, L.; et al. Diagnostic, Clinical and Post-SARS-CoV-2 Scenarios in Cancer Patients with SARS-CoV-2: Retrospective Analysis in Three German Cancer Centers. Cancers 2021, 13, 2917. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons From the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72 314 Cases From the Chinese Center for Disease Control and Prevention. Jama 2020, 323, 1239–1242. [Google Scholar] [CrossRef]
- Shapiro, L.C.; Thakkar, A.; Campbell, S.T.; Forest, S.K.; Pradhan, K.; Gonzalez-Lugo, J.D.; Quinn, R.; Bhagat, T.D.; Choudhary, G.S.; McCort, M.; et al. Efficacy of booster doses in augmenting waning immune responses to COVID-19 vaccine in patients with cancer. Cancer Cell 2022, 40, 3–5. [Google Scholar] [CrossRef] [PubMed]
- Ruthrich, M.M.; Giessen-Jung, C.; Borgmann, S.; Classen, A.Y.; Dolff, S.; Gruner, B.; Hanses, F.; Isberner, N.; Kohler, P.; Lanznaster, J.; et al. COVID-19 in cancer patients: Clinical characteristics and outcome-an analysis of the LEOSS registry. Ann. Hematol. 2021, 100, 383–393. [Google Scholar] [CrossRef] [PubMed]
- Pagano, L.; Salmanton-García, J.; Marchesi, F.; Busca, A.; Corradini, P.; Hoenigl, M.; Klimko, N.; Koehler, P.; Pagliuca, A.; Passamonti, F.; et al. COVID-19 infection in adult patients with hematological malignancies: A European Hematology Association Survey (EPICOVIDEHA). J. Hematol. Oncol. 2021, 14, 168. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, A.L.; Labaki, C.; Hsu, C.Y.; Bakouny, Z.; Balanchivadze, N.; Berg, S.A.; Blau, S.; Daher, A.; El Zarif, T.; Friese, C.R.; et al. COVID-19 vaccination and breakthrough infections in patients with cancer. Ann Oncol 2022, 33, 340–346. [Google Scholar] [CrossRef] [PubMed]
- Boeckel, G.R.; Hölscher, S.D.; Bürger, C.; Jacob, T.; Krekeler, C.; Shumilov, E.; Reicherts, C.; Bleckmann, A.; Lenz, G.; Vollenberg, R.; et al. Comprehensive Treatment of Hematological Patients with SARS-CoV-2 Infection Including Anti-SARS-CoV-2 Monoclonal Antibodies: A Single-Center Experience Case Series. Curr. Oncol. 2022, 29, 2312–2325. [Google Scholar] [CrossRef] [PubMed]
- Pagano, L.; Salmanton-García, J.; Marchesi, F.; López-García, A.; Lamure, S.; Itri, F.; Gomes-Silva, M.; Dragonetti, G.; Falces-Romero, I.; van Doesum, J.; et al. COVID-19 in vaccinated adult patients with hematological malignancies: Preliminary results from EPICOVIDEHA. Blood 2022, 139, 1588–1592. [Google Scholar] [CrossRef]
- Fendler, A.; Shepherd, S.T.C.; Au, L.; Wu, M.; Harvey, R.; Schmitt, A.M.; Tippu, Z.; Shum, B.; Farag, S.; Rogiers, A.; et al. Omicron neutralising antibodies after third COVID-19 vaccine dose in patients with cancer. Lancet 2022, 399, 905–907. [Google Scholar] [CrossRef]
- Mittelman, M.; Magen, O.; Barda, N.; Dagan, N.; Oster, H.S.; Leader, A.; Balicer, R. Effectiveness of the BNT162b2mRNA COVID-19 vaccine in patients with hematological neoplasms in a nationwide mass vaccination setting. Blood 2022, 139, 1439–1451. [Google Scholar] [CrossRef]
- Fendler, A.; de Vries, E.G.E.; GeurtsvanKessel, C.H.; Haanen, J.B.; Wörmann, B.; Turajlic, S.; von Lilienfeld-Toal, M. COVID-19 vaccines in patients with cancer: Immunogenicity, efficacy and safety. Nat. Rev. Clin. Oncol. 2022, 19, 385–401. [Google Scholar] [CrossRef]
- Oosting, S.F.; van der Veldt, A.A.M.; GeurtsvanKessel, C.H.; Fehrmann, R.S.N.; van Binnendijk, R.S.; Dingemans, A.C.; Smit, E.F.; Hiltermann, T.J.N.; den Hartog, G.; Jalving, M.; et al. mRNA-1273 COVID-19 vaccination in patients receiving chemotherapy, immunotherapy, or chemoimmunotherapy for solid tumours: A prospective, multicentre, non-inferiority trial. Lancet Oncol. 2021, 22, 1681–1691. [Google Scholar] [CrossRef]
- Becerril-Gaitan, A.; Vaca-Cartagena, B.F.; Ferrigno, A.S.; Mesa-Chavez, F.; Barrientos-Gutiérrez, T.; Tagliamento, M.; Lambertini, M.; Villarreal-Garza, C. Immunogenicity and risk of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) infection after Coronavirus Disease 2019 (COVID-19) vaccination in patients with cancer: A systematic review and meta-analysis. Eur. J. Cancer 2022, 160, 243–260. [Google Scholar] [CrossRef]
- Liebers, N.; Speer, C.; Benning, L.; Bruch, P.M.; Kraemer, I.; Meissner, J.; Schnitzler, P.; Kräusslich, H.G.; Dreger, P.; Mueller-Tidow, C.; et al. Humoral and cellular responses after COVID-19 vaccination in anti-CD20-treated lymphoma patients. Blood 2022, 139, 142–147. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Parameter | Non-Vaccinated, n = 84 | Vaccinated, n = 49 | p-Value * | ||
|---|---|---|---|---|---|
| Vaccination status | 84/133 | 63% | 49/133 | 37% | |
| Gender (M/F), n (ratio) | 47/37 | 56%/44% | 34/15 | 69%/31% | 0.127 |
| Median age, years (range) | 58 | 19–85 | 65 | 24–85 | 0.060 |
| Cancer entities, n | n = 84 | n = 49 | |||
| Solid tumors, n (%) | 42/84 | 50% | 17/49 | 35% | 0.088 |
| Lung cancer Breast cancer Gastrointestinal cancer Sarcoma Gynecologic cancer Endocrine cancer Brain cancer Melanoma Urogenital cancer Ear, nose, and throat carcinoma | 11 8 8 4 2 3 1 1 3 1 | 13% 10% 10% 4% 2% 4% 1% 1% 4% 1% | 6 1 3 2 - 1 - - 3 1 | 13% 2% 6% 4% - 2% - - 6% 2% | |
| Hematologic malignancies, n (%) | 42/84 | 50% | 32/49 | 65% | 0.088 |
| Lymphoma -B-cell lymphoma -T-cell lymphoma Multiple myeloma Acute leukemia -ALL -AML Others | 28 27 1 2 11 6 5 1 | 33% 32% 1% 2% 14% 8% 6% 1% | 23 21 - - 7 2 5 2 | 47% 43% - - 14% 4% 10% 4% | |
| Cancer treatment preceding SARS-CoV-2 positivity, n (%) | 0.280 | ||||
| Cytostatic therapy -cytostatic agents only -combined with immunotherapy -combined with targeted therapy -combined with radiotherapy Immunotherapy -immunotherapy mono-regimen -combined with radiotherapy Targeted therapy Surgery Hormonal therapy Radiotherapy No therapy yet due to first diagnosis or “watch and wait” strategy Aftercare following systemic cancer treatment | 47 27 13 4 3 10 7 3 4 4 1 2 5 11 | 57% 32% 16% 5% 4% 12% 8% 4% 5% 5% 1% 2% 6% 12% | 21 6 11 2 2 1 1 - 6 2 - - 8 11 | 44% 13% 23% 4% 4% 2% 2% - 12% 4% - - 16% 22% | |
| Number of therapy lines at SARS-CoV-2 positivity, n (%) | 0.184 | ||||
| No therapy yet | 5 | 6% | 7 | 14% | |
| 1 therapy line | 38 | 46% | 23 | 48% | |
| 2 therapy lines | 21 | 25% | 7 | 14% | |
| 3 therapy lines | 4 | 5% | 4 | 8% | |
| ≥4 therapy lines | 16 | 18% | 8 | 16% | |
| Remission status at SARS-CoV-2 positivity, n (%) | 0.169 | ||||
| Complete remission | 19 | 23% | 14 | 29% | |
| Partial remission | 16 | 19% | 14 | 29% | |
| Stable disease | 13 | 15% | 5 | 10% | |
| Relapsed/progressive disease | 25 | 30% | 6 | 12% | |
| Not yet assessed | 11 | 13% | 10 | 20% | |
| Comorbidities, n(%) | 61/84 | 73% | 40/49 | 82% | 0.245 |
| 1 comorbidity | 22 | 36% | 14 | 35% | |
| 2 comorbidities | 20 | 33% | 12 | 30% | |
| 3 comorbidities | 13 | 21% | 8 | 20% | |
| ≥4 comorbidities | 6 | 10% | 6 | 15% | |
| Parameter | Non-Vaccinated, n = 84 | Vaccinated, n = 49 | ||
|---|---|---|---|---|
| Median time from last cancer treatment to first positive SARS-CoV-2 RT-PCR test §, days | 13 | 19 | ||
| Patients with COVID-19 symptoms during the whole FU | 60/84 | 71% | 35/49 | 71% |
| COVID-19 symptoms (multiple answers possible), n (%) | 60/84 | 71% | 35/49 | 71% |
| Cough | 41/60 | 68% | 31/35 | 89% |
| Fever | 40/60 | 67% | 19/35 | 54% |
| Dyspnea | 35/60 | 58% | 14/35 | 40% |
| Gastrointestinal symptoms | 9/60 | 15% | 7/35 | 20% |
| Chest pain | 6/60 | 10% | 3/35 | 9% |
| Laboratory results at SARS-CoV-2 detection | ||||
| WBCs × 109/L, median (range) * | 5.7 | 0.3–42.9 | 5,4 | 0.4–47.6 |
| CRP, mg/dl, median (range) ** | 21. | 0.7–308 | 16 | 0.3–273 |
| PCT, ng/mL, median (range) *** | 0.17 | 0.0–84,3 | 0,1 | 0–3.1 |
| LDH, U/L, median (range) **** | 277 | 86–2830 | 292 | 125–2117 |
| Lymphocytopenia (<1.0 × 109/L) (data available for 46 unvaccinated and 15 vaccinated patients) | 20/46 | 43% | 8/15 | 53% |
| Chest imaging for diagnosing COVID-19, n (%) (data available for 77 unvaccinated and 42 vaccinated patients) multiple answers possible | ||||
| X-ray | 27/49 | 55% | 7/16 | 44% |
| CT | 31/49 | 63% | 9/16 | 56% |
| Ultrasound | 3/49 | 6% | - | - |
| Total number of patients underwent imaging for diagnosing COVID-19,n(%) | 49/77 | 64% | 16/42 | 38% |
| Imaging results,n(%) | ||||
| Signs of pneumonia | 32/49 | 65% | 10/16 | 63% |
| No indication of pneumonia | 17/49 | 35% | 6/16 | 37% |
| §Confirmed secondary bacterial infections in COVID-19 cases,n(%) | 12/84 | 14% | 7/49 | 14% |
| Parameter | Non-Vaccinated (n = 84) | Vaccinated (n = 49) | ||
|---|---|---|---|---|
| Severity of SARS-CoV-2 infection, n (%) | ||||
| Asymptomatic SARS-CoV-2 course | 24/84 | 29% | 14/49 | 29% |
| COVID-19 -mild course -severe course -critical course | 60 24/84 19/84 17/84 | 71% 29% 22% 20% | 35 24/49 9/49 2/49 | 71% 49% 18% 4% |
| Patient care, n (%) | ||||
| Outpatients | 29 | 35% | 14 | 29% |
| Inpatients -admitted because of COVID-19 symptoms -routine admission prior to positive SARS-CoV-2 test, of them: -admission of asymptomatic SARS-CoV-2 cases for observation/ therapy | 55/84 33/84 18/84 4/84 | 65% 39% 21% 5% | 35/49 25/49 5/49 5/49 | 71% 51% 10% 10% |
| Requiring wards during hospitalization, n (%) | 55/84 | 65% | 35/49 | 71% |
| General ward | 38/55 | 69% | 31/35 | 89% |
| IMC/ICU | 17/55 | 31% | 4/35 | 11% |
| Non- and invasive respiratory support, n (%) | 13/55 | 24% | 4/35 | 14% |
| Non-invasive respiratory support -high-flow oxygen -non-invasive mechanical ventilation Invasive mechanical ventilation | 8/55 6/55 2/55 5/55 | 15% 11% 4% 9% | 2/35 2/35 - 2/35 | 7% 7% - 7% |
| Median length of hospital stay of patients admitted because of COVID-19, days, range | 11 | 1–100 | 5 | 1–33 |
| Treatment modalities related to SARS-CoV-2 infection, n (%) among data available for 81/84 unvaccinated and 47/49 vaccinated patient, (multiple answers possible) | ||||
| No therapy at all | 24/81 | 30% | 9/47 | 19% |
| Symptomatic therapy only | 19/81 | 23% | 12/47 | 26% |
| Specific COVID-19 therapy | 38/81 | 47% | 26/47 | 55% |
| -virostatics: remdesevir, molnupiravir -dexamethasone Antibody-based therapy -anti-IL-6 receptor/anti-IL-6 antibody -convalescent plasma -antibody against spike protein JAK-Inhibitor/ serine protease inhibitors | 10/38 4/38 20/38 2/38 8/38 10/38 1/38 | 26% 11% 52% 5% 21% 26% 3% | 4/26 5/26 20/26 - - 20/26 1/26 | 15% 19% 77% - - 77% 4% |
| Antibiotic therapy | 23/38 | 61% | 3/26 | 12% |
| Treatment delay due to SARS-CoV-2 among 69/84 unvaccinated and 34/49 vaccinated patients with ongoing or planned cancer therapy before, n (%) | 58/69 | 84% | 22/34 | 65% |
| Median time from SARS-CoV-2 diagnosis to restart of therapy | 26 | 0–70 | 12 | 0–56 |
| Median time from SARS-CoV-2 detection to last follow-up, weeks, range within both groups | 5 (0–62) | |||
| Remission status at last follow-up, n (%) ** | ||||
| Complete remission | 22 | 26% | 11 | 25% |
| Partial remission | 16 | 19% | 15 | 34% |
| Stable disease | 24 | 29% | 10 | 23% |
| Relapse/progressive disease | 22 | 26% | 8 | 18% |
| Survival status at last follow-up, n (%) | ||||
| Alive | 65 | 77% | 46 | 94% |
| Dead | 19 | 23% | 3 | 6% |
| Causes of death | ||||
| COVID-19 | 10/84 | 12% | 1/49 | 2% |
| Relapsed/refractory malignancy | 9/84 | 11% | 2/49 | 4% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shumilov, E.; Aperdannier, L.; Schmidt, N.; Szuszies, C.; Neesse, A.; Hoffknecht, P.; Khandanpour, C.; Mikesch, J.-H.; Stelljes, M.; Boeckel, G.R.; et al. Clinical Post-SARS-CoV-2 Infection Scenarios in Vaccinated and Non-Vaccinated Cancer Patients in Three German Cancer Centers: A Retrospective Analysis. Cancers 2022, 14, 3746. https://doi.org/10.3390/cancers14153746
Shumilov E, Aperdannier L, Schmidt N, Szuszies C, Neesse A, Hoffknecht P, Khandanpour C, Mikesch J-H, Stelljes M, Boeckel GR, et al. Clinical Post-SARS-CoV-2 Infection Scenarios in Vaccinated and Non-Vaccinated Cancer Patients in Three German Cancer Centers: A Retrospective Analysis. Cancers. 2022; 14(15):3746. https://doi.org/10.3390/cancers14153746
Chicago/Turabian StyleShumilov, Evgenii, Lena Aperdannier, Nicole Schmidt, Christoph Szuszies, Albrecht Neesse, Petra Hoffknecht, Cyrus Khandanpour, Jan-Henrik Mikesch, Matthias Stelljes, Göran Ramin Boeckel, and et al. 2022. "Clinical Post-SARS-CoV-2 Infection Scenarios in Vaccinated and Non-Vaccinated Cancer Patients in Three German Cancer Centers: A Retrospective Analysis" Cancers 14, no. 15: 3746. https://doi.org/10.3390/cancers14153746