
Sarcopenia as a Predictor of Short- and Long-Term Outcomes in Patients Surgically Treated for Malignant Pleural Mesothelioma

 , ,
, ,  ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
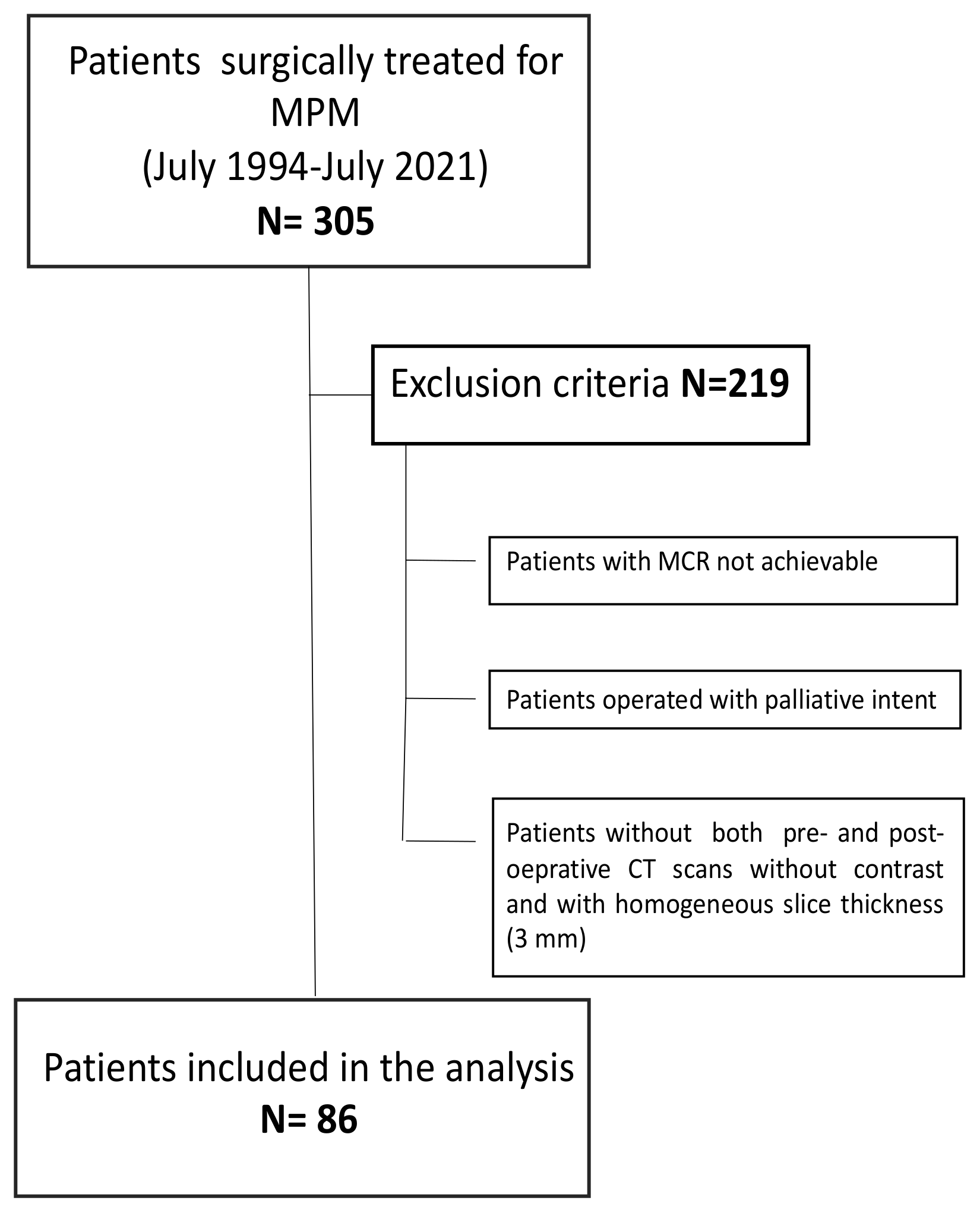
2.1. Study Population
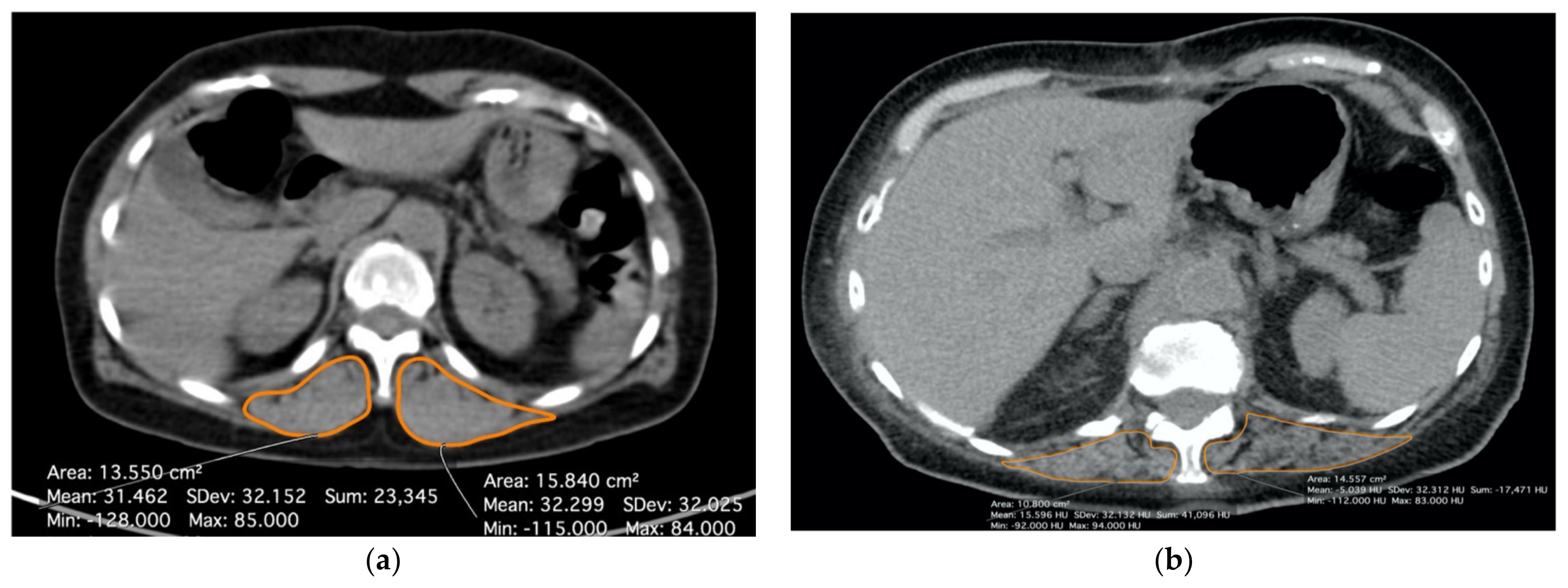
2.2. Radiological Evaluation of the Sarcopenia
2.3. Statistical Analysis
3. Results
3.1. Demographic and Clinical Data
3.2. Post-Operative Outcomes
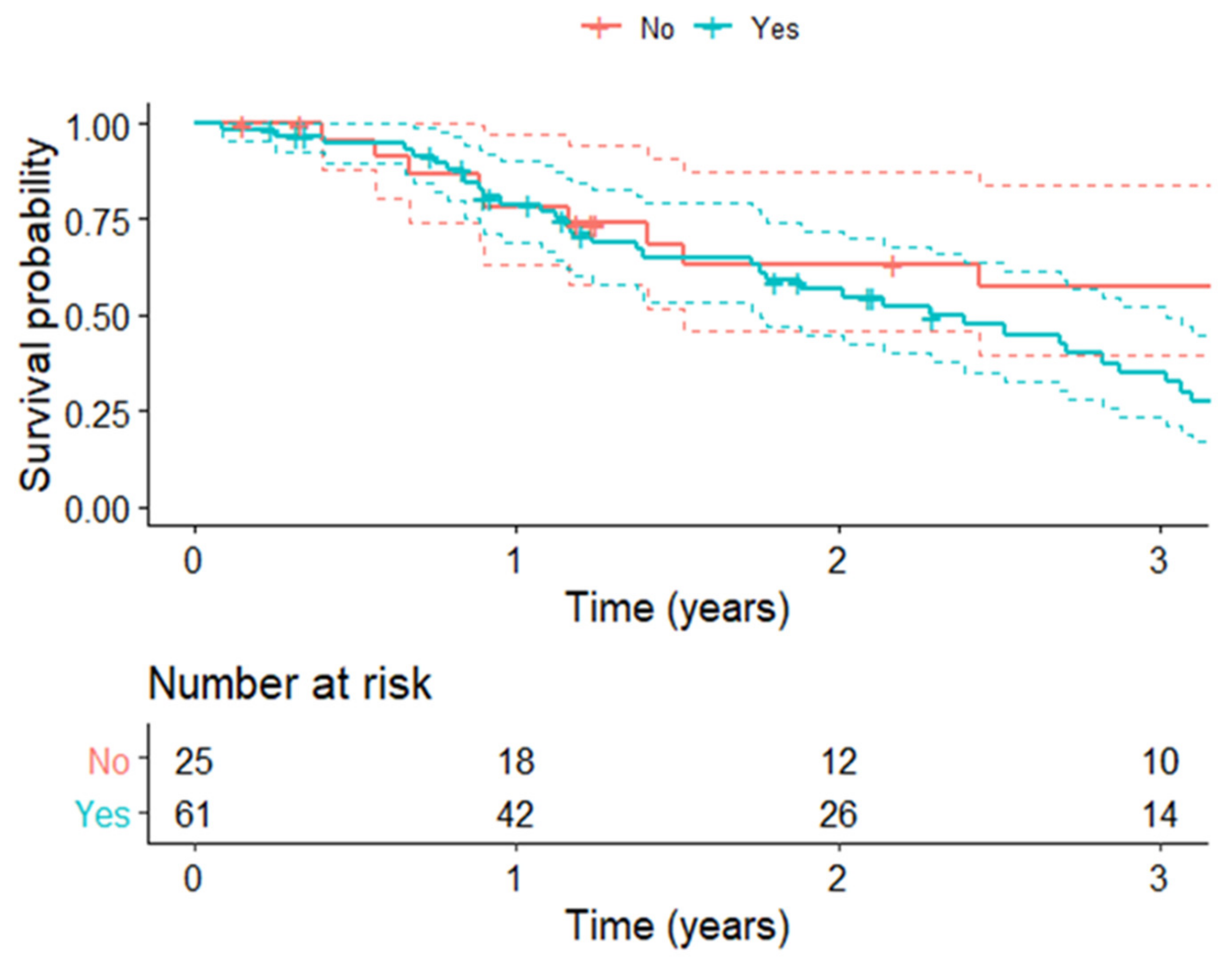
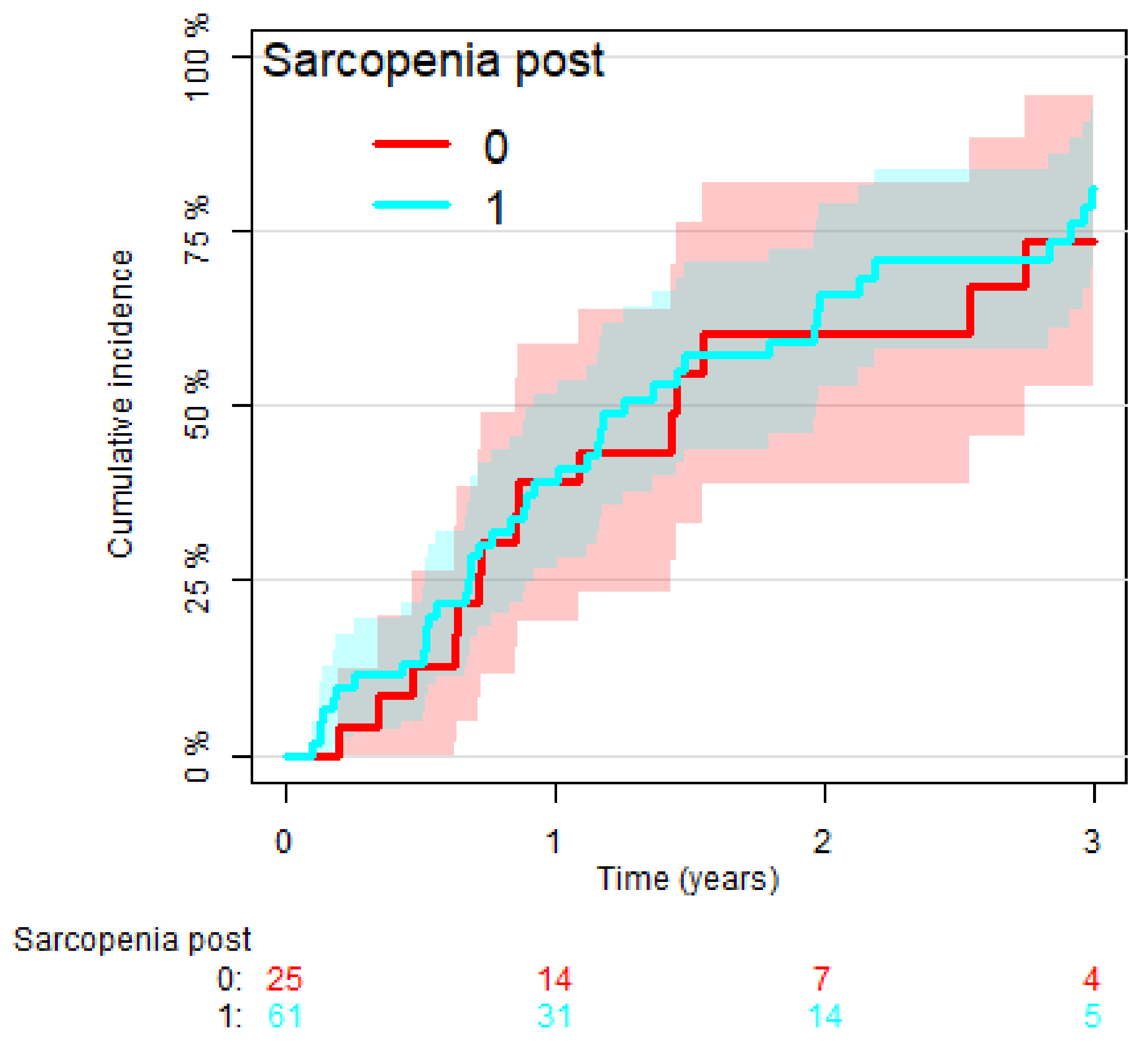
3.3. Analysis of Overall Survival and Cumulative Incidence of Relapse
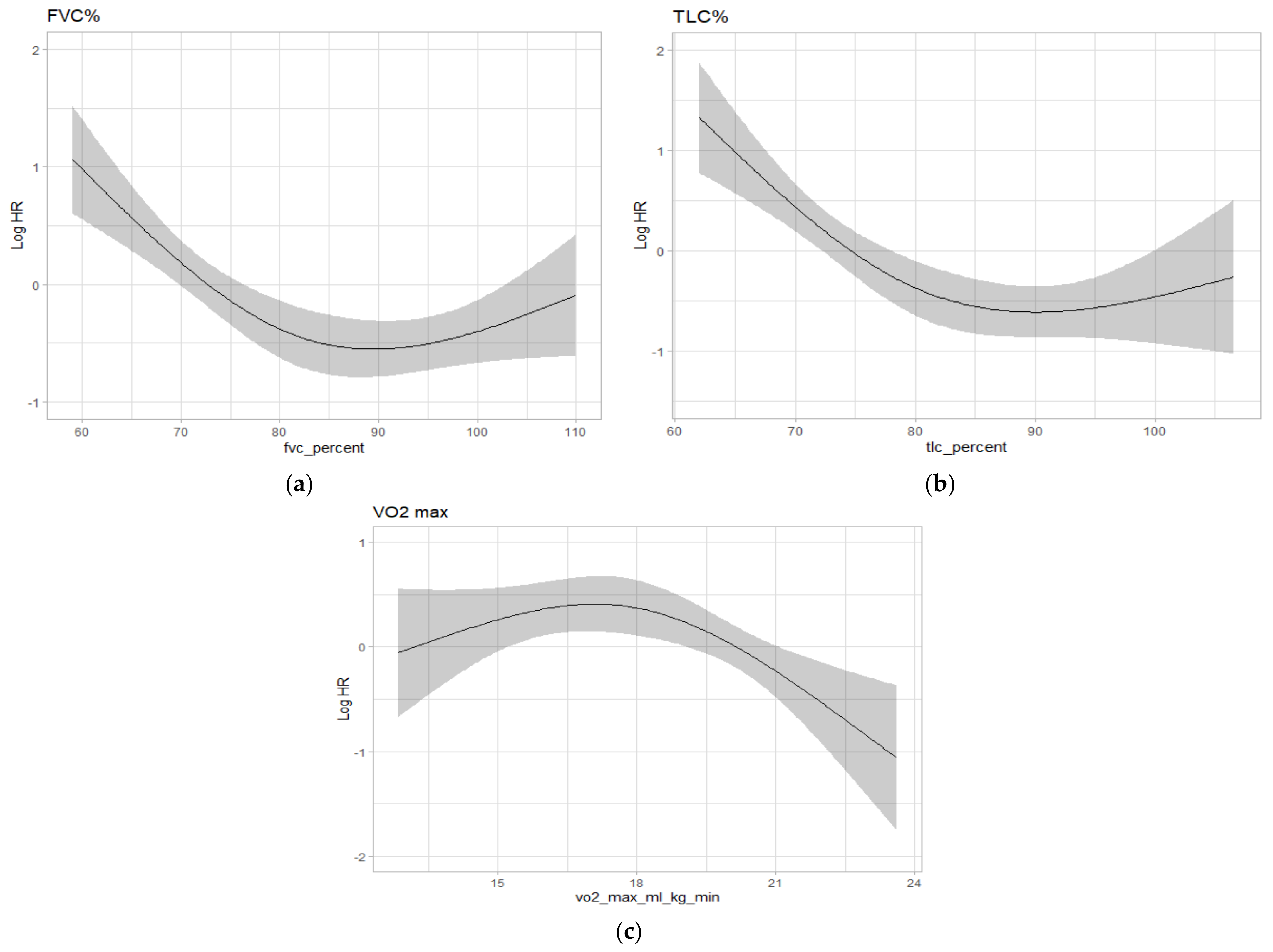
3.4. Analysis of Pre-Operative Pulmonary Function
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Opitz, I.; Scheerpereel, A.; Berghmans, T.; Psallidas, I.; Glatzer, M.; Rigau, D.; Astoul, P.; Bolukbas, S.; Boyd, J.; Coolen, J.; et al. ERS/ESTS/EACTS guidelines for the management of malignant pleural mesothelioma. Eur. Respir. J. 2020, 55, 1900953. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayeer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cruz-Jentoft, A.J.; Bayens, J.P.; Bauer, J.M.; Bahat, G.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.P.; Rolland, Y.; et al. Sarcopenia: European Consensus on definition and diagnosis: Report of the European Working Group on sarcopenia in older people. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef] [Green Version]
- Kawamura, T.; Makuuchi, R.; Tokunaga, M.; Tanizawa, Y.; Bando, E.; Yasui, H.; Aoyama, T.; Inano, T.; Terashima, M. Long-term outcomes of gastric cancer patients with preoperative sarcopenia. Ann. Surg. Oncol. 2018, 25, 1625–1632. [Google Scholar] [CrossRef]
- Vergara-Fernandez, O.; Trejo-Avila, M.; Salgado-Nesme, N. Sarcopenia in patients with colorectal cancer. A comprehensive review. World J. Clin. Cases 2020, 8, 1188–1202. [Google Scholar] [CrossRef]
- El Amrani, M.; Vermersch, M.; Fullbert, M.; Prodeau, M.; Lecolle, K.; Hebbar, M.; Ernst, O.; Pruvot, F.R.; Truant, S. Impact of sarcopenia on outcomes of patients undergoing pancreatectomy. Medicine 2018, 97, e12076. [Google Scholar] [CrossRef]
- Fujiwara, N.; Nakagawa, H.; Kudo, Y.; Tateishi, R.; Taguri, M.; Watadani, T.; Nakagomi, R.; Kondo, M.; Nakatsuka, T.; Minami, T.; et al. Sarcopenia, intramuscolar fat deposition and visceral adiposity indipendently predict the outcome of hepatocellular carcinoma. J. Hepatol. 2015, 63, 131–140. [Google Scholar] [CrossRef] [Green Version]
- Kuroki, L.M.; Mangano, M.; Allsworth, J.E.; Menias, C.O.; Massad, L.S.; Powell, M.A.; Mutch, D.G.; Thaker, P.H. Pre-operative assessment of muscle mass to predict surgical complications and prognosis in patients with endometrial cancer. Ann. Surg. Oncol. 2015, 22, 972–979. [Google Scholar] [CrossRef] [Green Version]
- Noguchi, G.; Kawahara, T.; Kobayashi, K.; Tsutsumi, S.; Ohtake, S.; Osaka, K.; Umemoto, S.; Nakaigawa, N.; Uemura, H.; Kishida, T.; et al. A lower psoas muscle volume was associated with a higher rate of recurrence in male clear cell renal cell carcinoma. PLoS ONE 2020, 2, e0226581. [Google Scholar] [CrossRef] [Green Version]
- Shinohara, S.; Otsuki, R.; Kobayashi, K.; Sugaya, M.; Matsuo, M.; Nakagawa, M. Impact of sarcopenia on surgical outcomes in non-small cell lung cancer. Ann. Surg. Oncol. 2020, 27, 2427–2435. [Google Scholar] [CrossRef]
- Nikkuni, E.; Hirama, T.; Hayasaka, K.; Kumata, S.; Kotan, S.; Watanabe, Y.; Oishi, H.; Niikawa, H.; Kohzuki, M.; Okada, Y. Recovery physical function in lung transplant recipients with sarcopenia. BMC Pulm. Med. 2021, 21, 124. [Google Scholar] [CrossRef]
- Lee, S.; Paik, H.C.; Haam, S.J.; Lee, C.Y.; Nam, K.S.; Jung, H.S.; Do, Y.W.; Shu, J.W.; Lee, J.G. Sarcopenia of thoracic muscle mass is not a risk factor for survival in lung transplant recipients. J. Thorac. Dis. 2016, 8, 2011–2017. [Google Scholar] [CrossRef] [Green Version]
- Rozenberg, D.; Wickerson, L.; Singer, L.G.; Mathur, S. Saropenia in lung transplantation: A systematic review. J. Heart Lung Transplant. 2014, 33, 1203–1212. [Google Scholar] [CrossRef]
- Goodpaster, B.H.; Thaete, F.L.; Kelley, D.E. Composition of skeletal muscle evaluated with computed tomography. Ann. N. Y. Acad. Sci. 2000, 904, 18–24. [Google Scholar] [CrossRef]
- Aubrey, J.; Esfandiari, N.; Baracos, V.E.; Buteau, F.A.; Frenette, J.; Putman, C.T.; Mazurak, V.C. Measurement of skeletal muscle radiation attenuation and basis of its biological variation. Acta Physiol. 2014, 210, 489–497. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.; Kuk, J.L.; Davidson, L.E.; Hudson, R.; Kilpatrick, K.; Graham, T.E.; Ross, R. Exercise without weight loss is an effective strategy for obesity reduction in obese individuals with and without type II diabetes. J. Appl. Physiol. 2005, 99, 1220–1225. [Google Scholar] [CrossRef]
- Kim, E.Y.; Kim, Y.J.; Kim, Y.S.; Kim, K.W.; Jeon, J.Y.; Kim, K.G. Prognostic significance of radiodensity-based skeletal muscle quantification using preoperative CT in resected non-small cell lung cancer. J. Thorac. Dis. 2021, 13, 754–761. [Google Scholar] [CrossRef]
- Jeffrey, E.; Gary Lee, E.C.; Newton, R.U.; Lyons-Wall, P.; McVeigh, J.; Nowak, A.K.; Cheah, H.M.; Nguyen, B.; Fitzgerald, D.B. Body composition and nutritional status in malignant pleural mesothelioma: Implications for activity levels and qaulity of life. Eur. J. Clin. Nutr. 2019, 73, 1412–1421. [Google Scholar] [CrossRef]
- Boutin, R.D.; Kaptuch, J.M.; Bateni, C.P.; Chalfant, J.S.; Yao, L. Influence of IV contrast administration on CT measures of muscle and bone attenuation: Implications for sarcopenia and osteoporosis evaluation. Am. J. Roentgenol. 2016, 207, 1046–1054. [Google Scholar] [CrossRef]
- Derstine, B.A.; Holcombe, S.A.; Goulson, R.L.; Ross, B.E.; Wang, N.C.; Sullivan, G.A.; Su, G.L.; Wang, S.C. Quantifying sarcopenia reference using lumbar and thoracic muscle areas in a healthy population. J. Nutrit. Health Aging 2017, 21, 180–185. [Google Scholar] [CrossRef] [PubMed]
- Giraudo, C.; Librizzi, G.; Fichera, G.; Motta, R.; Balestro, E.; Calabrese, F.; Carretta, G.; Cattelan, A.M.; Navalesi, P.; Pelloso, M.; et al. Reduced muscle mass as a predictor of intensive care unit hospitalization in COVID-19 patients. PLoS ONE 2021, 16, e0253433. [Google Scholar] [CrossRef] [PubMed]
- De Jong, C.; Chargi, N.; Herder, G.J.M.; Van Harleem, S.W.A.; Van der Meer, F.; Van Lindert, A.S.R.; Ten Heuvel, A.; Brouwer, J.; De Jong, P.A.; Devriese, L.A.; et al. The association between skeletal muscle measures and chemotherapy-induced toxicity in non-small cell lung cancer patients. J. Cachexia Sarcopenia Muscle 2022, 13, 1554–1564. [Google Scholar] [CrossRef] [PubMed]
- Cattikas, N.M.; Bahat, Z.; Orven, M.M.; Bahat, G. Older cancer patients receiveing radiotherapy: A systematic review for the role of sarcopenia in treatment outcomes. Aging Clin. Exp. Res. 2022, 34, 1747–1759. [Google Scholar] [CrossRef] [PubMed]
- Sachar, S.S.; Williams, G.R.; Muss, H.B.; NishijimaT, F. Prognostic value of sarcopenia in adults with solid tumors: A meta-analysis and systematic review. Eur. J. Cancer 2016, 57, 58–67. [Google Scholar] [CrossRef]
- Agalar, C.; Sokmen, S.; Arslan, C.; Altay, C.; Basara, I.; Canda, A.E.; Obuz, F. The impact of sarcopenia on morbidity and long-term survival among patients with peritoneal metastases of colorectal origin treated with cytoreductive surgery and hypertermic intraperitoneal chemotherapy: A 10-year longitudinal analysis of a single-center experience. Tech. Coloproctol. 2020, 24, 301–308. [Google Scholar]
- Neto, N.I.P.; Murari, A.S.P.; Oyama, L.M.; Otoch, J.P.; Alcantara, P.S.M.; Tokeshi, F.; Figuredo, R.G.; Joana Alves, M.; Correia Lima, J.D.C.; Marques de Matos-Neto, E.; et al. Peritumoral adipose tissue pro-inflammattory cytokines are associated with tumoral growth factors in cancer cachexia patients. J. Cachexia Sarcopenia Muscle 2018, 9, 1101–1108. [Google Scholar] [CrossRef] [Green Version]
- Clavien, P.A.; Barkun, J.; De Oliveira, M.L.; Vauthey, J.N.; Dindo, D.; Schulick, R.D.; De Santibanes, E.; Pekolj, J.; Slankamenac, K.; Bassi, C. The Clavien-Dindo classification of surgical complications: Five-year experience. Ann. Surg. 2009, 250, 187–196. [Google Scholar] [CrossRef] [Green Version]
- Nakamura, R.; Inage, Y.; Tobita, R.; Yoneyama, S.; Numata, T.; Oto, K.; Yanai, H.; Endo, T.; Inadome, Y.; Sakashita, S.; et al. Sarcopenia in resected NSCLC: Effect on post-operative outcomes. J. Thorac. Oncol. 2018, 13, 895–903. [Google Scholar] [CrossRef] [Green Version]
- Nagano, A.; Wakabayashi, H.; Maeda, K.; Kohura, Y.; Miyazaki, S.; Mori, T.; Fujiwara, D. Respiratory sarcopenia and sarcopenic respiratory disability: Concepts, diagnosis and treatment. J. Nutr. Health Aging 2021, 25, 507–515. [Google Scholar] [CrossRef]
- Sawaya, Y.; Shiba, T.; Ishizaka, M.; Hirose, T.; Sato, R.; Kubo, A.; Urano, T. Sarcopenia is not associated with inspiratory muscle sternght but with expiratory muscle strenght among older adults requiring long-term carae/support. Peer J. 2022, 10, e12958. [Google Scholar] [CrossRef]
- Verhoek, O.G.; Jungblut, L.; Lauk, O.; Opitz, I.; Frauenfelder, T.; Martini, K. Sarcopenia, precardial adipose tissue, and high tumor volume as outcome predictors in surgically treated pleural mesothelioma. Diagnostics 2022, 12, 99. [Google Scholar] [CrossRef]
- Nakano, T.; Chahinian, A.P.; Shinjo, M.; Tonomura, A.; Miyake, M.; Togawa, N.; Ninomiya, K.; Higashino, K. Interleukin 6 and its relationship to clinical parameters in patients with malignant pleural mesothelioma. Br. J. Cancer 1998, 77, 907–912. [Google Scholar] [CrossRef] [Green Version]
- Ghanim, B.; Hoda, M.A.; Winter, M.P.; Klikovits, T.; Alimohammadi, A.; Hegedus, B.; Dome, B.; Grusch, M.; Arns, M.; Schenk, P.; et al. Pretreatment serum C-reactive proteinlevels predict benefit from multimodal treatment including radical surgery in malignant pleural mesothelioma: A retrospective multicenter analysis. Ann. Surg. 2012, 256, 357–362. [Google Scholar] [CrossRef]
- Ghanim, B.; Hoda, M.A.; Klikovits, T.; Winter, M.P.; Alimohammadi, A.; Grusch, M.; Dome, B.; Arns, M.; Schenk, P.; Jakopovic, M.; et al. Circulating fibrinogen is a prognostic and predictive biomarker in malignant pleural mesothelioma. Br. J. Cancer 2014, 18, 984–990. [Google Scholar] [CrossRef] [Green Version]
- Greb, D.; Hebeisen, M.; Matter, A.; Opitz, I.; Lauk, O. Prospective validation d extension of the multimodality prognostic score for the treatment allocation of pleural mesothelioma patients. Eur. J. Cardiothor. Surg. 2022, 62, ezac085. [Google Scholar] [CrossRef]
- Takamori, S.; Toyokawa, G.; Shimokawa, M.; Kinoshita, F.; Kozuma, Y.; Matsubara, T.; Haratake, N.; Akamine, T.; Hirai, F.; Seto, T.; et al. The C-reactive protein/albumin ratio is a novel significant prognostic factor in malignant pleural mesothelioma: A retrospective multi-institutional study. Ann. Surg. Oncol. 2018, 25, 1555–1563. [Google Scholar] [CrossRef]
- Chen, N.; Liu, S.; Huang, L.; Li, W.; Yang, W.; Cong, T.; Ding, L.; Qiu, M. Prognostic significance of neutrophil-to-lymphoccyte ratio in patients with malignant pleural mesothelioma: A meta-analysis. Oncotarget 2017, 8, 57460–57469. [Google Scholar] [CrossRef] [Green Version]
- Pinato, D.J.; Mauri, F.A.; Ramakrishnan, R.; Wahab, L.; Lloyd, T.; Sharma, R. Inflammation-based prognostic indeces in malignant pleural mesothelioma. J. Thorac. Oncol. 2012, 7, 587–594. [Google Scholar] [CrossRef] [Green Version]
- Leon-Idougourram, S.; Perez-Gomez, J.M.; Munoz Jimenez, C.; L-Lopez, F.; Manzano Garcia, G.; Molina Puertas, M.J.; Herman-Sanchez, N.; Alonso-Echague, R.; Calanas Continente, A. Morphofunctional and molecular assessment of nutritional status in head and neck cancer patients undergoing systemic treatment: Role of inflammasone and clinical nutrition. Cancers 2022, 14, 494. [Google Scholar] [CrossRef]
- Linton, A.; van Zandwijk, N.; Reid, G.; Clarke, S.; Cao, C.; Kao, S. Inflammation in malignant plerual mesothelioma-friend or foe? Ann. Cardiothorac. Surg. 2012, 1, 516–522. [Google Scholar]
- Vogl, M.; Rosenmayr, A.; Bohanes, T.; Scheed, A.; Brndiar, M.; Stubenberger, E.; Ghanim, B. Biomarkers for malignant pleural mesothelioma—A novel view on inflammation. Cancers 2021, 3, 658. [Google Scholar] [CrossRef]
- Hacker, U.T.; Hasenclever, D.; Baber, R.; Linder, N.; Busse, H.; Obermannova, R.; Zdrazilova-Dubska, L.; Valik, D.; Lordick, F. Modified Glasgow prognostic score (mGPS) is correlated with sarcopenia and dominates the prognostic role of baseline body composition parameters in advanced gastric and esophagogastric junction cancer patients undergoing first-line treatment form the phase III EXPAND trial. Ann. Oncol. 2022, 33, 685–692. [Google Scholar]
- Mansfield, A.S.; Brown, R.J.; Sammon, C.; Daumont, M.J.; McKenna, M.; Sanzari, J.K.; Forde, P.M. The predictive and prognostic nature of programme death-ligand 1 in malignant pleural mesothelioma: A systematic literature review. JTO Clin. Res. Rep. 2022, 3, 100315. [Google Scholar]
- McGovern, J.; Dolan, R.D.; Horgan, P.G.; Laird, B.J.; McMillan, D.C. Computed tomography-defined low skeletal muscle index and density in cancer patients: Observation from a systematic review. J. Cachexia Sarcopenia Muscle 2021, 12, 1408–1417. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Overall (n = 86) |
|---|---|
| Age (years) | 66 (62–71) |
| Sex | |
| F | 21 (24%) |
| M | 65 (76%) |
| Smoker | |
| No | 34 (40%) |
| Yes | 10 (12%) |
| Former | 42 (48%) |
| Asbestos exposure | |
| No | 34 (39.5%) |
| Yes | 52 (60.5%) |
| Surgery-side | |
| Right | 56 (65%) |
| Left | 30 (35%) |
| Type of surgery | |
| PD/EPD | 62 (72%) |
| EPP | 24 (28%) |
| Post-operative histology | |
| Epithelioid | 68 (79%) |
| Biphasic | 16 (19%) |
| Desmoid | 2 (2%) |
| Neo-adjuvant CT | |
| Yes | 86 (100%) |
| No | 0 (0%) |
| Adjuvant RT | |
| Yes | 72 (84%) |
| No | 14 (16%) |
| pTNM (8th edition) | |
| Ia | 5 (6%) |
| Ib | 43 (50%) |
| II | 8 (9%) |
| IIIa | 10 (12%) |
| IIIb | 0 (0%) |
| IV | 16 (19%) |
| Is | 1 (1%) |
| CR | 3 (3%) |
| Pre-op FVC (% predicted) | 81 (70–92) |
| Pre-op FEV1 (% predicted) | 82 (74–92) |
| Pre-op TLC (% predicted) | 79 (71–88) |
| Pre-op DLCO (% predicted) | 66 (60–78) |
| Pre-op VO2max (mL/Kg/min) | 17.9 (16.5–20.7) |
| Pre-op BMI (Kg/m2) | 26.1 (24.5–28.4) |
| Pre-operative sarcopenia | |
| Yes (<30 HU) | 57 (66%) |
| No (>30 HU) | 29 (34%) |
| Pre-op paravertebral muscle density (HU) | 27 (21–34) |
| Post-operative sarcopenia | |
| Yes (<30 HU) | 63 (74%) |
| No (>30 HU) | 23 (26%) |
| Post-op paravertebral muscle density (HU) | 25 (17–30) |
| Overall Survival (months) | 21 (11–38) |
| Disease-free survival (months) | 13 (7–24) |
| Variable | Pre-Op Sarcopenia (n = 57) | No Sarcopenia (n = 29) | p Value |
|---|---|---|---|
| Age (years) | 67 (63–71) | 64 (57–67) | 0.022 |
| Sex | 0.3 | ||
| F | 16 (28%) | 5 (17%) | |
| M | 41 (72%) | 24 (83%) | |
| Smoker | 0.5 | ||
| No | 22 (39%) | 12 (41%) | |
| Yes | 4 (7%) | 4 (15%) | |
| Former | 31 (54%) | 13 (44%) | |
| Asbestos exposure | 0.037 | ||
| No | 17 (30%) | 17 (58%) | |
| Yes | 40 (70%) | 12 (42%) | |
| Surgery side | 0.4 | ||
| Right | 39 (68%) | 17 (59%) | |
| Left | 18 (32%) | 12 (41%) | |
| Type of surgery | 0.14 | ||
| PD/EPD | 44 (77%) | 18 (62%) | |
| EPP | 13 (23%) | 11 (38%) | |
| Neo-adjuvant CT | - | ||
| Yes | 57 (100%) | 29 (100%) | |
| No | 0 (0%) | 0 (0%) | |
| Adjuvant RT | 0.5 | ||
| Yes | 47 (83%) | 26 (90%) | |
| No | 10 (17%) | 3 (10%) | |
| pTNM (8th edition) | 0.3 | ||
| Ia | 5 (9%) | 0 (0%) | |
| Ib | 28 (49%) | 15 (52%) | |
| II | 6 (10%) | 2 (7%) | |
| IIIa | 5 (9%) | 5 (17%) | |
| IIIb | 0 (0%) | 0 (0%) | |
| IV | 9 (16%) | 7 (24%) | |
| Is | 1 (2%) | 0 (0%) | |
| CR | 3 (5%) | 0 (0%) | |
| Pre-op FVC (% predicted) | 82 (70–91) | 78 (70–94) | 0.6 |
| Pre-op FEV1 (% predicted) | 84 (73–92) | 82 (75–94) | 0.7 |
| Pre-op TLC (% predicted) | 80 (72–88) | 78 (70–84) | 0.4 |
| Pre-op DLCO (% predicted) | 66 (59–78) | 68 (62–77) | 0.6 |
| Pre-op VO2max (mL/Kg/min) | 17.4 (16.6–20.2) | 19.5 (16.3–21.1) | 0.2 |
| Pre-op BMI (Kg/m2) | 26.7 (24.7–28.7) | 25.8 (24.5–26.7) | 0.2 |
| Pre-op paravertebral muscle density (HU) | 24 (17–27) | 38 (34–41) | <0.001 |
| Variable | Post-Op Sarcopenia (n = 61) | No Sarcopenia (n = 25) | p Value |
|---|---|---|---|
| Age (years) | 68 (64–73) | 64 (58–70) | 0.0014 |
| Sex | 0.3 | ||
| F | 17 (28%) | 5 (20%) | |
| M | 44 (72%) | 20 (80%) | |
| Smoker | 0.059 | ||
| No | 27 (44%) | 9 (35%) | |
| Yes | 2 (3%) | 5 (19%) | |
| Former | 32 (53%) | 11 (46%) | |
| Asbestos exposure | 0.2 | ||
| No | 20 (32%) | 17 (49%) | |
| Yes | 41 (68%) | 18 (51%) | |
| Surgery side | 0.3 | ||
| Right | 43 (70%) | 15 (59%) | |
| Left | 18 (30%) | 10 (41%) | |
| Type of surgery | 0.6 | ||
| PD/EPD | 45 (74%) | 17 (69%) | |
| EPP | 16 (26%) | 8 (31%) | |
| Neo-adjuvant CT | - | ||
| Yes | 61 (100%) | 25 (100%) | |
| No | 0 (0%) | 0 (0%) | |
| Adjuvant RT | 0.3 | ||
| Yes | 50 (82%) | 22 (89%) | |
| No | 11 (18%) | 3 (11%) | |
| pTNM (8th edition) | 0.3 | ||
| Ia | 7 (11%) | 0 (0%) | |
| Ib | 30 (50%) | 13 (51%) | |
| II | 7 (11%) | 2 (8%) | |
| IIIa | 7 (11%) | 3 (13%) | |
| IIIb | 0 (0%) | 0 (0%) | |
| IV | 8 (13%) | 6 (23%) | |
| Is | 0 (0%) | 1 (5%) | |
| CR | 2 (4%) | 0 (0%) | |
| Pre-op FVC (% predicted) | 80 (70–87) | 81 (70–98) | 0.6 |
| Pre-op FEV1 (% predicted) | 83 (73–90) | 82 (75–97) | 0.5 |
| Pre-op TLC (% predicted) | 80 (70–87) | 79 (74–88) | >0.9 |
| Pre-op DLCO (% predicted) | 66 (54–77) | 68 (61–82) | 0.3 |
| Pre-op VO2 max (mL/Kg/min) | 17.3 (16.6–20.4) | 18.8 (16.6–20.4) | 0.2 |
| Pre-op BMI (Kg/m2) | 26.2 (24.3–28.4) | 25.9 (24.7–28.4) | 0.2 |
| Pre-op paravertebral muscle density (HU) | 21 (16–27) | 34 (30–41) | <0.001 |
| Variable | Pre-Op Sarcopenia (n = 57) | No Sarcopenia (n = 29) | p Value |
|---|---|---|---|
| Length of hospital stay (d) | 14 (11–21) | 12 (10–20) | 0.9 |
| Post-operative complications | 0.04 | ||
| Yes | 37 (65%) | 12 (41%) | |
| No | 20 (35%) | 17 (59%) | |
| Clavien–Dindo classification | 0.14 | ||
| 1 + 2 | 42 (73%) | 15 (51%) | |
| 3 + 4 + 5 | 15 (27%) | 14 (49%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Faccioli, E.; Terzi, S.; Giraudo, C.; Zuin, A.; Modugno, A.; Labella, F.; Zambello, G.; Lorenzoni, G.; Schiavon, M.; Gregori, D.; et al. Sarcopenia as a Predictor of Short- and Long-Term Outcomes in Patients Surgically Treated for Malignant Pleural Mesothelioma. Cancers 2022, 14, 3699. https://doi.org/10.3390/cancers14153699
Faccioli E, Terzi S, Giraudo C, Zuin A, Modugno A, Labella F, Zambello G, Lorenzoni G, Schiavon M, Gregori D, et al. Sarcopenia as a Predictor of Short- and Long-Term Outcomes in Patients Surgically Treated for Malignant Pleural Mesothelioma. Cancers. 2022; 14(15):3699. https://doi.org/10.3390/cancers14153699
Chicago/Turabian StyleFaccioli, Eleonora, Stefano Terzi, Chiara Giraudo, Andrea Zuin, Antonella Modugno, Francesco Labella, Giovanni Zambello, Giulia Lorenzoni, Marco Schiavon, Dario Gregori, and et al. 2022. "Sarcopenia as a Predictor of Short- and Long-Term Outcomes in Patients Surgically Treated for Malignant Pleural Mesothelioma" Cancers 14, no. 15: 3699. https://doi.org/10.3390/cancers14153699