
Factors Predicting Surgical Effort Using Explainable Artificial Intelligence in Advanced Stage Epithelial Ovarian Cancer

 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
- Patient: age, year of diagnosis, year of surgery, Eastern Co-operative Oncology Group (ECOG) performance status (PS), histology type, grade (low and high), and stage (FIGO 3 or 4), pre-treatment, and pre-surgery Ca125.
- Operative/tumor factors: timing of surgery (PDS or IDS), presence of ascites (yes/no), intra-operative blood transfusion (yes/no), site of intra-operative bulk of the disease, size of the largest bulk of the disease, PCI and intra-operative mapping of ovarian cancer (IMO).
- Human factors addressing surgical heuristics: age of consultant surgeon, years of experience as a consultant, volume case within the cohort, and training status, i.e., whether the consultant was trained within the institution or not.
3. Results
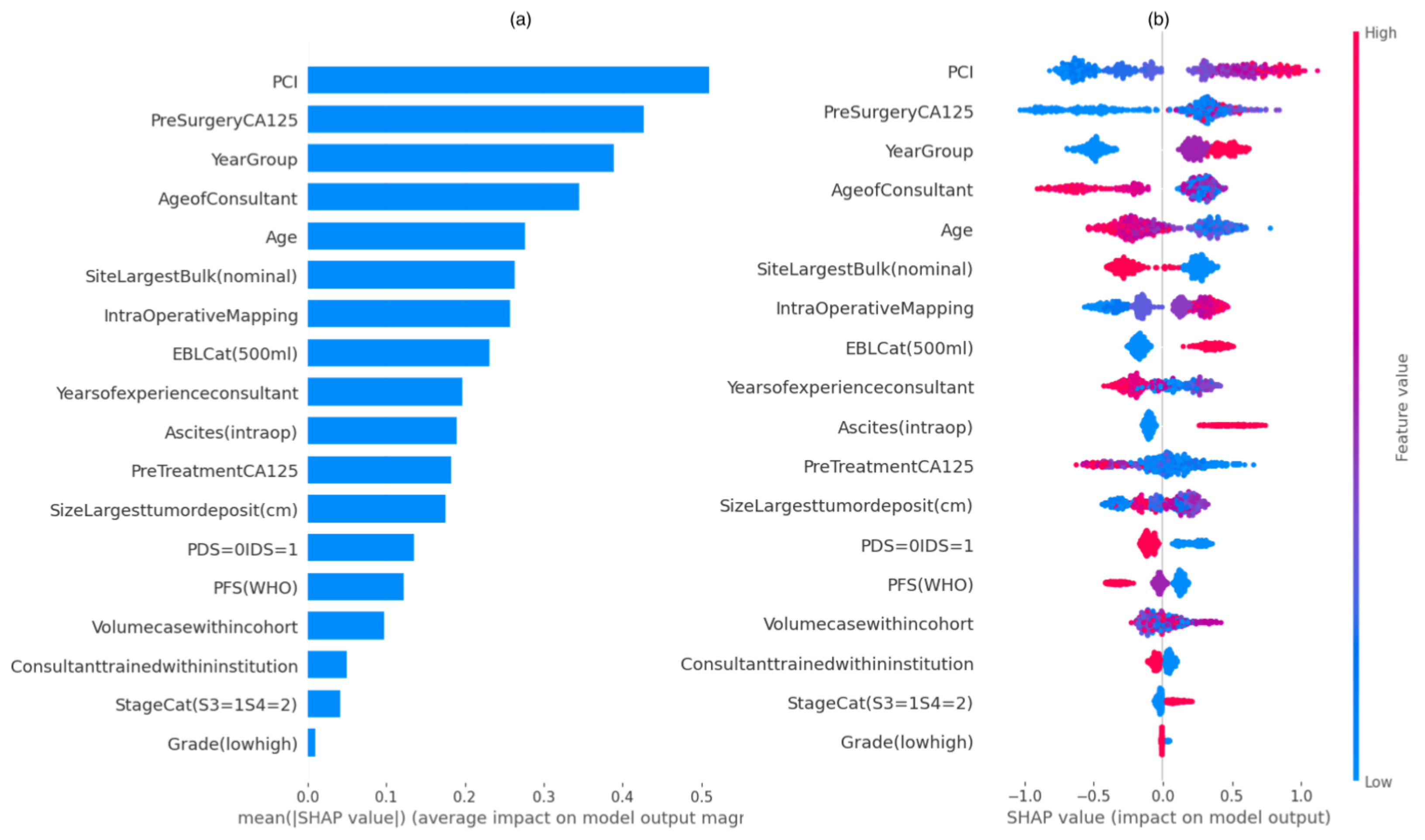
3.1. Feature Analysis
SHAP Summary Plots
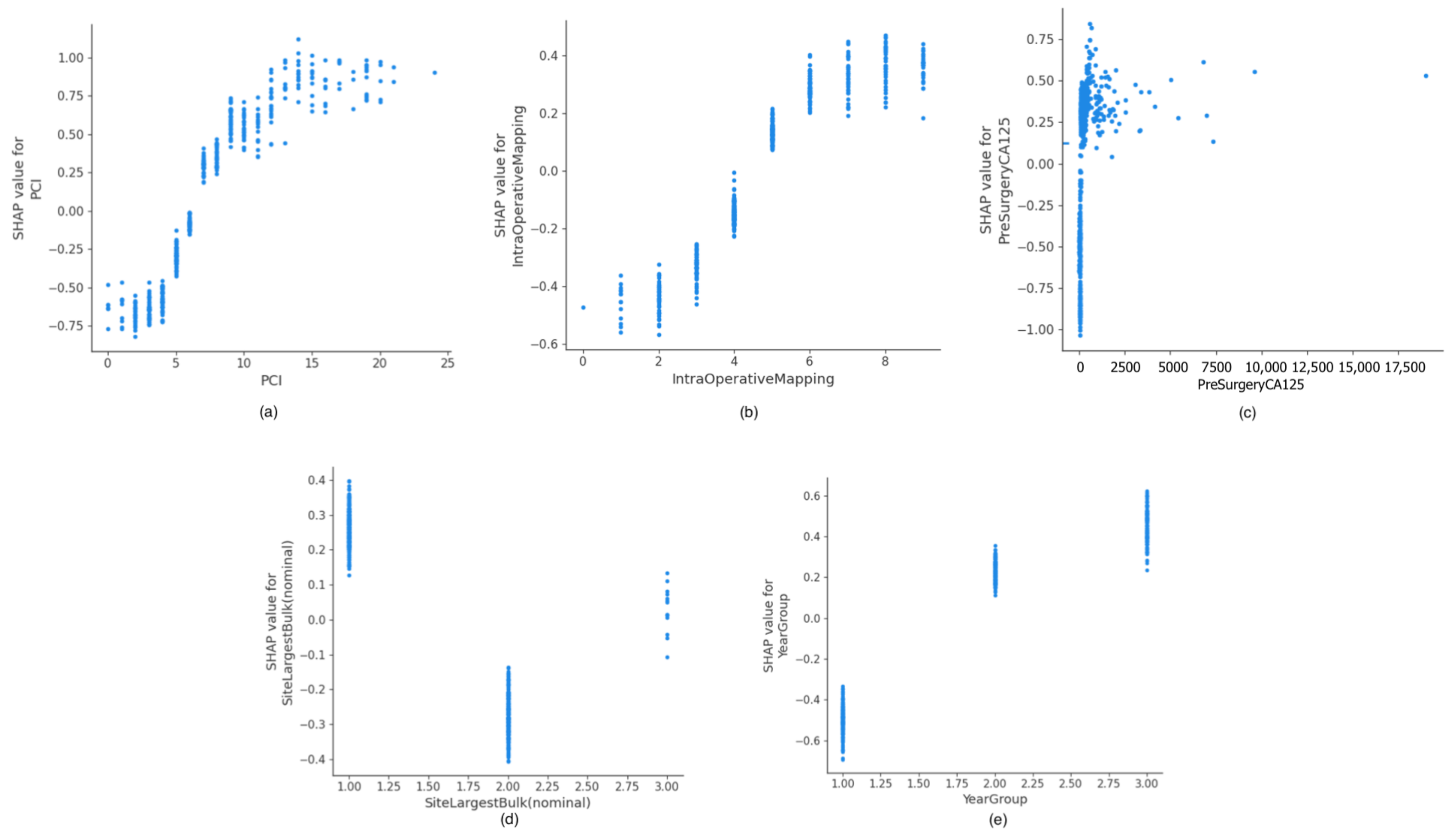
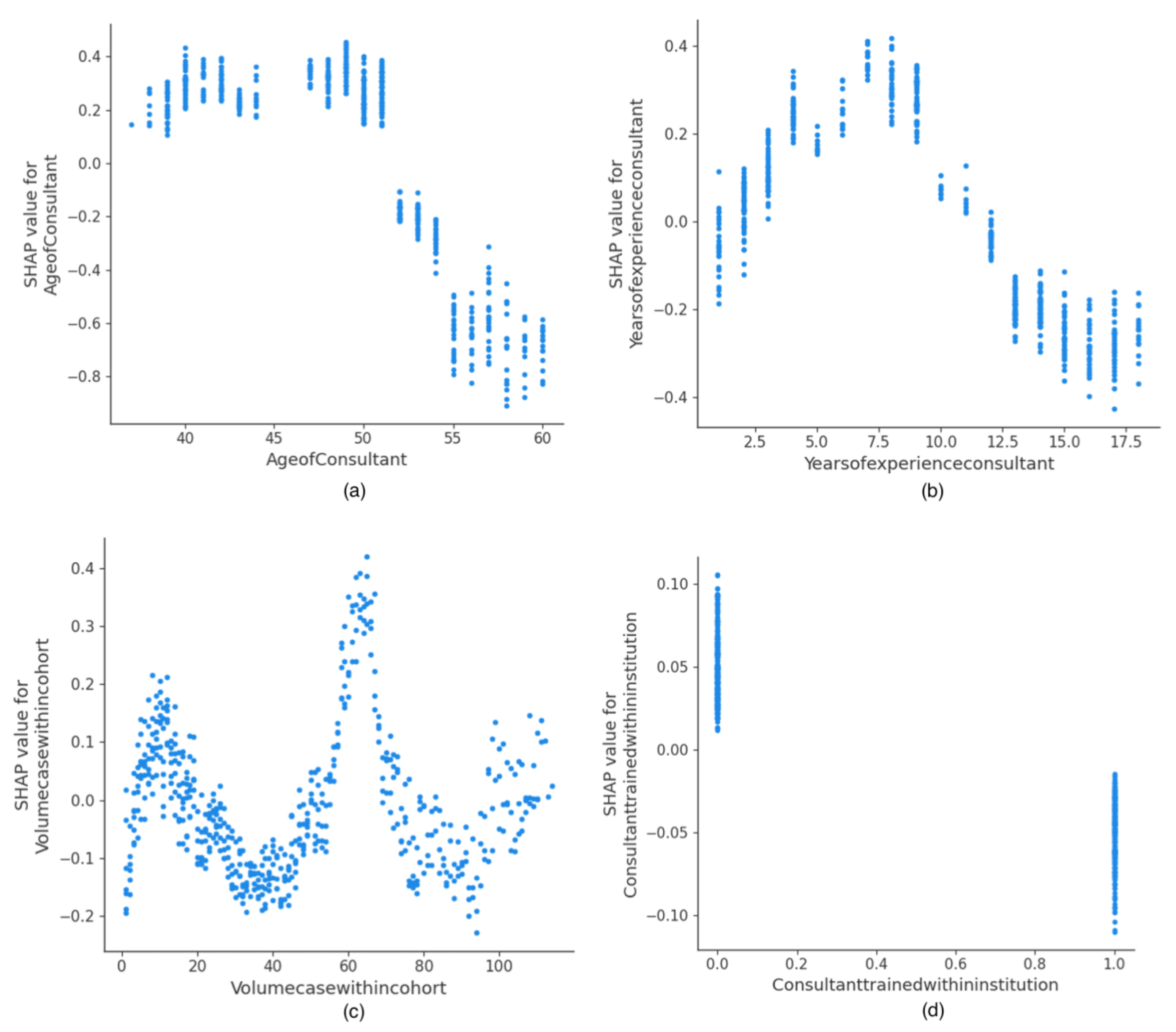
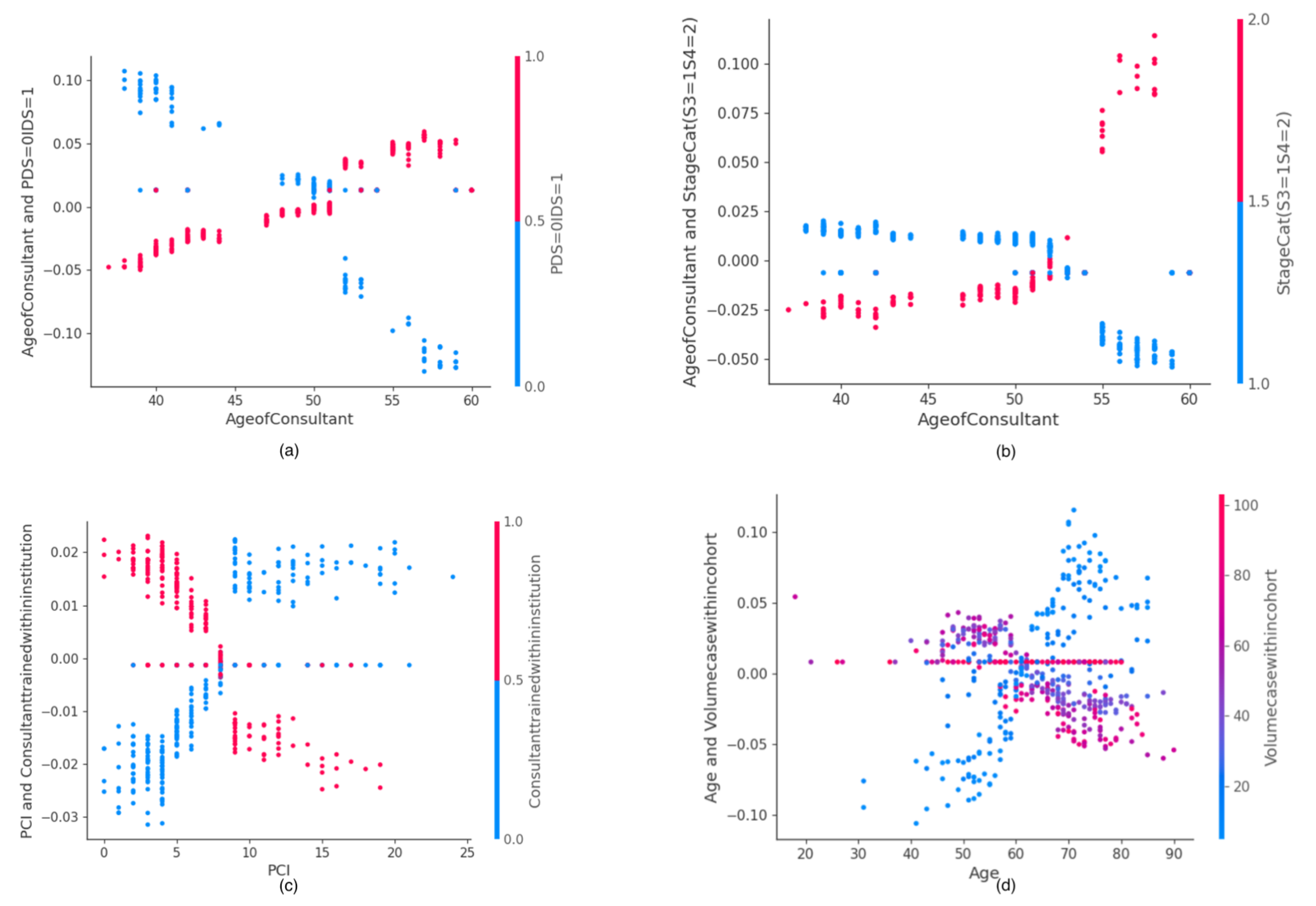
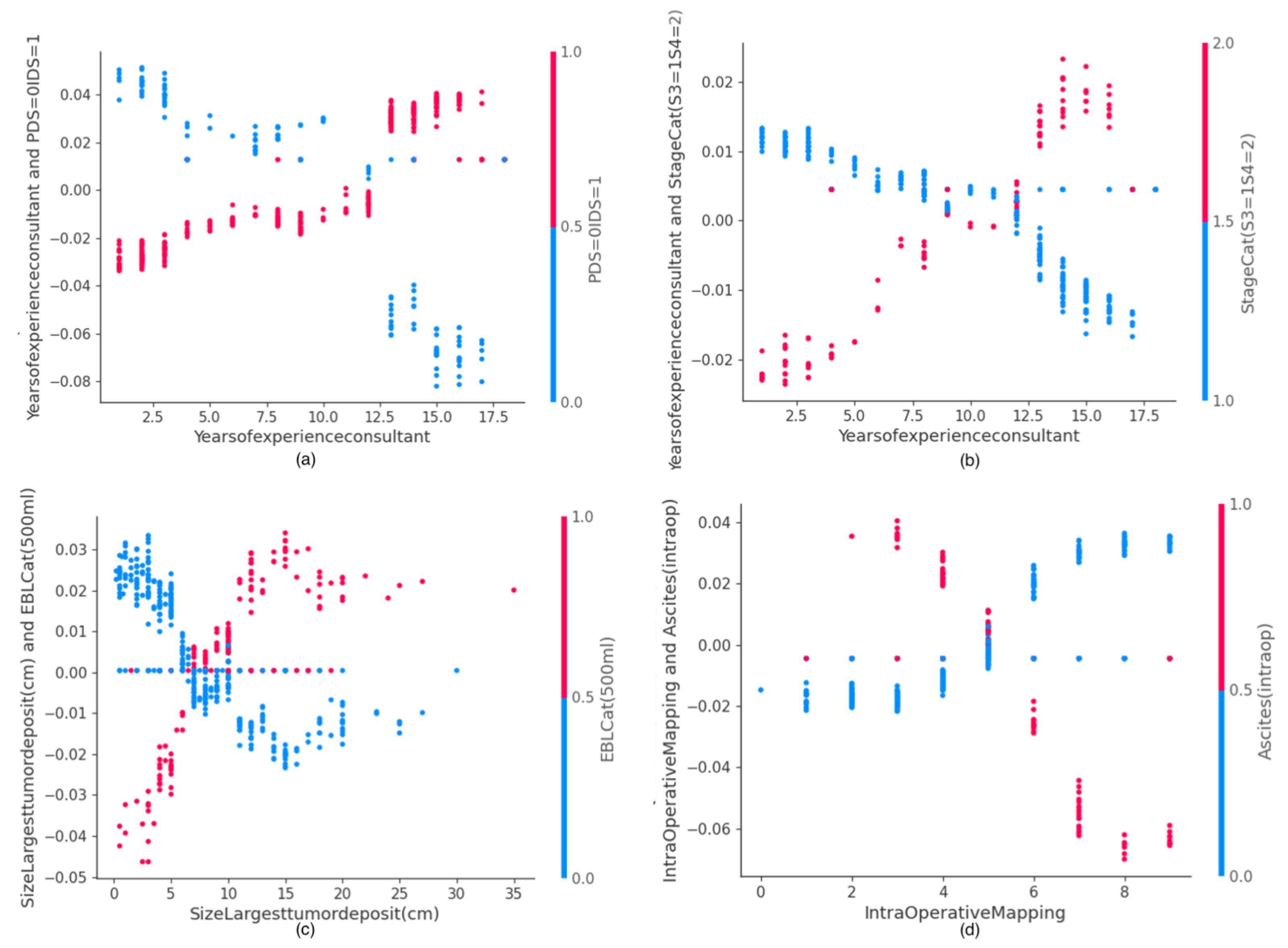
3.2. SHAP Dependence Plots of Human Intuition Features
3.3. SHAP Value Interaction Plots of Features Related to Human Factors




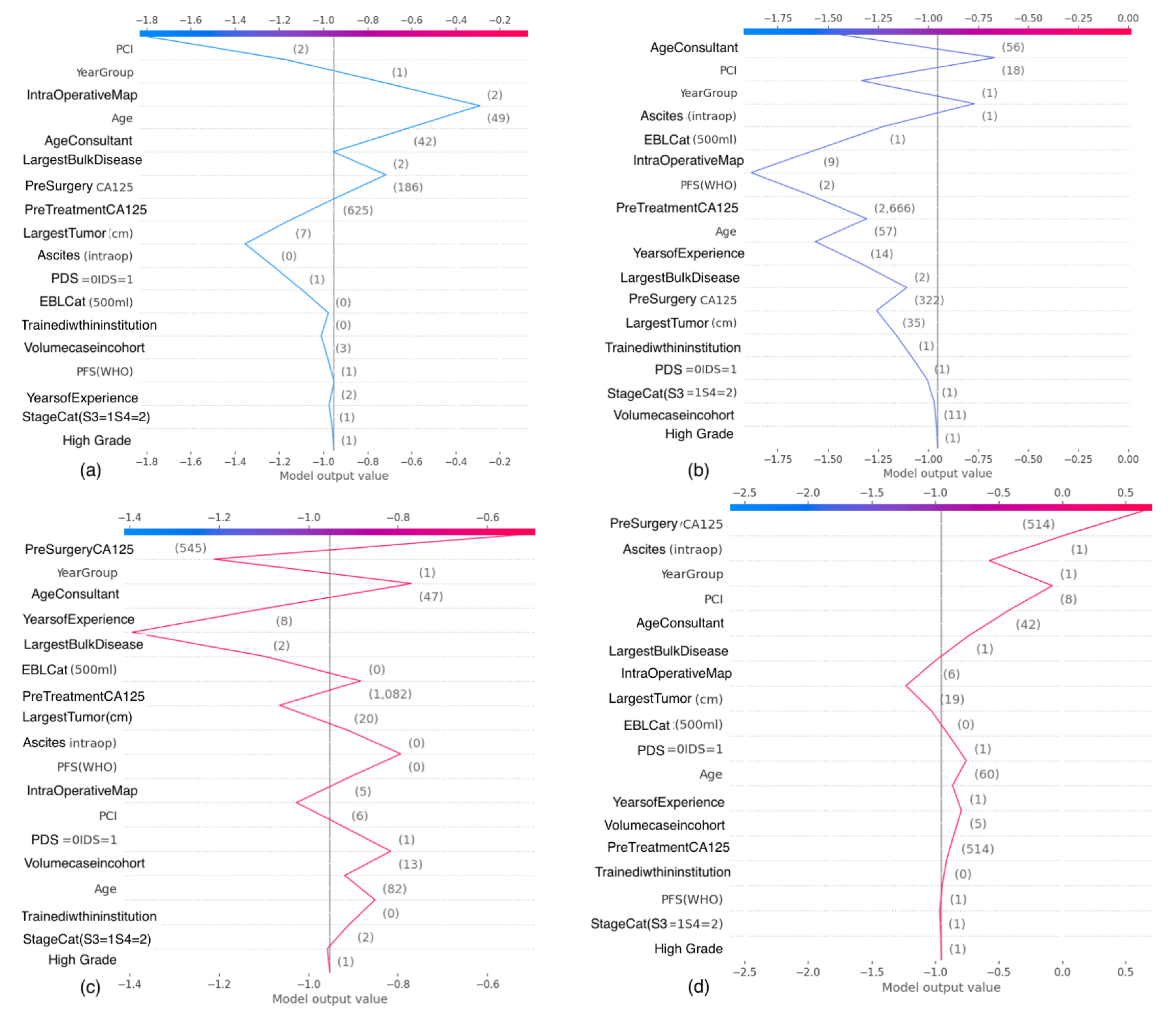
3.4. SHAP Decision Plots
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AI | Artificial Intelligence |
| XAI | Explainable Artificial Intelligence |
| XGBoost | eXtreme Gradient Boosting |
| SHAP | Shapley Additive Explanations |
| AUC-ROC | Area under Curve-Receiver Operator Curve |
| CT | Computer Tomography |
| DS | Disease Score |
| ECOG | Eastern Cooperative Oncology Group |
| EOC | Epithelial ovarian cancer |
| FIGO | Federation International of Obstetrics and Gynaecology |
| IDS | Interval debulking surgery |
| PDS | Primary debulking surgery |
| CEA | Carcinoembryonic antigen |
| HE4 | Human Epididymis 4 |
| NHS | National Health System |
| ML | Machine Learning |
| NACT | Neoadjuvant chemotherapy |
| ACT | Adjuvant Chemotherapy |
| PPM | Patient Pathway Manager |
| MDT | Multidisciplinary team |
| BGCS | British Gynaecologic Cancer Society |
| CPEX | Cardiopulmonary exercise |
| ESGO | European Society Gynaecological Oncology |
| CCU | Critical care admission |
| SD | Standard deviation |
| CV | Cross validation |
| IMO | Intra-operative mapping of ovarian cancer |
| PCI | Peritoneal Cancer Index |
| NSQIP | National Surgical Quality Improvement Program |
| PS | Performance status |
| RD | Residual disease |
| R0 | No residual—complete cytoreduction |
| SCS | Surgical complexity score |
| SJUH | St James’s University Hospital |
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2019. CA Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hacker, N.; Berek, J.; Lagasse, L.; Nieberg, R.; Elashoff, R. Primary cytoreductive surgery for epithelial ovarian cancer. Obstet. Gynecol. 1983, 61, 413–420. [Google Scholar] [PubMed]
- Querleu, D.; Planchamp, F.; Chiva, L.; Fotopoulou, C.; Barton, D.; Cibula, D.; Aletti, G.; Carinelli, S.; Creutzberg, C.; Davidson, B.; et al. European Society of Gynaecological Oncology (ESGO) Guidelines for Ovarian Cancer Surgery. Int. J. Gynecol. Cancer 2017, 27, 1534–1542. [Google Scholar] [CrossRef]
- Winter, W.E.; Maxwell, G.L.; Tian, C.; Carlson, J.W.; Ozols, R.F.; Rose, P.G.; Markman, M.; Armstrong, D.K.; Muggia, F.; McGuire, W.P. Prognostic Factors for Stage III Epithelial Ovarian Cancer: A Gynecologic Oncology Group Study. J. Clin. Oncol. 2007, 25, 3621–3627. [Google Scholar] [CrossRef] [PubMed]
- Bristow, R.E.; Chi, D.S. Platinum-based neoadjuvant chemotherapy and interval surgical cytoreduction for advanced ovarian cancer: A meta-analysis. Gynecol. Oncol. 2006, 103, 1070–1076. [Google Scholar] [CrossRef]
- Aletti, G.D.; Gostout, B.S.; Podratz, K.C.; Cliby, W.A. Ovarian cancer surgical resectability: Relative impact of disease, patient status, and surgeon. Gynecol. Oncol. 2006, 100, 33–37. [Google Scholar] [CrossRef]
- NICE. Ultra -Radical (Extensive) Surgery for Advanced Ovarian Cancer; Interventional Procedures Guidance (IPG470); National Institute for Health and Care Excellence: London, UK, 2011. [Google Scholar]
- Barton, D.; Adib, T.; Butler, J. Surgical practice of UK gynaecological oncologists in the treatment of primary advanced epithelial ovarian cancer (PAEOC): A questionnaire survey. Gynecol. Oncol. 2013, 131, 347–351. [Google Scholar] [CrossRef]
- Aletti, G.D.; Dowdy, S.C.; Podratz, K.C.; Cliby, W.A. Relationship among surgical complexity, short-term morbidity, and overall survival in primary surgery for advanced ovarian cancer. Am. J. Obstet. Gynecol. 2007, 197, 676.e1–676.e7. [Google Scholar] [CrossRef]
- Zhou, J.; Zeng, Z.Y.; Li, L. Progress of artificial intelligence in gynecological malignant tumors. Cancer Manag. Res. 2020, 12, 12823. [Google Scholar] [CrossRef]
- Lu, M.; Fan, Z.; Xu, B.; Chen, L.; Zheng, X.; Li, J.; Znati, T.; Mi, Q.; Jiang, J. Using machine learning to predict ovarian cancer. Int. J. Med. Inform. 2020, 141, 104195. [Google Scholar] [CrossRef]
- Kawakami, E.; Tabata, J.; Yanaihara, N.; Ishikawa, T.; Koseki, K.; Iida, Y.; Saito, M.; Komazaki, H.; Shapiro, J.S.; Goto, C.; et al. Application of artificial intelligence for preoperative diagnostic and prognostic prediction in epithelial ovarian cancer based on blood biomarkers. Clin. Cancer Res. 2019, 25, 3006–3015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laios, A.; Katsenou, A.; Tan, Y.S.; Johnson, R.; Otify, M.; Kaufmann, A.; Munot, S.; Thangavelu, A.; Hutson, R.; Broadhead, T.; et al. Feature Selection is Critical for 2-Year Prognosis in Advanced Stage High Grade Serous Ovarian Cancer by Using Machine Learning. Cancer Control 2021, 28, 10732748211044678. [Google Scholar] [CrossRef] [PubMed]
- Healey, M.A.; Shackford, S.R.; Osler, T.M.; Rogers, F.B.; Burns, E. Complications in surgical patients. Arch. Surg. 2002, 137, 611–618. [Google Scholar] [CrossRef]
- Loftus, T.J.; Tighe, P.J.; Filiberto, A.C.; Efron, P.A.; Brakenridge, S.C.; Mohr, A.M.; Rashidi, P.; Upchurch, G.R.; Bihorac, A. Artificial intelligence and surgical decision-making. JAMA Surg. 2020, 155, 148–158. [Google Scholar] [CrossRef]
- Kopecky, K.E.; Urbach, D.; Schwarze, M.L. Risk calculators and decision aids are not enough for shared decision making. JAMA Surg. 2019, 154, 3–4. [Google Scholar] [CrossRef]
- Ferrer, R.A.; Green, P.A.; Barrett, L.F. Affective Science Perspectives on Cancer Control: Strategically Crafting a Mutually Beneficial Research Agenda. Perspect. Psychol. Sci. 2015, 10, 328–345. [Google Scholar] [CrossRef] [Green Version]
- Leeds, I.L.; Rosenblum, A.J.; Wise, P.E.; Watkins, A.C.; Goldblatt, M.I.; Haut, E.R.; Efron, J.E.; Johnston, F.M. Eye of the beholder: Risk calculators and barriers to adoption in surgical trainees. Surgery 2018, 164, 1117–1123. [Google Scholar] [CrossRef] [PubMed]
- Das, N.; Talaat, A.; Naik, R.; Lopes, A.; Godfrey, K.; Hatem, M.; Edmondson, R. Risk adjusted surgical audit in gynaecological oncology: P-POSSUM does not predict outcome. Eur. J. Surg. Oncol. 2006, 32, 1135–1138. [Google Scholar] [CrossRef]
- Szender, J.B.; Frederick, P.J.; Eng, K.H.; Akers, S.N.; Lele, S.B.; Odunsi, K. Evaluation of the National Surgical Quality Improvement Program Universal Surgical Risk Calculator for a Gynecologic Oncology Service. Int. J. Gynecol. Cancer 2015, 25, 512–520. [Google Scholar] [CrossRef] [Green Version]
- Amann, J.; Blasimme, A.; Vayena, E.; Frey, D.; Madai, V.I. Explainability for artificial intelligence in healthcare: A multidisciplinary perspective. BMC Med. Inform. Decis. Mak. 2020, 20, 310. [Google Scholar] [CrossRef]
- Newsham, A.C.; Johnston, C.; Hall, G.; Leahy, M.G.; Smith, A.B.; Vikram, A.; Donnelly, A.M.; Velikova, G.; Selby, P.J.; Fisher, S.E. Development of an advanced database for clinical trials integrated with an electronic patient record system. Comput. Biol. Med. 2011, 41, 575–586. [Google Scholar] [CrossRef] [PubMed]
- Mutch, D.G.; Prat, J. 2014 FIGO staging for ovarian, fallopian tube and peritoneal cancer. Gynecol. Oncol. 2014, 133, 401–404. [Google Scholar] [CrossRef] [PubMed]
- Fotopoulou, C.; Hall, M.; Cruickshank, D.; Gabra, H.; Ganesan, R.; Hughes, C.; Kehoe, S.; Ledermann, J.; Morrison, J.; Naik, R.; et al. British Gynaecological Cancer Society (BGCS) epithelial ovarian/fallopian tube/primary peritoneal cancer guidelines: Recommendations for practice. Eur. J. Obstet. Gynecol. Reprod. Biol. 2017, 213, 123–139. [Google Scholar] [CrossRef]
- Spanjersberg, W.R.; Reurings, J.; Keus, F.; van Laarhoven, C.J. Fast track surgery versus conventional recovery strategies for colorectal surgery. Cochrane Database Syst. Rev. 2011, 2. [Google Scholar] [CrossRef] [PubMed]
- Nelson, G.; Bakkum-Gamez, J.; Kalogera, E.; Glaser, G.; Altman, A.; Meyer, L.A.; Taylor, J.S.; Iniesta, M.; Lasala, J.; Mena, G.; et al. Guidelines for perioperative care in gynecologic/oncology: Enhanced Recovery After Surgery (ERAS) Society recommendations—2019 update. Int. J. Gynecol. Cancer 2019, 29, 651–668. [Google Scholar] [CrossRef] [PubMed]
- Laios, A.; De Oliveira Silva, R.V.; Dantas De Freitas, D.L.; Tan, Y.S.; Saalmink, G.; Zubayraeva, A.; Johnson, R.; Kaufmann, A.; Otify, M.; Hutson, R.; et al. Machine Learning-Based Risk Prediction of Critical Care Unit Admission for Advanced Stage High Grade Serous Ovarian Cancer Patients Undergoing Cytoreductive Surgery: The Leeds-Natal Score. J. Clin. Med. 2022, 11, 87. [Google Scholar] [CrossRef]
- Poole, J.; Nordin, A. Overview of Ovarian Cancer in England: Incidence, Mortality and Survival; Trent Cancer Registry: Sheffield, UK, 2012. [Google Scholar]
- Querleu, D.; Planchamp, F.; Chiva, L.; Fotopoulou, C.; Barton, D.; Cibula, D.; Aletti, G.; Carinelli, S.; Creutzberg, C.; Davidson, B.; et al. European Society of Gynaecologic Oncology Quality Indicators for Advanced Ovarian Cancer Surgery. Int. J. Gynecol. Cancer 2016, 26, 1354–1363. [Google Scholar] [CrossRef] [Green Version]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205. [Google Scholar] [CrossRef]
- Metawa, N.; Nguyen, P.T.; Le Hoang Thuy To Nguyen, Q.; Elhoseny, M.; Shankar, K. Internet of Things Enabled Financial Crisis Prediction in Enterprises Using Optimal Feature Subset Selection-Based Classification Model. Big Data 2021, 9, 331–342. [Google Scholar] [CrossRef]
- Jacquet, P.; Sugarbaker, P.H. Clinical research methodologies in diagnosis and staging of patients with peritoneal carcinomatosis. In Peritoneal Carcinomatosis: Principles of Management; Sugarbaker, P.H., Ed.; Springer: Boston, MA, USA, 1996; pp. 359–374. [Google Scholar] [CrossRef]
- Sehouli, J.; Könsgen, D.; Mustea, A.; Oskay-Özcelik, G.; Katsares, I.; Weidemann, H.; Lichtenegger, W. “IMO”—Intraoperatives Mapping des Ovarialkarzinoms. Zentralblatt für Gynäkologie 2003, 125, 129–135. [Google Scholar]
- Freund, Y.; Schapire, R.E. A Decision-Theoretic Generalization of On-Line Learning and an Application to Boosting. J. Comput. Syst. Sci. 1997, 55, 119–139. [Google Scholar] [CrossRef] [Green Version]
- Zhu, M.; Min, W.; Wang, Q.; Zou, S.; Chen, X. PFLU and FPFLU: Two novel non-monotonic activation functions in convolutional neural networks. Neurocomputing 2021, 429, 110–117. [Google Scholar] [CrossRef]
- Linardatos, P.; Papastefanopoulos, V.; Kotsiantis, S. Explainable AI: A Review of Machine Learning Interpretability Methods. Entropy 2021, 23, 18. [Google Scholar] [CrossRef]
- Chakraborty, D.; Ivan, C.; Amero, P.; Khan, M.; Rodriguez-Aguayo, C.; Başağaoğlu, H.; Lopez-Berestein, G. Explainable Artificial Intelligence Reveals Novel Insight into Tumor Microenvironment Conditions Linked with Better Prognosis in Patients with Breast Cancer. Cancers 2021, 13, 3450. [Google Scholar] [CrossRef] [PubMed]
- Laios, A.; Kalampokis, E.; Johnson, R.; Thangavelu, A.; Tarabanis, C.; Nugent, D.; De Jong, D. Explainable Artificial Intelligence for Prediction of Complete Surgical Cytoreduction in Advanced-Stage Epithelial Ovarian Cancer. J. Pers. Med. 2022, 12, 607. [Google Scholar] [CrossRef]
- Mahner, S.; Heitz, F.; Burges, A.; Reuss, A.; Kraemer, B.; Schmalfeldt, B.; Sehouli, J.; Lampe, B.; Schnelzer, A.; Wimberger, P.; et al. TRUST: Trial of radical upfront surgical therapy in advanced ovarian cancer (ENGOT ov33/AGO-OVAR OP7). J. Clin. Oncol. 2017, 35, TPS5602. [Google Scholar] [CrossRef]
- Waljee, J.F.; Greenfield, L.J.; Dimick, J.B.; Birkmeyer, J.D. Surgeon age and operative mortality in the United States. Ann. Surg. 2006, 244, 353. [Google Scholar] [CrossRef] [PubMed]
- Nalliah, R. Clinical decision making-choosing between intuition, experience and scientific evidence. Br. Dent. J. 2016, 221, 752–754. [Google Scholar] [CrossRef] [Green Version]
- Tesar, P. Heuristics in cardiothoracic surgery. ANZ J. Surg. 2008, 78, 1106–1108. [Google Scholar] [CrossRef]
- Hollingshead, A.B.; Wittenbaum, G.M.; Paulus, P.B.; Hirokawa, R.Y.; Ancona, D.G.; Peterson, R.S.; Jehn, K.A.; Yoon, K. A Look at Groups from the Functional Perspective. In Theories of Small Groups: Interdisciplinary Perspectives; Poole, M.S., Hollingshead, A.B., Eds.; SAGE Group: Newcastle upon Tyne, UK, 2005; pp. 21–62. [Google Scholar] [CrossRef]
- Satkunasivam, R.; Klaassen, Z.; Ravi, B.; Fok, K.H.; Menser, T.; Kash, B.; Miles, B.J.; Bass, B.; Detsky, A.S.; Wallis, C.J. Relation between surgeon age and postoperative outcomes: A population-based cohort study. CMAJ 2020, 192, E385–E392. [Google Scholar] [CrossRef] [Green Version]
- Jónsdóttir, B.; Lomnytska, M.; Poromaa, I.S.; Silins, I.; Stålberg, K. The peritoneal cancer index is a strong predictor of incomplete cytoreductive surgery in ovarian cancer. Ann. Surg. Oncol. 2021, 28, 244–251. [Google Scholar] [CrossRef] [PubMed]
- Kehoe, S.; Hook, J.; Nankivell, M.; Jayson, G.C.; Kitchener, H.; Lopes, T.; Luesley, D.; Perren, T.; Bannoo, S.; Mascarenhas, M.; et al. Primary chemotherapy versus primary surgery for newly diagnosed advanced ovarian cancer (CHORUS): An open-label, randomised, controlled, non-inferiority trial. Lancet 2015, 386, 249–257. [Google Scholar] [CrossRef]
- Hall, M.; Savvatis, K.; Nixon, K.; Kyrgiou, M.; Hariharan, K.; Padwick, M.; Owens, O.; Cunnea, P.; Campbell, J.; Farthing, A.; et al. Maximal-effort cytoreductive surgery for ovarian cancer patients with a high tumor burden: Variations in practice and impact on outcome. Ann. Surg. Oncol. 2019, 26, 2943–2951. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weller, J.; Boyd, M.; Cumin, D. Teams, tribes and patient safety: Overcoming barriers to effective teamwork in healthcare. Postgrad. Med J. 2014, 90, 149–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crawford, S.C.; Vasey, P.A.; Paul, J.; Hay, A.; Davis, J.A.; Kaye, S.B. Does aggressive surgery only benefit patients with less advanced ovarian cancer? Results from an international comparison within the SCOTROC-1 Trial. J. Clin. Oncol. 2005, 23, 8802–8811. [Google Scholar] [CrossRef]
- Charness, G.; Karni, E.; Levin, D. Individual and group decision making under risk: An experimental study of Bayesian updating and violations of first-order stochastic dominance. J. Risk Uncertain. 2007, 35, 129–148. [Google Scholar] [CrossRef] [Green Version]
- Blasier, R.B. The problem of the aging surgeon: When surgeon age becomes a surgical risk factor. Clin. Orthop. Relat. Res. 2009, 467, 402–411. [Google Scholar] [CrossRef] [Green Version]
- Laios, A.; Gryparis, A.; DeJong, D.; Hutson, R.; Theophilou, G.; Leach, C. Predicting complete cytoreduction for advanced ovarian cancer patients using nearest-neighbor models. J. Ovarian Res. 2020, 13, 117. [Google Scholar] [CrossRef]
- Kumar, A.; Cliby, W.A. Advanced ovarian Cancer: Weighing the risks and benefits of surgery. Clin. Obstet. Gynecol. 2020, 63, 74–79. [Google Scholar] [CrossRef]
- Wise, J. Survey of UK doctors highlights blame culture within the NHS. BMJ 2018, 362, k4001. [Google Scholar] [CrossRef]
- Chi, D.S.; Eisenhauer, E.L.; Zivanovic, O.; Sonoda, Y.; Abu-Rustum, N.R.; Levine, D.A.; Guile, M.W.; Bristow, R.E.; Aghajanian, C.; Barakat, R.R. Improved progression-free and overall survival in advanced ovarian cancer as a result of a change in surgical paradigm. Gynecol. Oncol. 2009, 114, 26–31. [Google Scholar] [CrossRef] [PubMed]
- Lalys, F.; Jannin, P. Surgical process modelling: A review. Int. J. Comput. Assist. Radiol. Surg. 2014, 9, 495–511. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fotopoulou, C.; Concin, N.; Planchamp, F.; Morice, P.; Vergote, I.; du Bois, A.; Querleu, D. Quality indicators for advanced ovarian cancer surgery from the European Society of Gynaecological Oncology (ESGO): 2020 update. Int. J. Gynecol. Cancer 2020, 30, 436–440. [Google Scholar] [CrossRef] [PubMed]
- Phillips, A.; Balega, J.; Nevin, J.; Singh, K.; Elattar, A.; Kehoe, S.; Sundar, S. Reporting ‘Denominator’ data is essential for benchmarking and quality standards in ovarian cancer. Gynecol. Oncol. 2017, 146, 94–100. [Google Scholar] [CrossRef] [Green Version]
- Clark, R.M.; Rice, L.W.; del Carmen, M.G. Thirty-day unplanned hospital readmission in ovarian cancer patients undergoing primary or interval cytoreductive surgery: Systematic literature review. Gynecol. Oncol. 2018, 150, 370–377. [Google Scholar] [CrossRef]
- Maier-Hein, L.; Vedula, S.S.; Speidel, S.; Navab, N.; Kikinis, R.; Park, A.; Eisenmann, M.; Feussner, H.; Forestier, G.; Giannarou, S.; et al. Surgical data science for next-generation interventions. Nat. Biomed. Eng. 2017, 1, 691–696. [Google Scholar] [CrossRef]
- Urushibara, A.; Saida, T.; Mori, K.; Ishiguro, T.; Sakai, M.; Masuoka, S.; Satoh, T.; Masumoto, T. Diagnosing uterine cervical cancer on a single T2-weighted image: Comparison between deep learning versus radiologists. Eur. J. Radiol. 2021, 135, 109471. [Google Scholar] [CrossRef]
- Reuss, A.; du Bois, A.; Harter, P.; Fotopoulou, C.; Sehouli, J.; Aletti, G.; Guyon, F.; Greggi, S.; Mosgaard, B.J.; Reinthaller, A.; et al. TRUST: Trial of Radical Upfront Surgical Therapy in advanced ovarian cancer (ENGOT ov33/AGO-OVAR OP7). Int. J. Gynecol. Cancer 2019, 29, 1327–1331. [Google Scholar] [CrossRef]
- Sundar, S.; Kumar, S.; Long, J.; Balega, J.; Fotopoulou, C.; Broadhead, T.; Duncan, T.; Morrison, J.; Tidy, J.; Kolomainen, D.; et al. Patient-reported outcomes after surgery in advanced ovarian cancer: Initial results from the international, prospective, multicentre SOCQER 2 study. In Proceedings of the 17th Biennial meeting of the International Gynecologic Cancer Society, Kyoto, Japan, 14–16 September 2018. [Google Scholar]
- Gunning, D.; Stefik, M.; Choi, J.; Miller, T.; Stumpf, S.; Yang, G.Z. XAI—Explainable artificial intelligence. Sci. Robot. 2019, 4, eaay7120. [Google Scholar] [CrossRef] [Green Version]
- Pillay, B.; Wootten, A.C.; Crowe, H.; Corcoran, N.; Tran, B.; Bowden, P.; Crowe, J.; Costello, A.J. The impact of multidisciplinary team meetings on patient assessment, management and outcomes in oncology settings: A systematic review of the literature. Cancer Treat. Rev. 2016, 42, 56–72. [Google Scholar] [CrossRef]
- Grote, T.; Berens, P. On the ethics of algorithmic decision-making in healthcare. J. Med. Ethics 2020, 46, 205–211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chhabra, K.R.; Sacks, G.D.; Dimick, J.B. Surgical Decision Making: Challenging Dogma and Incorporating Patient Preferences. JAMA 2017, 317, 357–358. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical Characteristics 1 | Overall (n = 560) | Train Set (n = 392) | Test Set (n = 168) | p-Value | SCS > 4 Group (n = 165) | SCS < 5 Group (n = 395) | p-Value |
|---|---|---|---|---|---|---|---|
| Age | 64 ± 11 | 64 ± 11 | 63 ± 11 | 0.76 | 61 ± 12 | 64 ± 11 | 0.003 |
| High grade | 504 (90%) | 354 (90%) | 150 (89%) | 0.83 | 144 (87%) | 360 (91%) | 0.21 |
| Stage 3 | 406 (72%) | 287 (73%) | 119 (71%) | 0.63 | 113 (68%) | 293 (74%) | 0.2 |
| PFS (WHO) at diagnosis | 0.69 | 0.001 | |||||
| 0 | 266 (47%) | 183 (47%) | 83 (49%) | 95 (58%) | 171 (43%) | ||
| 1 | 208 (37%) | 151 (38%) | 57 (34%) | 55 (33%) | 153 (39%) | ||
| 2 | 67 (12%) | 47 (12%) | 20 (12%) | 8 (5%) | 59 (15%) | ||
| 3 | 17 (3%) | 10 (2%) | 7 (4%) | 5 (3%) | 12 (3%) | ||
| 4 | 2 (0.3%) | 1 (0.2%) | 1 (0.5%) | 2 (1%) | 0 (0%) | ||
| Age of Consultant | 49 ± 6 | 49 ± 6 | 49 ± 6 | 0.31 | 48 ± 6 | 50 ± 6 | 0.001 |
| Volume case within cohort | 45 ± 31 | 46 ± 32 | 44 ± 29 | 0.36 | 46 ± 30 | 45 ± 32 | 0.83 |
| Years of experience | 10 ± 5 | 10 ± 5 | 9 ± 5 | 0.34 | 9 ± 5 | 10 ± 5 | 0.001 |
| Consultant trained within the institution | 250 (45%) | 181 (46%) | 69 (41%) | 0.3 | 60 (36%) | 190 (48%) | 0.01 |
| Timing of surgery | 0.001 | ||||||
| Interval Debulking | 388 (69%) | 274 (70%) | 114 (68%) | 0.7 | 90 (55%) | 298 (75%) | |
| Primary Debulking | 172 (31%) | 118 (30%) | 54 (32%) | 75 (45%) | 97 (25%) | ||
| Year | 0.96 | 0.001 | |||||
| Baseline 2014-15 | 184 (33%) | 128 (33%) | 56 (33%) | 22 (13%) | 162 (41%) | ||
| Transition 2016-17 | 195 (35%) | 136 (35%) | 59 (35%) | 67 (41%) | 128 (32%) | ||
| Evaluation 2018-19 | 181 (32%) | 128 (33%) | 53 (31%) | 76 (46%) | 105 (26%) | ||
| EBL > 500 mL | 179 (32%) | 128 (33%) | 51 (30%) | 0.66 | 86 (52%) | 93 (24%) | 0.001 |
| Pre-Treatment CA125 | 1515 ± 2710 | 1545 ± 2762 | 1445 ± 2592 | 0.68 | 1237 ± 2318 | 1630 ± 2853 | 0.088 |
| Pre-Surgery CA125 | 411 ± 1175 | 381 ± 899 | 476 ± 1649 | 0.91 | 443 ± 968 | 397 ± 1252 | 0.64 |
| Size Largest Tumor Deposit (cm) | 8.9 ± 5.6 | 9 ± 5.4 | 8.5 ± 6 | 0.34 | 10.4 ± 5.5 | 8.3 ± 5.5 | <0.001 |
| PCI | 7 ± 4 | 7 ± 4 | 7 ± 5 | 0.78 | 10 ± 5 | 6 ± 4 | 0.001 |
| Largest Bulk of disease (nominal) | 0.88 | 0.99 | |||||
| Ovary | 294 (52%) | 207 (53%) | 87 (52%) | 92 (56%) | 202 (51%) | ||
| Omentum | 252 (45%) | 176 (45%) | 76 (45%) | 66 (40%) | 186 (47%) | ||
| Miscellaneous | 14 (2%) | 9 (2%) | 5 (3%) | 7 (4%) | 7 (2%) | ||
| Intra Operative Mapping | 5 #xB1; 2 | 5 ± 2 | 5 ± 2 | 0.62 | 6 ± 2 | 5 ± 2 | 0.001 |
| Ascites (intra-op) (mL) | 130 (23%) | 93 (24%) | 37 (22%) | 0.74 | 57 (35%) | 73 (18%) | 0.001 |
| Precision | Recall | F1-Score | |
|---|---|---|---|
| Group 1 (SCS < 5) | 0.84 | 0.77 | 0.80 |
| Group 2 (SCS > 4) | 0.56 | 0.67 | 0.61 |
| Precision | Recall | F1-Score | |
|---|---|---|---|
| Group 1 (SCS < 5) | 0.84 | 0.69 | 0.76 |
| Group 2 (SCS > 4) | 0.51 | 0.71 | 0.59 |
| Algorithm | Hyperparameters 1 |
|---|---|
| XGBoost | ‘max_depth’: 3, ‘alpha’: 0.001, ‘subsample’: 0.75, ‘learning_rate’: 0.01, ‘n_estimators’: 500, ‘colsample_bytree’: 0.75, ‘colsample_bylevel’: 0.75, ‘scale_pos_weight’: 2.39 |
| DNN | activation function: GeLU, dense dropout: 0.1, learning rate: 0.01, batch size: 20, epochs: 9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Laios, A.; Kalampokis, E.; Johnson, R.; Munot, S.; Thangavelu, A.; Hutson, R.; Broadhead, T.; Theophilou, G.; Leach, C.; Nugent, D.; et al. Factors Predicting Surgical Effort Using Explainable Artificial Intelligence in Advanced Stage Epithelial Ovarian Cancer. Cancers 2022, 14, 3447. https://doi.org/10.3390/cancers14143447
Laios A, Kalampokis E, Johnson R, Munot S, Thangavelu A, Hutson R, Broadhead T, Theophilou G, Leach C, Nugent D, et al. Factors Predicting Surgical Effort Using Explainable Artificial Intelligence in Advanced Stage Epithelial Ovarian Cancer. Cancers. 2022; 14(14):3447. https://doi.org/10.3390/cancers14143447
Chicago/Turabian StyleLaios, Alexandros, Evangelos Kalampokis, Racheal Johnson, Sarika Munot, Amudha Thangavelu, Richard Hutson, Tim Broadhead, Georgios Theophilou, Chris Leach, David Nugent, and et al. 2022. "Factors Predicting Surgical Effort Using Explainable Artificial Intelligence in Advanced Stage Epithelial Ovarian Cancer" Cancers 14, no. 14: 3447. https://doi.org/10.3390/cancers14143447