
Biomarkers of Trastuzumab-Induced Cardiac Toxicity in HER2- Positive Breast Cancer Patient Population

 , , , , ,
, , , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.1.1. Radiotherapy Technique
2.1.2. Primary Assessment (Baseline)
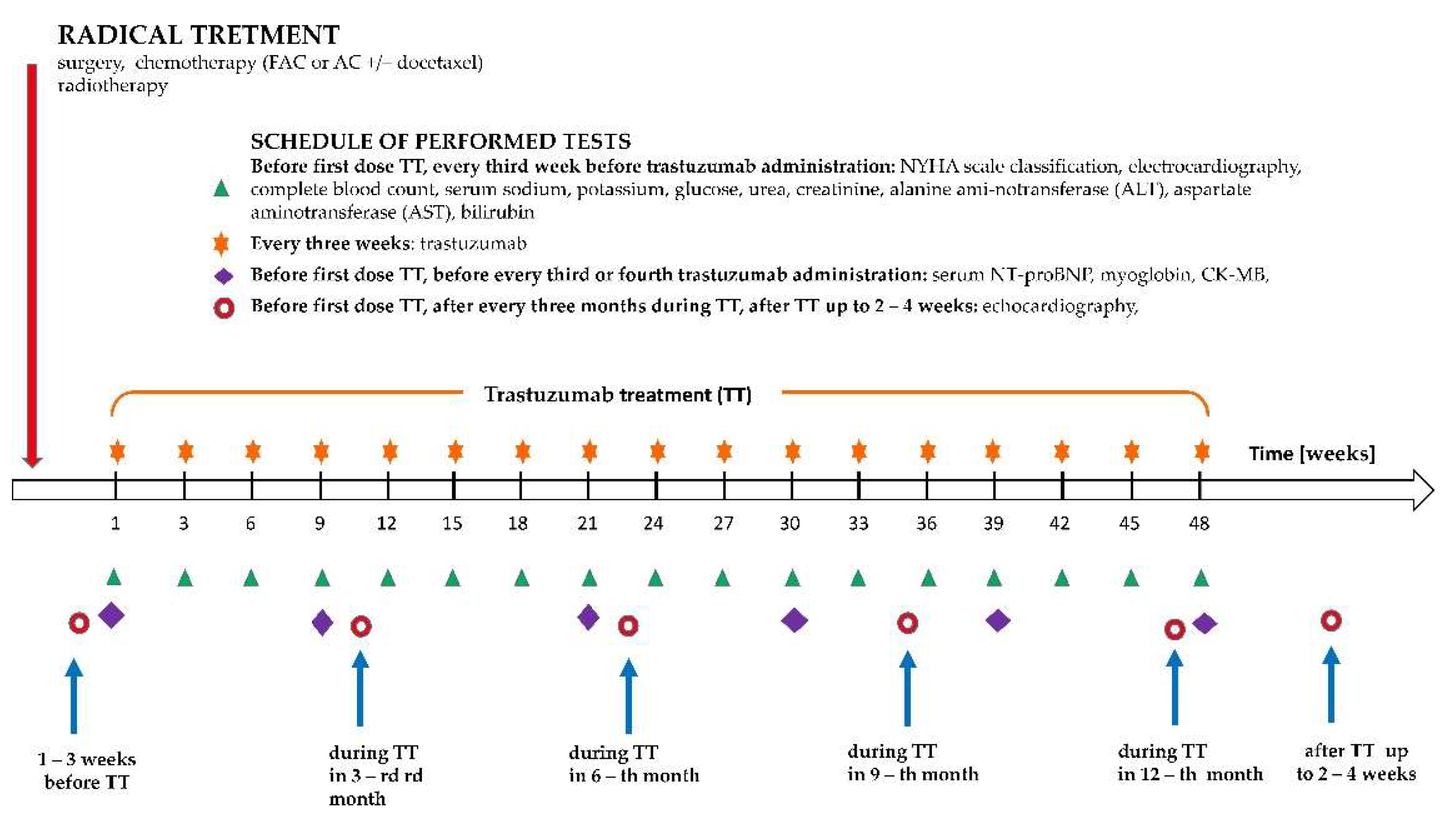
2.1.3. Cardiac and Biomarker Evaluation
2.1.4. Clinical Outcome
2.2. Laboratory Analysis
2.3. Ethical Considerations
2.4. Statistical Analysis
3. Results
3.1. Baseline characteristics
3.2. Key Outcome Measures
3.2.1. Cardiac Complications Prevalence, Clinical Parameters, and Risk Factors
3.2.2. TIC Occurrence According to Levels of Clinical and Biochemical Parameters
4. Discussion
Study Limitations
5. Conclusions
Clinical Implications
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Shin, H.R. Global Activity of Cancer Registries and Cancer Control and Cancer Incidence Statistics in Korea. J. Prev. Med. Public Health 2008, 41, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Mathers, C.; Parkin, D.M.; Piñeros, M.; Znaor, A.; Bray, F. Estimating the Global Cancer Incidence and Mortality in 2018: GLOBOCAN Sources and Methods. Int. J. Cancer 2019, 144, 1941–1953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loibl, S.; Poortmans, P.; Morrow, M.; Denkert, C.; Curigliano, G. Breast Cancer. Lancet 2021, 397, 1750–1769. [Google Scholar] [CrossRef]
- Zhu, H.; Doğan, B.E. American Joint Committee on Cancer’s Staging System for Breast Cancer, Eighth Edition: Summary for Clinicians. Eur. J. Breast Health 2021, 17, 234–238. [Google Scholar] [CrossRef] [PubMed]
- Mohanty, S.S.; Sahoo, C.R.; Padhy, R.N. Role of Hormone Receptors and HER2 as Prospective Molecular Markers for Breast Cancer: An Update. Genes Dis. 2021, 9, 648–658. [Google Scholar] [CrossRef]
- Cameron, D.; Piccart-Gebhart, M.J.; Gelber, R.D.; Procter, M.; Goldhirsch, A.; de Azambuja, E.; Castro, G.; Untch, M.; Smith, I.; Gianni, L.; et al. 11 Years’ Follow-up of Trastuzumab after Adjuvant Chemotherapy in HER2-Positive Early Breast Cancer: Final Analysis of the HERceptin Adjuvant (HERA) Trial. Lancet 2017, 389, 1195–1205. [Google Scholar] [CrossRef] [Green Version]
- Goutsouliak, K.; Veeraraghavan, J.; Sethunath, V.; De Angelis, C.; Osborne, C.K.; Rimawi, M.F.; Schiff, R. Towards Personalized Treatment for Early Stage HER2-Positive Breast Cancer. Nat. Rev. Clin. Oncol. 2019, 17, 233–250. [Google Scholar] [CrossRef]
- Gonciar, D.; Mocan, L.; Zlibut, A.; Mocan, T.; Agoston-Coldea, L. Cardiotoxicity in HER2-Positive Breast Cancer Patients. Heart Fail. Rev. 2021, 26, 919–935. [Google Scholar] [CrossRef]
- Earl, H.M.; Hiller, L.; Vallier, A.L.; Loi, S.; McAdam, K.; Hughes-Davies, L.; Harnett, A.N.; Ah-See, M.L.; Simcock, R.; Rea, D.; et al. 6 versus 12 Months of Adjuvant Trastuzumab for HER2-Positive Early Breast Cancer (PERSEPHONE): 4-Year Disease-Free Survival Results of a Randomised Phase 3 Non-Inferiority Trial. Lancet 2019, 393, 2599–2612. [Google Scholar] [CrossRef] [Green Version]
- Grela-Wojewoda, A.; Pacholczak-Madej, R.; Adamczyk, A.; Korman, M.; Püsküllüoğlu, M. Cardiotoxicity Induced by Protein Kinase Inhibitors in Cancer Patient Population. Int. J. Mol. Sci. 2022, 23, 2815. [Google Scholar] [CrossRef]
- Litvak, A.; Batukbhai, B.; Russell, S.D.; Tsai, H.L.; Rosner, G.L.; Jeter, S.C.; Armstrong, D.; Emens, L.A.; Fetting, J.; Wolff, A.C.; et al. Racial Disparities in the Rate of Cardiotoxicity of HER2-Targeted Therapies among Women with Early Breast Cancer. Cancer 2018, 124, 1904–1911. [Google Scholar] [CrossRef] [PubMed]
- Shaikh, A.Y.; Shih, J.A. Chemotherapy-Induced Cardiotoxicity. Curr. Heart Fail. Rep. 2012, 9, 117–127. [Google Scholar] [CrossRef] [PubMed]
- Słowik, A.J.; Jagielski, P.; Potocki, P.; Streb, J.; Ochenduszko, S.; Wysocki, P.; Gajos, G.; Konduracka, E. Anthracycline-Induced Cardiotoxicity Prevention with Angiotensin-Converting Enzyme Inhibitor Ramipril in Women with Low-Risk Breast Cancer: Results of a Prospective Randomized Study. Kardiol. Pol. 2020, 78, 131–137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koutsoukis, A.; Ntalianis, A.; Repasos, E.; Kastritis, E.; Dimopoulos, M.A.; Paraskevaidis, I. Cardio-Oncology: A Focus on Cardiotoxicity. Eur. Cardiol. Rev. 2018, 13, 64–69. [Google Scholar] [CrossRef]
- Lidbrink, E.; Chmielowska, E.; Otremba, B.; Bouhlel, A.; Lauer, S.; Liste Hermoso, M.; Nüesch, E.; Shing, M.; Misra, V. A Real-World Study of Cardiac Events in >3700 Patients with HER2-Positive Early Breast Cancer Treated with Trastuzumab: Final Analysis of the OHERA Study. Breast Cancer Res. Treat. 2019, 174, 187–196. [Google Scholar] [CrossRef] [Green Version]
- Russo, G.; Cioffi, G.; Gori, S.; Tuccia, F.; Boccardi, L.; Khoury, G.; Lestuzzi, C.; Maurea, N.; Oliva, S.; Faggiano, P.; et al. Role of Hypertension on New Onset Congestive Heart Failure in Patients Receiving Trastuzumab Therapy for Breast Cancer. J. Cardiovasc. Med. 2014, 15, 141–146. [Google Scholar] [CrossRef]
- Guenancia, C.; Lefebvre, A.; Cardinale, D.; Yu, A.F.; Ladoire, S.; Ghiringhelli, F.; Zeller, M.; Rochette, L.; Cottin, Y.; Vergely, C. Obesity as a Risk Factor for Anthracyclines and Trastuzumab Cardiotoxicity in Breast Cancer: A Systematic Review and Meta-Analysis. J. Clin. Oncol. 2016, 34, 3157–3165. [Google Scholar] [CrossRef] [Green Version]
- Jawa, Z.; Perez, R.M.; Garlie, L.; Singh, M.; Qamar, R.; Khandheria, B.K.; Jahangir, A.; Shi, Y. Risk Factors of Trastuzumab-Induced Cardiotoxicity in Breast Cancer A Meta-Analysis. Medicine 2016, 95, e5195. [Google Scholar] [CrossRef]
- Udagawa, C.; Nakamura, H.; Ohnishi, H.; Tamura, K.; Shimoi, T.; Yoshida, M.; Yoshida, T.; Totoki, Y.; Shibata, T.; Zembutsu, H. Whole Exome Sequencing to Identify Genetic Markers for Trastuzumab-Induced Cardiotoxicity. Cancer Sci. 2018, 109, 446–452. [Google Scholar] [CrossRef] [Green Version]
- Pinheiro, E.A.; Fetterman, K.A.; Burridge, P.W. HiPSCs in Cardio-Oncology: Deciphering the Genomics. Cardiovasc. Res. 2019, 115, 935–948. [Google Scholar] [CrossRef]
- Alawadi, F.; Abusnana, S.; Afandi, B.; Aldahmani, K.M.; Alhajeri, O.; Aljaberi, K.; Alkaabi, J.; Almadani, A.; Bashier, A.; Beshyah, S.A.; et al. Emirates Diabetes Society Consensus Guidelines for the Management of Type 2 Diabetes Mellitus–2020. Dubai Diabetes Endocrinol. J. 2020, 26, 1–20. [Google Scholar] [CrossRef]
- McKee, P.A.; Castelli, W.P.; McNamara, P.M.; Kannel, W.B. The Natural History of Congestive Heart Failure: The Framingham Study. N. Engl. J. Med. 1971, 285, 1441–1446. [Google Scholar] [CrossRef] [PubMed]
- Criscitiello, C.; Curigliano, G. HER2 Signaling Pathway and Trastuzumab Cardiotoxicity. Futur. Oncol. 2013, 9, 179–181. [Google Scholar] [CrossRef] [PubMed]
- Guglin, M.; Cutro, R.; Mishkin, J.D. Trastuzumab-Induced Cardiomyopathy. J. Card. Fail. 2008, 14, 437–444. [Google Scholar] [CrossRef]
- Slamon, D.; Eiermann, W.; Robert, N.; Pienkowski, T.; Martin, M.; Press, M.; Mackey, J.; Glaspy, J.; Chan, A.; Pawlicki, M.; et al. Adjuvant Trastuzumab in HER2-Positive Breast Cancer. N. Engl. J. Med. 2011, 365, 1273–1283. [Google Scholar] [CrossRef] [Green Version]
- Piccart-Gebhart, M.J.; Procter, M.; Leyland-Jones, B.; Goldhirsch, A.; Untch, M.; Smith, I.; Gianni, L.; Baselga, J.; Bell, R.; Jackisch, C.; et al. Trastuzumab after Adjuvant Chemotherapy in HER2-Positive Breast Cancer. N. Engl. J. Med. 2005, 353, 1659–1672. [Google Scholar] [CrossRef] [Green Version]
- Vici, P.; Viola, G.; Botti, C.; Rossi, S.; Vitucci, C.; Corsetti, S.; Di Lauro, L.; Sergi, D.; Foggi, P.; Perri, P.; et al. Docetaxel in the Adjuvant Therapy of HER-2 Positive Breast Cancer Patients. Clin. Ter. 2008, 159, 449–452. [Google Scholar]
- Perez, E.A.; Romond, E.H.; Suman, V.J.; Jeong, J.H.; Sledge, G.; Geyer, C.E.; Martino, S.; Rastogi, P.; Gralow, J.; Swain, S.M.; et al. Trastuzumab plus Adjuvant Chemotherapy for Human Epidermal Growth Factor Receptor 2-Positive Breast Cancer: Planned Joint Analysis of Overall Survival from NSABP B-31 and NCCTG N9831. J. Clin. Oncol. 2014, 32, 3744–3752. [Google Scholar] [CrossRef]
- Bowles, E.J.A.; Wellman, R.; Feigelson, H.S.; Onitilo, A.A.; Freedman, A.N.; Delate, T.; Allen, L.A.; Nekhlyudov, L.; Goddard, K.A.B.; Davis, R.L.; et al. Risk of Heart Failure in Breast Cancer Patients after Anthracycline and Trastuzumab Treatment: A Retrospective Cohort Study. J. Natl. Cancer Inst. 2012, 104, 1293–1305. [Google Scholar] [CrossRef]
- Sato, A.; Yoshihisa, A.; Miyata-Tatsumi, M.; Oikawa, M.; Kobayashi, A.; Ishida, T.; Ohtake, T.; Takeishi, Y. Valvular Heart Disease as a Possible Predictor of Trastuzumab-Induced Cardiotoxicity in Patients with Breast Cancer. Mol. Clin. Oncol. 2018, 10, 37–42. [Google Scholar] [CrossRef] [Green Version]
- Grela-Wojewoda, A.; Niemiec, J.; Sas-Korczyńska, B.; Zemełka, T.; Puskulluoglu, M.; Wysocki, W.M.; Wojewoda, T.; Pacholczak-Madej, R.; Adamczyk, A.; Mucha-Małecka, A.; et al. Adjuvant Combined Therapy with Trastuzumab in Patients with HER2-Positive Breast Cancer and Cardiac Alterations: Implications for Optimal Cardio-Oncology Care. Pol. Arch. Intern. Med. 2022. [Google Scholar] [CrossRef] [PubMed]
- Zamorano, J.L.; Lancellotti, P.; Muñoz, D.R.; Aboyans, V.; Asteggiano, R.; Galderisi, M.; Habib, G.; Lenihan, D.J.; Lip, G.Y.H.; Lyon, A.R.; et al. 2016 ESC Position Paper on Cancer Treatments and Cardiovascular Toxicity Developed under the Auspices of the ESC Committee for Practice Guidelines: The Task Force for Cancer Treatments and Cardiovascular Toxicity of the European Society of Cardiology (ESC). Russ. J. Cardiol. 2017, 143, 105–139. [Google Scholar] [CrossRef] [PubMed]
- Bloom, M.W.; Hamo, C.E.; Cardinale, D.; Ky, B.; Nohria, A.; Baer, L.; Skopicki, H.; Lenihan, D.J.; Gheorghiade, M.; Lyon, A.R.; et al. Cancer Therapy-Related Cardiac Dysfunction and Heart Failure: Part 1: Definitions, Pathophysiology, Risk Factors, and Imaging. Circ. Hear Fail. 2016, 9, e002661. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tassan-Mangina, S.; Codorean, D.; Metivier, M.; Costa, B.; Himberlin, C.; Jouannaud, C.; Blaise, A.M.; Elaerts, J.; Nazeyrollas, P. Tissue Doppler Imaging and Conventional Echocardiography after Anthracycline Treatment in Adults: Early and Late Alterations of Left Ventricular Function during a Prospective Study. Eur. J. Echocardiogr. 2006, 7, 141–146. [Google Scholar] [CrossRef] [Green Version]
- Blancas, I.; Martín-Pérez, F.J.; Garrido, J.M.; Rodríguez-Serrano, F. NT-ProBNP as Predictor Factor of Cardiotoxicity during Trastuzumab Treatment in Breast Cancer Patients. Breast 2020, 54, 106–113. [Google Scholar] [CrossRef]
- Cardinale, D.; Colombo, A.; Torrisi, R.; Sandri, M.T.; Civelli, M.; Salvatici, M.; Lamantia, G.; Colombo, N.; Cortinovis, S.; Dessanai, M.A.; et al. Trastuzumab-Induced Cardiotoxicity: Clinical and Prognostic Implications of Troponin I Evaluation. J. Clin. Oncol. 2010, 28, 3910–3916. [Google Scholar] [CrossRef]
- Sandri, M.T.; Salvatici, M.; Cardinale, D.; Zorzino, L.; Passerini, R.; Lentati, P.; Leon, M.; Civelli, M.; Martinelli, G.; Cipolla, C.M. N-Terminal pro-B-Type Natriuretic Peptide after High-Dose Chemotherapy: A Marker Predictive of Cardiac Dysfunction? Clin. Chem. 2005, 51, 1405–1410. [Google Scholar] [CrossRef] [Green Version]
- Horacek, J.M.; Pudil, R.; Jebavy, L.; Tichy, M.; Zak, P.; Maly, J. Assessment of Anthracycline-Induced Cardiotoxicity with Biochemical Markers. Exp. Oncol. 2007, 29, 309–313. [Google Scholar]
- Meinardi, M.T.; Van Veldhuisen, D.J.; Gietema, J.A.; Dolsma, W.V.; Boomsma, F.; Van Den Berg, M.P.; Volkers, C.; Haaksma, J.; De Vries, E.G.E.; Sleijfer, D.T.; et al. Prospective Evaluation of Early Cardiac Damage Induced by Epirubicin-Containing Adjuvant Chemotherapy and Locoregional Radiotherapy in Breast Cancer Patients. J. Clin. Oncol. 2001, 19, 2746–2753. [Google Scholar] [CrossRef]
- Horacek, J.M.; Tichy, M.; Jebavy, L.; Pudil, R.; Ulrychova, M.; Maly, J. Use of Multiple Biomarkers for Evaluation of Anthracycline-Induced Cardiotoxicity in Patients with Acute Myeloid Leukemia. Exp. Oncol. 2008, 30, 157–159. [Google Scholar]
- Stanton, S.E.; Ward, M.M.; Christos, P.; Sanford, R.; Lam, C.; Cobham, M.V.; Donovan, D.; Scheff, R.J.; Cigler, T.; Moore, A.; et al. Pro1170 Ala Polymorphism in HER2-Neu Is Associated with Risk of Trastuzumab Cardiotoxicity. BMC Cancer 2015, 15, 267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ponde, N.; Bradbury, I.; Lambertini, M.; Ewer, M.; Campbell, C.; Ameels, H.; Zardavas, D.; Di Cosimo, S.; Baselga, J.; Huober, J.; et al. Cardiac biomarkers for early detection and prediction of trastuzumab and/or lapatinib-induced cardiotoxicity in patients with HER2-positive early-stage breast cancer: A NeoALTTO sub-study (BIG 1-06). Breast Cancer Res Treat. 2018, 168, 631–638. [Google Scholar] [CrossRef] [PubMed]
- Kreutzfeldt, J.; Rozeboom, B.; Dey, N.; De, P. The Trastuzumab Era: Current and Upcoming Targeted HER2+ Breast Cancer Therapies. Am. J. Cancer Res. 2020, 10, 1045–1067. [Google Scholar]
- Opolski, G.; Krzakowski, M.; Szmit, S.; Banach, J.; Chudzik, M.; Cygankiewicz, I.; Drozdz, J.; Filipiak, K.J.; Grabowski, M.; Kaczmarek, K.; et al. Recommendations of National Team of Cardiologic and Oncologic Supervision on Cardiologic Safety of Patients with Breast Cancer. The Prevention and Treatment of Cardiovascular Complications in Breast Cancer. The Task Force of National Consultants in Cardiology and Clinical Oncology for the Elaboration of Recommendations of Cardiologic Proceeding with Patients with Breast Cancer. Kardiol. Pol. 2011, 69, 520–530. [Google Scholar] [PubMed]
- Tajstra, M.; Blamek, S.; Skoczylas, I.; Majsnerowska, A.; Niedziela, J.T.; Gadula-Gacek, E.; Bobek-Billewicz, B.; Gąsior, M.; Jarząb, M. Two Professions against Two Killer Diseases: The Rationale, Organization, and Initial Experience of a Cardio-Oncology Service. Kardiol. Pol. 2021, 79, 139–146. [Google Scholar] [CrossRef]
- Teske, A.J.; Linschoten, M.; Kamphuis, J.A.M.; Naaktgeboren, W.R.; Leiner, T.; van der Wall, E.; Kuball, J.; van Rhenen, A.; Doevendans, P.A.; Cramer, M.J.; et al. Cardio-Oncology: An Overview on Outpatient Management and Future Developments. Neth. Heart J. 2018, 26, 521–532. [Google Scholar] [CrossRef] [Green Version]
- De Baat, E.C.; Naaktgeboren, W.R.; Leiner, T.; Teske, A.J.; Habets, J.; Grotenhuis, H.B. Update in Imaging of Cancer Therapy-Related Cardiac Toxicity in Adults. Open Heart 2021, 8, e001506. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Parameter | No. of Patients (%) | |
|---|---|---|
| Surgical treatment | BCT | 99 (76.2) |
| Madden radical mastectomy | 31 (23.8) | |
| Stage of breast cancer | I | 32 (24.6) |
| IIA | 52 (40.0) | |
| IIB | 22 (16.9) | |
| IIIA | 24 (18.5) | |
| Laterality | Left | 67 (51.5) |
| Right | 63 (48.5) | |
| Treatment | Radiotherapy | 102 (78.5) |
| Hormonal therapy | 66 (50.8) | |
| Chemotherapy | 127 (97.7) | |
| Docetaxel administration | 34 (26.2) | |
| Anthracycline dose [mg/m2] | 0 | 2 (1.5) |
| 240 | 73 (56.2) | |
| 300 | 4 (3.1) | |
| 360 | 49 (37.7) | |
| 480 | 2 (1.5) | |
| Comorbidities | Ischemic Heart Disease | 19 (14.6) |
| Hypertension | 34 (26.2) | |
| Type II Diabetes | 5 (3.8) | |
| BMI [kg/m2] | 19–25 | 40 (30.8) |
| 25–30 | 49 (37.7) | |
| >30 | 41 (31.5) | |
| Complication | All Cases: 130 | ||
|---|---|---|---|
| No. of Cases with Interruption of TT | No. of Cases with Cessation of TT | No. of TT Cycles in Patients with TT Cessation | |
| Decrease in LVEF | 10 (7.7%) | 3 (2.3%) | 7, 8, 12 |
| Decrease in LVEF + heart failure | 2 (1.5%) | 2 (1.5%) | 1, 11 |
| Decrease in LVEF + arrhythmia | 1 (0.8%) | 0 | - |
| Decrease in LVEF + arrhythmia + heart failure | 1 (0.8%) | 1 (0.8%) | 6 |
| Heart failure | 3 (2.3%) | 3 (2.3%) | 7, 15, 15 |
| Arrhythmia | 1 (0.8%) | 0 | - |
| Arrhythmia + heart failure | 1 (0.8%) | 0 | - |
| Severe valvular regurgitation | 2 (1.5%) | 2 (1.5%) | 9, 12 |
| Cardiac conduction disorder | 1 (0.8%) | 1 (0.8%) | 11 |
| Exacerbation of coronary artery disease | 2 (1.5%) | 2 (1.5%) | 4, 12 |
| Total | 24 (18.5%) | 14 (10.8%) | - |
| Parameter | No. of Patients | Cardiotoxicity Present in n (%) | p | |
|---|---|---|---|---|
| Ischemic Heart Disease | Yes | 19 | 4 (21.1) | 0.75 a |
| No | 111 | 20 (18.0) | ||
| Hypertension | Yes | 34 | 7 (20.6) | 0.80 a |
| No | 96 | 17 (17.7) | ||
| Diabetes mellitus | Yes | 5 | 1 (20.0) | 1 a |
| No | 125 | 23 (18.4) | ||
| BMI | Normal range | 40 | 6 (15.0) | 0.19 b |
| Overweight | 49 | 13 (26.5) | ||
| Obese | 41 | 5 (12.2) | ||
| NT-proBNP | Elevated | 12 | 3 (25.0) | 0.696 a |
| Within normal limits | 117 | 21 (17.9) | ||
| Myoglobin | Elevated | 46 | 8 (17.4) | 1 a |
| Within normal limits | 83 | 16 (19.3) | ||
| CK-MB | Elevated | 4 | 1 (25.0) | 0.57 a |
| Within normal limits | 125 | 23 (18.4) | ||
| Increase in NT-proBNP level during therapy c | Yes | 10 | 2 (20.0) | 1 a |
| No | 118 | 21 (17.8) | ||
| Increase in myoglobin level during therapy c | Yes | 57 | 10 (17.5) | 1 a |
| No | 71 | 13 (18.3) | ||
| Increase in CK-MB level during therapy c | Yes | 9 | 3 (33.3) | 0.20 a |
| No | 119 | 20 (16.8) | ||
| Radiotherapy | Yes | 102 | 19 (18.6) | 1 a |
| No | 28 | 5 (17.9) | ||
| Hormone therapy | Yes | 66 | 12 (18.2) | 1 a |
| No | 64 | 12 (18.7) | ||
| Chemotherapy | Yes | 127 | 24 (18.9) | 1 a |
| No | 3 | 0 (0.0) | ||
| Docetaxel | Yes | 34 | 9 (26.5) | 0.21 a |
| No | 93 | 15 (16.1) | ||
| No. of docetaxel cycles | 4 | 23 | 4 (17.4) | 0.08 b |
| 1–3 | 11 | 5 (45.4) | ||
| 0 | 93 | 15 (16.1) | ||
| Anthracycline dose [mg/m²] | 240 or 300 | 77 | 13 (16.9) | 0.64 a |
| 360 or 480 | 51 | 11 (21.6) | ||
| Mitral valve insufficiency | Yes | 90 | 18 (20.0) | 0.45 a |
| No | 39 | 5 (12.8) | ||
| Tricuspid valve insufficiency | Yes | 30 | 5 (16. 7) | 1 a |
| No | 99 | 18 (18.2) | ||
| Aortic valve insufficiency | Yes | 24 | 5 (20.8) | 0.77 a |
| No | 105 | 18 (17.1) | ||
| Coexistent regurgitations | Yes | 98 | 20 (20.4) | 0.28 a |
| No | 31 | 3 (9.7) | ||
| Mean Value of 6 Measurements before/during/after Trastuzumab Therapy | |||||
|---|---|---|---|---|---|
| Parameter | Category | N | NT-pro-BNP Mean (SD) | M Mean (SD) | CK-MB Mean (SD) |
| Total | 129 | 88.4 (116.8) | 16.8 (20.9) | 3.0 (9.2) | |
| Age | ≤54 years | 66 | 70.9 (102.8) | 13.7 (7.7) | 2.0 (0.9) |
| >54 years | 63 | 106.8 (128.2) a | 20.1 (28.6) b | 4.0 (13.1) | |
| BMI | Normal weight: BMI ≤ 25 | 48 | 96.8 (122.1) | 14.1 (8.2) | 1.9 (0.8) |
| Overweight: BMI > 25 | 81 | 83.5 (114.1) | 18.5 (25.6) | 3.6 (11.5) | |
| DM | Not present | 124 | 89.4 (118.8) | 17.0 (21.3) | 3.0 (9.4) |
| Present | 5 | 65.3 (43.3) | 12.8 (6.6) | 1.8 (1.0) | |
| AH | Not present | 96 | 88.2 (131.1) | 17.2 (23.8) | 3.3 (10,6) |
| Present | 33 | 89.0 (59.5) | 15.8 (8.1) | 2.0 (1.2) | |
| IHD | Not present | 110 | 85.9 (123.2) | 16.7 (22.23) | 3.1 (9.9) |
| Present | 19 | 103.2 (70.2) | 17.4 (10.98) | 2.0 (0.9) | |
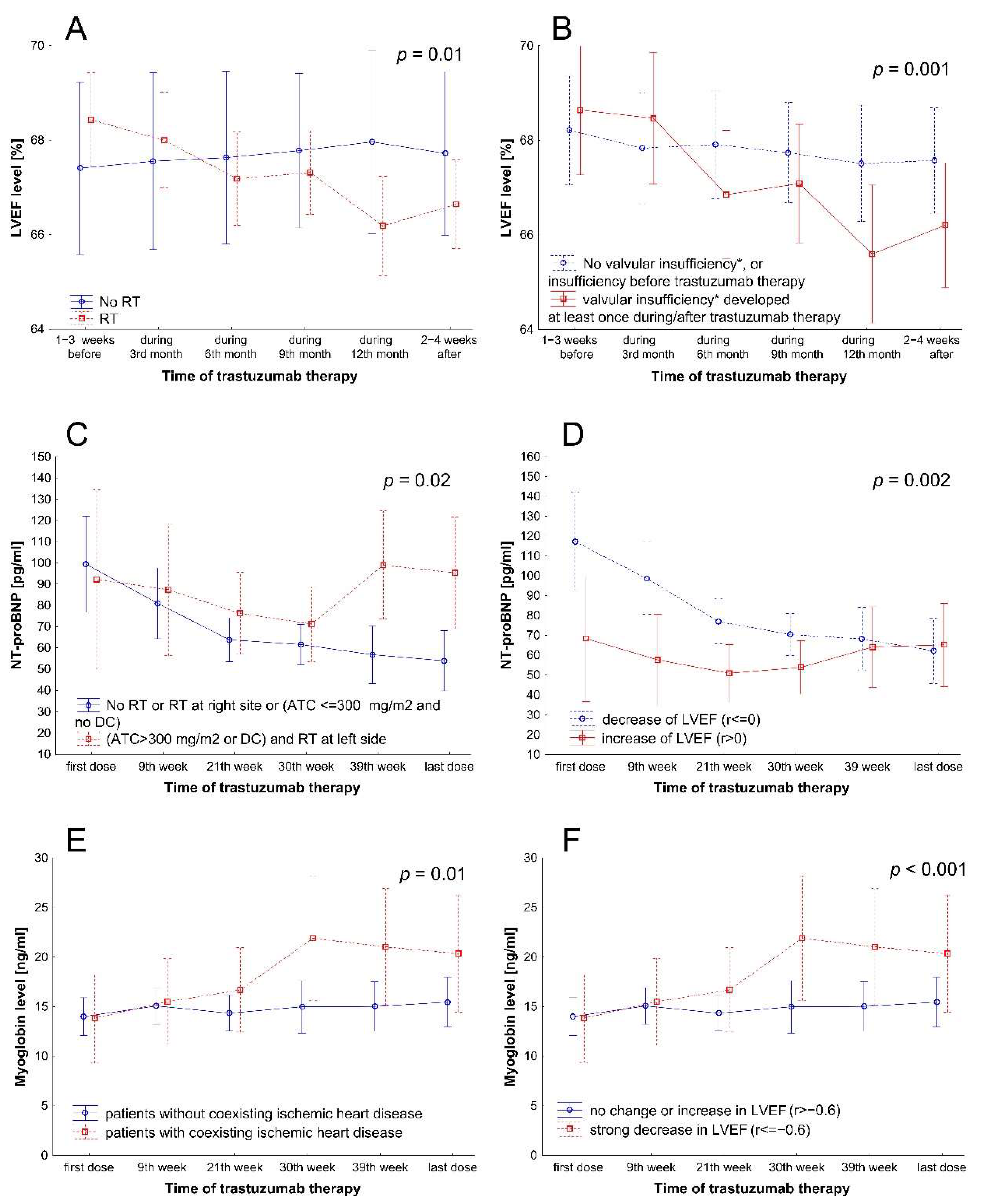
| RT or ChT | No RT or RT at right site or (ATC ≤ 300 mg/m2 and no DC) | 97 | 77.6 (92.5) | 14.5 (8.8) | 2.2 (2.1) |
| (ATC > 300 mg/m2 or DC) and RT at left side | 32 | 121.4 (168.4) b | 23.8 (38.8) | 5.3 (18.1) | |
| HT | Not administered | 62 | 103.2 (157.0) | 19.4 (28.7) | 4.0 (13.2) |
| Administered | 67 | 74.8 (57.3) | 14.4 (8.6) | 2.0 (1.0) | |
| Valvular insufficiency of any grade * | Not present or present before and during/after trastuzumab therapy | 67 | 65.8 (52.1) | 15.8 (10.1) | 2.4 (2.4) |
| Developed during or after (not before) trastuzumab therapy | 47 | 79.1 (48.4) b | 14.3 (8.0) | 2.0 (1.1) | |
| LVEF | Decrease during/after trastuzumab therapy * | 79 | 103.6 (141.1) | 17.8 (26.2) | 3.6 (11.7) |
| Increase during/after trastuzumab therapy ** | 48 | 61.8 (50.0) a | 15.6 (7.0) | 2.0 (0.8) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grela-Wojewoda, A.; Püsküllüoğlu, M.; Sas-Korczyńska, B.; Zemełka, T.; Pacholczak-Madej, R.; Wysocki, W.M.; Wojewoda, T.; Adamczyk, A.; Lompart, J.; Korman, M.; et al. Biomarkers of Trastuzumab-Induced Cardiac Toxicity in HER2- Positive Breast Cancer Patient Population. Cancers 2022, 14, 3353. https://doi.org/10.3390/cancers14143353
Grela-Wojewoda A, Püsküllüoğlu M, Sas-Korczyńska B, Zemełka T, Pacholczak-Madej R, Wysocki WM, Wojewoda T, Adamczyk A, Lompart J, Korman M, et al. Biomarkers of Trastuzumab-Induced Cardiac Toxicity in HER2- Positive Breast Cancer Patient Population. Cancers. 2022; 14(14):3353. https://doi.org/10.3390/cancers14143353
Chicago/Turabian StyleGrela-Wojewoda, Aleksandra, Mirosława Püsküllüoğlu, Beata Sas-Korczyńska, Tomasz Zemełka, Renata Pacholczak-Madej, Wojciech M. Wysocki, Tomasz Wojewoda, Agnieszka Adamczyk, Joanna Lompart, Michał Korman, and et al. 2022. "Biomarkers of Trastuzumab-Induced Cardiac Toxicity in HER2- Positive Breast Cancer Patient Population" Cancers 14, no. 14: 3353. https://doi.org/10.3390/cancers14143353