
Methods for Drainage of Distal Malignant Biliary Obstruction after ERCP Failure: A Systematic Review and Network Meta-Analysis


 , , , , , ,
, , , , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
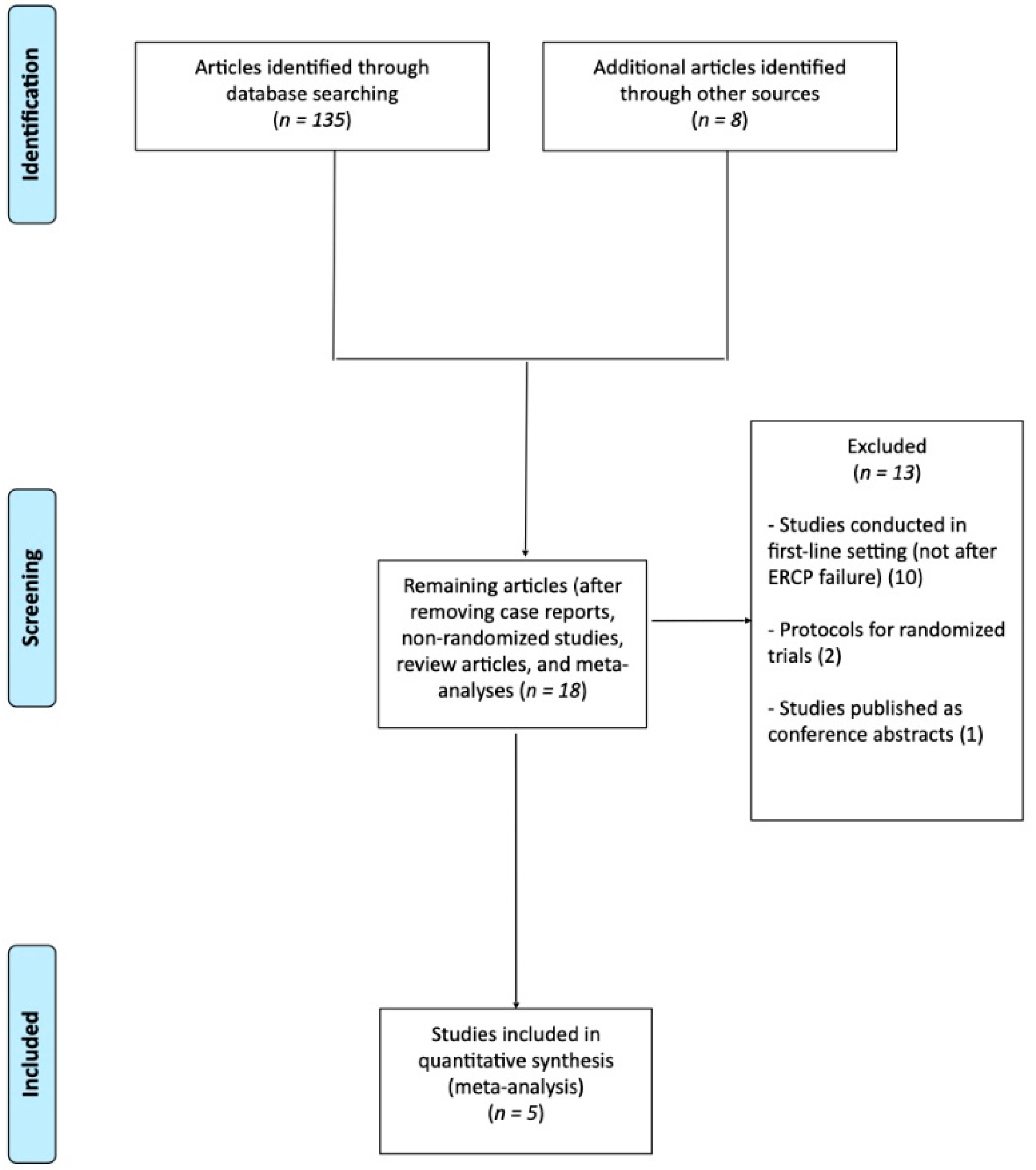
2.1. Selection Criteria
2.2. Search Strategy, Data Abstraction and Risk of Bias Assessment
2.3. Outcomes Assessed
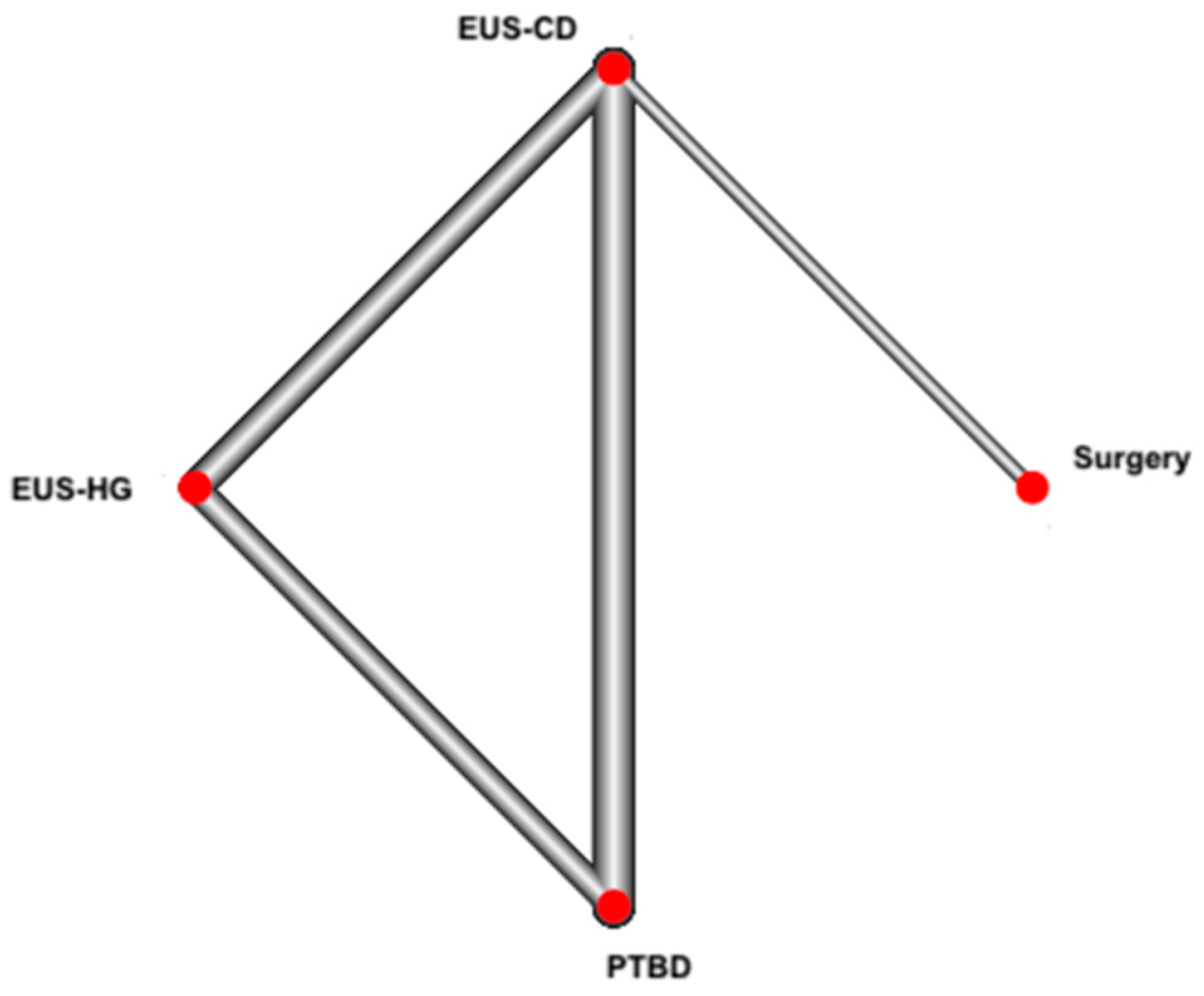
2.4. Statistical Analysis
2.5. Quality of Evidence
3. Results
3.1. Characteristics of Included Studies
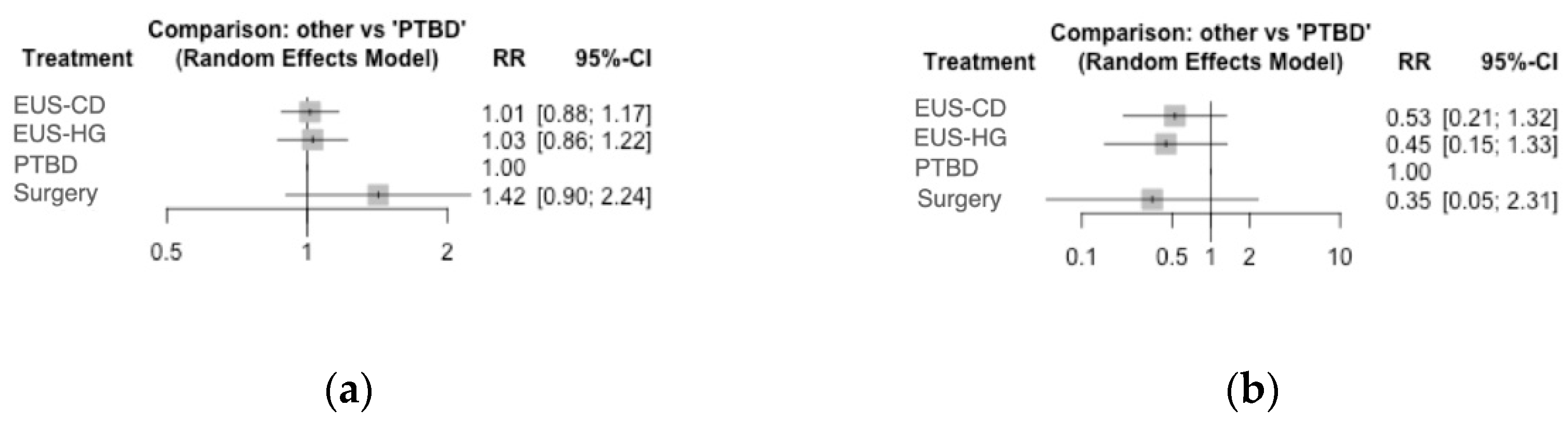
3.2. Clinical Success Rate
3.3. Secondary Outcomes
3.4. Quality of Evidence
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Cote, G.A.; Singh, S.; Bucksot, L.G.; Pannell-Lazzelli, L.; Schmidt, S.E.; Fogel, E.; McHenry, L.; Watkins, J.; Sherman, S. Association between volume of endoscopic retrograde cholangiopancreatography at an academic medical center and use of pancreatobiliary therapy. Clin. Gastroenterol. Hepatol. 2012, 10, 920–924. [Google Scholar] [CrossRef] [PubMed]
- Nennstiel, S.; Weber, A.; Frick, G.; Haller, B.; Meining, A.; Schmid, R.M.; Neu, B. Drainage-related complications in percutaneous transhepatic biliary drainage: An analysis over 10 years. J. Clin. Gastroenterol. 2015, 49, 764–770. [Google Scholar] [CrossRef] [PubMed]
- Oh, H.C.; Lee, S.K.; Lee, T.Y.; Kwon, S.; Lee, S.S.; Seo, D.-W.; Kim, M.-H. Analysis of percutaneous transhepatic cholangioscopy-related complications and the risk factors for those complications. Endoscopy 2007, 39, 731–736. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.A.; Akbar, A.; Baron, T.H.; Khan, S.; Kocak, M.; Alastal, Y.; Hammad, T.; Lee, W.M.; Sofi, A.; Artifon, E.L.A.; et al. Endoscopic ultrasound-guided biliary drainage: A systematic review and meta-analysis. Dig. Dis. Sci. 2016, 61, 684–703. [Google Scholar] [CrossRef] [PubMed]
- Hedjoudje, A.; Sportes, A.; Grabar, S.; Zhang, A.; Koch, S.; Vuitton, L.; Prat, F. Outcomes of endoscopic ultrasound-guided biliary drainage: A systematic review and meta-analysis. United Eur. Gastroenterol. J. 2019, 7, 60–68. [Google Scholar] [CrossRef] [Green Version]
- Wang, K.; Zhu, J.; Xing, L.; Wang, Y.; Jin, Z.; Li, Z. Assessment of efficacy and safety of EUS-guided biliary drainage: A systematic review. Gastrointest. Endosc. 2016, 83, 1218–1227. [Google Scholar] [CrossRef] [PubMed]
- Mao, K.; Hu, B.; Sun, F.; Wan, K. Choledochoduodenostomy versus Hepaticogastrostomy in Endoscopic Ultrasound-guided Drainage for Malignant Biliary Obstruction: A Meta-analysis and Systematic Review. Surg. Laparosc. Endosc. Percutan. Tech. 2021, 32, 124–132. [Google Scholar] [CrossRef]
- Kawakubo, K.; Isayama, H.; Kato, H.; Itoi, T.; Kawakami, H.; Hanada, K.; Ishiwatari, H.; Yasuda, I.; Kawamoto, H.; Itokawa, F.; et al. Multicenter retrospective study of endoscopic ultrasound-guided biliary drainage for malignant biliary obstruction in Japan. J. Hepatobiliary. Pancreat. Sci. 2014, 21, 328–334. [Google Scholar] [CrossRef]
- Uemura, R.S.; Khan, M.A.; Otoch, J.P.; Kahaleh, M.; Montero, E.F.; Artifon, E.L.A. EUS-guided Choledochoduodenostomy versus Hepaticogastrostomy: A Systematic Review and Meta-analysis. J. Clin. Gastroenterol. 2018, 52, 123–130. [Google Scholar] [CrossRef]
- Minaga, K.; Ogura, T.; Shiomi, H.; Imai, H.; Hoki, N.; Takenaka, M.; Nishikiori, H.; Yamashita, Y.; Hisa, T.; Kato, H.; et al. Comparison of the efficacy and safety of endoscopic ultrasound-guided choledochoduodenostomy and hepaticogastrostomy for malignant distal biliary obstruction: Multicenter, randomized, clinical trial. Dig. Endosc. 2019, 31, 575–582. [Google Scholar] [CrossRef] [Green Version]
- Sharaiha, R.Z.; Khan, M.A.; Kamal, F.; Tyberg, A.; Tombazzi, C.R.; Ali, B.; Tombazzi, C.; Kahaleh, M. Efficacy and safety of EUS-guided biliary drainage in comparison with percutaneous biliary drainage when ERCP fails: A systematic review and meta-analysis. Gastrointest. Endosc. 2017, 85, 904–914. [Google Scholar] [CrossRef] [PubMed]
- Dumonceau, J.M.; Tringali, A.; Papanikolaou, I.S.; Blero, D.; Mangiavillano, B.; Schmidt, A.; Vanbiervliet, G.; Costamagna, G.; Devière, J.; García-Cano, J.; et al. Endoscopic biliary stenting: Indications, choice of stents, and results: European Society of Gastrointestinal Endoscopy (ESGE) Clinical Guideline—Updated October 2017. Endoscopy 2018, 50, 910–930. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cotton, P.B.; Eisen, G.M.; Aabakken, L.; Baron, T.H.; Hutter, M.M.; Jacobson, B.C.; Mergener, K.; Nemcej, A., Jr.; Petersen, B.T.; Petrini, J.L.; et al. A lexicon for endoscopic adverse events: Report of an ASGE workshop. Gastrointest. Endosc. 2010, 71, 446–454. [Google Scholar] [CrossRef] [PubMed]
- White, I.R.; Barrett, J.K.; Jackson, D.; Higgins, J.P. Consistency and inconsistency in network meta-analysis: Model estimation using multivariate meta-regression. Res. Synth. Methods 2012, 3, 111–125. [Google Scholar] [CrossRef] [Green Version]
- Salanti, G.; Ades, A.E.; Ioannidis, J.P. Graphical methods and numerical summaries for presenting results from multiple-treatment meta-analysis: An overview and tutorial. J. Clin. Epidemiol. 2011, 64, 163–171. [Google Scholar] [CrossRef] [PubMed]
- Puhan, M.A.; Schünemann, H.J.; Murad, M.H.; Li, T.; Brignardello-Petersen, R.; Singh, J.A.; Kessels, A.G.; Guyatt, G.H. A GRADE Working Group approach for rating the quality of treatment effect estimates from network meta-analysis. BMJ 2014, 349, g5630. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Artifon, E.L.; Aparicio, D.; Paione, J.B.; Lo, S.K.; Bordini, A.; Rabello, C.; Otoch, J.P.; Gupta, K. Biliary drainage in patients with unresectable, malignant obstruction where ERCP fails: Endoscopic ultrasonography-guided choledochoduodenostomy versus percutaneous drainage. J. Clin. Gastroenterol. 2012, 46, 768–774. [Google Scholar] [CrossRef] [PubMed]
- Lee, T.H.; Choi, J.H.; do Park, H.; Song, T.J.; Kim, D.U.; Paik, W.H.; Hwangbo, Y.; Lee, S.S.; Seo, D.W.; Lee, S.K.; et al. Similar Efficacies of Endoscopic Ultrasound-guided Transmural and Percutaneous Drainage for Malignant Distal Biliary Obstruction. Clin. Gastroenterol. Hepatol. 2016, 14, 1011–1019. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Artifon, E.L.; Loureiro, J.F.; Baron, T.H.; Fernandes, K.; Kahaleh, M.; Marson, F.P. Surgery or EUS-guided choledochoduodenostomy for malignant distal biliary obstruction after ERCP failure. Endosc. Ultrasound 2015, 4, 235–243. [Google Scholar] [CrossRef] [Green Version]
- Artifon, E.L.; Marson, F.P.; Gaidhane, M.; Kahaleh, M.; Otoch, J.P. Hepaticogastrostomy or choledochoduodenostomy for distal malignant biliary obstruction after failed ERCP: Is there any difference? Gastrointest. Endosc. 2015, 81, 950–959. [Google Scholar] [CrossRef] [PubMed]
- Giovannini, M.; Moutardier, V.; Pesenti, C.; Bories, E.; Lelong, B.; Delpero, J.R. Endoscopic ultrasound-guided bilioduodenal anastomosis: A new technique for biliary drainage. Endoscopy 2001, 33, 898–900. [Google Scholar] [CrossRef] [PubMed]
- Mangiavillano, B.; Moon, J.H.; Crinò, S.F.; Larghi, A.; Pham, K.D.; Teoh, A.Y.B.; Paduano, D.; Lee, Y.N.; Yoo, H.W.; Shin, I.S.; et al. Safety and efficacy of a novel electrocautery-enhanced lumen-apposing metal stent in interventional EUS procedures (with video). Gastrointest. Endosc. 2022, 95, 115–122. [Google Scholar] [CrossRef] [PubMed]
- Teoh, A.Y.B.; Kongkam, P.; Bapaye, A.; Ratanachu, T.; Reknimitr, R.; Lakthakia, S.; Chan, S.M.; Gadhikar, H.P.; Korrapati, S.K.; Lee, Y.N.; et al. Use of a novel lumen apposing metallic stent for drainage of the bile duct and gallbladder: Long term outcomes of a prospective international trial. Dig. Endosc. 2021, 33, 1139–1145. [Google Scholar] [CrossRef]
- Amato, A.; Sinagra, E.; Celsa, C.; Enea, M.; Buda, A.; Vieceli, F.; Scaramella, L.; Belletrutti, P.; Fugazza, A.; Cammà, C.; et al. Efficacy of lumen-apposing metal stents or self-expandable metal stents for endoscopic ultrasound-guided choledochoduodenostomy: A systematic review and meta-analysis. Endoscopy 2021, 53, 1037–1047. [Google Scholar] [CrossRef] [PubMed]
- Fugazza, A.; Fabbri, C.; Di Mitri, R.; Petrone, M.C.; Colombo, M.; Cugia, L.; Amato, A.; Forti, E.; Binda, C.; Maida, M.; et al. EUS-guided choledochoduodenostomy for malignant distal biliary obstruction after failed ERCP: A retrospective nationwide analysis. Gastrointest. Endosc. 2022, 95, 896.e1–904.e1. [Google Scholar] [CrossRef] [PubMed]
- Giovannini, M.; Napoleon, B.; Barthet, M.; Caillol, F.; Pesenti, C. Multicenter randomized phase II study: Percutaneous biliary drainage vs EUS guided biliary drainage: Results of the intermediate analysis [abstract]. Gastrointest. Endosc. 2015, 81, AB174. [Google Scholar] [CrossRef]
- Anderloni, A.; Fugazza, A.; Spadaccini, M.; Colombo, M.; Gabbiadini, R.; Siracusano, L.V.; Pressiani, T.; Repici, A. Single-session EUS-guided gastroenterostomy and hepaticogastrostomy using dedicated metal stents (with videos). Endosc. Ultrasound 2021, 10, 214–215. [Google Scholar] [CrossRef]
- Salerno, R.; Davies, S.E.C.; Mezzina, N.; Ardizzone, S. Comprehensive review on EUS-guided biliary drainage. World J. Gastrointest. Endosc. 2019, 11, 354–364. [Google Scholar] [CrossRef]
- Spadaccini, M.; Binda, C.; Fugazza, A.; Repici, A.; Tarantino, I.; Fabbri, C.; Cugia, L.; Anderloni, A.; On Behalf of the Interventional Endoscopy Amp Ultra Sound I-Eus Group. Informed Consent for Endoscopic Biliary Drainage: Time for a New Paradigm. Medicina 2022, 58, 331. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Study, Year | Location; Time Period | Neoplasia | Intervention (N) | Control (N) | Max Diameter Common Bile Duct (mm) | Age | Gender, Male | Definition of Clinical Success |
|---|---|---|---|---|---|---|---|---|
| EUS-choledochoduodenostomy vs. PTBD | ||||||||
| Artifon, 2012 [18] | Brazil; 2007–2011 | Pancreatic adenocarcinoma 16, Ampullary adenocarcinoma 1, Hematologic neoplasia 2, Cholangiocarcinoma 2, Metastasis 3, Gastric carcinoma 1. | EUS-CD with SEMS (13) | PTBD with SEMS (12) | EUS-CD 13.7 (9 to 28) PTBD 11.9 (8 to 23) | EUS-CD 63.4 ± 11.1 PTBD 71 ± 11.9 | EUS-CD 9 (69.2%) PTBD 8 (66.6%) | Improvement of clinical symptoms and decrease in liver enzymes |
| Lee, 2016 (I) [19] * | Korea; 2014–2015 | Cholangiocarcinoma 21, Pancreatic adenocarcinoma 24, Gallbladder carcinoma 8, Ampullary adenocarcinoma 1, Metastasis 4, Gastric carcinoma cancer 5, Duodenal carcinoma 3 | EUS-CD with SEMS (8) | PTBD with SEMS (32) | EUS-CD 11.2 ± 4.38 PTBD 12.6 ± 6.18 | EUS-CD 66.5 (40–83) PTBD 68.4 (52–82) | EUS-CD NR PTBD 24 (75%) | Decrease in bilirubin level to less than 50% of baseline within 7 days, or less than 75% within 30 days. |
| EUS-choledochoduodenostomy vs. Surgical hepaticojejunostomy | ||||||||
| Artifon, 2015 [20] | Brazil; 2011–2013 | NR | EUS-CD with SEMS (16) | Surgical hepaticojejunostomy (16) | EUS-CD 20 Hepaticojejunostomy 20 | EUS-CD 65 ± 12.2 Hepaticojejunostomy 68.1 ± 19.5 | EUS-CD 7 (43.7%) Hepaticojejunostomy 7 (43.7%) | Decrease in bilirubin level to less than 50% of baseline within 7 days |
| EUS-choledochoduodenostomy vs. EUS-hepaticogastrostomy | ||||||||
| Minaga, 2019 [10] | Japan; 2013–2016 | Pancreatobiliary cancer 41, Other 6 | EUS-CD with SEMS (23) | EUS-HG with SEMS (24) | NR | EUS-CD 73 (41–83) EUS-HG 72.5 (46–88) | EUS-CD 10 (43.4%) EUS-HG 14 (58.3%) | Decrease in bilirubin level to less than 50% of baseline within 14 days |
| Artifon, 2015 [21] | Brazil; 2010–2013 | Pancreatic adenocarcinoma 33, Metastatic adenopathy 8, Ampullary carcinoma 4, Neuroendocrine tumor 2, Gallbladder cancer 1, Duodenal carcinoma 1 | EUS-CD with SEMS (24) | EUS-HG with SEMS (25) | EUS-CD 22.23 ± 4.09 EUS-HG 21.43 ± 4.88 | EUS-CD 65.7 (15–74) EUS-HG 66.25 (14–28) | EUS-CD 11 (45.8%) EUS-HG 11 (44%) | Decrease in bilirubin level to less than 50% of baseline within 7 days |
| EUS-hepaticogastrostomy vs. PTBD | ||||||||
| Lee, 2016 (II) [19] * | Korea; 2014–2015 | Cholangiocarcinoma 21, Pancreatic adenocarcinoma 24, Gallbladder carcinoma 8, Ampullary adenocarcinoma 1, Metastasis 4, Gastric carcinoma cancer 5, Duodenal carcinoma 3 | EUS-HG with SEMS (24) | PTBD with SEMS (32) | NR PTBD 12.6 ± 6.18 | EUS-HG 66.5 (40–83) PTBD 68.4 (52–82) | EUS-HG NR PTBD 24 (75%) | Decrease in bilirubin level to less than 50% of baseline within 7 days, or less than 75% within 30 days. |
| Clinical Success Rate | Adverse Event Rate | |||
|---|---|---|---|---|
| Risk Ratio (95% CI) | Quality of Evidence | Risk Ratio (95% CI) | Quality of Evidence | |
| All treatments vs. PTBD | ||||
| EUS-CD | 1.01 (0.88–1.17) | Low | 0.53 (0.21–1.32) | Low |
| EUS-HG | 1.03 (0.86–1.22) | Low | 0.45 (0.15–1.33) | Low |
| Surgery | 1.42 (0.90–2.24) | Low | 0.35 (0.05–2.31) | Low |
| vs. EUS-CD | ||||
| EUS-HG | 1.01 (0.87–1.17) | Low | 0.85 (0.39–1.82) | Low |
| Surgery | 1.40 (0.91–2.13) | Low | 0.66 (0.12–3.46) | Low |
| vs. EUS-HG | ||||
| Surgery | 1.38 (0.88–2.16) | Low | 0.78 (0.12–4.83) | Low |
| Clinical Success Rate | Adverse Event Rate | ||
|---|---|---|---|
| Surgery | 0.54 | Surgery | 0.63 |
| EUS-HG | 0.42 | EUS-HG | 0.57 |
| EUS-CD | 0.34 | EUS-CD | 0.48 |
| PTBD | 0.31 | PTBD | 0.13 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Facciorusso, A.; Mangiavillano, B.; Paduano, D.; Binda, C.; Crinò, S.F.; Gkolfakis, P.; Ramai, D.; Fugazza, A.; Tarantino, I.; Lisotti, A.; et al. Methods for Drainage of Distal Malignant Biliary Obstruction after ERCP Failure: A Systematic Review and Network Meta-Analysis. Cancers 2022, 14, 3291. https://doi.org/10.3390/cancers14133291
Facciorusso A, Mangiavillano B, Paduano D, Binda C, Crinò SF, Gkolfakis P, Ramai D, Fugazza A, Tarantino I, Lisotti A, et al. Methods for Drainage of Distal Malignant Biliary Obstruction after ERCP Failure: A Systematic Review and Network Meta-Analysis. Cancers. 2022; 14(13):3291. https://doi.org/10.3390/cancers14133291
Chicago/Turabian StyleFacciorusso, Antonio, Benedetto Mangiavillano, Danilo Paduano, Cecilia Binda, Stefano Francesco Crinò, Paraskevas Gkolfakis, Daryl Ramai, Alessandro Fugazza, Ilaria Tarantino, Andrea Lisotti, and et al. 2022. "Methods for Drainage of Distal Malignant Biliary Obstruction after ERCP Failure: A Systematic Review and Network Meta-Analysis" Cancers 14, no. 13: 3291. https://doi.org/10.3390/cancers14133291