
Machine Learning Based on MRI DWI Radiomics Features for Prognostic Prediction in Nasopharyngeal Carcinoma

 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Inclusion and Exclusion Criteria
2.3. Endpoints
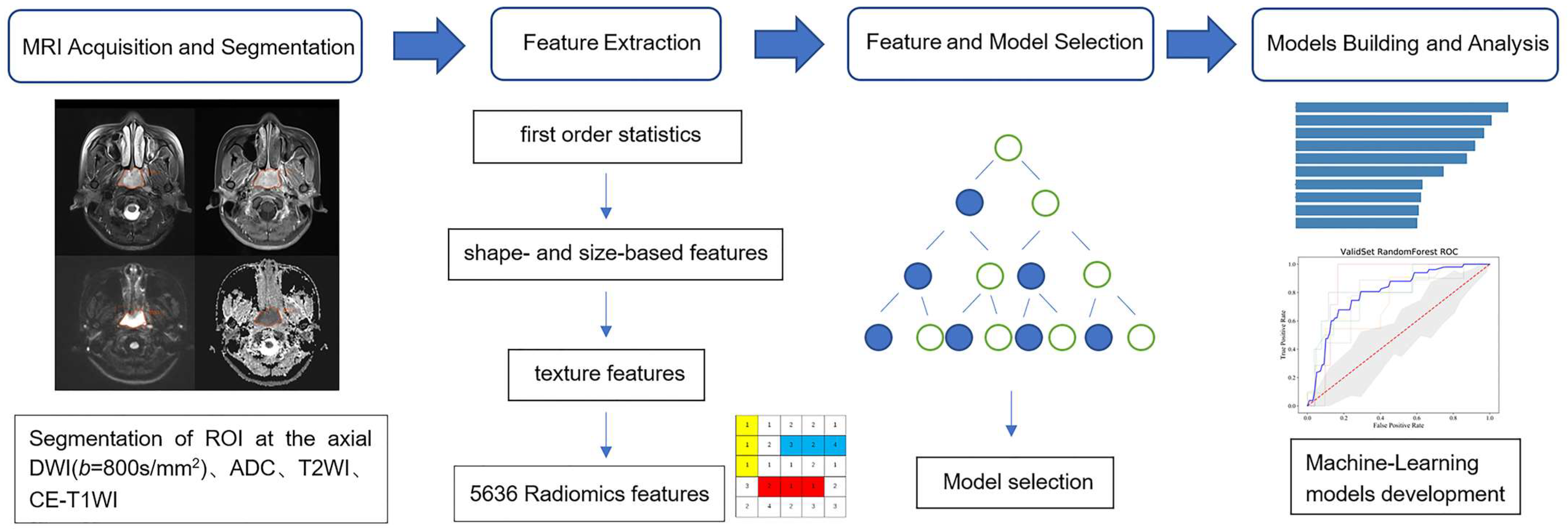
2.4. MRI Acquisition
2.5. Segmentation and Feature Extraction
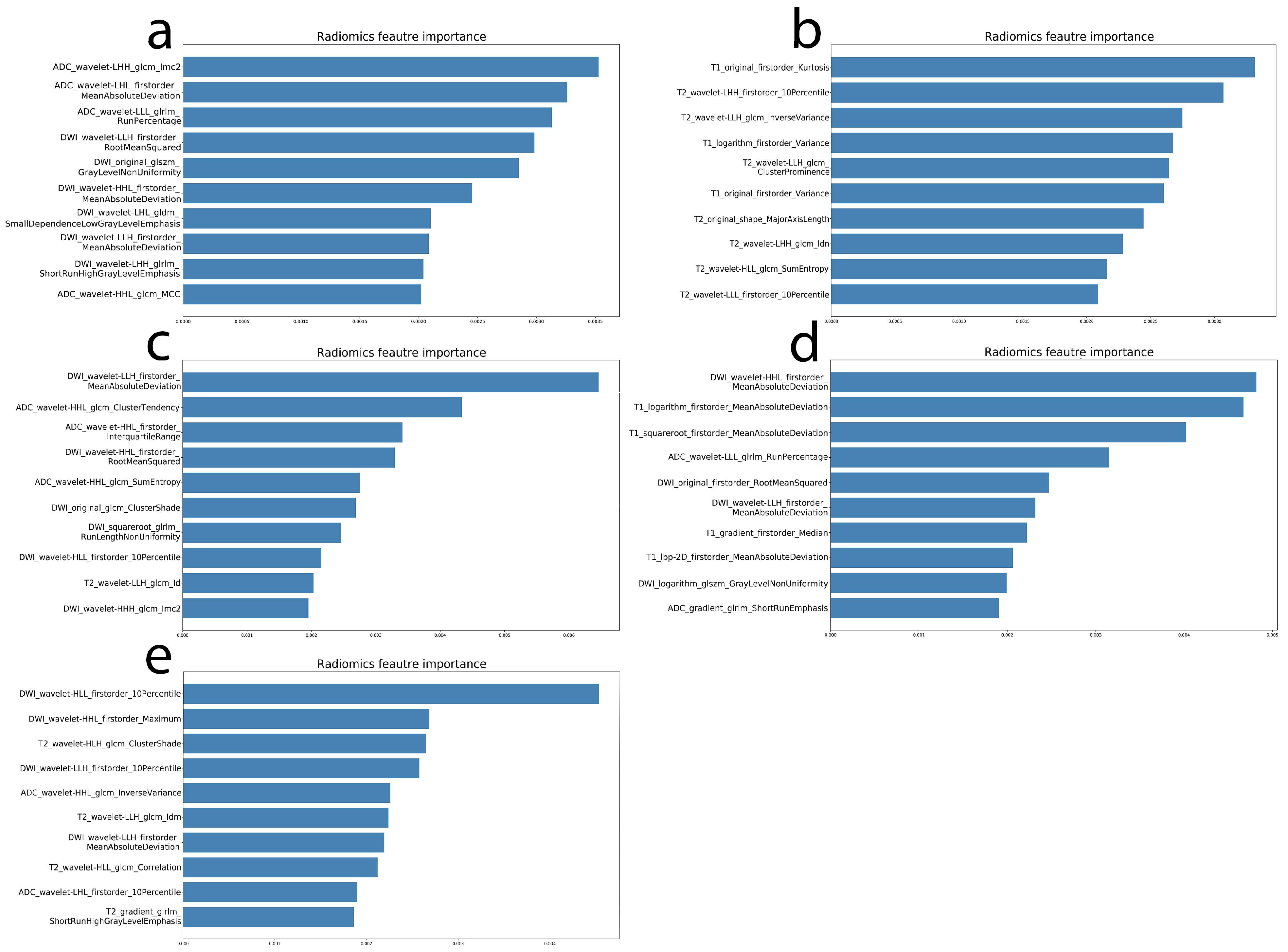
2.6. Radiomics Feature and Model Selection
2.7. Prediction Model Building
3. Results
3.1. Clinical Characteristics Analysis
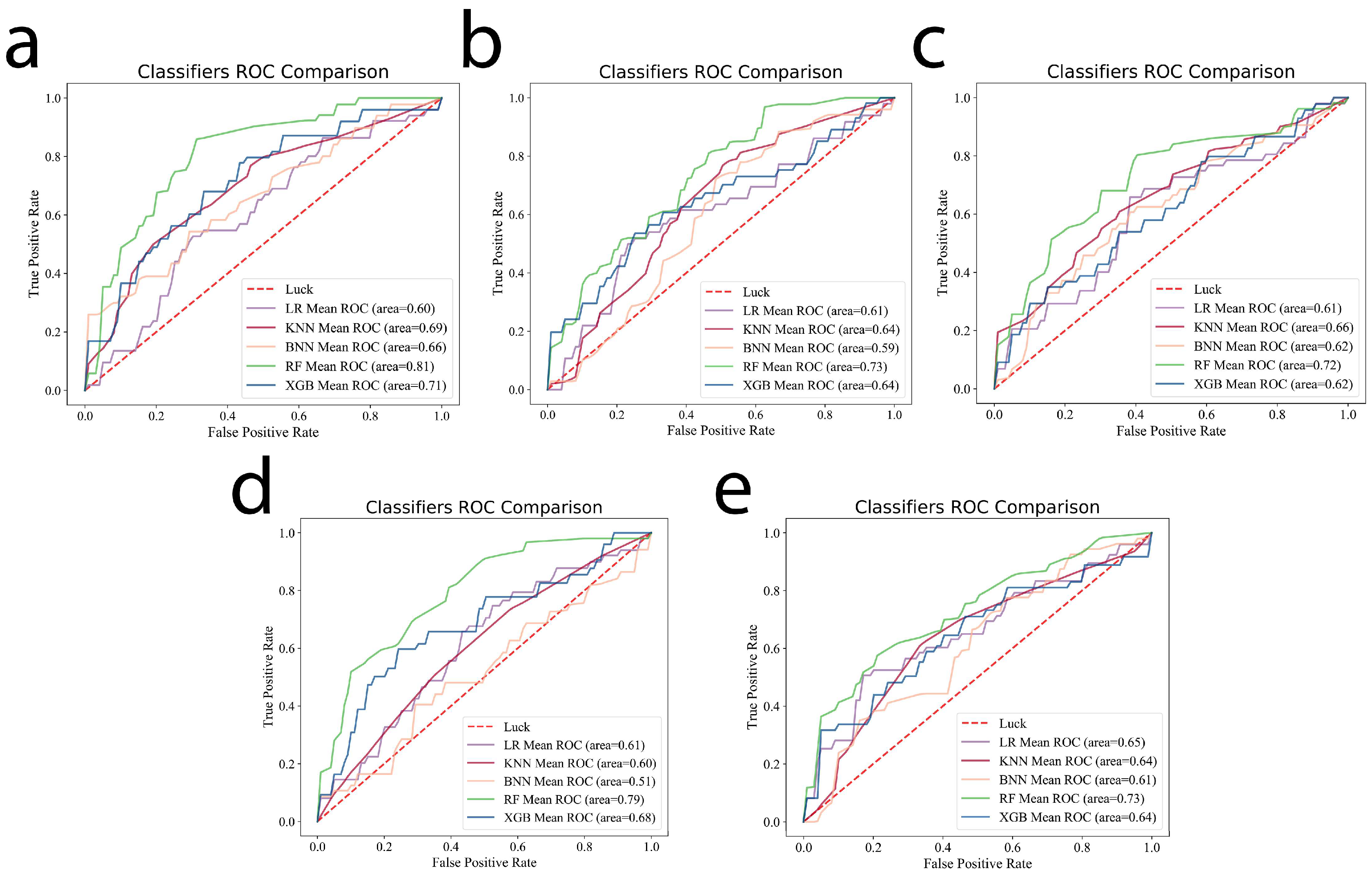
3.2. Machine Learning Model Selection
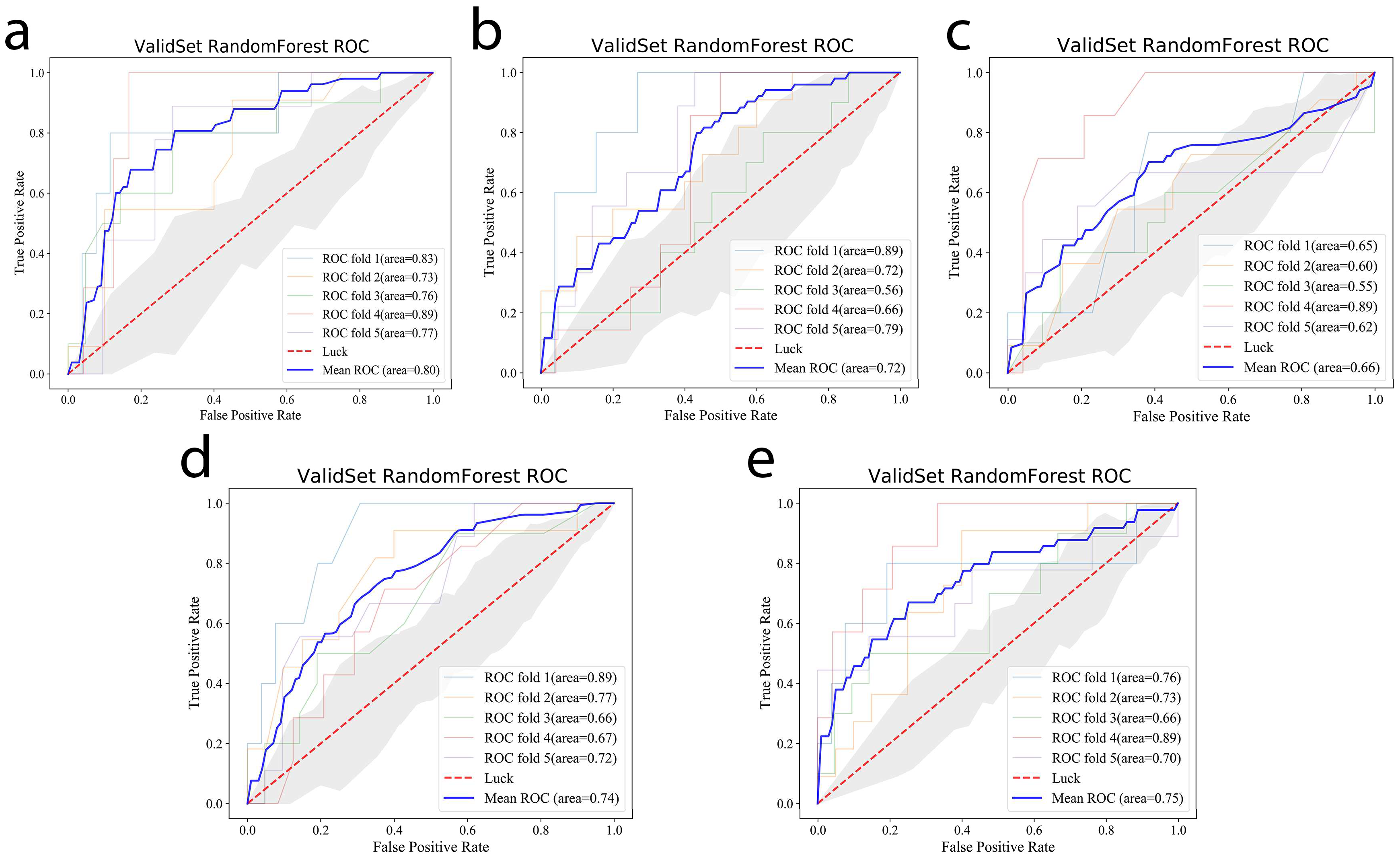
3.3. Prediction Performance of the Models
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chen, Y.P.; Chan, A.T.; Le, Q.T.; Blanchard, P.; Sun, Y.; Ma, J. Nasopharyngeal carcinoma. Lancet 2019, 394, 64–80. [Google Scholar] [CrossRef]
- Jozkowiak, M.; Dyszkiewicz-Konwinska, M.; Ramlau, P.; Kranc, W.; Spaczynska, J.; Wierzchowski, M.; Kaczmarek, M.; Jodynis-Liebert, J.; Piotrowska-Kempisty, H. Individual and Combined Treatments with Methylated Resveratrol Analogue DMU-214 and Gefitinib Inhibit Tongue Cancer Cells Growth via Apoptosis Induction and EGFR Inhibition. Int. J. Mol. Sci. 2021, 22, 6180. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.W.; Ma, B.B.; Ng, W.T.; Chan, A.T. Management of Nasopharyngeal Carcinoma: Current Practice and Future Perspective. J. Clin. Oncol. 2015, 33, 3356–3364. [Google Scholar] [CrossRef]
- Dagogo-Jack, I.; Shaw, T.A. Tumour heterogeneity and resistance to cancer therapies. Nat. Rev. Clin. Oncol. 2018, 15, 81–94. [Google Scholar] [CrossRef]
- Li, X.H.; Chang, H.; Xu, B.Q.; Tao, Y.L.; Gao, J.; Chen, C.; Qu, C.; Zhou, S.; Liu, S.R.; Wang, X.H.; et al. An inflammatory biomarker-based nomogram to predict prognosis of patients with nasopharyngeal carcinoma: An analysis of a prospective study. Cancer Med. 2017, 6, 310–319. [Google Scholar] [CrossRef]
- Nilsson, J.S.; Forslund, O.; Andersson, F.C.; Lindstedt, M.; Greiff, L. Intralesional EBV-DNA load as marker of prognosis for nasopharyngeal cancer. Sci. Rep. 2019, 9, 15432. [Google Scholar] [CrossRef] [Green Version]
- Li, G.; Gao, J.; Tao, Y.L.; Xu, B.Q.; Tu, Z.W.; Liu, Z.G.; Zeng, M.S. Increased pretreatment levels of serum LDH and ALP as poor prognostic factors for nasopharyngeal carcinoma. Chin. J. Cancer Res. 2019, 31, 197–206. [Google Scholar] [CrossRef] [Green Version]
- Liu, N.; Chen, N.Y.; Cui, R.X.; Li, W.F.; Li, Y.; Wei, R.R.; Zhang, M.Y.; Sun, Y.; Huang, B.J.; Chen, M.; et al. Prognostic value of a microRNA signature in nasopharyngeal carcinoma a microRNA expression analysis. Lancet Oncol. 2012, 13, 633–641. [Google Scholar] [CrossRef]
- Ren, X.Y.; Yang, X.J.; Cheng, B.; Chen, X.Z.; Zhang, T.p.; He, Q.m.; Li, B.; Li, Y.; Tang, X.; Wen, X.; et al. HOPX hypermethylation promotes metastasis via activating SNAIL transcription in nasopharyngeal carcinoma. Nat. Commun. 2017, 8, 14053. [Google Scholar] [CrossRef]
- Engku, N.S.; Ahmad, A.I.; Chan, Y.Y. Diagnostic and Prognostic Indications of Nasopharyngeal Carcinoma. Diagnostics 2020, 10, 611. [Google Scholar] [CrossRef]
- Su, L.; Zhang, M.W.; Zhang, W.J.; Cai, C.; Hong, J. Pretreatment hematologic markers as prognostic factors in patients with nasopharyngeal carcinoma: A systematic review and meta-analysis. Medicine 2017, 96, e6364. [Google Scholar] [CrossRef] [PubMed]
- Lambin, P.; Leijenaar, R.T.; Deist, T.M.; Peerlings, J.; de Jong, E.E.C.; Timmeren, J.V.; Sanduleanu, S.; Larue, R.; Even, A.J.G.; Jochems, A.; et al. Radiomics: The bridge between medical imaging and personalized medicine. Nat. Rev. Clin. Oncol. 2017, 14, 749–762. [Google Scholar] [CrossRef] [PubMed]
- Limkin, E.J.; Sun, R.; Dercle, L.; Zacharaki, E.I.; Robert, C.; Reuz, S.; Schernberg, A.; Paragios, N.; Deutsch, E.; Fert, C. Promises and challenges for the implementation of computational medical imaging (radiomics) in oncology. Ann. Oncol. 2017, 28, 1191–1206. [Google Scholar] [CrossRef] [PubMed]
- Zhao, L.; Gong, J.; Xi, Y.B.; Xu, M.; Li, C.; Kang, X.W.; Yin, Y.T.; Qin, W.; Yin, H.; Shi, M. MRI-based radiomics nomogram may predict the response to induction chemotherapy and survival in locally advanced nasopharyngeal carcinoma. Eur. Radiol. 2020, 30, 537–546. [Google Scholar] [CrossRef]
- Zhang, B.; Ouyang, F.S.; Gu, D.S.; Dong, Y.H.; Zhang, L.; Mo, X.K.; Huang, W.H.; Xing, Z.S. Advanced nasopharyngeal carcinoma: Pre-treatment prediction of progression based on multi-parametric MRI radiomics. Oncotarget 2017, 8, 72457–72465. [Google Scholar] [CrossRef] [Green Version]
- Kim, M.J.; Choi, Y.; Sung, Y.E.; Lee, Y.S.; Kim, Y.S.; Ahn, K.J.; Kim, M.S. Early risk-assessment of patients with nasopharyngeal carcinoma: The added prognostic value of MR-based radiomics. Transl. Oncol. 2021, 14, 101180. [Google Scholar] [CrossRef]
- Tang, L.; Zhou, X.J. Diffusion MRI of cancer: From low to high b-values. J. Magn. Reson. Imaging 2019, 49, 23–40. [Google Scholar] [CrossRef] [Green Version]
- Messina, C.; Bignone, R.; Bruno, A.; Bruno, A.; Bruno, F.; Calandri, M.; Caruso, D.; Coppolino, P.; Robertis, R.D.; Gentili, F.; et al. Diffusion-Weighted Imaging in Oncology: An Update. Cancers 2020, 12, 1493. [Google Scholar] [CrossRef]
- Norris, C.D.; Quick, S.E.; Parker, J.G.; Koontz, N.A. Diffusion MR Imaging in the Head and Neck: Principles and Applications. Neuroimaging Clin. N. Am. 2020, 30, 261–282. [Google Scholar] [CrossRef]
- Widmann, G.; Henninger, B.; Kremser, C.; Jaschke, W. MRI Sequences in Head & Neck Radiology—State of the Art. Rofo 2017, 189, 413–422. [Google Scholar] [CrossRef] [Green Version]
- Zhang, S.H.; Song, M.F.; Zhao, Y.S.; Xu, S.S.; Sun, Q.C.; Zhai, G.; Liang, D.; Wu, G.; Li, Z.C. Radiomics nomogram for preoperative prediction of progression-free survival using diffusion-weighted imaging in patients with muscle-invasive bladder cancer. Eur. J. Radiol. 2020, 131, 109–219. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Wu, J.J.; Zhang, Q.H.; Hua, Z.Y.; Qi, W.J.; Wang, N.; Lin, T.; Sheng, L.J.; Cui, D.H.; Liu, J.H.; et al. Radiomics Analysis Based on Multiparametric MRI for Predicting Early Recurrence in Hepatocellular Carcinoma After Partial Hepatectomy. J. Magn. Reson. Imaging 2021, 53, 1066–1079. [Google Scholar] [CrossRef] [PubMed]
- Zhong, Q.Z.; Long, L.H.; Liu, A.; Li, C.M.; Xiu, X.; Hou, X.Y.; Wu, Q.H.; Gao, H.; Xu, Y.G.; Zhao, T.; et al. Radiomics of Multiparametric MRI to Predict Biochemical Recurrence of Localized Prostate Cancer After Radiation Therapy. Front. Oncol. 2020, 10, 731. [Google Scholar] [CrossRef]
- Amin, M. AJCC Cancer Staging Manual, 8th ed.; Springer: Berlin/Heidelberg, Germany, 2018. [Google Scholar]
- Ou, S.I.; Zell, J.A.; Ziogas, A.; Anton-Culver, H. Epidemiology of nasopharyngeal carcinoma in the United States: Improved survival of Chinese patients within the keratinizing squamous cell carcinoma histology. Ann. Oncol. 2007, 18, 29–35. [Google Scholar] [CrossRef]
- Breiman, L. Random Forests. Mach. Learn. 2001, 45, 5–32. [Google Scholar] [CrossRef] [Green Version]
- Efron, B.; Tibshirani, R. Improvements on Cross-Validation: The 632+ Bootstrap Method. J. Am. Stat. Assoc. 1997, 92, 548–560. [Google Scholar] [CrossRef]
- Li, S.; Deng, Y.Q.; Zhu, Z.L.; Hua, H.L.; Tao, Z.Z. A Comprehensive Review on Radiomics and Deep Learning for Nasopharyngeal Carcinoma Imaging. Diagnostics 2021, 11, 1523. [Google Scholar] [CrossRef]
- Gao, Y.; Mao, Y.T.; Lu, S.H.; Tan, L.; Li, G.; Chen, J.; Huang, D.H.; Zhang, X.; Qiu, Y.Z.; Liu, Y. Magnetic resonance imaging-based radiogenomics analysis for predicting prognosis and gene expression profile in advanced nasopharyngeal carcinoma. Head Neck 2021, 43, 3730–3742. [Google Scholar] [CrossRef]
- Zhang, B.; Tian, J.; Dong, D.; Gu, D.S.; Dong, Y.H.; Zhang, L.; Lian, Z.Y.; Liu, J.; Luo, X.N.; Pei, S.F.; et al. Radiomics Features of Multiparametric MRI as Novel Prognostic Factors in Advanced Nasopharyngeal Carcinoma. Clin. Cancer Res. 2017, 23, 4259–4269. [Google Scholar] [CrossRef] [Green Version]
- Kang, L.; Niu, Y.L.; Huang, R.; Lin, S.; Tang, Q.L.; Chen, A.L.; Fan, Y.X.; Lang, J.Y.; Yin, G.; Zhang, P. Predictive Value of a Combined Model Based on Pre-Treatment and Mid-Treatment MRI-Radiomics for Disease Progression or Death in Locally Advanced Nasopharyngeal Carcinoma. Front. Oncol. 2021, 11, 774455. [Google Scholar] [CrossRef]
- Yang, K.X.; Tian, J.F.; Zhang, B.; Li, M.; Xie, W.J.; Zou, Y.T.; Tan, Q.Y.; Liu, L.H.; Zhu, J.B.; Shou, A.; et al. A multidimensional nomogram combining overall stage, dose volume histogram parameters and radiomics to predict progression-free survival in patients with locoregionally advanced nasopharyngeal carcinoma. Oral Oncol. 2019, 98, 85–91. [Google Scholar] [CrossRef]
- Gatenby, R.A.; Grove, O.; Gillies, R.J. Quantitative imaging in Cancer evolution and ecology. Radiology 2013, 269, 8–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oostendorp, M.; Post, M.J.; Backes, W.H. Vessel Growth and Function: Depiction with Contrast-enhanced MR Imaging. Radiology 2009, 251, 217–335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, C.R.; Cheng, P.; Cheng, J.L.; Zhang, Y.; Sun, M.T.; Xie, S.S.; Zhang, X.N. Differential diagnosis of nasopharyngeal carcinoma and nasopharyngeal lymphoma based on DCE-MRI and RESOLVE-DWI. Eur. Radiol. 2020, 30, 110–118. [Google Scholar] [CrossRef] [PubMed]
- Baxter, G.C.; Graves, M.J.; Gilbert, F.J.; Patterson, A.J. A Meta-analysis of the Diagnostic Performance of Diffusion MRI for Breast Lesion Characterization. Radiology 2019, 291, 632–641. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Type | Positive (%) N = 42 | Negative (%) N = 112 | p-Value |
|---|---|---|---|---|
| Gender | Male | 34 | 77 | 0.516 |
| Female | 8 | 35 | ||
| Age (years) | Range | 19–68 | 23–63 | 0.810 |
| Overall stage | I | 0 | 2 | 0.026 |
| II | 3 | 20 | ||
| III | 17 | 56 | ||
| IVa | 17 | 34 | ||
| IVb | 5 | 0 | ||
| T stage | I | 2 | 25 | 0.915 |
| II | 12 | 22 | ||
| III | 13 | 37 | ||
| IV | 15 | 28 | ||
| N stage | 0 | 1 | 9 | 0.034 |
| 1 | 11 | 48 | ||
| 2 | 21 | 45 | ||
| 3 | 9 | 10 | ||
| M stage | 0 | 42 | 107 | 0.085 |
| 1 | 0 | 5 | ||
| Histology | WHO type I | 0 | 1 | |
| WHO type II–III | 42 | 111 | 0.540 |
| Models | AUC | Accuracy | Specificity | Precision |
|---|---|---|---|---|
| DWI + ADC | 0.80 (95% CI: 0.79–0.81) | 0.766 | 0.926 | 0.620 |
| T2WI + CE-T1WI | 0.72 (95% CI: 0.71–0.74) | 0.752 | 0.930 | 0.520 |
| DWI + ADC + T2WI | 0.66 (95% CI: 0.64–0.68) | 0.779 | 0.925 | 0.689 |
| DWI + ADC + CE-T1WI | 0.74(95% CI: 0.73–0.76) | 0.766 | 0.918 | 0.548 |
| DWI + ADC + T2WI + CE-T1WI | 0.75 (95% CI: 0.74–0.76) | 0.766 | 0.923 | 0.811 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hu, Q.; Wang, G.; Song, X.; Wan, J.; Li, M.; Zhang, F.; Chen, Q.; Cao, X.; Li, S.; Wang, Y. Machine Learning Based on MRI DWI Radiomics Features for Prognostic Prediction in Nasopharyngeal Carcinoma. Cancers 2022, 14, 3201. https://doi.org/10.3390/cancers14133201
Hu Q, Wang G, Song X, Wan J, Li M, Zhang F, Chen Q, Cao X, Li S, Wang Y. Machine Learning Based on MRI DWI Radiomics Features for Prognostic Prediction in Nasopharyngeal Carcinoma. Cancers. 2022; 14(13):3201. https://doi.org/10.3390/cancers14133201
Chicago/Turabian StyleHu, Qiyi, Guojie Wang, Xiaoyi Song, Jingjing Wan, Man Li, Fan Zhang, Qingling Chen, Xiaoling Cao, Shaolin Li, and Ying Wang. 2022. "Machine Learning Based on MRI DWI Radiomics Features for Prognostic Prediction in Nasopharyngeal Carcinoma" Cancers 14, no. 13: 3201. https://doi.org/10.3390/cancers14133201