
Postoperative Recurrences in Patients Operated for Pheochromocytomas and Paragangliomas: New Data Supporting Lifelong Surveillance

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Statistical Analysis
3. Results
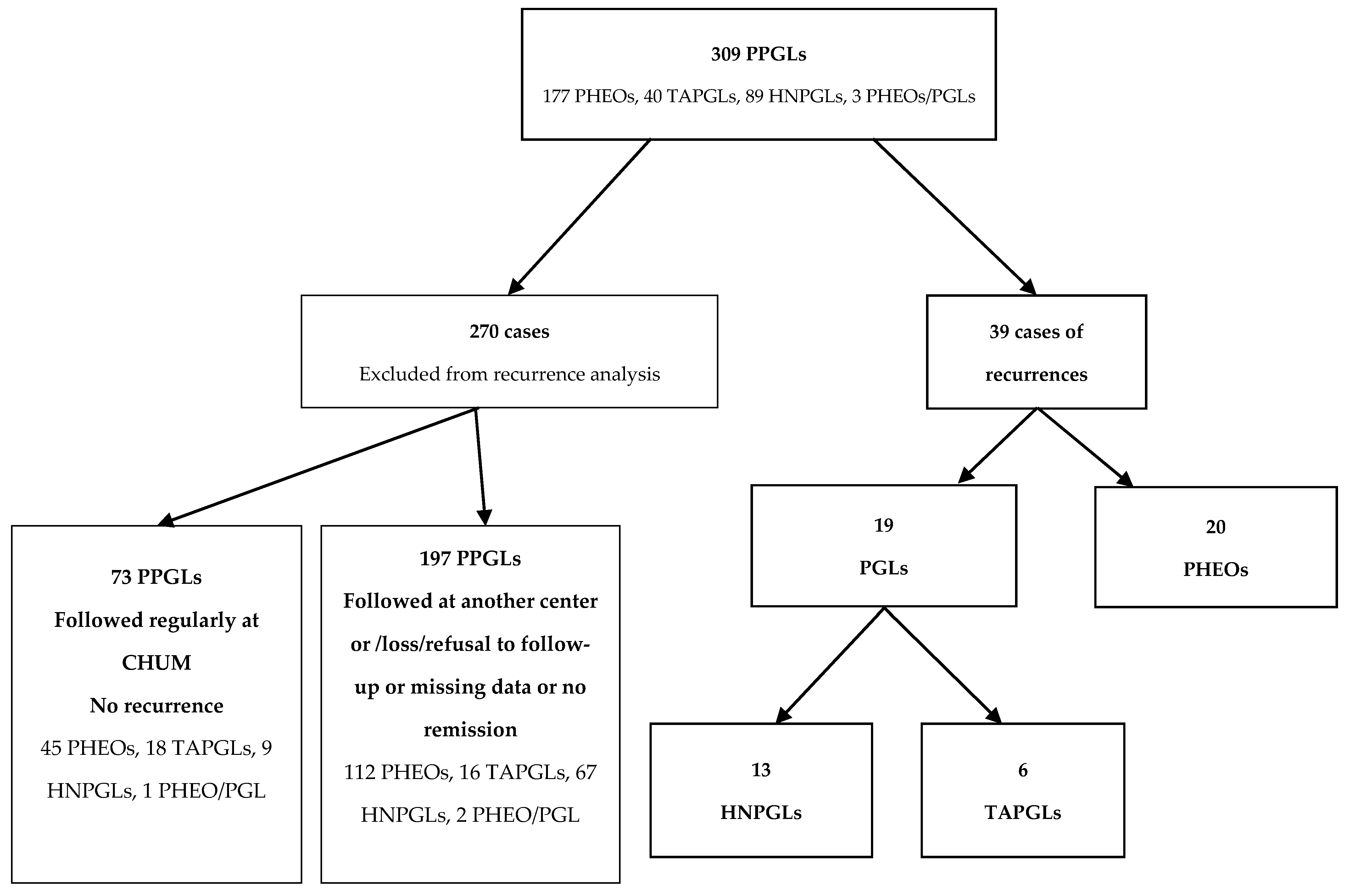
3.1. Patient Cohort
3.2. Characteristics of PHEOs with Recurrences
3.3. Characteristics of HNPGLs with Recurrences
3.4. Characteristics of TAPGLs with Recurrences
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Turchini, J.; Cheung, V.K.; Tischler, A.S.; De Krijger, R.R.; Gill, A.J. Pathology and genetics of phaeochromocytoma and paraganglioma. Histopathology 2018, 72, 97–105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lenders, J.W.; Duh, Q.Y.; Eisenhofer, G.; Gimenez-Roqueplo, A.P.; Grebe, S.K.; Murad, M.H.; Naruse, M.; Pacak, K.; Young, W.F., Jr. Pheochromocytoma and paraganglioma: An endocrine society clinical practice guideline. J. Clin. Endocrinol. Metab. 2014, 99, 1915–1942. [Google Scholar] [CrossRef] [PubMed]
- Plouin, P.F.; Fitzgerald, P.; Rich, T.; Ayala-Ramirez, M.; Perrier, N.D.; Baudin, E.; Jimenez, C. Metastatic pheochromocytoma and paraganglioma: Focus on therapeutics. Horm. Metab. Res. 2012, 44, 390–399. [Google Scholar] [CrossRef]
- Brouwers, F.M.; Eisenhofer, G.; Tao, J.J.; Kant, J.A.; Adams, K.T.; Linehan, W.M.; Pacak, K. High frequency of SDHB germline mutations in patients with malignant catecholamine-producing paragangliomas: Implications for genetic testing. J. Clin. Endocrinol. Metab. 2006, 91, 4505–4509. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turkova, H.; Prodanov, T.; Maly, M.; Martucci, V.; Adams, K.; Widimsky, J., Jr.; Chen, C.C.; Ling, A.; Kebebew, E.; Stratakis, C.A.; et al. Characteristics and outcomes of metastatic sdhb and sporadic pheochromocytoma/paraganglioma: An national institutes of health study. Endocr. Pract. 2016, 22, 302–314. [Google Scholar] [CrossRef] [PubMed]
- Nölting, S.; Bechmann, N.; Taieb, D.; Beuschlein, F.; Fassnacht, M.; Kroiss, M.; Eisenhofer, G.; Grossman, A.; Pacak, K. Personalized management of pheochromocytoma and paraganglioma. Endocr. Rev. 2022, 43, 199–239, Erratum in Endocr. Rev. 2022, 43, 440. [Google Scholar] [CrossRef]
- Williams, S.T.; Chatzikyriakou, P.; Carroll, P.V.; McGowan, B.M.; Velusamy, A.; White, G.; Obholzer, R.; Akker, S.; Tufton, N.; Casey, R.T.; et al. SDHC phaeochromocytoma and paraganglioma: A UK-wide case series. Clin. Endocrinol. 2022, 96, 499–512. [Google Scholar] [CrossRef]
- Jimenez, C. Treatment for patients with malignant pheochromocytomas and paragangliomas: A perspective from the hallmarks of cancer. Front. Endocrinol. 2018, 9, 277. [Google Scholar] [CrossRef]
- Schreiner, F.; Beuschlein, F. Disease monitoring of patients with pheochromocytoma or paraganglioma by biomarkers and imaging studies. Best Pract. Res. Clin. Endocrinol. Metab. 2020, 34, 101347. [Google Scholar] [CrossRef]
- Dhir, M.; Li, W.; Hogg, M.E.; Bartlett, D.L.; Carty, S.E.; McCoy, K.L.; Challinor, S.M.; Yip, L. Clinical predictors of malignancy in patients with pheochromocytoma and paraganglioma. Ann. Surg. Oncol. 2017, 24, 3624–3630. [Google Scholar] [CrossRef]
- Eisenhofer, G.; Lenders, J.W.; Siegert, G.; Bornstein, S.R.; Friberg, P.; Milosevic, D.; Mannelli, M.; Linehan, W.M.; Adams, K.; Timmers, H.J.; et al. Plasma methoxytyramine: A novel biomarker of metastatic pheochromocytoma and paraganglioma in relation to established risk factors of tumour size, location and SDHB mutation status. Eur. J. Cancer 2012, 48, 1739–1749. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schovanek, J.; Martucci, V.; Wesley, R.; Fojo, T.; Del Rivero, J.; Huynh, T.; Adams, K.; Kebebew, E.; Frysak, Z.; Stratakis, C.A.; et al. The size of the primary tumor and age at initial diagnosis are independent predictors of the metastatic behavior and survival of patients with SDHB-related pheochromocytoma and paraganglioma: A retrospective cohort study. BMC Cancer 2014, 14, 523. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amar, L.; Servais, A.; Gimenez-Roqueplo, A.P.; Zinzindohoue, F.; Chatellier, G.; Plouin, P.F. Year of diagnosis, features at presentation, and risk of recurrence in patients with pheochromocytoma or secreting paraganglioma. J. Clin. Endocrinol. Metab. 2005, 90, 2110–2116. [Google Scholar] [CrossRef] [PubMed]
- Venugopal, S.; Chhabria, M.; Quartuccio, M. Recurrence of pheochromocytoma with metastases after resection of primary tumor. Cureus 2020, 12, e8328. [Google Scholar] [CrossRef] [PubMed]
- Parasiliti-Caprino, M.; Lucatello, B.; Lopez, C.; Burrello, J.; Maletta, F.; Mistrangelo, M.; Migliore, E.; Tassone, F.; La Grotta, A.; Pia, A.; et al. Predictors of recurrence of pheochromocytoma and paraganglioma: A multicenter study in Piedmont, Italy. Hypertens Res. 2020, 43, 500–510. [Google Scholar] [CrossRef] [PubMed]
- Plouin, P.F.; Amar, L.; Dekkers, O.M.; Fassnacht, M.; Gimenez-Roqueplo, A.P.; Lenders, J.W.; Lussey-Lepoutre, C.; Steichen, O. European Society of Endocrinology Clinical Practice Guideline for long-term follow-up of patients operated on for a phaeochromocytoma or a paraganglioma. Eur. J. Endocrinol. 2016, 174, G1–G10. [Google Scholar] [CrossRef] [Green Version]
- Amar, L.; Lussey-Lepoutre, C.; Lenders, J.W.; Djadi-Prat, J.; Plouin, P.F.; Steichen, O. Management of endocrine disease: Recurrence or new tumors after complete resection of pheochromocytomas and paragangliomas: A systematic review and meta-analysis. Eur. J. Endocrinol. 2016, 175, R135–R145. [Google Scholar] [CrossRef] [Green Version]
- Holscher, I.; van den Berg, T.J.; Dreijerink, K.M.; Engelsman, A.F.; Nieveen van Dijkum, E.J. Recurrence rate of sporadic pheochromocytomas after curative adrenalectomy: A systematic review and meta-analysis. J. Clin. Endocrinol. Metab. 2020, 106, 588–597. [Google Scholar] [CrossRef]
- Castro-Vega, L.J.; Buffet, A.; De Cubas, A.A.; Cascón, A.; Menara, M.; Khalifa, E.; Amar, L.; Azriel, S.; Bourdeau, I.; Chabre, O.; et al. Germline mutations in FH confer predisposition to malignant pheochromocytomas and paragangliomas. Hum. Mol. Genet. 2014, 23, 2440–2446. [Google Scholar] [CrossRef] [Green Version]
- Alguire, C.; Chbat, J.; Forest, I.; Godbout, A.; Bourdeau, I. Unusual presentation of pheochromocytoma: Thirteen years of anxiety requiring psychiatric treatment. Endocrinol. Diabetes Metab. Case Rep. 2018, 2018, 17–0176. [Google Scholar] [CrossRef] [Green Version]
- Johnston, P.C.; Mullan, K.R.; Atkinson, A.B.; Eatock, F.C.; Wallace, H.; Gray, M.; Hunter, S.J. Recurrence of phaeochromocytoma and abdominal paraganglioma after initial surgical intervention. Ulster Med. J. 2015, 84, 102–106. [Google Scholar] [PubMed]
- van Heerden, J.A.; Roland, C.F.; Carney, J.A.; Sheps, S.G.; Grant, C.S. Long-term evaluation following resection of apparently benign pheochromocytoma(s)/paraganglioma(s). World J. Surg. 1990, 14, 325–329. [Google Scholar] [CrossRef] [PubMed]
- Timmers, H.J.; Brouwers, F.M.; Hermus, A.R.; Sweep, F.C.; Verhofstad, A.A.; Verbeek, A.L.; Pacak, K.; Lenders, J.W. Metastases but not cardiovascular mortality reduces life expectancy following surgical resection of apparently benign pheochromocytoma. Endocr. Relat. Cancer 2008, 15, 1127. [Google Scholar] [CrossRef] [PubMed]
- Shen, W.T.; Grogan, R.; Vriens, M.; Clark, O.H.; Duh, Q.Y. One hundred two patients with pheochromocytoma treated at a single institution since the introduction of laparoscopic adrenalectomy. Arch. Surg. 2010, 145, 893–897. [Google Scholar] [CrossRef] [Green Version]
- Press, D.; Akyuz, M.; Dural, C.; Aliyev, S.; Monteiro, R.; Mino, J.; Mitchell, J.; Hamrahian, A.; Siperstein, A.; Berber, E. Predictors of recurrence in pheochromocytoma. Surgery 2014, 156, 1523–1527. [Google Scholar] [CrossRef]
- Contrera, K.J.; Yong, V.; Reddy, C.A.; Liu, S.W.; Lorenz, R.R. Recurrence and progression of head and neck paragangliomas after treatment. Otolaryngol. Head Neck Surg. 2020, 162, 504–511. [Google Scholar] [CrossRef]
- Thai, E.; Gnetti, L.; Gilli, A.; Caruana, P.; Dalla Valle, R.; Buti, S. Very late recurrence of an apparently benign pheochromocytoma. J. Cancer Res. Ther. 2015, 11, 1036. [Google Scholar] [CrossRef]
- Assadipour, Y.; Sadowski, S.M.; Alimchandani, M.; Quezado, M.; Steinberg, S.M.; Nilubol, N.; Patel, D.; Prodanov, T.; Pacak, K.; Kebebew, E. SDHB mutation status and tumor size but not tumor grade are important predictors of clinical outcome in pheochromocytoma and abdominal paraganglioma. Surgery 2017, 161, 230–239. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Recurrent PPGLs Who Underwent Genetic Testing (n = 23) * | PPGLs With No Recurrences Who Underwent Genetic Testing (n = 66) | |||
|---|---|---|---|---|
| Genes with Germline Pathogenic Variant, n (%) | 12 (52.2) | 21 (31.8) | ||
| n (%) | Delay to Recurrence in Months Mean (Min–Max) | n (%) | Follow-Up Time in Months Mean (Min–Max) | |
| NF1, n (%) | 0 (0.0) | - | 5 (23.8) | 131 (66–233) |
| RET, n (%) | 3 (25.0) | 113 (14–240) | 4 (19.0) | 208.5 (172–234) |
| SDHB, n (%) | 3 (25.0) | 143 (26–288) | 4 (19.0) | 51 (30–61) |
| SDHC, n (%) | 2 (16.7) | 91.5 (39–144) | 3 (14.3) | 157 (101–232) |
| MAX, n (%) | 0 (0.0) | - | 2 (9.5) | 91.5 (31–152) |
| FH, n (%) | 1 (8.3) | 60 | 1 (4.8) | 42 |
| SDHA, n (%) | 2 (16.7) | 119 (58–180) | 1 (4.8) | 196 |
| VHL, n (%) | 0 (0.0) | - | 1 (4.8) | 146 |
| SDHD, n (%) | 1 (8.3) | 38 | 0 (0.0) | - |
| No pathogenic variant, n (%) | 10 (43.5) | 38 (57.6) | ||
| Variant of unknown significance, n (%) | 0 (0) | 7 (10.6) | ||
| PHEOs N = 20 | HNPGLs N = 13 | TAPGLs N = 6 | |
|---|---|---|---|
| Female n (%) | 14 (70.0) | 11 (84.6) | 2 (33.3) |
| Age at diagnosis (y) Mean (min–max) | 42.4 (16–67) | 46.2 (27–57) | 30.3 (15–45) |
| Age at recurrence (y) Mean (min–max) | 53.25 (19–78) | 53 (30–71) | 45.2 (27–60) |
| Delay to recurrence (months) mean;median (min–max) | 120.9; 77.5 (14–584) | 82.4; 67 (24–180) | 176.7; 188 (26–312) |
| Mean of maximal tumor diameter at initial diagnosis (cm) (min–max) * | 8.2 (3–24) | 2.7 (0.2–7.5) | 9.6 (3–14) |
| Local recurrence n (%) | 5 (25.0) | 11 (84.6) | 2 (33.3) |
| Metastatic recurrence n (%) | 15 (75.0) | 2 (15.4) | 4 (66.7) |
| Population | Recurrence Rate | Tumor Types | Predictors of Recurrence | Time of Recurrence | Local or Metastatic | |
|---|---|---|---|---|---|---|
| Van Heerden et al., 1990 [22] | 98 PPGLs | 6.5% | 6 PHEOs | - | 5–13 years | 33.3% local 66.6% metastatic |
| Amar et al., 2005 [13] | 192 PPGLs | 5 year: 6.5% 10 year: 16.1% | 22 PHEOs 7 PGLs | Age Tumor site Familial disease | - | 48.3% local 51.7% metastatic |
| Timmers et al., 2008 [23] | 69 PHEOs | 13.0% | 9 PHEOs | - | 1–14 years | 22.2% local 77.8% metastatic |
| Shen et al., 2010 [24] | 102 PPGLs | 6.9% | 7 PHEOs | - | 6 months–17 years | 100% local 0% metastatic |
| Press et al., 2014 [25] | 135 PHEOs | 6% | 8 PHEOs | tumor size > 5 cm | 7–106 months | 25% local 75% metastatic |
| Johnston et al., 2015 [21] | 52 PHEOs and TAPGLs | 5.8% | 2 PHEOs 1 TAPGL | - | 8–17.7 years | 100% local |
| Amar et al., 2016 [17] * Meta-Analysis | 38 studies 2396 curative surgeries for PHEOs or TAPGLs. Median of 94% PHEOs. | 1–34% (median 6%) | - | Syndromic presentation PGLs | Median 60 months | - |
| Contrera et al., 2020 [26] | 189 HNPGLs | 4 years: 8.2% 10 years: 17.1% | 42 HNPGLs | Tumor site | Median 18.4 years | 90.5% local 9.5% metastatic |
| Parasiliti-Caprino et al., 2020 [15] | 242 PPGLs | 17.4% | 35 PHEOs 7 PGLs | Genetic mutation Large tumors | Median 2.9 years | 59.5% local 40.5% metastatic |
| Holscher et al., 2020 [18] * Meta-analysis | 13 studies 430 PPGLs | 3% | - | - | Median 49.4 months | 25% local 75% metastatic |
| Parisien-La Salle et al., 2022 | 309 PPGLs | 12.6% | 20 PHEOs 13 HNPGLs 6 TAPGLs | - | 1–48 years | 46.2% local 53.8% metastatic |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Parisien-La Salle, S.; Chbat, J.; Lacroix, A.; Perrotte, P.; Karakiewicz, P.; Saliba, I.; Le, X.K.; Olney, H.J.; Bourdeau, I. Postoperative Recurrences in Patients Operated for Pheochromocytomas and Paragangliomas: New Data Supporting Lifelong Surveillance. Cancers 2022, 14, 2942. https://doi.org/10.3390/cancers14122942
Parisien-La Salle S, Chbat J, Lacroix A, Perrotte P, Karakiewicz P, Saliba I, Le XK, Olney HJ, Bourdeau I. Postoperative Recurrences in Patients Operated for Pheochromocytomas and Paragangliomas: New Data Supporting Lifelong Surveillance. Cancers. 2022; 14(12):2942. https://doi.org/10.3390/cancers14122942
Chicago/Turabian StyleParisien-La Salle, Stefanie, Jessica Chbat, André Lacroix, Paul Perrotte, Pierre Karakiewicz, Issam Saliba, Xuan Kim Le, Harold J. Olney, and Isabelle Bourdeau. 2022. "Postoperative Recurrences in Patients Operated for Pheochromocytomas and Paragangliomas: New Data Supporting Lifelong Surveillance" Cancers 14, no. 12: 2942. https://doi.org/10.3390/cancers14122942