
Detecting Early-Stage Oral Cancer from Clinically Diagnosed Oral Potentially Malignant Disorders by DNA Methylation Profile


 ,
, 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Sample Collection
2.2. Purification of DNA
2.3. Methylation Analysis
2.4. Statistical Analysis
2.5. Cytology
3. Results
3.1. Clinicopathological Characteristics of Patients with OPMDs
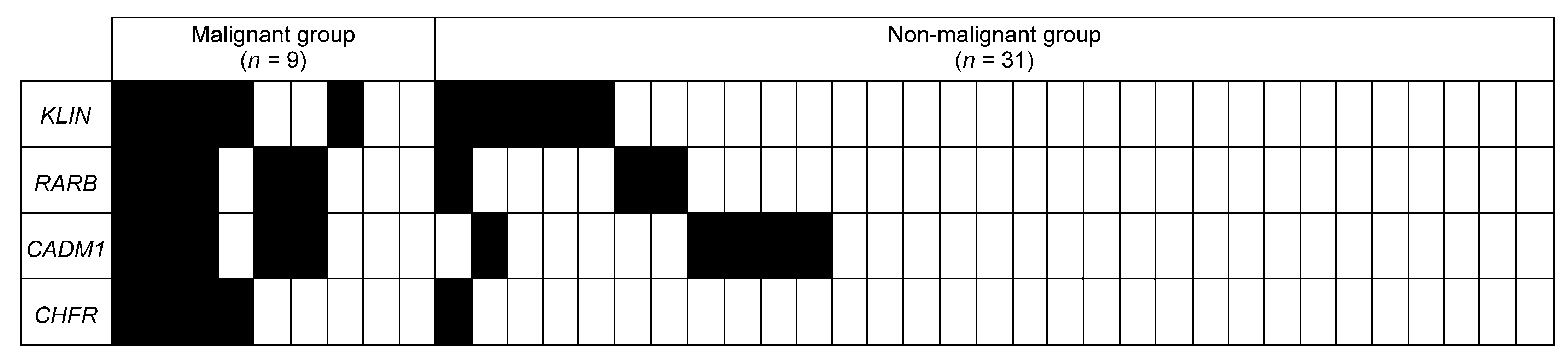
3.2. Diagnostic Performance of Each Gene on the Training Set
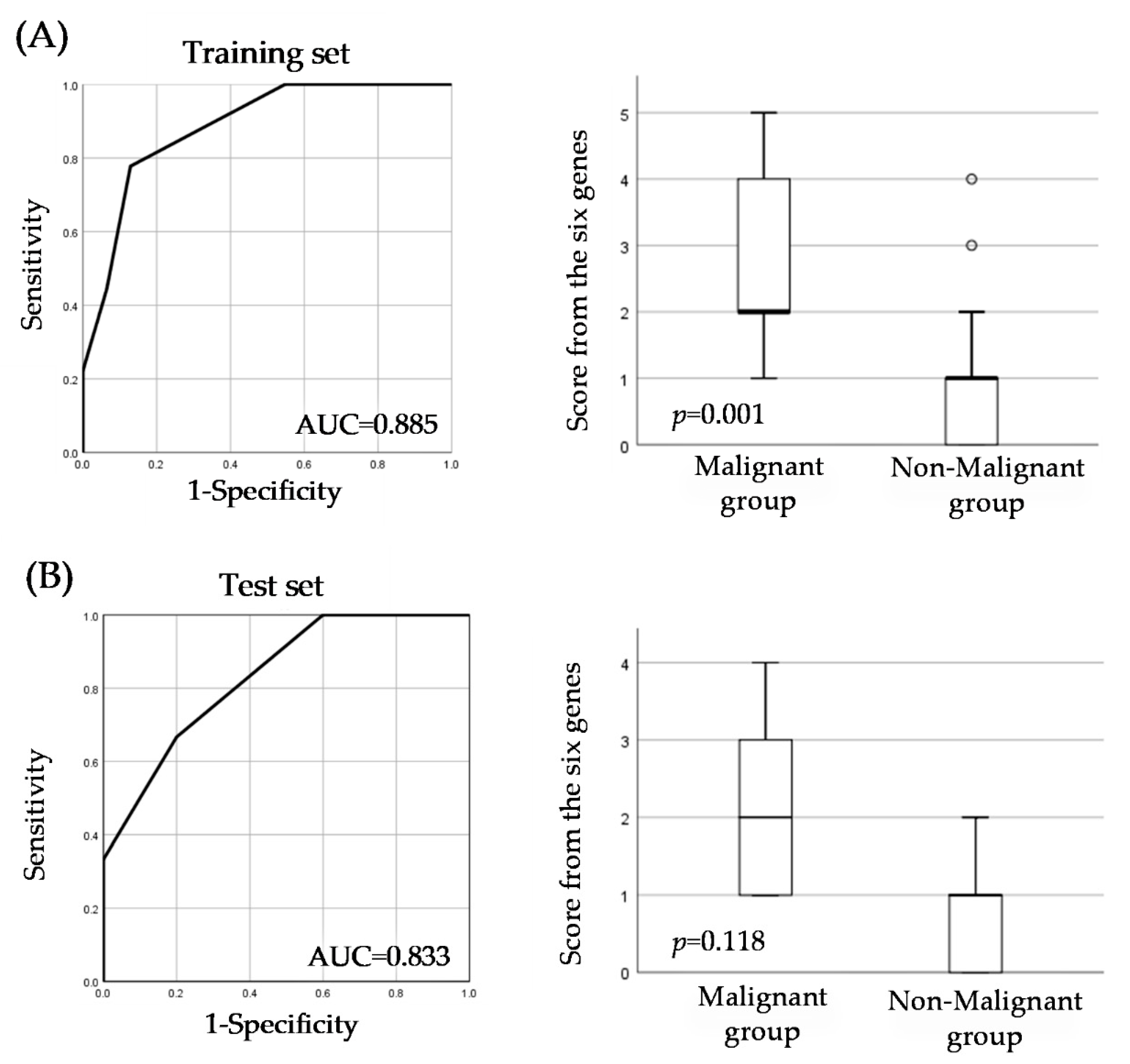
3.3. Evaluation of a Unique Predictive Score for Early-Stage Cancer Identification
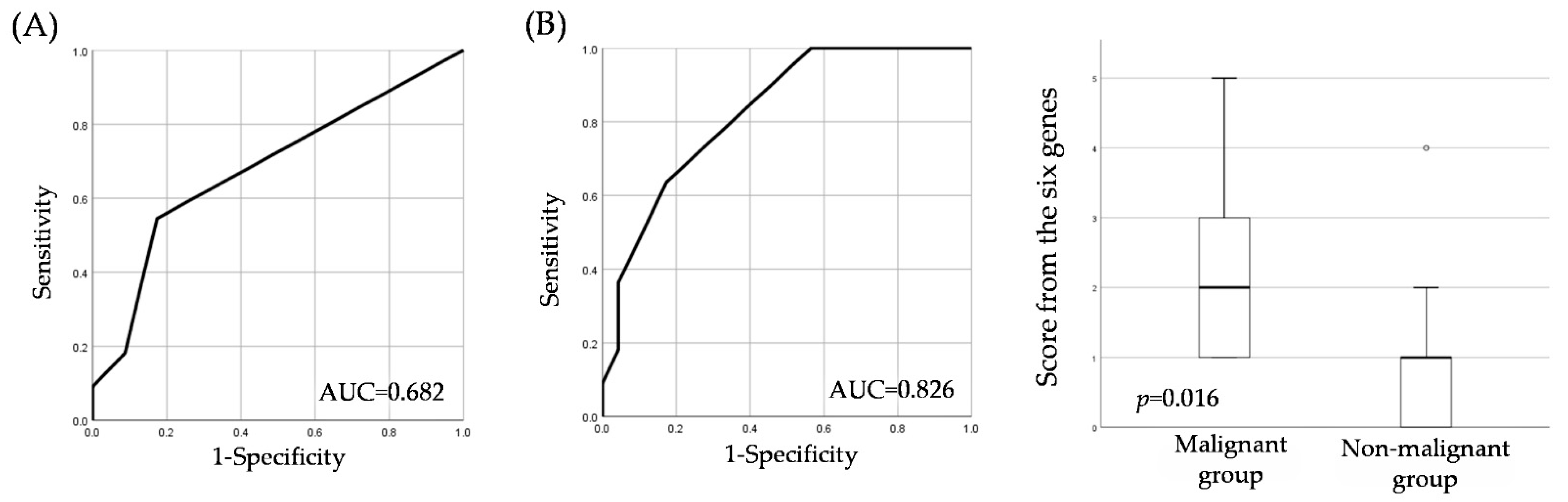
3.4. Comparing Cytology and the Score from the Six Genes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Fuchs, F.E.; Jemal, A. Cancer statistics. CA Cancer J. Clin. 2022, 72, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Zanoni, D.K.; Montero, P.H.; Migliacci, J.C.; Shah, J.P.; Wong, R.J.; Ganly, I.; Patel, S.G. Survival outcomes after treatment of cancer of the oral cavity (1985–2015). Oral Oncol. 2019, 90, 115–121. [Google Scholar] [CrossRef] [PubMed]
- Warnakulasuriya, S.; Kujan, O.; Aguirre-Urizar, J.M.; Bagan, J.V.; González-Moles, M.; Kerr, A.R.; Lodi, G.; Mello, F.W.; Monteiro, L.; Ogden, G.R.; et al. Oral potentially malignant disorders: A consensus report from an international seminar on nomenclature and classification, convened by the WHO Collaborating Centre for Oral Cancer. Oral Dis. 2021, 27, 1862–1880. [Google Scholar] [CrossRef] [PubMed]
- Warnakulasuriya, S. Clinical features and presentation of oral potentially malignant disorders. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2018, 125, 582–590. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Speight, P.M.; Khurram, S.A.; Kujan, O. Oral potentially malignant disorders: Risk of progression to malignancy. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2018, 125, 612–627. [Google Scholar] [CrossRef] [Green Version]
- Navone, R.; Burlo, P.; Pich, A.; Pentenero, M.; Broccoletti, R.; Marsico, A.; Gandolfo, S. The impact of liquid-based oral cytology on the diagnosis of oral squamous dysplasia and carcinoma. Cytopathology 2007, 18, 356–360. [Google Scholar] [CrossRef]
- Sekine, J.; Nakatani, E.; Hideshima, K.; Iwahashi, T.; Sasaki, H. Diagnostic accuracy of oral cancer cytology in a pilot study. Diagn. Pathol. 2017, 12, 27. [Google Scholar] [CrossRef] [Green Version]
- Kulis, M.; Esteller, M. DNA methylation and cancer. Adv. Genet. 2010, 70, 27–56. [Google Scholar]
- Baylin, S.B.; Jones, P.A. Epigenetic Determinants of Cancer. Cold Spring Harb. Perspect. Biol. 2016, 8, a019505. [Google Scholar] [CrossRef] [Green Version]
- Morgan, A.E.; Davies, T.J.; Mc Auley, M.T. The role of DNA methylation in ageing and cancer. Proc. Nutr. Soc. 2018, 77, 412–422. [Google Scholar] [CrossRef]
- Pan, Y.; Liu, G.; Zhou, F.; Su, B.; Fuling, Z. DNA methylation profiles in cancer diagnosis and therapeutics. Clin. Exp. Med. 2018, 18, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Delpu, Y.; Cordelier, P.; Cho, W.C.; Torrisani, J. DNA methylation and cancer diagnosis. Int. J. Mol. Sci. 2013, 14, 15029–15058. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barton, C.A.; Hacker, N.F.; Clark, S.; O’Brien, P.M. DNA methylation changes in ovarian cancer: Implications for early diagnosis, prognosis and treatment. Gynecol. Oncol. 2008, 109, 129–139. [Google Scholar] [CrossRef] [PubMed]
- Bai, Y.; Tong, W.; Xie, F.; Zhu, L.; Wu, H.; Shi, R.; Wang, L.; Yang, L.; Liu, Z.; Miao, F.; et al. DNA methylation biomarkers for diagnosis of primary liver cancer and distinguishing hepatocellular carcinoma from intrahepatic cholangiocarcinoma. Aging 2021, 13, 17592–17606. [Google Scholar] [CrossRef]
- Natale, F.; Vivo, M.; Falco, G.; Angrisano, T. Deciphering DNA methylation signatures of pancreatic cancer and pancreatitis. Clin. Epigenetics 2019, 11, 132. [Google Scholar] [CrossRef] [Green Version]
- Casás-Selves, M.; Degregori, J. How cancer shapes evolution, and how evolution shapes cancer. Evol. Educ. Outreach 2011, 4, 624–634. [Google Scholar] [CrossRef] [Green Version]
- Yuspa, S.H.; Długosz, A.A.; Cheng, C.K.; Denning, M.F.; Tennenbaum, T.; Glick, A.B.; Weinberg, W.C. Role of oncogenes and tumor suppressor genes in multistage carcinogenesis. J. Invest. Dermatol. 1994, 103, 90s–95s. [Google Scholar] [CrossRef] [Green Version]
- Malki, A.; Abu ElRuz, R.; Gupta, I.; Allouch, A.; Vranic, S.; Al Moustafa, A.-E. Molecular Mechanisms of Colon Cancer Progression and Metastasis: Recent Insights and Advancements. Int. J. Mol. Sci. 2020, 22, 130. [Google Scholar] [CrossRef]
- Shaw, R. The epigenetics of oral cancer. Int. J. Oral Maxillofac. Surg. 2006, 35, 101–108. [Google Scholar] [CrossRef]
- Emfietzoglou, R.; Pachymanolis, E.; Piperi, C. Impact of Epigenetic Alterations in the Development of Oral Diseases. Curr. Med. Chem. 2021, 28, 1091–1103. [Google Scholar] [CrossRef]
- Bonar-Alvarez, P.; Perez-Sayans, M.; Padín-Iruegas, E.; Suarez-Penaranda, J.M.; Oliveira-Alves, M.; Blanco Carrion, A.; García-Garcia, A. State of methylation and epigenome studies in some types of head and neck cancer. Biomed. Res. 2018, 29, 2944–2955. [Google Scholar]
- López, M.; Aguirre, J.M.; Cuevas, N.; Anzola, M.; Videgain, J.; Aguirregaviria, J.; Pancorbo, M.M. Gene promoter hypermethylation in oral rinses of leukoplakia patients--A diagnostic and/or prognostic tool? Eur. J. Cancer 2003, 39, 2306–2309. [Google Scholar] [CrossRef]
- Arantes, L.M.; de Carvalho, A.C.; Melendez, M.E.; Centrone, C.; Góis-Filho, J.; Toporcov, T.; Caly, D.; Tajara, E.; Goloni-Bertollo, E. Validation of methylation markers for diagnosis of oral cavity cancer. Eur. J. Cancer 2015, 51, 632–641. [Google Scholar] [CrossRef] [PubMed]
- Ferlazzo, N.; Currò, M.; Zinellu, A.; Caccamo, D.; Isola, G.; Ventura, V.; Carru, C.; Matarese, G.; Ientile, R. Influence of MTHFR Genetic Background on p16 and MGMT Methylation in Oral Squamous Cell Cancer. Int. J. Mol. Sci. 2017, 18, 724. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jayaprakash, C.; Radhakrishnan, R.; Ray, S.; Satyamoorthy, K. Promoter methylation of MGMT in oral carcinoma: A population-based study and meta-analysis. Arch. Oral Biol. 2017, 80, 197–208. [Google Scholar] [CrossRef] [PubMed]
- Gissi, D.B.; Tarsitano, A.; Gabusi, A.; Rossi, R.; Attardo, G.; Lenzi, J.; Marchetti, C.; Montebugnoli, L.; Foschini, M.P.; Morandi, L. 13-gene DNA Methylation Analysis from Oral Brushing: A Promising Non Invasive Tool in the Follow-up of Oral Cancer Patients. J. Clin. Med. 2019, 8, 2107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagata, S.; Hamada, T.; Yamada, N.; Yokoyama, S.; Kitamoto, S.; Kanmura, Y.; Nomura, M.; Kamikawa, Y.; Yonezawa, S.; Sugihara, K. Aberrant DNA methylation of tumor-related genes in oral rinse: A noninvasive method for detection of oral squamous cell carcinoma. Cancer 2012, 118, 4298–4308. [Google Scholar] [CrossRef]
- Nygren, A.O.; Ameziane, N.; Duarte, H.M.B.; Vijzelaar, R.N.C.P.; Waisfisz, Q.; Hess, C.J.; Schouten, J.P.; Errami, A. Methylation-specific MLPA (MS-MLPA): Simultaneous detection of CpG methylation and copy number changes of up to 40 sequences. Nucleic Acids Res. 2005, 33, e128. [Google Scholar] [CrossRef] [Green Version]
- Schouten, J.P.; McElgunn, C.J.; Waaijer, R.; Zwijnenburg, D.; Diepvens, F.; Pals, G. Relative quantification of 40 nucleic acid sequences by multiplex ligation-dependent probe amplification. Nucleic Acids Res. 2002, 30, e57. [Google Scholar] [CrossRef] [Green Version]
- Gurioli, G.; Salvi, S.; Martignano, F.; Foca, F.; Gunelli, R.; Costantini, M.; Cicchetti, G.; De Giorgi, U.; Sbarba, P.D.; Calistri, D.; et al. Methylation pattern analysis in prostate cancer tissue: Identification of biomarkers using an MS-MLPA approach. J. Transl. Med. 2016, 14, 249. [Google Scholar] [CrossRef] [Green Version]
- Dvorakova, E.; Chmelarova, M.; Laco, J.; Palicka, V.; Spacek, J. Methylation analysis of tumor suppressor genes in endometroid carcinoma of endometrium using MS-MLPA. Biomed. Pap. Med Fac. Univ. Palacky Olomouc Czech Repub. 2013, 157, 298–303. [Google Scholar] [CrossRef] [PubMed]
- Noorlag, R.; van Kempen, P.M.; Moelans, C.B.; de Jong, R.; Blok, L.E.; Koole, R.; van Es, R.J.J.; Willems, S.M. Promoter hypermethylation using 24-gene array in early head and neck cancer: Better outcome in oral than in oropharyngeal cancer. Epigenetics 2014, 9, 1220–1227. [Google Scholar] [CrossRef] [PubMed]
- Baba, S.; Baba, S.; Kato, K.; Long, N.K.; Hatano, Y.; Kimura, M.; Okano, Y.; Yamada, Y.; Shibata, T. Aberrant promoter hypermethylation of the CHFR gene in oral squamous cell carcinomas. Oncol. Rep. 2009, 22, 1173–1179. [Google Scholar] [PubMed] [Green Version]
- Ribeiro, I.P.; Caramelo, F.; Esteves, L.; Oliveira, A.; Marques, F.; Barroso, L.; Melo, J.B.; Carreira, I.M. Genomic and epigenetic signatures associated with survival rate in oral squamous cell carcinoma patients. J. Cancer 2018, 9, 1885–1895. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khor, G.H.; Froemming, G.R.A.; Zain, R.B.; Abraham, M.T.; Thong, K.L. Screening of differential promoter hypermethylated genes in primary oral squamous cell carcinoma. Asian Pac. J. Cancer Prev. 2014, 15, 8957–8961. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leichsenring, A.; Losi-Guembarovski, R.; Maciel, M.E.; Losi-Guembarovski, A.; Oliveira, B.W.; Ramos, G.; Cavalcanti, T.C.S.; Bicalho, M.G.; Cavalli, I.J.; Cólus, I.M.S.; et al. CYP1A1 and GSTP1 polymorphisms in an oral cancer case-control study. Braz. J. Med. Biol. Res. 2006, 39, 1569–1574. [Google Scholar] [CrossRef] [PubMed]
- Buenahora, M.R.; Lafaurie, G.I.; Perdomo, S.J. Identification of HPV16-p16(INK4a) mediated methylation in oral potentially malignant disorder. Epigenetics 2021, 16, 1016–1030. [Google Scholar] [CrossRef]
- Ringström, E.; Peters, E.; Hasegawa, M.; Posner, M.; Liu, M.; Kelsey, K.T. Human papillomavirus type 16 and squamous cell carcinoma of the head and neck. Clin. Cancer Res. 2002, 8, 3187–3192. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Training Set | Test Set | |||||
|---|---|---|---|---|---|---|
| Non-Malignant Group | Malignant Group | Non-Malignant Group | Malignant Group | |||
| n = 31 | n = 9 | n = 10 | n = 6 | |||
| R | 71 (30–86) | 74 (37–81) | 68.5 (45–83) | 63 (24–87) | ||
| Sex, n (%) | ||||||
| Male | 16 (51.6) | 5 (55.5) | p = 1.000 | 4 (40.0) | 3 (50.0) | p = 1.000 |
| Female | 15 (48.3) | 4 (44.4) | 6 (60.0) | 3 (50.0) | ||
| Smoking, n (%) | ||||||
| Yes | 11 (36.6) | 4 (44.4) | p = 0.441 | 2 (20.0) | 3 (50.0) | p = 0.299 |
| No | 20 (64.5) | 5 (55.5) | 8 (80.0) | 3 (50.0) | ||
| Drinking, n (%) | ||||||
| Yes | 10 (32.2) | 4 (44.4) | p = 0.255 | 3 (30.0) | 2 (33.3) | p = 1.000 |
| No | 21 (67.7) | 5 (55.5) | 7 (70.0) | 4 (66.7) | ||
| Clinic diagnosis, n (%) | ||||||
| Intractable stomatitis | 2 (6.4) | 2 (22.2) | 1 (10.0) | 1 (16.7) | ||
| Lichen planus | 13 (41.9) | 2 (22.2) | 4 (40.0) | 1 (16.7) | ||
| Leucoplakia | 16 (51.6) | 5 (55.5) | 5 (50.5) | 4 (66.7) | ||
| Pathological diagnosis, n (%) | ||||||
| Chronic stomatitis | 12 (38.7) | 2 (20.0) | ||||
| Lichen planus | 2 (6.4) | 2 (20.0) | ||||
| Epithelial hyperplasia | 6 (19.3) | |||||
| Epithelial dysplasia | 11 (35.4) | 5 (50.0) | ||||
| Squamous cell papilloma | 1 (10.0) | |||||
| SCC intraepithelial | 4 (44.4) | 1 (16.7) | ||||
| SCC | 5 (55.5) | 5 (83.3) | ||||
| Gene Name | Sensitivity | Specificity | PPV | NPV | Fischer‘s Exact Test | AUC |
|---|---|---|---|---|---|---|
| % | % | % | % | p-Value | ||
| RARB | 55.6 | 90.3 | 62.5 | 87.5 | 0.008 | 0.731 |
| KLLN | 55.6 | 83.9 | 50.0 | 86.7 | 0.029 | 0.708 |
| CHFR | 44.4 | 96.8 | 80.0 | 85.7 | 0.006 | 0.708 |
| CADM1 | 55.6 | 83.9 | 50.0 | 86.7 | 0.029 | 0.703 |
| TP73 | 55.6 | 83.9 | 50.0 | 86.7 | 0.029 | 0.690 |
| GSTP1 | 22.2 | 96.8 | 66.7 | 81.1 | 0.121 | 0.685 |
| BRCA1 | 33.3 | 96.8 | 75.0 | 83.3 | 0.030 | 0.676 |
| ESR1 | 77.8 | 61.3 | 36.8 | 90.5 | 0.060 | 0.672 |
| ATM | 44.4 | 83.9 | 44.4 | 83.9 | 0.168 | 0.658 |
| TIMP3 | 44.4 | 80.6 | 40.0 | 83.3 | 0.190 | 0.652 |
| BRCA2 | 44.4 | 83.9 | 44.4 | 83.9 | 0.168 | 0.629 |
| CASP8 | 44.4 | 71.0 | 30.8 | 81.5 | 0.437 | 0.627 |
| MLH | 55.6 | 64.5 | 31.3 | 83.3 | 0.441 | 0.609 |
| APC | 33.3 | 87.1 | 42.9 | 81.8 | 0.316 | 0.606 |
| Sample Set | Cutoff * | Malignant Group | Non-Malignant Group | Sensitivity | Specificity | PPV | NPV | Fischer’s Exact Test | AUC |
|---|---|---|---|---|---|---|---|---|---|
| % | % | % | % | p-Value | |||||
| Training set (n= 40) | ≥2 genes | 7 | 4 | 77.8 | 87.1 | 63.6 | 93.1 | 0.001 | 0.885 |
| <2 genes | 2 | 27 | |||||||
| Test set (n = 16) | ≥2 genes | 4 | 2 | 66.7 | 80.0 | 66.7 | 80.0 | 0.118 | 0.833 |
| <2 genes | 2 | 8 |
| Biopsy | |||||
|---|---|---|---|---|---|
| SCC | Dysplasia | Others | |||
| Cytology | |||||
| SCC | 1 | p = 0.580 | |||
| HSIL | 1 | 2 | |||
| LSIL | 4 | 2 | |||
| NILM | 5 | 8 | 11 | ||
| Score from the six genes | |||||
| ≥2 genes | 7 | 2 | 2 | p = 0.016 | |
| <2 genes | 4 | 8 | 11 | ||
| Diagnostic Method | Cutoff | Malignant Group | Non-Malignant Group | Sensitivity | Specificity | PPV | NPV | Fischer’s Exact Test | AUC |
|---|---|---|---|---|---|---|---|---|---|
| % | % | % | % | p-Value | |||||
| Cytology | SCC and HSIL | 2 | 2 | 18.2 | 91.3 | 50.0 | 70.0 | 0.580 | 0.682 |
| LSIL and NILM | 9 | 21 | |||||||
| Score from the six genes | ≥2 genes | 7 | 4 | 63.6 | 82.6 | 63.6 | 82.6 | 0.016 | 0.826 |
| <2 genes | 4 | 19 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mori, K.; Hamada, T.; Beppu, M.; Tsuchihashi, H.; Goto, Y.; Kume, K.; Hijioka, H.; Nishi, K.; Mishima, Y.; Sugiura, T. Detecting Early-Stage Oral Cancer from Clinically Diagnosed Oral Potentially Malignant Disorders by DNA Methylation Profile. Cancers 2022, 14, 2646. https://doi.org/10.3390/cancers14112646
Mori K, Hamada T, Beppu M, Tsuchihashi H, Goto Y, Kume K, Hijioka H, Nishi K, Mishima Y, Sugiura T. Detecting Early-Stage Oral Cancer from Clinically Diagnosed Oral Potentially Malignant Disorders by DNA Methylation Profile. Cancers. 2022; 14(11):2646. https://doi.org/10.3390/cancers14112646
Chicago/Turabian StyleMori, Kazuki, Tomofumi Hamada, Mahiro Beppu, Hiroki Tsuchihashi, Yuichi Goto, Kenichi Kume, Hiroshi Hijioka, Keitaro Nishi, Yumiko Mishima, and Tsuyoshi Sugiura. 2022. "Detecting Early-Stage Oral Cancer from Clinically Diagnosed Oral Potentially Malignant Disorders by DNA Methylation Profile" Cancers 14, no. 11: 2646. https://doi.org/10.3390/cancers14112646