
Impact of Extended Use of Ablation Techniques in Cirrhotic Patients with Hepatocellular Carcinoma: A Cost-Effectiveness Analysis

 , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Results
2.1. Study Population
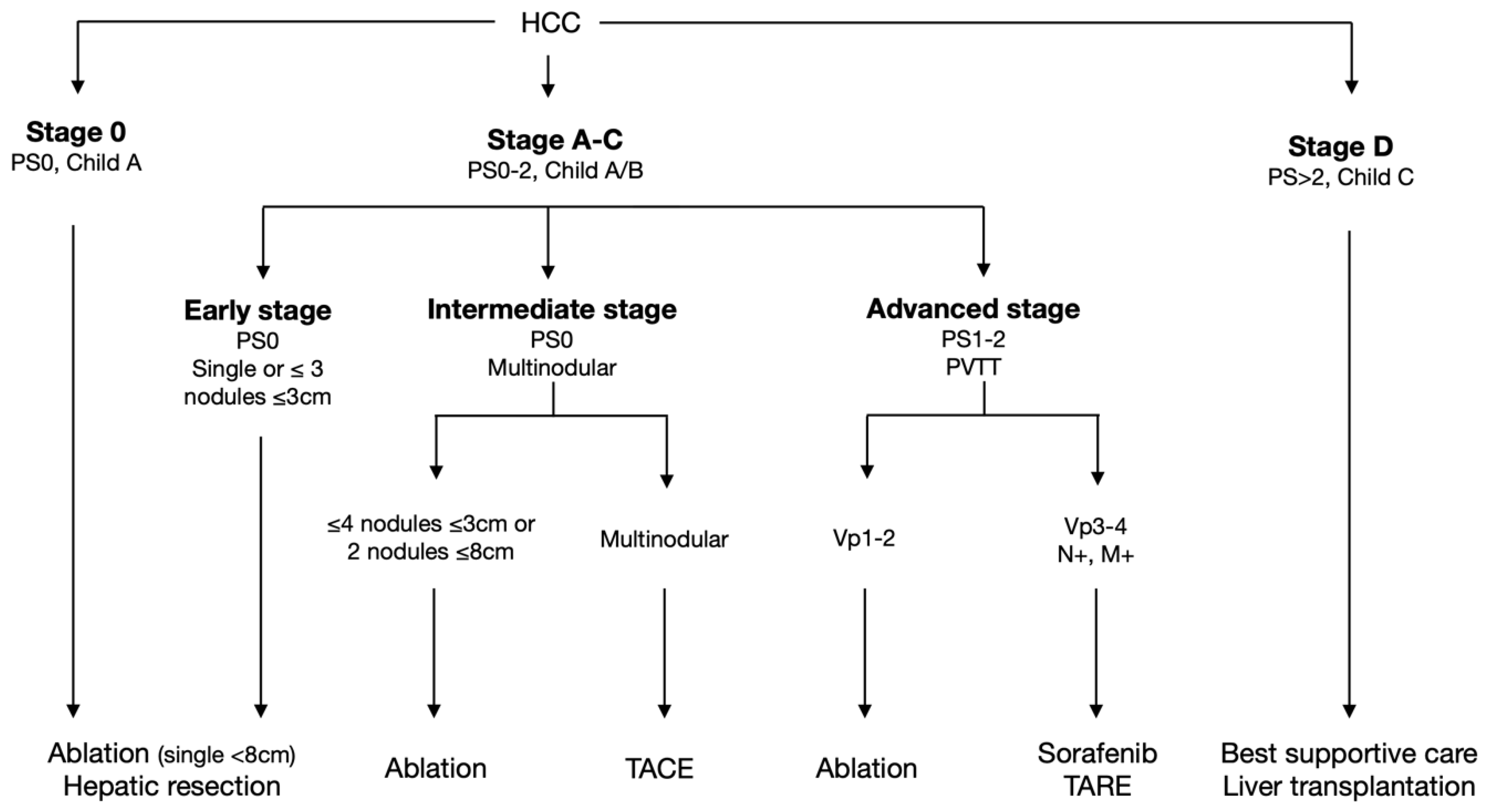
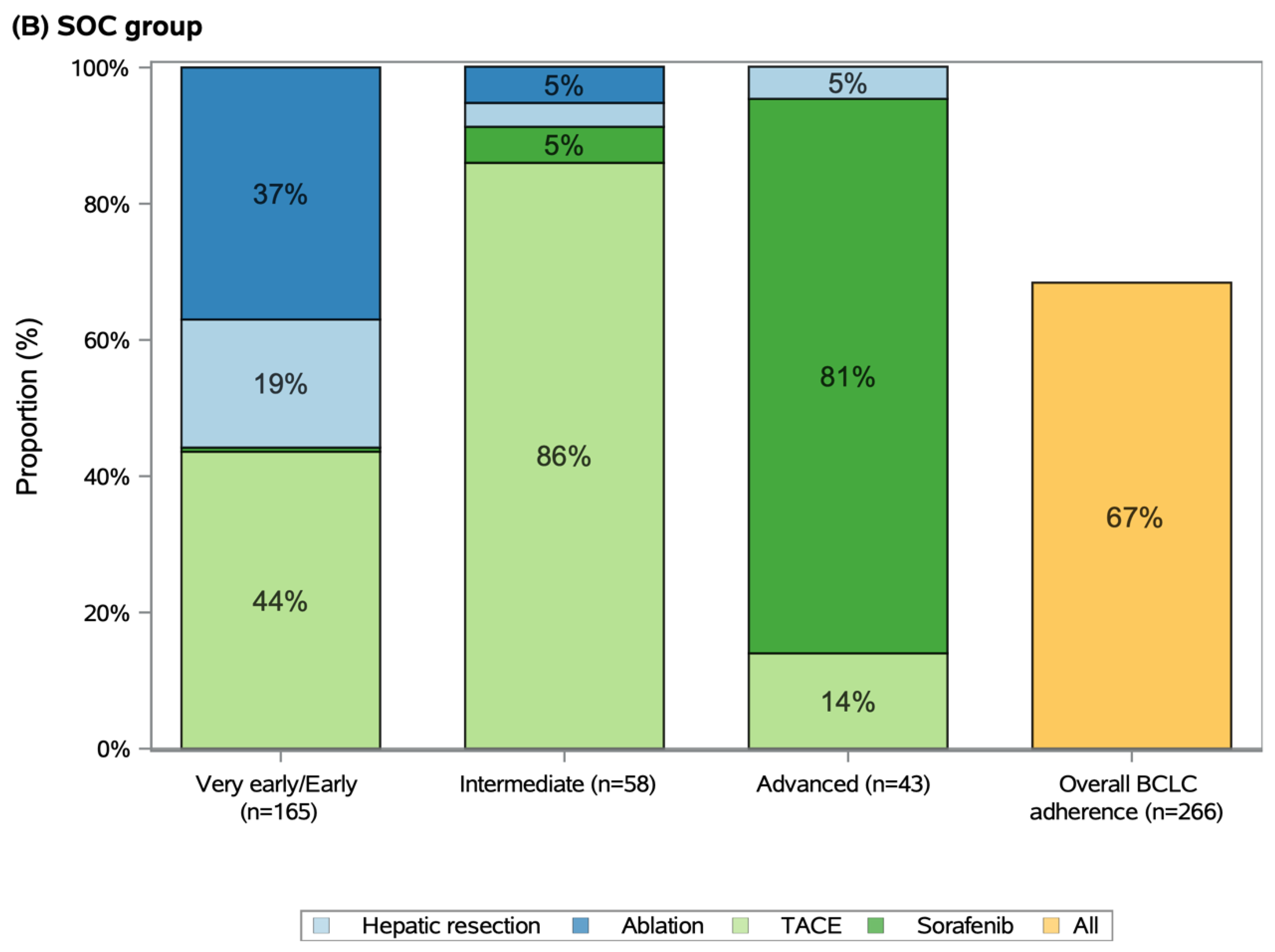
2.2. Allocation of First-Line Treatments
2.3. Therapeutic Trajectories after First-Line Treatments
2.4. Overall Survival Analysis
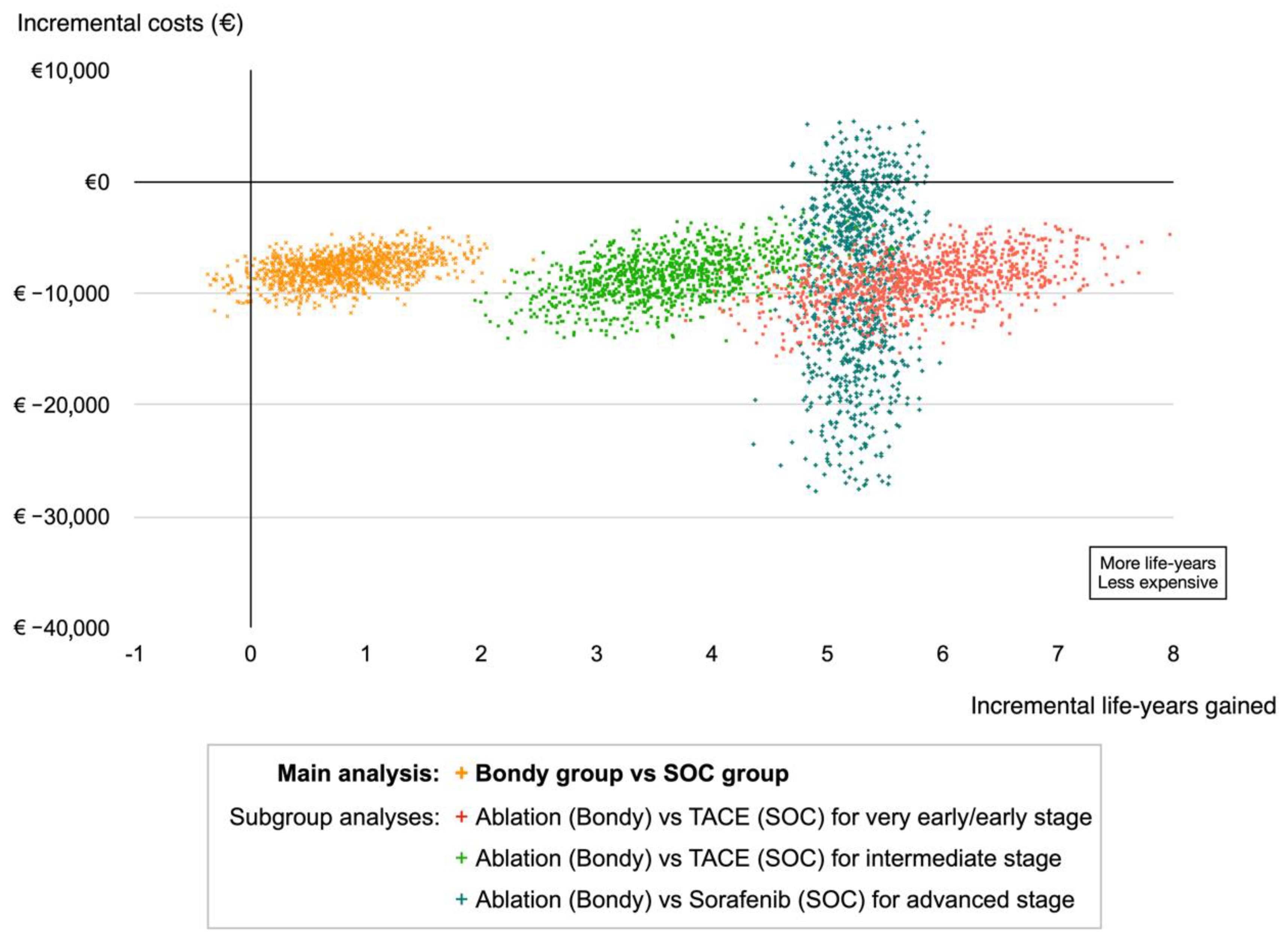
2.5. Cost Effectiveness Analysis
3. Discussion
4. Materials and Methods
4.1. Patient Selection
4.2. Outcome
4.3. Model Structure
4.4. Health Costs
4.5. Cost-Effectiveness Analysis
4.6. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Llovet, J.M.; Brú, C.; Bruix, J. Prognosis of Hepatocellular Carcinoma: The BCLC staging classification. Semin. Liver Dis. 1999, 19, 329–338. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, M.; Roayaie, S.; Konstadoulakis, M. Strategies for the management of hepatocellular carcinoma. Nat. Clin. Pr. Oncol. 2007, 4, 424–432. [Google Scholar] [CrossRef] [PubMed]
- Mazzaferro, V.; Regalia, E.; Doci, R.; Andreola, S.; Pulvirenti, A.; Bozzetti, F.; Montalto, F.; Ammatuna, M.; Morabito, A.; Gennari, L. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. N. Engl. J. Med. 1996, 334, 693–699. [Google Scholar] [CrossRef] [PubMed]
- Yao, F.Y.; Bass, N.M.; Nikolai, B.; Merriman, R.; Davern, T.J.; Kerlan, R.; Ascher, N.L.; Roberts, J.P. A follow-up analysis of the pattern and predictors of dropout from the waiting list for liver transplantation in patients with hepatocellular carcinoma: Implications for the current organ allocation policy. Liver Transpl. 2003, 9, 684–692. [Google Scholar] [CrossRef] [PubMed]
- Cherqui, D.; Laurent, A.; Mocellin, N.; Tayar, C.; Luciani, A.; Van Nhieu, J.T.; Decaens, T.; Hurtova, M.; Memeo, R.; Mallat, A.; et al. Liver resection for transplantable hepatocellular carcinoma: Long-term survival and role of secondary liver transplantation. Ann. Surg. 2009, 250, 738–746. [Google Scholar] [CrossRef]
- Varela, M.; Sala, M.; Llovet, J.M.; Bruix, J. Treatment of hepatocellular carcinoma: Is there an optimal strategy? Cancer Treat. Rev. 2003, 29, 99–104. [Google Scholar] [CrossRef]
- Nahon, P.; Layese, R.; Bourcier, V.; Cagnot, C.; Marcellin, P.; Guyader, D.; Pol, S.; Larrey, D.; De Lédinghen, V.; Ouzan, D.; et al. Incidence of hepatocellular carcinoma after direct antiviral therapy for HCV in patients with cirrhosis included in surveillance programs. Gastroenterology 2018, 155, 1436–1450.e6. [Google Scholar] [CrossRef] [Green Version]
- Ganne-Carrié, N.; Chaffaut, C.; Bourcier, V.; Archambeaud, I.; Perarnau, J.-M.; Oberti, F.; Roulot, D.; Moreno, C.; Louvet, A.; Dao, T.; et al. Estimate of hepatocellular carcinoma incidence in patients with alcoholic cirrhosis. J. Hepatol. 2018, 69, 1274–1283. [Google Scholar] [CrossRef]
- Forner, A.; Reig, M.E.; de Lope, C.R.; Bruix, J. Current strategy for staging and treatment: The BCLC update and future prospects. Semin. Liver Dis. 2010, 30, 61–74. [Google Scholar] [CrossRef]
- Leoni, S.; Piscaglia, F.; Serio, I.; Terzi, E.; Pettinari, I.; Croci, L.; Marinelli, S.; Benevento, F.; Golfieri, R.; Bolondi, L. Adherence to AASLD guidelines for the treatment of hepatocellular carcinoma in clinical practice: Experience of the Bologna liver oncology group. Dig. Liver Dis. 2014, 46, 549–555. [Google Scholar] [CrossRef]
- Kikuchi, L.; Chagas, A.L.; Alencar, R.S.S.M.; Tani, C.; Diniz, M.A.; D’Albuquerque, L.A.C.; Carrilho, F.J. Adherence to BCLC recommendations for the treatment of hepatocellular carcinoma: Impact on survival according to stage. Clinics 2017, 72, 454–460. [Google Scholar] [CrossRef]
- Reig, M.; Forner, A.; Rimola, J.; Ferrer-Fàbrega, J.; Burrel, M.; Garcia-Criado, Á.; Kelley, R.K.; Galle, P.R.; Mazzaferro, V.; Salem, R.; et al. BCLC strategy for prognosis prediction and treatment recommendation: The 2022 update. J. Hepatol. 2022, 76, 681–693. [Google Scholar] [CrossRef]
- Sutter, O.; Calvo, J.; N’Kontchou, G.; Nault, J.-C.; Ourabia, R.; Nahon, P.; Ganne-Carrié, N.; Bourcier, V.; Zentar, N.; Bouhafs, F.; et al. Safety and efficacy of irreversible electroporation for the treatment of hepatocellular carcinoma not amenable to thermal ablation techniques: A retrospective single-center case series. Radiology 2017, 284, 877–886. [Google Scholar] [CrossRef]
- N’Kontchou, G.; Nault, J.-C.; Sutter, O.; Bourcier, V.; Coderc, E.; Grando, V.; Nahon, P.; Ganne-Carrié, N.; Diallo, A.; Sellier, N.; et al. Multibipolar radiofrequency ablation for the treatment of mass-forming and infiltrative hepatocellular carcinomas > 5 Cm: Long-term results. Liver Cancer 2019, 8, 172–185. [Google Scholar] [CrossRef]
- Seror, O.; N’Kontchou, G.; Haddar, D.; Dordea, M.; Ajavon, Y.; Ganne, N.; Trinchet, J.C.; Beaugrand, M.; Sellier, N. Large infiltrative hepatocellular carcinomas: Treatment with percutaneous intraarterial ethanol injection alone or in combination with conventional percutaneous ethanol injection. Radiology 2005, 234, 299–309. [Google Scholar] [CrossRef]
- Blaise, L.; Pereira, H.; Vilgrain, V.; Sutter, O.; Gigante, E.; Walter, A.; Ganne-Carrié, N.; Nahon, P.; Bouattour, M.; Dioguardi Burgio, M.; et al. Percutaneous ablation for locally advanced hepatocellular carcinoma with tumor portal invasion. Clin. Res. Hepatol. Gastroenterol. 2021, 45, 101731. [Google Scholar] [CrossRef]
- Song, K.D.; Lee, M.W.; Rhim, H.; Kang, T.W.; Cha, D.I.; Sinn, D.H.; Lim, H.K. Percutaneous US/MRI fusion-guided radiofrequency ablation for recurrent subcentimeter hepatocellular carcinoma: Technical feasibility and therapeutic outcomes. Radiology 2018, 288, 878–886. [Google Scholar] [CrossRef]
- Kondo, Y.; Yoshida, H.; Shiina, S.; Tateishi, R.; Teratani, T.; Omata, M. Artificial ascites technique for percutaneous radiofrequency ablation of liver cancer adjacent to the gastrointestinal tract. Br. J. Surg. 2006, 93, 1277–1282. [Google Scholar] [CrossRef]
- Nault, J.-C.; Sutter, O.; Nahon, P.; Ganne-Carrié, N.; Séror, O. Percutaneous treatment of hepatocellular carcinoma: State of the art and innovations. J. Hepatol. 2018, 68, 783–797. [Google Scholar] [CrossRef] [Green Version]
- Nahon, P.; Vibert, E.; Nault, J.-C.; Ganne-Carrié, N.; Ziol, M.; Seror, O. Optimizing curative management of hepatocellular carcinoma. Liver Int. 2020, 40, 109–115. [Google Scholar] [CrossRef] [Green Version]
- Cadier, B.; Bulsei, J.; Nahon, P.; Seror, O.; Laurent, A.; Rosa, I.; Layese, R.; Costentin, C.; Cagnot, C.; Durand-Zaleski, I.; et al. Early detection and curative treatment of hepatocellular carcinoma: A cost-effectiveness analysis in France and in the United States. Hepatology 2017, 65, 1237–1248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, J.-W.; Chen, M.; Colombo, M.; Roberts, L.R.; Schwartz, M.; Chen, P.-J.; Kudo, M.; Johnson, P.; Wagner, S.; Orsini, L.S.; et al. Global patterns of hepatocellular carcinoma management from diagnosis to death: The BRIDGE study. Liver Int. 2015, 35, 2155–2166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roberts, S.K.; Gazzola, A.; Lubel, J.; Gow, P.; Bell, S.; Nicoll, A.; Dev, A.; Fink, M.A.; Sood, S.; Knight, V.; et al. Treatment choice for early-stage hepatocellular carcinoma in real-world practice: Impact of treatment stage migration to transarterial chemoembolization and treatment response on survival. Scand. J. Gastroenterol. 2018, 53, 1368–1375. [Google Scholar] [CrossRef]
- Ho, E.Y.; Cozen, M.L.; Shen, H.; Lerrigo, R.; Trimble, E.; Ryan, J.C.; Corvera, C.U.; Monto, A.; HOVAS Group. Expanded use of aggressive therapies improves survival in early and intermediate hepatocellular carcinoma. HPB 2014, 16, 758–767. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohnike, K.; Steffen, I.G.; Seidensticker, M.; Hass, P.; Damm, R.; Peters, N.; Seidensticker, R.; Schütte, K.; Arend, J.; Bornschein, J.; et al. Radioablation by image-guided (HDR) brachytherapy and transarterial chemoembolization in hepatocellular carcinoma: A randomized phase II trial. Cardiovasc. Intervent. Radiol. 2019, 42, 239–249. [Google Scholar] [CrossRef] [PubMed]
- N’Kontchou, G.; Aout, M.; Laurent, A.; Nahon, P.; Ganne-Carrié, N.; Grando, V.; Baghad, I.; Roulot, D.; Trinchet, J.C.; Sellier, N.; et al. Survival after radiofrequency ablation and salvage transplantation in patients with hepatocellular carcinoma and child-pugh A cirrhosis. J. Hepatol. 2012, 56, 160–166. [Google Scholar] [CrossRef] [PubMed]
- Sutter, O.; Fihri, A.; Ourabia-Belkacem, R.; Sellier, N.; Diallo, A.; Seror, O. Real-time 3D virtual target fluoroscopic display for challenging hepatocellular carcinoma ablations using cone beam CT. Technol. Cancer Res. Treat. 2018, 17, 1533033818789634. [Google Scholar] [CrossRef]
- Kim, K.M.; Sinn, D.H.; Jung, S.-H.; Gwak, G.-Y.; Paik, Y.-H.; Choi, M.S.; Lee, J.H.; Koh, K.C.; Paik, S.W. The recommended treatment algorithms of the BCLC and HKLC staging systems: Does following these always improve survival rates for HCC patients? Liver Int. 2016, 36, 1490–1497. [Google Scholar] [CrossRef]
- Salem, R.; Johnson, G.E.; Kim, E.; Riaz, A.; Bishay, V.; Boucher, E.; Fowers, K.; Lewandowski, R.; Padia, S.A. Yttrium-90 radioembolization for the treatment of solitary, unresectable HCC: The LEGACY study. Hepatology 2021, 74, 2342–2352. [Google Scholar] [CrossRef]
- Goutté, N.; Sogni, P.; Bendersky, N.; Barbare, J.C.; Falissard, B.; Farges, O. Geographical variations in incidence, management and survival of hepatocellular carcinoma in a western country. J. Hepatol. 2017, 66, 537–544. [Google Scholar] [CrossRef] [Green Version]
- Bruix, J.; Sherman, M. Management of hepatocellular carcinoma: An update. Hepatology 2011, 53, 1020–1022. [Google Scholar] [CrossRef]
- European association for the study of the liver; european organisation for research and treatment of cancer EASL-EORTC clinical practice guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2012, 56, 908–943. [CrossRef] [Green Version]
- Petit, A.; Hocquelet, A.; N’kontchou, G.; Varin, E.; Sellier, N.; Seror, O.; Sutter, O. No-touch multi-bipolar radiofrequency ablation for the treatment of subcapsular hepatocellular carcinoma ≤ 5 Cm not puncturable via the non-tumorous liver parenchyma. Cardiovasc Intervent. Radiol. 2020, 43, 273–283. [Google Scholar] [CrossRef] [PubMed]
- Loriaud, A.; Denys, A.; Seror, O.; Vietti Violi, N.; Digklia, A.; Duran, R.; Trillaud, H.; Hocquelet, A. Hepatocellular carcinoma abutting large vessels: Comparison of four percutaneous ablation systems. Int. J. Hyperth. 2018, 34, 1171–1178. [Google Scholar] [CrossRef]
- Hocquelet, A.; Aubé, C.; Rode, A.; Cartier, V.; Sutter, O.; Manichon, A.F.; Boursier, J.; N’kontchou, G.; Merle, P.; Blanc, J.-F.; et al. Comparison of no-touch multi-Bipolar vs. monopolar radiofrequency ablation for small HCC. J. Hepatol. 2017, 66, 67–74. [Google Scholar] [CrossRef]
- Seror, O.; N’Kontchou, G.; Nault, J.-C.; Rabahi, Y.; Nahon, P.; Ganne-Carrié, N.; Grando, V.; Zentar, N.; Beaugrand, M.; Trinchet, J.-C.; et al. Hepatocellular carcinoma within Milan criteria: No-touch multibipolar radiofrequency ablation for treatment-long-term results. Radiology 2016, 280, 611–621. [Google Scholar] [CrossRef]
- Nault, J.-C.; Nkontchou, G.; Nahon, P.; Grando, V.; Bourcier, V.; Barge, S.; Ziol, M.; Sellier, N.; Ganne-Carrie, N.; Seror, O. Percutaneous treatment of localized infiltrative hepatocellular carcinoma developing on cirrhosis. Ann. Surg. Oncol. 2016, 23, 1906–1915. [Google Scholar] [CrossRef] [PubMed]
- Seror, O.; N’Kontchou, G.; Ibraheem, M.; Ajavon, Y.; Barrucand, C.; Ganne, N.; Coderc, E.; Trinchet, J.C.; Beaugrand, M.; Sellier, N. Large (>or = 5.0-Cm) HCCs: Multipolar RF ablation with three internally cooled bipolar electrodes—Initial experience in 26 patients. Radiology 2008, 248, 288–296. [Google Scholar] [CrossRef]
- Seror, O.; Haddar, D.; N’Kontchou, G.; Ajavon, Y.; Trinchet, J.-C.; Beaugrand, M.; Sellier, N. Radiofrequency ablation for the treatment of liver tumors in the caudate lobe. J. Vasc. Interv. Radiol. 2005, 16, 981–990. [Google Scholar] [CrossRef]
- Sonnenberg, F.A.; Beck, J.R. Markov Models in Medical Decision Making: A practical guide. Med. Decis. Mak. 1993, 13, 322–338. [Google Scholar] [CrossRef]
- Welton, N.J.; Ades, A.E. Estimation of Markov chain transition probabilities and rates from fully and partially observed data: Uncertainty propagation, evidence synthesis, and model calibration. Med. Decis. Mak. 2005, 25, 633–645. [Google Scholar] [CrossRef] [PubMed]
- ATIH: Agence technique de l’information Sur l’hospitalisation. Available online: https://www.atih.sante.fr/ (accessed on 15 May 2021).
- Husereau, D.; Drummond, M.; Petrou, S.; Carswell, C.; Moher, D.; Greenberg, D.; Augustovski, F.; Briggs, A.H.; Mauskopf, J.; Loder, E.; et al. Consolidated health economic evaluation reporting standards (CHEERS) statement. BMJ 2013, 346, f1049. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murphy, B.; Fraeman, K. A General SAS® Macro to Implement Optimal N:1 Propensity Score Matching within a Maximum Radius. Available online: https://support.sas.com/resources/papers/proceedings17/0812-2017.pdf (accessed on 13 July 2021).
- Sterne, J.A.C.; White, I.R.; Carlin, J.B.; Spratt, M.; Royston, P.; Kenward, M.G.; Wood, A.M.; Carpenter, J.R. Multiple imputation for missing data in epidemiological and clinical research: Potential and pitfalls. BMJ 2009, 338, b2393. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline Characteristics | Unmatched Cohort | Matched Cohort | ||||
|---|---|---|---|---|---|---|
| Bondy Group | SOC Group | p-Value | Bondy Group | SOC Group | p-Value | |
| n = 272 | n = 557 | n = 266 | n = 266 | |||
| Age, mean (+/−SD) | 66 (+/−11) | 63 (+/−10) | <0.001 | 66 (+/−11) | 66 (+/−10) | 0.37 |
| Male, n (%) | 219 (81%) | 464 (83%) | 0.32 | 214 (80%) | 211 (79%) | 0.75 |
| Co-morbidity index, n (%) | 0.33 | 0.09 | ||||
| ≤1 | 262 (96%) | 528 (95%) | 256 (96%) | 247 (93%) | ||
| >1 | 10 (4%) | 29 (5%) | 10 (4%) | 19 (7%) | ||
| Cause of cirrhosis, n (%) | 0.02 | 0.87 | ||||
| Alcohol | 118 (43%) | 190 (34%) | 113 (42%) | 117 (44%) | ||
| HCV | 89 (33%) | 227 (41%) | 89 (33%) | 88 (33%) | ||
| HBV | 34 (13%) | 83 (15%) | 34 (13%) | 32 (12%) | ||
| NASH | 20 (7%) | 40 (7%) | 20 (8%) | 22 (8%) | ||
| Others | 11 (4%) | 18 (3%) | 12 (5%) | 8 (3%) | ||
| Child-Pugh score, n (%) | 0.14 | 0.88 | ||||
| A (5–6) | 249 (92%) | 491 (88%) | 243 (91%) | 244 (92%) | ||
| B (7–9) | 23 (8%) | 66 (12%) | 23 (9%) | 22 (8%) | ||
| AFP level, n (%) | 0.70 | 0.45 | ||||
| ≤100 ng/mL | 191 (70%) | 398 (71%) | 189 (71%) | 178 (67%) | ||
| 100–1000 ng/mL | 50 (18%) | 97 (17%) | 48 (18%) | 50 (19%) | ||
| >1000 ng/mL | 31 (11%) | 62 (11%) | 29 (11%) | 38 (14%) | ||
| Portal hypertension, n (%) | 158 (58%) | 297 (53%) | 0.20 | 154 (58%) | 146 (55%) | 0.48 |
| Size of the largest tumor node, n (%) | 0.42 | 0.29 | ||||
| ≤30 mm | 116 (43%) | 260 (47%) | 115 (43%) | 119 (45%) | ||
| 30–60 mm | 91 (33%) | 181 (32%) | 90 (34%) | 93 (35%) | ||
| >60 mm | 65 (24%) | 116 (21%) | 61 (23%) | 54 (20%) | ||
| Number of tumors, n (%) | 0.12 | 0.57 | ||||
| 1 | 170 (63%) | 314 (56%) | 165 (62%) | 166 (62%) | ||
| 2/3 | 63 (23%) | 167 (30%) | 63 (24%) | 61 (23%) | ||
| ≥4 | 39 (14%) | 76 (14%) | 38 (14%) | 39 (15%) | ||
| Bilobar involvment, n (%) | 65 (24%) | 146 (26%) | 0.47 | 64 (24%) | 64 (24%) | 1 |
| Vascular invasion, n (%) | 42 (15%) | 63 (11%) | 0.09 | 38 (14%) | 43 (16%) | 0.55 |
| BCLC staging, n (%) | 0.01 | 0.57 | ||||
| Very early | 16 (6%) | 60 (11%) | 16 (6%) | 22 (8%) | ||
| Early | 159 (58%) | 290 (52%) | 157 (59%) | 143 (54%) | ||
| Intermediate | 55 (20%) | 144 (26%) | 55 (21%) | 58 (22%) | ||
| Advanced | 42 (15%) | 63 (11%) | 38 (14%) | 43 (16%) | ||
| First-line treatment, n (%) | <0.001 | <0.001 | ||||
| Hepatic resection | 1 (1%) | 69 (12%) | 1 (<1%) | 35 (13%) | ||
| Ablation | 190 (70%) | 144 (26%) | 188 (71%) | 64 (24%) | ||
| TACE | 48 (18%) | 283 (51%) | 47 (18%) | 128 (48%) | ||
| TARE or Sorafenib | 32 (12%) | 60 (11%) | 30 (11%) | 39 (15%) | ||
| Probability of First-Line Treatment | Bondy Group | SOC Group | |||
| Hepatic resection | 0.4% | 13.2% | |||
| Ablation | 70.7% | 24.0% | |||
| TACE | 17.7% | 48.1% | |||
| Sorafenib | 11.2% | 14.7% | |||
| First-Line | Costs and Life-Years Per Patient | Bondy Group | SOC Group | Net Effects | ICER (€/LYG) |
| Hepatic resection | Cost | €127 ($140) | €4417 ($4860) | €−4290 ($−4720) | |
| Life-years | 0.1 | 2.6 | −2.5 | ||
| Ablation | Cost | €14,488 ($15,937) | €4904 ($5394) | €9584 ($10,543) | |
| Life-years | 11.1 | 3.8 | 7.3 | ||
| TACE | Cost | €2268 ($2495) | €13,478 ($14,826) | €−11,210 ($−12,331) | |
| Life-years | 0.7 | 4.3 | −3.6 | ||
| Sorafenib | Cost | €1322 ($1454) | €2694 ($2963) | €−1372 ($−1509) | |
| Life-years | 0.2 | 0.5 | −0.3 | ||
| Average total | Cost | €18,205 ($20,026) | €25,493 ($28,043) | €−7288 ($−8017) | Dominant |
| Life-years | 12 | 11.2 | 0.8 | ||
| Parameters | Distribution | Mode | Minimum | Maximum |
|---|---|---|---|---|
| Health state cost | Gamma | |||
| Hepatic resection | €17,666 ($19,432) | €16,900 ($18,590) | €18,300 ($20,130) | |
| Ablation | €4895 ($5385) | €4400 ($4840) | €5000 ($5500) | |
| TACE | €5708 ($6279) | €5500 ($6050) | €5800 ($6380) | |
| Sorafenib | €4500 ($4950) | €2935 ($3229) | €10,320 ($11,352) | |
| Liver transplantation | €51,779 ($56,957) | €48,900 ($53,790) | €54,000 ($59,400) | |
| Follow-up after hepatic resection or ablation | €146 ($161) | €100 ($110) | €500 ($550) | |
| Follow-up after TACE | €379 ($417) | €100 ($110) | €800 ($880) | |
| Follow-up after liver transplantation | €1514 ($1665) | €594 ($653) | €2000 ($2200) | |
| Start age | Triangular | 65 | 60 | 67 |
| Transition probabilities | Beta | Original value | 10% lower | 10% higher |
| Discount rate | Triangular | 3% | 0% | 6% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ramtohul, T.; Vilgrain, V.; Soubrane, O.; Bouattour, M.; Luciani, A.; Kobeiter, H.; Mule, S.; Tacher, V.; Laurent, A.; Amaddeo, G.; et al. Impact of Extended Use of Ablation Techniques in Cirrhotic Patients with Hepatocellular Carcinoma: A Cost-Effectiveness Analysis. Cancers 2022, 14, 2634. https://doi.org/10.3390/cancers14112634
Ramtohul T, Vilgrain V, Soubrane O, Bouattour M, Luciani A, Kobeiter H, Mule S, Tacher V, Laurent A, Amaddeo G, et al. Impact of Extended Use of Ablation Techniques in Cirrhotic Patients with Hepatocellular Carcinoma: A Cost-Effectiveness Analysis. Cancers. 2022; 14(11):2634. https://doi.org/10.3390/cancers14112634
Chicago/Turabian StyleRamtohul, Toulsie, Valérie Vilgrain, Olivier Soubrane, Mohamed Bouattour, Alain Luciani, Hicham Kobeiter, Sébastien Mule, Vania Tacher, Alexis Laurent, Giuliana Amaddeo, and et al. 2022. "Impact of Extended Use of Ablation Techniques in Cirrhotic Patients with Hepatocellular Carcinoma: A Cost-Effectiveness Analysis" Cancers 14, no. 11: 2634. https://doi.org/10.3390/cancers14112634