
Concordance, Correlation, and Clinical Impact of Standardized PD-L1 and TIL Scoring in SCCHN

 , , , , ,
, , , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Population and Sample Selection
2.2. Evaluation of the Tumor Microenvironment
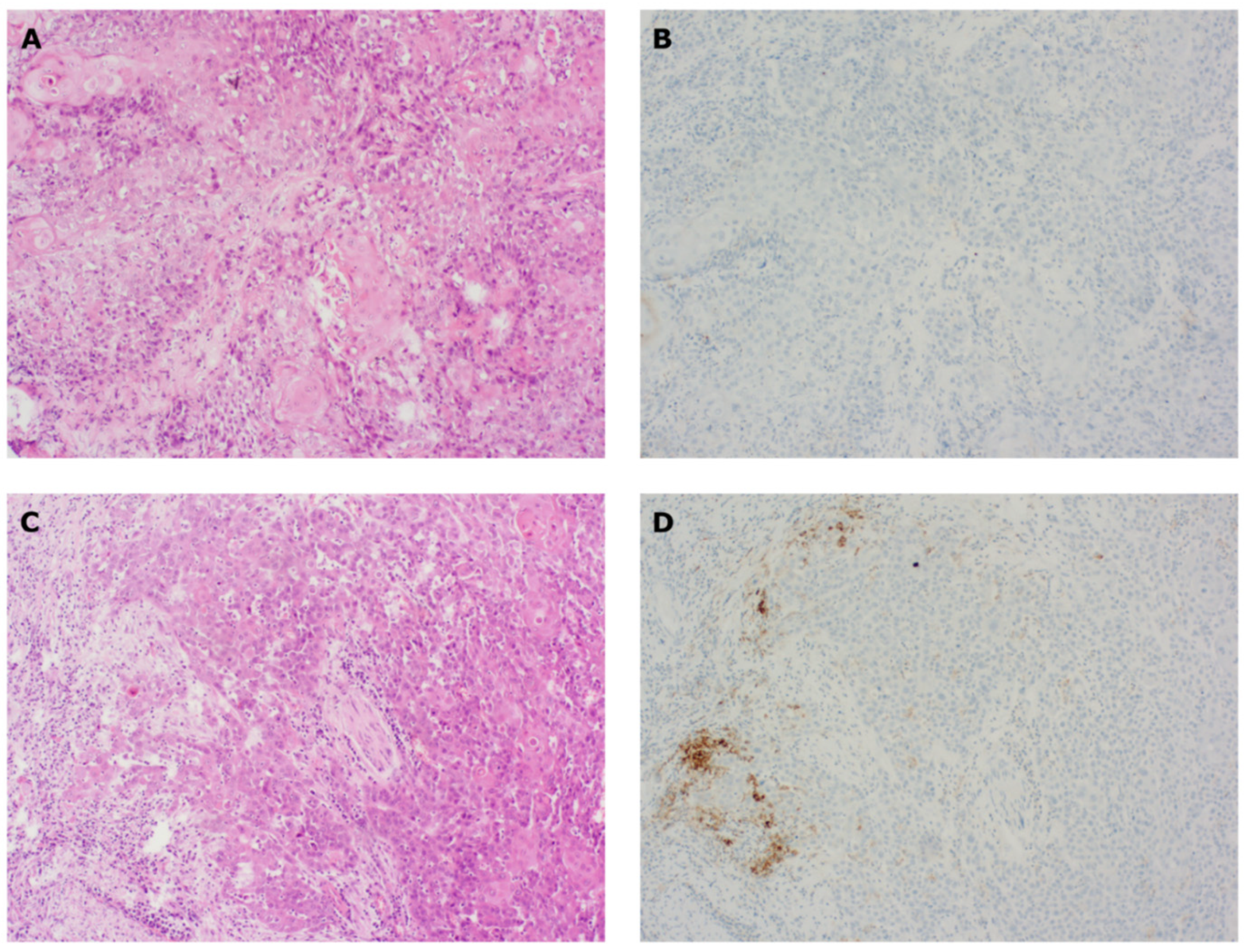
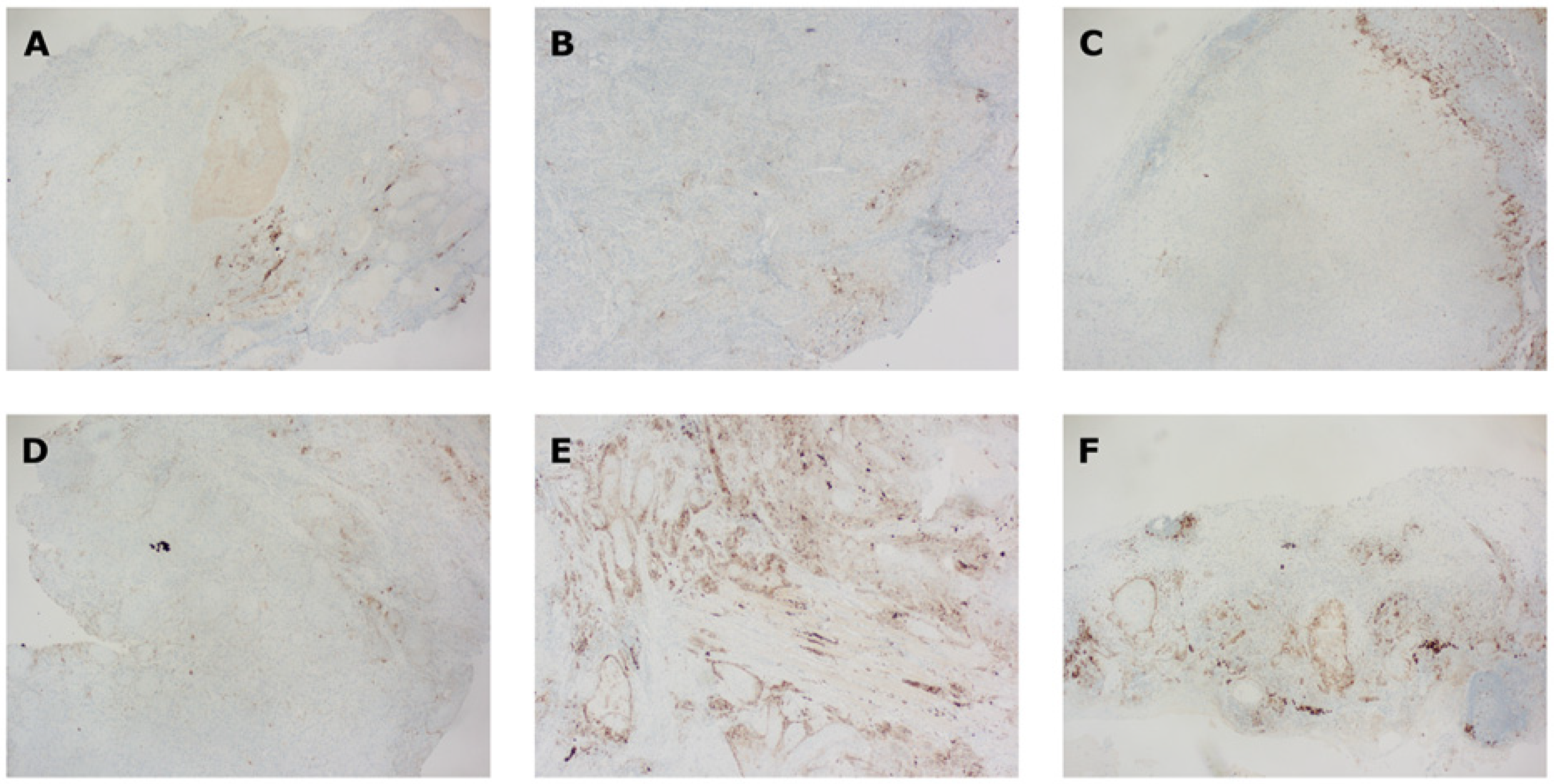
2.2.1. PD-L1 IHC
2.2.2. TIL Scoring
2.3. Statistics
3. Results
3.1. PD-L1 CPS and TIL Scores
3.2. Tissue Concordance
3.2.1. CPS
3.2.2. TIL Count
3.3. Temporal Heterogeneity
3.4. Correlation between CPS, TILs, and Clinicopathological Parameters
3.5. Effect of CPS and TILs on Survival Outcome
3.5.1. DFS
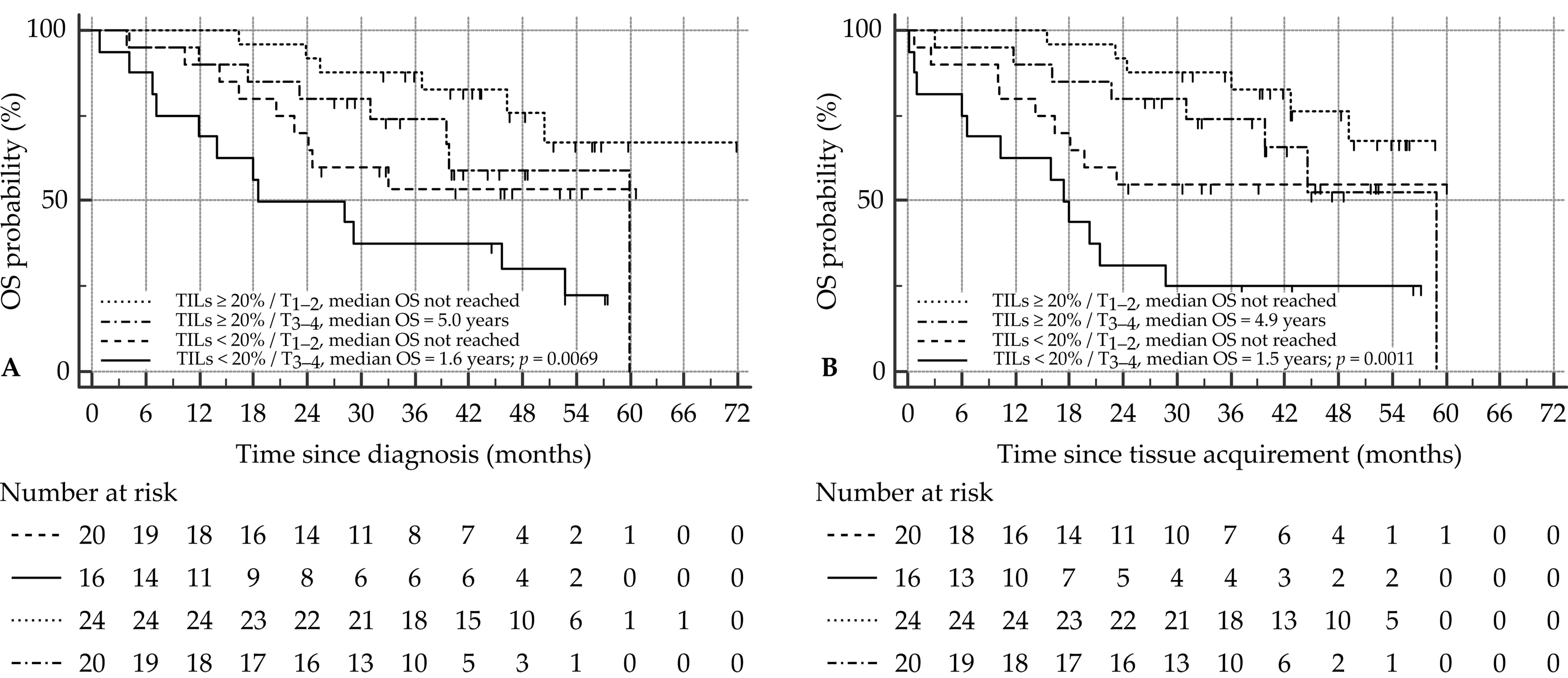
3.5.2. OS since Time of Diagnosis
3.5.3. OS since Time of Tissue Acquirement
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- De Keukeleire, S.J.; Vermassen, T.; Hilgert, E.; Creytens, D.; Ferdinande, L.; Rottey, S. Immuno-Oncological Biomarkers for Squamous Cell Cancer of the Head and Neck: Current State of the Art and Future Perspectives. Cancers 2021, 13, 1714. [Google Scholar] [CrossRef] [PubMed]
- Oliva, M.; Spreafico, A.; Taberna, M.; Alemany, L.; Coburn, B.; Mesia, R.; Siu, L. Immune biomarkers of response to immune-checkpoint inhibitors in head and neck squamous cell carcinoma. Ann. Oncol. 2019, 30, 57–67. [Google Scholar] [CrossRef] [PubMed]
- Ferris, R.L.; Blumenschein, G.; Fayette, J.; Guigay, J.; Colevas, A.D.; Licitra, L.; Harrington, K.; Kasper, S.; Vokes, E.E.; Even, C.; et al. Nivolumab for Recurrent Squamous-Cell Carcinoma of the Head and Neck. N. Engl. J. Med. 2016, 375, 1856–1867. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zandberg, D.P.; Algazi, A.P.; Jimeno, A.; Good, J.S.; Fayette, J.; Bouganim, N. Durvalumab for recurrent or metastatic head and neck squamous cell carcinoma: Results from a single-arm, phase II study in patients with ≥25% tumour cell PD-L1 expression who have progressed on platinum-based chemotherapy. Eur. J. Cancer 2019, 107, 142–152. [Google Scholar] [CrossRef] [Green Version]
- Denaro, N.; Carlo Merlano, M. Immunotherapy in head and neck squamous cell cancer. Clin. Exp. Otorhinolaryngol. 2018, 11, 217–223. [Google Scholar] [CrossRef]
- Bauml, J.; Seiwert, T.Y.; Pfister, D.G.; Worden, F.; Liu, S.V.; Gilbert, J.; Saba, N.F.; Weiss, J.; Wirth, L.; Sukari, A.; et al. Pembrolizumab for platinum- and cetuximab-refractory head and neck cancer: Results from a single-arm, phase II study. J. Clin. Oncol. 2017, 35, 1542–1549. [Google Scholar] [CrossRef]
- McCusker, M.G.; Orkoulas-Razis, D.; Mehra, R. Potential of pembrolizumab in metastatic or recurrent head and neck cancer: Evidence to date. OncoTargets Ther. 2020, 13, 3047–3059. [Google Scholar] [CrossRef] [Green Version]
- Seiwert, T.Y.; Burtness, B.; Mehra, R.; Weiss, J.; Berger, R.; Eder, J.P.; McClanahan, T.; Lunceford, J.; Gause, C.; Cheng, J.D.; et al. Safety and clinical activity of pembrolizumab for treatment of recurrent or metastatic squamous cell carcinoma of the head and neck (KEYNOTE-012): An open-label, multicentre, phase 1b trial. Lancet Oncol. 2016, 17, 956–965. [Google Scholar] [CrossRef]
- Ott, P.A.; Bang, Y.-J.; Piha-Paul, S.A.; Razak, A.R.A.; Bennouna, J.; Soria, J.-C.; Rugo, H.S.; Cohen, R.B.; O’Neil, B.H.; Mehnert, J.M.; et al. T-cell–inflamed gene-expression profile, programmed death ligand 1 expression, and tumor mutational burden predict efficacy in patients treated with pembrolizumab across 20 cancers: KEYNOTE-028. J. Clin. Oncol. 2019, 37, 318–327. [Google Scholar] [CrossRef]
- Burtness, B.; Harrington, K.J.; Greil, R.; Soulières, D.; Tahara, M.; De Castro, G. Pembrolizumab alone or with chemotherapy versus cetuximab with chemotherapy for recurrent or metastatic squamous cell carcinoma of the head and neck (KEYNOTE-048): A randomised, open-label, phase 3 study. Lancet 2019, 394, 1915–1928. [Google Scholar] [CrossRef]
- Hendry, S.; Salgado, R.; Gevaert, T.; Russell, P.A.; John, T.; Thapa, B.; Christie, M.; van de Vijver, K.; Estrada, M.V.; Gonzalez-Ericsson, P.I.; et al. Assessing Tumor-infiltrating Lymphocytes in Solid Tumors: A Practical Review for Pathologists and Proposal for a Standardized Method from the International Immunooncology Biomarkers Working Group: Part 1: Assessing the Host Immune Response, TILs in Invasive Breast Carcinoma and Ductal Carcinoma In Situ, Metastatic Tumor Deposits and Areas for Further Research. Adv. Anat. Pathol. 2017, 24, 235–251. [Google Scholar] [PubMed] [Green Version]
- Hendry, S.; Salgado, R.; Gevaert, T.; Russell, P.A.; John, T.; Thapa, B.; Christie, M.; van de Vijver, K.; Estrada, M.V.; Gonzalez-Ericsson, P.I.; et al. Assessing Tumor-Infiltrating Lymphocytes in Solid Tumors: A Practical Review for Pathologists and Proposal for a Standardized Method from the International Immuno-Oncology Biomarkers Working Group: Part 2: TILs in Melanoma, Gastrointestinal Tract Carcinomas, Non-Small Cell Lung Carcinoma and Mesothelioma, Endometrial and Ovarian Carcinomas, Squamous Cell Carcinoma of the Head and Neck, Genitourinary Carcinomas, and Primary Brain Tumors. Adv. Anat. Pathol. 2017, 24, 311–335. [Google Scholar] [PubMed]
- De Keukeleire, S.; Vermassen, T.; De Meulenaere, A.; Duprez, F.; Deron, P.; Huvenne, W.; Duprez, F.; Creytens, D.; Van Dorpe, J.; Rottey, S.; et al. TILs in oropharyngeal carcinoma: Prognostic value and evaluation of a standardized method. Pathology 2021, 53, 836–843. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, J.H.; Lelkaitis, G.; Håkansson, K.; Vogelius, I.R.; Johannesen, H.H.; Fischer, M.; Bentzen, S.M.; Specht, L.; Kristensen, C.A.; von Buchwald, C.; et al. Intratumor heterogeneity of PD-L1 expression in head and neck squamous cell carcinoma. Br. J. Cancer 2019, 120, 1003–1006. [Google Scholar] [CrossRef] [Green Version]
- Cimino-Mathews, A.; Thompson, E.A.; Taube, J.M.; Ye, X.; Lu, Y.; Meeker Al Xu, H.; Sharma, R.; Lecksell, K.; Cornish, T.; Cuka, N.; et al. PD-L1 (B7-H1) expression and the immune tumor microenvironment in primary and metastatic breast carcinomas. Hum Pathol. 2016, 25, 1032–1057. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Yin, X.; Zhang, H.; Sun, G.; Yang, Y.; Chen, J.; Zhu, X.; Zhao, P.; Liu, J.; Chen, N.; et al. Differential expression of TIM-3 between primary and metastatic sites in renal cell carcinoma. BMC Cancer 2019, 19, 49. [Google Scholar] [CrossRef]
- Svensson, M.C.; Borg, D.; Zhang, C.; Hedner, C.; Nodin, B.; Uhlén, M.; Mardinoglu, A.; Leandersson, K.; Jirström, K. Expression of PD-L1 and PD-1 in chemoradiotherapy-Naïve esophageal and gastric adenocarcinoma: Relationship with mismatch repair status and survival. Front. Oncol. 2019, 9, 136. [Google Scholar] [CrossRef]
- Manson, Q.F.; Schrijver, W.A.M.E.; ter Hoeve, N.D.; Moelans, C.B.; van Diest, P.J. Frequent discordance in PD-1 and PD-L1 expression between primary breast tumors and their matched distant metastases. Clin. Exp. Metastasis 2019, 36, 29–37. [Google Scholar] [CrossRef] [Green Version]
- Straub, M.; Drecoll, E.; Pfarr, N.; Weichert, W.; Langer, R.; Hapfelmeier, A.; Götz, E.; Wolf, K.D.; Kolk, A.; Specht, K. CD274/PD-L1 gene amplification and PD-L1 protein expression are common events in squamous cell carcinoma of the oral cavity. Oncotarget 2016, 7, 12024–12034. [Google Scholar] [CrossRef] [Green Version]
- Okada, S.; Itoh, K.; Ishihara, S.; Shimada, J.; Kato, D.; Tsunezuka, H.; Miyata, N.; Hirano, S.; Teramukai, S.; Inoue, M. Significance of PD-L1 expression in pulmonary metastases from head and neck squamous cell carcinoma. Surg. Oncol. 2018, 27, 259–265. [Google Scholar] [CrossRef]
- Zou, Y.; Hu, X.; Zheng, S.; Yang, A.; Li, X.; Tang, H.; Kong, Y.; Xie, X. Discordance of immunotherapy response predictive biomarkers between primary lesions and paired metastases in tumours: A multidimensional analysis. EBioMedicine 2021, 63, 103137. [Google Scholar] [CrossRef] [PubMed]
- Mansfield, A.S.; Aubry, M.C.; Moser, J.C.; Harrington, S.M.; Dronca, R.S.; Park, S.S.; Dong, H. Temporal and spatial discordance of programmed cell death-ligand 1 expression and lymphocyte tumor infiltration between paired primary lesions and brain metastases in lung cancer. Ann. Oncol. 2016, 27, 1953–1958. [Google Scholar] [CrossRef] [PubMed]
- Gagné, A.; Wang, E.; Bastien, N.; Orain, M.; Desmeules, P.; Pagé, S.; Trahan, S.; Couture, C.; Joubert, D.; Joubert, P. Impact of Specimen Characteristics on PD-L1 Testing in Non–Small Cell Lung Cancer: Validation of the IASLC PD-L1 Testing Recommendations. J. Thorac. Oncol. 2019, 14, 2062–2070. [Google Scholar] [CrossRef]
- Paintal, A.S.; Brockstein, B.E. PD-L1 CPS Scoring Accuracy in Small Biopsies and Aspirate Cell Blocks from Patients with Head and Neck Squamous Cell Carcinoma. Head Neck Pathol. 2019, 14, 657–665. [Google Scholar] [CrossRef]
- Tsao, M.S.; Kerr, K.M.; Kockx, M.; Beasley, M.B.; Borczuk, A.C.; Botling, J.; Bubendorf, J.; Chirieac, L.; Chen, G.; Chou, G.T.; et al. PD-L1 Immunohistochemistry Comparability Study in Real-Life Clinical Samples: Results of Blueprint Phase 2 Project. J. Thorac. Oncol. 2018, 13, 1302–1311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neuman, T.; London, M.; Kania-Almog, J.; Litvin, A.; Zohar, Y.; Fridel, L.; Sandbank, J.; Barshak Vainer, G. A harmonization study for the use of 22C3 PD-L1 immunohistochemical staining on ventana’s platform. J. Thorac. Oncol. 2016, 11, 1863–1868. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crosta, S.; Boldorini, R.; Bono, F.; Brambilla, V.; Dainese, E.; Fusco, N.; Gianatta, A.; L’Imperio, V.; Morbine, P.; Pagni, F. PD-L1 testing and squamous cell carcinoma of the head and neck: A multicenter study on the diagnostic reproducibility of different protocols. Cancers 2021, 13, 292. [Google Scholar] [CrossRef]
- Dako. PD-L1 IHC 22C3 pharmDx Interpretation Manual—Head and Neck Squamous Cell Carcinoma (HNSCC); Agilent Technologies, Inc.: Santa Clara, CA, USA, 2019; pp. 1–72. [Google Scholar]
- Althammer, S.; Tan, T.H.; Spitzmüller, A.; Rognoni, L.; Wiestler, T.; Herz, T.; Widmaier, M.; Rebellato, M.; Kaplon, H.; Damotte, D.; et al. Automated image analysis of NSCLC biopsies to predict response to anti-PD-L1 therapy. J. Immunother. Cancer 2019, 7, 121. [Google Scholar] [CrossRef] [Green Version]
- Inge, L.J.; Dennis, E. Development and applications of computer image analysis algorithms for scoring of PD-L1 immunohistochemistry. Immuno-Oncol. Technol. 2020, 6, 2–8. [Google Scholar] [CrossRef]
- Scognamiglio, T.; Chen, Y.T. Beyond the Percentages of PD-L1-Positive Tumor Cells: Induced Versus Constitutive PD-L1 Expression in Primary and Metastatic Head and Neck Squamous Cell Carcinoma. Head Neck Pathol. 2018, 12, 221–229. [Google Scholar] [CrossRef]
- Taube, J.M.; Anders, R.A.; Young, G.D.; Xu, H.; Sharma, R.; McMiller, T.L.; Chen, S.; Klein, A.P.; Pardoll, D.M.; Topalian, S.L.; et al. Colocalization of inflammatory response with B7-H1 expression in human melanocytic lesions supports an adaptive resistance mechanism of immune escape. Sci. Transl. Med. 2012, 4, 127ra37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Meulenaere, A.; Vermassen, T.; Aspeslagh, S.; Deron, P.; Duprez, F.; Laukens, D.; Van Dorpe, J.; Ferdinande, L.; Rottey, S. Tumor PD-L1 status and CD8+ tumor-infiltrating T cells: Markers of improved prognosis in oropharyngeal cancer. Oncotarget 2017, 8, 80443–80452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ren, D.; Hua, Y.; Yu, B.; Ye, X.; He, Z.; Li, C.; Wang, J.; Mo, Y.; Wei, X.; Chen, Y.; et al. Predictive biomarkers and mechanisms underlying resistance to PD1/PD-L1 blockade cancer immunotherapy. Mol. Cancer 2020, 19, 19. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Canteli, M.; Granda-Díaz, R.; del Rio-Ibisate, N.; Allonca, E.; López-Alvarez, F.; Agorreta, J.; Garmendia, I.; Montuenga, L.M.; Garcia-Pedrero, J.M.; Rodrigo, J.P. PD-L1 expression correlates with tumor-infiltrating lymphocytes and better prognosis in patients with HPV-negative head and neck squamous cell carcinomas. Cancer Immunol. Immunother. 2020, 69, 2089–2100. [Google Scholar] [CrossRef]
- Cavalcanti, E.; Armentano, R.; Valentini, A.M.; Chieppa, M.; Caruso, M.L. Role of PD-L1 expression as a biomarker for GEP neuroendocrine neoplasm grading. Cell Death Dis. 2017, 8, e3004. [Google Scholar] [CrossRef]
- Huynh, T.G.; Morales-Oyarvide, V.; Campo, M.J.; Gainor, J.F.; Bozkurtlar, E.; Uruga, H.; Zhao, L.; Gomez-Caraballo, M.; Hata, A.N.; Mark, E.J.; et al. Programmed cell death ligand 1 expression in resected lung adenocarcinomas: Association with immune microenvironment. J. Thorac. Oncol. 2016, 11, 1869–1878. [Google Scholar] [CrossRef] [Green Version]
- Jin, Y.; Shen, X.; Pan, Y.; Zheng, Q.; Chen, H.; Hu, H.; Yuan, L. Correlation between PD-L1 expression and clinicopathological characteristics of non-small cell lung cancer: A real-world study of a large Chinese cohort. J. Thorac. Dis. 2019, 11, 4591–4601. [Google Scholar] [CrossRef]
- Naso, J.R.; Wang, G.; Pender, A.; Wong, S.K.; Zhu, J.; Ho, C.; Ionescu, D.N.; Chen, Z. Intratumoral heterogeneity in programmed death-ligand 1 immunoreactivity is associated with variation in non-small cell lung carcinoma histotype. Histopathology 2020, 76, 394–403. [Google Scholar] [CrossRef]
- Wang, J.; Tian, S.; Sun, J.; Zhang, J.; Lin, L.; Hu, C. The presence of tumour-infiltrating lymphocytes (TILs) and the ratios between different subsets serve as prognostic factors in advanced hypopharyngeal squamous cell carcinoma. BMC Cancer 2020, 20, 731. [Google Scholar] [CrossRef]
- Balermpas, P.; Michel, Y.; Wagenblast, J.; Seitz, O.; Weiss, C.; Rödel, F.; Rödel, C.; Fokas, E. Tumour-infiltrating lymphocytes predict response to definitive chemoradiotherapy in head and neck cancer. Br. J. Cancer 2014, 110, 501–509. [Google Scholar] [CrossRef]
- Chen, S.W.; Li, S.H.; Shi, D.B.; Jiang, W.M.; Song, M.; Yang, A.K.; Li, Y.D.; Bei, J.X.; Chen, W.K.; Zhang, Q. Expression of PD-1/PD-L1 in head and neck squamous cell carcinoma and its clinical significance. Int. J. Biol. Markers 2019, 34, 398–405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, W.; Wong, M.C.M.; Thomson, P.J.; Li, K.-Y.; Su, Y. The prognostic role of PD-L1 expression for survival in head and neck squamous cell carcinoma: A systematic review and meta-analysis. Oral Oncol. 2018, 86, 81–90. [Google Scholar] [CrossRef] [PubMed]
- Schneider, S.; Kadletz, L.; Wiebringhaus, R.; Kenner, L.; Selzer, E.; Füreder, T.; Rajky, O.; Berghoff, A.S.; Preuser, M.; Heiduschka, G. PD-1 and PD-L1 expression in HNSCC primary cancer and related lymph node metastasis–impact on clinical outcome. Histopathology 2018, 73, 573–584. [Google Scholar] [CrossRef] [PubMed]
- Hirshoren, N.; Al-Kharouf, I.; Weinberger, J.M.; Eliashar, R.; Popovtzer, A.; Knaanie, A.; Fellig, Y.; Neuman, T.; Meir, K.; Maly, A.; et al. Spatial Intratumoral Heterogeneity Expression of PD-L1 Antigen in Head and Neck Squamous Cell Carcinoma. Oncology 2021, 99, 464–470. [Google Scholar] [CrossRef]
- Priante, A.V.M.; Castilho, E.C.; Kowalski, L.P. Second Primary Tumors in Patients with Head and Neck Cancer. Curr. Oncol. 2011, 13, 132–137. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age, Years (Median (Range)) | 62 (42–82) | |
| Gender | Female | 13 (16) |
| Male | 67 (84) | |
| Smoking history | ≥20 PY | 63 (79) |
| <20 PY | 17 (21) | |
| Alcohol abuse (≥30 U/week) | Yes | 50 (63) |
| No | 30 (68) | |
| Tumor site | Oral cavity | 39 (49) |
| Oropharynx | 12 (15) | |
| Hypopharynx | 13 (16) | |
| Larynx | 16 (20) | |
| T stage | 1 | 24 (30) |
| 2 | 20 (25) | |
| 3 | 18 (23) | |
| 4 | 18 (23) | |
| N stage | 0 | 46 (58) |
| 1+ | 34 (42) | |
| Prognostic stage | I | 16 (20) |
| II | 12 (15) | |
| III | 14 (18) | |
| IVa | 32 (40) | |
| IVb | 4 (5) | |
| IVc | 2 (3) | |
| Grade of differentiation | Good | 7 (9) |
| Moderate | 42 (53) | |
| Poor | 26 (33) | |
| Basaloid | 5 (6) | |
| Primary therapy | Surgery | 56 (70) |
| Radiotherapy | 11 (14) | |
| Radiochemotherapy | 12 (15) | |
| Chemotherapy | 1 (1) |
| Tissue Type | Blocks | TILs * | TILs ≥ 20% | CPS * | CPS < 1 | CPS 1–19 | CPS ≥ 20 |
|---|---|---|---|---|---|---|---|
| Biopsy | 58 | 15 (1–90) | 24/53 § | 2 (0–60) | 18 | 35 | 5 |
| Resection | 63 | 20 (0–80) | 36 | 5 (0–100) | 9 | 39 | 15 |
| Lymph node | 36 | 20 (0–80) | 15/26 § | 8 (0–100) | 5 | 22 | 9 |
| Distant metastasis | 6 | 4 (0–26) | 1 | 3 (0–30) | 3 | 3 | 0 |
| A. Biopsy vs. resection | ||||||
| CPS | Biopsy | |||||
| <1 | ≥1 | p | ||||
| Resection | <1 | 2 | (14) | 5 | (17) | 1.0000 |
| ≥1 | 12 | (86) | 25 | (83) | ||
| TILs | Biopsy | |||||
| <20% | ≥20% | p | ||||
| Resection | <20% | 14 | (56) | 3 | (19) | 0.0251 |
| ≥20% | 11 | (44) | 13 | (81) | ||
| B. Biopsy vs. lymph node | ||||||
| CPS | Biopsy | |||||
| <1 | ≥1 | p | ||||
| Lymph node | <1 | 3 | (38) | 0 | (0) | 0.0686 |
| ≥1 | 5 | (63) | 10 | (100) | ||
| TILs | Biopsy | |||||
| <20% | ≥20% | p | ||||
| Lymph node | <20% | 2 | (50) | 4 | (40) | 1.0000 |
| ≥20% | 2 | (50) | 6 | (60) | ||
| C. Resection vs. lymph node | ||||||
| CPS | Resection | |||||
| <1 | ≥1 | p | ||||
| Lymph node | <1 | 1 | (14) | 3 | (17) | 0.1481 |
| ≥1 | 0 | (86) | 23 | (83) | ||
| TILs | Resection | |||||
| <20% | ≥20% | p | ||||
| Lymph node | <20% | 3 | (43) | 5 | (46) | 1.0000 |
| ≥20% | 4 | (57) | 6 | (54) | ||
| D. Primary tumor vs. metastasis | ||||||
| CPS | Primary tumors | |||||
| <1 | ≥1 | p | ||||
| Metastasis | <1 | 2 | (40) | 4 | (13) | 0.1858 |
| ≥1 | 3 | (60) | 27 | (87) | ||
| TILs | Primary tumors | |||||
| <20% | ≥20% | p | ||||
| Metastasis | <20% | 5 | (56) | 7 | (44) | 0.6882 |
| ≥20% | 4 | (44) | 9 | (56) | ||
| Variables | CPS < 1 | CPS 1–19 | CPS ≥ 20 | p | TILs < 20% | TILs ≥ 20% | p | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Age < 65 years | ||||||||||||
| No | 7 | (14) | 30 | (61) | 12 | (24) | 0.8614 | 22 | (45) | 27 | (55) | 0.7960 |
| Yes | 5 | (16) | 20 | (65) | 6 | (19) | 13 | (42) | 18 | (58) | ||
| Second primary | ||||||||||||
| No | 7 | (12) | 37 | (64) | 14 | (24) | 0.4686 | 26 | (45) | 32 | (55) | 0.8051 * |
| Yes | 5 | (23) | 13 | (59) | 4 | (18) | 9 | (41) | 13 | (59) | ||
| Smoker | ||||||||||||
| <20 PY | 4 | (24) | 6 | (35) | 7 | (41) | 0.0310 | 9 | (53) | 8 | (47) | 0.4208 * |
| ≥20 PY | 8 | (13) | 44 | (70) | 11 | (17) | 26 | (41) | 37 | (59) | ||
| Alcohol abuse | ||||||||||||
| No | 5 | (17) | 15 | (50) | 10 | (33) | 0.1501 | 9 | (30) | 21 | (70) | 0.0657 * |
| Yes | 7 | (14) | 35 | (70) | 8 | (16) | 26 | (52) | 24 | (48) | ||
| P16 status | ||||||||||||
| Negative | 10 | (14) | 45 | (63) | 16 | (23) | 0.8060 | 31 | (44) | 40 | (56) | 1.0000 * |
| Positive | 2 | (22) | 5 | (56) | 2 | (22) | 4 | (44) | 5 | (56) | ||
| Topography | ||||||||||||
| Oral cavity | 6 | (15) | 24 | (62) | 9 | (23) | 0.8115 | 14 | (36) | 25 | (64) | 0.1328 |
| Oropharynx | 1 | (8) | 9 | (75) | 2 | (17) | 4 | (33) | 8 | (67) | ||
| Hypopharynx | 1 | (8) | 8 | (62) | 4 | (31) | 6 | (46) | 7 | (54) | ||
| Larynx | 4 | (25) | 9 | (56) | 3 | (19) | 11 | (69) | 5 | (31) | ||
| Differentiation | ||||||||||||
| Good | 3 | (43) | 4 | (57) | 0 | (0) | 0.0007 | 2 | (29) | 5 | (71) | 0.8106 |
| Moderate | 6 | (14) | 31 | (74) | 5 | (12) | 20 | (48) | 22 | (52) | ||
| Poor | 1 | (4) | 12 | (46) | 13 | (50) | 11 | (42) | 15 | (58) | ||
| Basaloid | 2 | (40) | 3 | (60) | 0 | (0) | 2 | (40) | 3 | (60) | ||
| AJCC stage | ||||||||||||
| I/II | 4 | (14) | 19 | (68) | 5 | (18) | 0.7316 | 11 | (39) | 17 | (61) | 0.5572 |
| III/IV | 8 | (15) | 31 | (60) | 13 | (25) | 24 | (46) | 28 | (54) | ||
| T stage | ||||||||||||
| 1–2 | 7 | (16) | 29 | (66) | 8 | (18) | 0.5927 | 19 | (43) | 25 | (57) | 0.9104 |
| 3–4 | 5 | (14) | 21 | (58) | 10 | (28) | 16 | (44) | 20 | (56) | ||
| N stage | ||||||||||||
| 0 | 10 | (22) | 26 | (57) | 10 | (22) | 0.1406 | 19 | (41) | 27 | (59) | 0.6103 |
| 1+ | 2 | (6) | 24 | (71) | 8 | (24) | 16 | (47) | 18 | (53) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Keukeleire, S.J.; Vermassen, T.; Deron, P.; Huvenne, W.; Duprez, F.; Creytens, D.; Van Dorpe, J.; Ferdinande, L.; Rottey, S. Concordance, Correlation, and Clinical Impact of Standardized PD-L1 and TIL Scoring in SCCHN. Cancers 2022, 14, 2431. https://doi.org/10.3390/cancers14102431
De Keukeleire SJ, Vermassen T, Deron P, Huvenne W, Duprez F, Creytens D, Van Dorpe J, Ferdinande L, Rottey S. Concordance, Correlation, and Clinical Impact of Standardized PD-L1 and TIL Scoring in SCCHN. Cancers. 2022; 14(10):2431. https://doi.org/10.3390/cancers14102431
Chicago/Turabian StyleDe Keukeleire, Stijn Jeroen, Tijl Vermassen, Philippe Deron, Wouter Huvenne, Fréderic Duprez, David Creytens, Jo Van Dorpe, Liesbeth Ferdinande, and Sylvie Rottey. 2022. "Concordance, Correlation, and Clinical Impact of Standardized PD-L1 and TIL Scoring in SCCHN" Cancers 14, no. 10: 2431. https://doi.org/10.3390/cancers14102431