
Rethinking the TNM Classification Regarding Direct Lymph Node Invasion in Pancreatic Ductal Adenocarcinoma

 , , , , and
, , , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Clinical Data
2.2. Histopathological Assessment: Grossing, Histological Examination and Reexamination of Lymph Node Metastases
2.3. Statistical Analysis
3. Results
3.1. Demographics
3.2. Survival Analysis
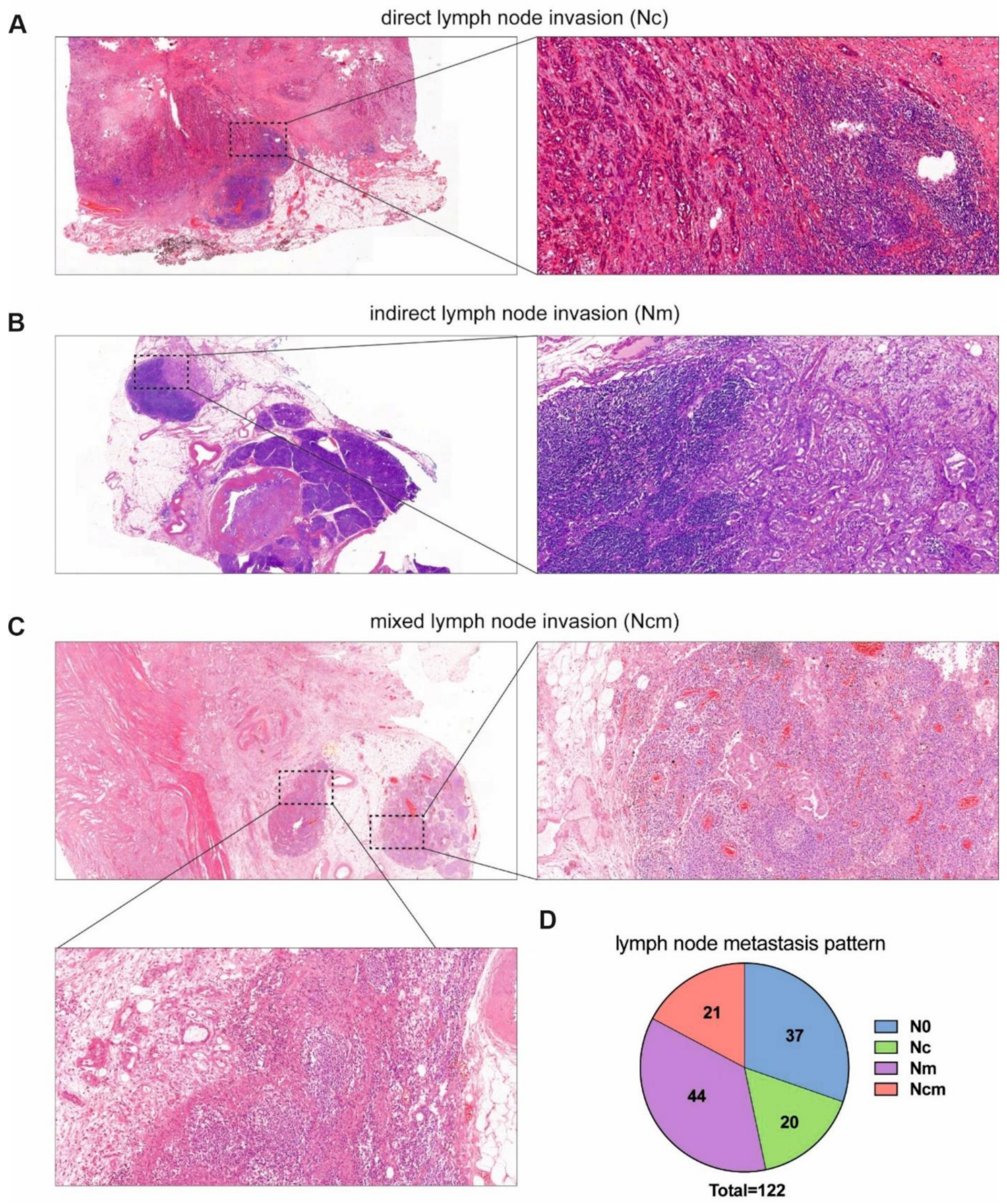
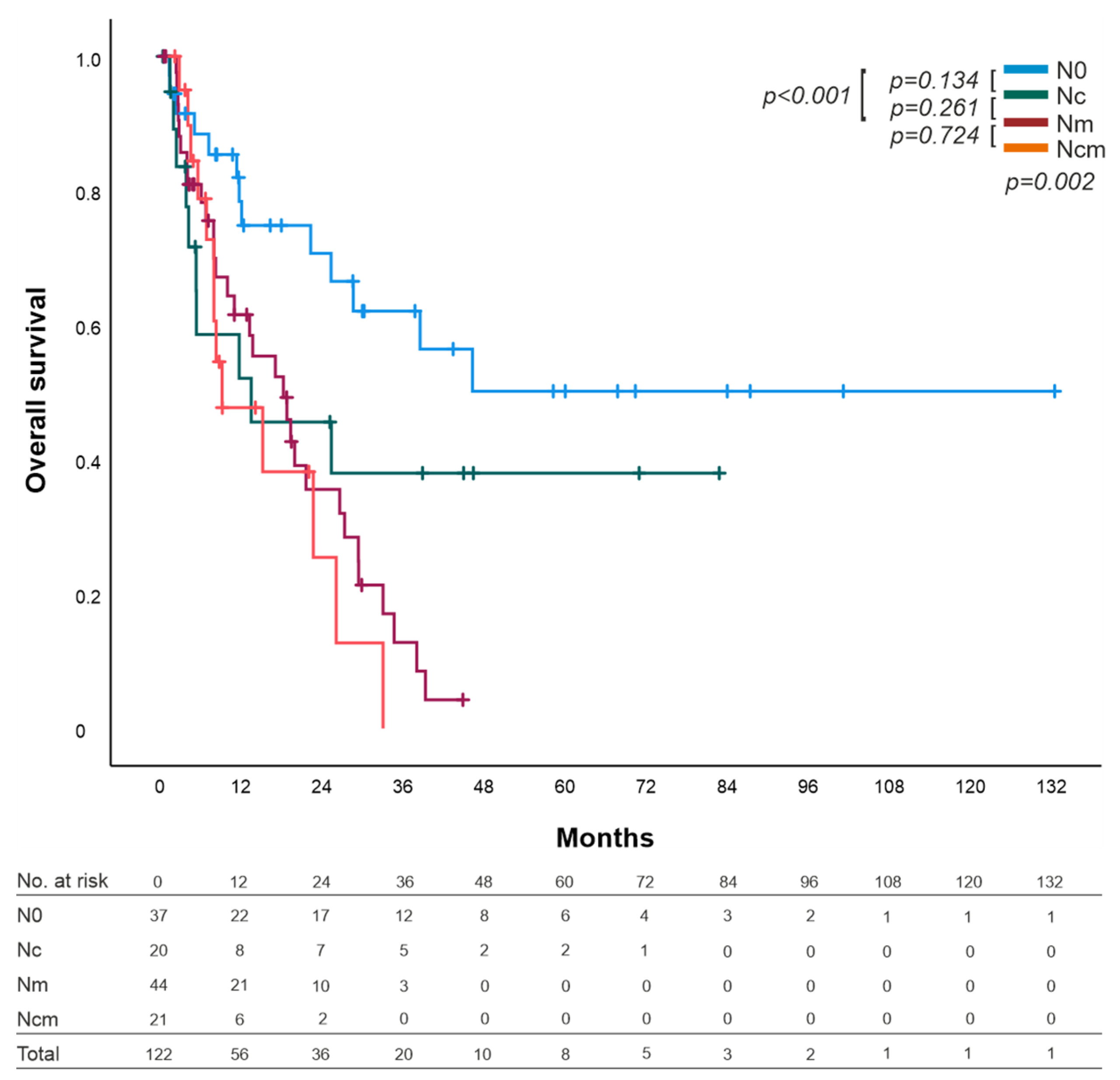
3.2.1. Analysis by the Mechanism of Lymph Node Invasion
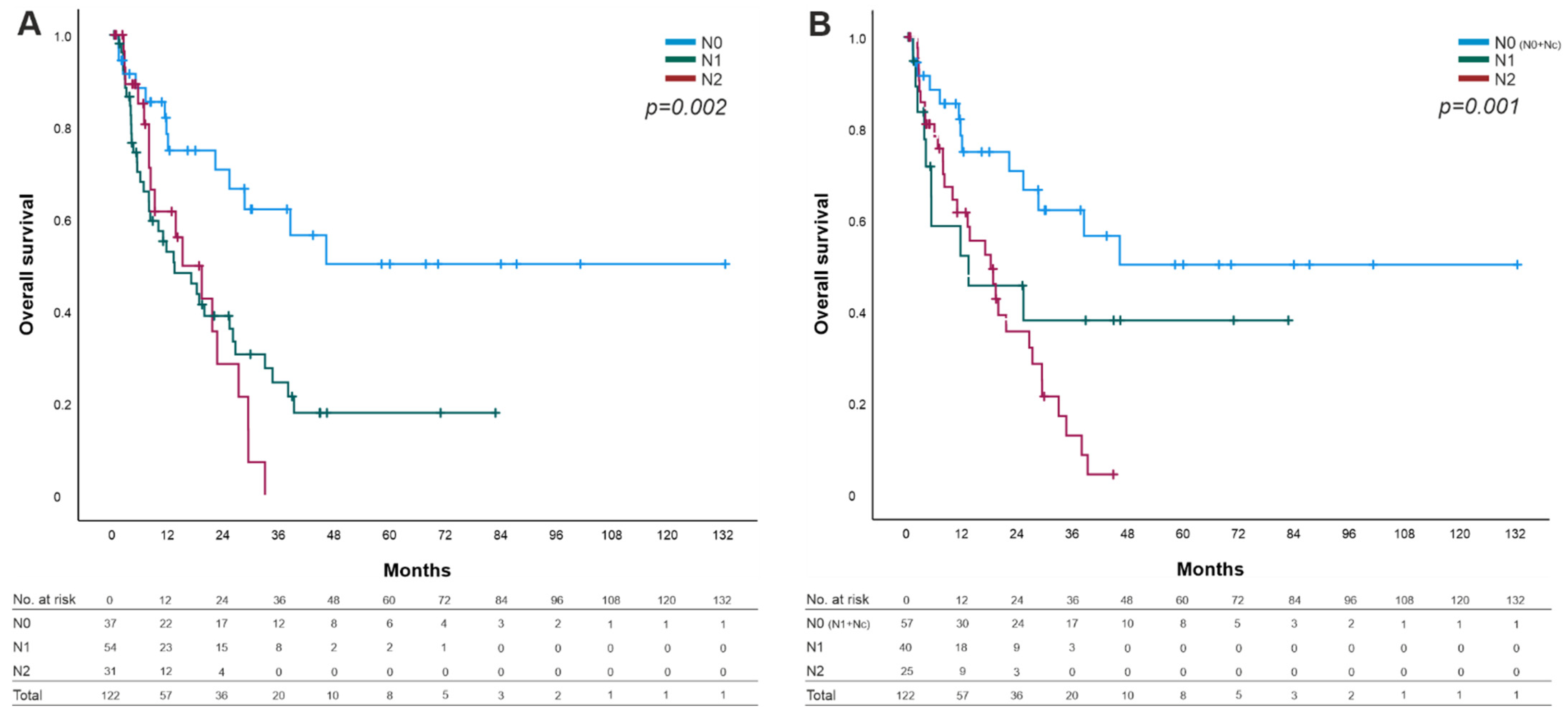
3.2.2. Overall Survival by TNM Classification and UICC Stages
3.3. Prognosis Factors
3.4. Contribution of Disease Recurrence by Node Invasion Mechanism
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rawla, P.; Sunkara, T.; Gaduputi, V. Epidemiology of pancreatic cancer: Global trends, etiology and risk factors. World J. Oncol. 2019, 10, 10–27. [Google Scholar] [CrossRef] [PubMed]
- Wild, C.P.; Weiderpass, E.; Stewart, B.W. (Eds.) World Cancer Report: Cancer Research for Cancer Prevention; International Agency for Research on Cancer: Lyon, France, 2020. Available online: http://publications.iarc.fr/586 (accessed on 23 June 2021).
- Berger, A.C.; Watson, J.C.; Ross, E.A.; Hoffman, J.P. The metastatic/examined lymph node ratio is an important prognostic factor after pancreaticoduodenectomy for pancreatic adenocarcinoma. Am. Surg. 2004, 70, 235. [Google Scholar]
- Showalter, T.N.; Winter, K.A.; Berger, A.C.; Regine, W.F.; Abrams, R.A.; Safran, H.; Hoffman, J.P.; Benson, A.B.; MacDonald, J.S.; Willett, C.G. The influence of total nodes examined, number of positive nodes, and lymph node ratio on survival after surgical resection and adjuvant chemoradiation for pancreatic cancer: A secondary analysis of RTOG 9704. Int. J. Radiat. Oncol. 2011, 81, 1328–1335. [Google Scholar] [CrossRef] [Green Version]
- Basturk, O.; Saka, B.; Balci, S.; Postlewait, L.M.; Knight, J.; Goodman, M.; Kooby, D.; Sarmiento, J.M.; El-Rayes, B.; Choi, H.; et al. Substaging of lymph node status in resected pancreatic ductal adenocarcinoma has strong prognostic correlations: Proposal for a revised N classification for TNM staging. Ann. Surg. Oncol. 2015, 22, 1187–1195. [Google Scholar] [CrossRef]
- Fukuda, Y.; Asaoka, T.; Maeda, S.; Hama, N.; Miyamoto, A.; Mori, M.; Doki, Y.; Nakamori, S. Prognostic impact of nodal statuses in patients with pancreatic ductal adenocarcinoma. Pancreatology 2017, 17, 279–284. [Google Scholar] [CrossRef] [PubMed]
- Konstantinidis, I.T.; Deshpande, V.; Zheng, H.; Wargo, J.A.; Fernandez-del Castillo, C.; Thayer, S.P.; Androutsopoulos, V.; Lauwers, G.Y.; Warshaw, A.L.; Ferrone, C.R. Does the mechanism of lymph node invasion affect survival in patients with pancreatic ductal adenocarcinoma? J. Gastrointest. Surg. 2010, 14, 261–267. [Google Scholar] [CrossRef]
- Pai, R.K.; Beck, A.H.; Mitchem, J.; Linehan, D.C.; Chang, D.T.; Norton, J.A.; Pai, R.K. Pattern of lymph node involvement and prognosis in pancreatic adenocarcinoma: Direct lymph node invasion has similar survival to node-negative disease. Am. J. Surg. Pathol. 2011, 35, 228–234. [Google Scholar] [CrossRef] [PubMed]
- Buc, E.; Couvelard, A.; Kwiatkowski, F.; Dokmak, S.; Ruszniewski, P.; Hammel, P.; Belghiti, J.; Sauvanet, A. Adenocarcinoma of the pancreas: Does prognosis depend on mode of lymph node invasion? Eur. J. Surg. Oncol. 2014, 40, 1578–1585. [Google Scholar] [CrossRef] [PubMed]
- Williams, J.L.; Nguyen, A.H.; Rochefort, M.; Muthusamy, V.R.; Wainberg, Z.A.; Dawson, D.W.; Tomlinson, J.S.; Hines, O.J.; Reber, H.A.; Donahue, T.R. Pancreatic cancer patients with lymph node involvement by direct tumor extension have similar survival to those with node-negative disease. J. Surg. Oncol. 2015, 112, 396–402. [Google Scholar] [CrossRef]
- Hoshikawa, M.; Ogata, S.; Nishikawa, M.; Kimura, A.; Einama, T.; Noro, T.; Aosasa, S.; Hase, K.; Tsujimoto, H.; Ueno, H.; et al. Pathomorphological features of metastatic lymph nodes as predictors of postoperative prognosis in pancreatic cancer. Medicine 2019, 98, e14369. [Google Scholar] [CrossRef] [PubMed]
- Byun, Y.; Lee, K.-B.; Jang, J.-Y.; Han, Y.; Choi, Y.J.; Kang, J.S.; Kim, H.; Kwon, W. Peritumoral lymph nodes in pancreatic cancer revisited; is it truly equivalent to lymph node metastasis? J. Hepatobiliary Pancreat. Sci. 2021, 28, 893–901. [Google Scholar] [CrossRef]
- Argentiero, A.; De Summa, S.; Di Fonte, R.; Iacobazzi, R.M.; Porcelli, L.; Da Vià, M.; Brunetti, O.; Azzariti, A.; Silvestris, N.; Solimando, A.G. Gene expression comparison between the lymph node-positive and-negative reveals a peculiar immune microenvironment signature and a theranostic role for WNT targeting in pancreatic ductal adenocarcinoma: A pilot study. Cancers 2019, 11, 942. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Solimando, A.G.; De Summa, S.; Vacca, A.; Ribatti, D. Cancer-Associated angiogenesis: The endothelial cell as a checkpoint for immunological patrolling. Cancers 2020, 12, 3380. [Google Scholar] [CrossRef] [PubMed]
- Ueno, M.; Morizane, C.; Ikeda, M.; Okusaka, T.; Ishii, H.; Furuse, J. A review of changes to and clinical implications of the eighth TNM classification of hepatobiliary and pancreatic cancers. Jpn. J. Clin. Oncol. 2019, 49, 1073–1082. [Google Scholar] [CrossRef] [PubMed]
- Roalsø, M.; Aunan, J.R.; Søreide, K. Refined TNM-staging for pancreatic adenocarcinoma-Real progress or much ado about nothing? Eur. J. Surg. Oncol. 2020, 46, 1554–1557. [Google Scholar] [CrossRef] [Green Version]
- Morales-Oyarvide, V.; Rubinson, D.A.; Dunne, R.F.; Kozak, M.M.; Bui, J.L.; Yuan, C.; Qian, Z.R.; Babic, A.; Da Silva, A.; Nowak, J.A.; et al. Lymph node metastases in resected pancreatic ductal adenocarcinoma: Predictors of disease recurrence and survival. Br. J. Cancer 2017, 117, 1874–1882. [Google Scholar] [CrossRef]
- Allen, P.J.; Kuk, D.; Castillo, C.F.-D.; Basturk, O.; Wolfgang, C.L.; Cameron, J.L.; Lillemoe, K.D.; Ferrone, C.R.; Morales-Oyarvide, V.; He, J.; et al. Multi-institutional validation study of the american joint commission on cancer (8th Edition) changes for T and N staging in patients with pancreatic adenocarcinoma. Ann. Surg. 2017, 265, 185–191. [Google Scholar] [CrossRef] [Green Version]
- van Roessel, S.; Kasumova, G.G.; Verheij, J.; Najarian, R.M.; Maggino, L.; de Pastena, M.; Malleo, G.; Marchegiani, G.; Salvia, R.; Ng, S.C.; et al. International validation of the eighth edition of the American joint committee on cancer (AJCC) TNM staging system in patients with resected pancreatic cancer. JAMA Surg. 2018, 153, e183617. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6583013/ (accessed on 23 June 2021). [CrossRef]
- Slidell, M.B.; Chang, D.C.; Cameron, J.L.; Wolfgang, C.; Herman, J.M.; Schulick, R.D.; Choti, M.A.; Pawlik, T.M. Impact of total lymph node count and lymph node ratio on staging and survival after pancreatectomy for pancreatic adenocarcinoma: A large, population-based analysis. Ann. Surg. Oncol. 2007, 15, 165–174. [Google Scholar] [CrossRef]
- Hartwig, W.; Hackert, T.; Hinz, U.; Gluth, A.; Bergmann, F.; Strobel, O.; Büchler, M.W.; Werner, J. Pancreatic cancer surgery in the new millennium: Better prediction of outcome. Ann. Surg. 2011, 254, 311–319. [Google Scholar] [CrossRef] [Green Version]
- Pyo, J.-S.; Kim, N.Y.; Son, B.K.; Chung, K.H. Prognostic implication of pN stage subdivision using metastatic lymph node ratio in resected pancreatic ductal adenocarcinoma. Int. J. Surg. Pathol. 2020, 28, 245–251. [Google Scholar] [CrossRef] [PubMed]
- House, M.G.; Gönen, M.; Jarnagin, W.R.; D’Angelica, M.; DeMatteo, R.P.; Fong, Y.; Brennan, M.F.; Allen, P.J. Prognostic significance of pathologic nodal status in patients with resected pancreatic cancer. J. Gastrointest. Surg. 2007, 11, 1549–1555. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| N0 (n = 37) | Nc (n = 20) | Nm (n = 44) | Ncm (n = 21) | Total (n = 122) | p-Value | ||
|---|---|---|---|---|---|---|---|
| Median Age (range) | 70.3 (35.4–84.4) | 70.3 (52.6–83) | 71.6 (36.8–84.5) | 69.2 (41.8–86.7) | 70.3 (35.4–86.7) | 0.402 | |
| Gender | 0.459 | ||||||
| female | 20 | 10 | 19 | 7 | 56 (45.9) | ||
| male | 17 | 10 | 25 | 14 | 66 (54.1) | ||
| T stage | 0.693 | ||||||
| T1 | 4 | 1 | 2 | 2 | 9 (7.4) | ||
| T2 | 13 | 10 | 24 | 9 | 56 (45.9) | ||
| T3 | 20 | 9 | 18 | 10 | 57 (46.7) | ||
| T4 | 0 | 0 | 0 | 0 | 0 | ||
| N stage | <0.001 | ||||||
| N0 | 37 | 0 | 0 | 0 | 37 (30.3) | ||
| N1 | 0 | 20 | 27 | 7 | 54 (44.3) | ||
| N2 | 0 | 0 | 17 | 14 | 31 (25.4) | ||
| Resection | 0.340 | ||||||
| R0 | 29 | 18 | 35 | 14 | 96 (78.7) | ||
| R1 | 8 | 2 | 9 | 7 | 26 (21.3) | ||
| Grade | 0.090 | ||||||
| G1 | 5 | 0 | 0 | 0 | 5 (4.1) | ||
| G2 | 20 | 11 | 21 | 11 | 63 (51.6) | ||
| G3 | 12 | 9 | 22 | 10 | 53 (43.4) | ||
| G4 | 0 | 0 | 1 | 0 | 1 (0.8) | ||
| Location | 0.035 | ||||||
| head | 24 | 17 | 41 | 19 | 101 (82.8) | ||
| corpus | 3 | 1 | 0 | 1 | 5 (4.1) | ||
| tail | 10 | 2 | 3 | 1 | 16 (13.1) | ||
| Invasion | |||||||
| ALI | 1 | 8 | 28 | 14 | 51 (41.8) | <0.001 | |
| VNI | 3 | 6 | 9 | 7 | 25 (20.5) | 0.115 | |
| PNI | 17 | 14 | 31 | 16 | 78 (63.9) | 0.486 |
| Univariate | Multivariate | |||||
|---|---|---|---|---|---|---|
| HR | CI 95% | p-Value | HR | CI 95% | p–Value | |
| age (<65/>65 years) | 01.217 | 0.708–2.091 | 0.478 | |||
| sex (male/female) | 0.671 | 0.411–1.097 | 0.112 | |||
| T stage (T1/T3) | 1.539 | 0.645–3.674 | 0.331 | |||
| resection (R0/R1) | 2.706 | 1.507–4.859 | 0.001 | 1.627 | 0.838–3.160 | 0.151 |
| grade (G2/G3) | 1.481 | 0.901–2.435 | 0.121 | |||
| PNI (no/yes) | 2.250 | 0.891–5.683 | 0.86 | |||
| VI (no/yes) | 2.387 | 1.336–4.266 | 0.003 | 2.504 | 1.384–4.515 | 0.002 |
| ALI (no/yes) | 2.378 | 1.420–3.983 | 0.001 | 1.6 | 0.861–2.973 | 0.137 |
| LNR (>0-<0.2/≥0.4) | 2.138 | 0.910–5.024 | 0.081 | |||
| Mechanism of lymph node invasion | ||||||
| Nc (no/yes) | 0.952 | 0.484–1.869 | 0.885 | |||
| N0-R(N0 + Nc)/Nm + Ncm | 2.567 | 1.511–4.359 | <0.001 | 3.024 | 1.709–5.352 | <0.001 |
| Total | N0 | Nc | Nm | Ncm | |||||
|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | ||
| Konstantinidis et al. 2010 | 336 | 168 | 50.0% | 32 | 9.5% | 131 | 39.0% | 5 | 1.5% |
| Pai et al. 2011 | 380 | 97 | 25.5% | 35 | 9.2% | 239 | 62.9% | 9 | 2.4% |
| Buc et al. 2014 | 301 | 87 | 28.9% | 19 | 6.3% | 179 | 59.5% | 16 | 5.3% |
| Williams et al. 2015 | 385 | 146 | 37.9% | 14 | 3.6% | 220 | 57.1% | 5 | 1.3% |
| Hoshikawa et al. 2019 | 98 | 10 | 10.2% | 14 | 14.3% | 66 | 67.3% | x | x |
| Byun et al. 2021 | 506 | 176 | 34.8% | 48 | 9.5% | 218 | 43.1% | 64 | 12.6% |
| Current study 2021 | 122 | 37 | 30.3% | 20 | 16.4% | 44 | 36.1% | 21 | 17.2% |
| N0 | Nc | Nm | Ncm | |||||
|---|---|---|---|---|---|---|---|---|
| n | OS Median | n | OS Median | n | OS Median | n | OS Median | |
| Konstantinidis et al. 2010 | 168 | 30.8 | 32 | x | 131 | x | 5 | x |
| Pai et al. 2011 | 97 | 30 | 35 | 21 * | 239 | 15 ** | 9 | 15 |
| Buc et al. 2014 | 87 | 57 | 19 | 34 ** | 179 | 33 ** | 16 | 22 |
| Williams et al. 2015 | 146 | 40.7 | 14 | 48.1 | 220 | 25.7 ** | 5 | x |
| Current study 2021 | 37 | x | 20 | 13.5 | 44 | 18.2 ** | 21 | 9.2 ** |
| Total | 535 | 120 | 813 | 56 | ||||
| Weighted Median OS | 30.8 | 21 | 25.7 | 15 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Speichinger, F.; Dragomir, M.P.; Schallenberg, S.; Loch, F.N.; Degro, C.E.; Baukloh, A.-K.; Hartmann, L.; Pozios, I.; Schineis, C.; Margonis, G.A.; et al. Rethinking the TNM Classification Regarding Direct Lymph Node Invasion in Pancreatic Ductal Adenocarcinoma. Cancers 2022, 14, 201. https://doi.org/10.3390/cancers14010201
Speichinger F, Dragomir MP, Schallenberg S, Loch FN, Degro CE, Baukloh A-K, Hartmann L, Pozios I, Schineis C, Margonis GA, et al. Rethinking the TNM Classification Regarding Direct Lymph Node Invasion in Pancreatic Ductal Adenocarcinoma. Cancers. 2022; 14(1):201. https://doi.org/10.3390/cancers14010201
Chicago/Turabian StyleSpeichinger, Fiona, Mihnea P. Dragomir, Simon Schallenberg, Florian N. Loch, Claudius E. Degro, Ann-Kathrin Baukloh, Lisa Hartmann, Ioannis Pozios, Christian Schineis, Georgios Antonios Margonis, and et al. 2022. "Rethinking the TNM Classification Regarding Direct Lymph Node Invasion in Pancreatic Ductal Adenocarcinoma" Cancers 14, no. 1: 201. https://doi.org/10.3390/cancers14010201