
Prognostic Impact of AHNAK2 Expression in Patients Treated with Radical Cystectomy

 , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Results
2.1. Tissues Immunostained for AHNAK2
2.2. Patient Characteristics
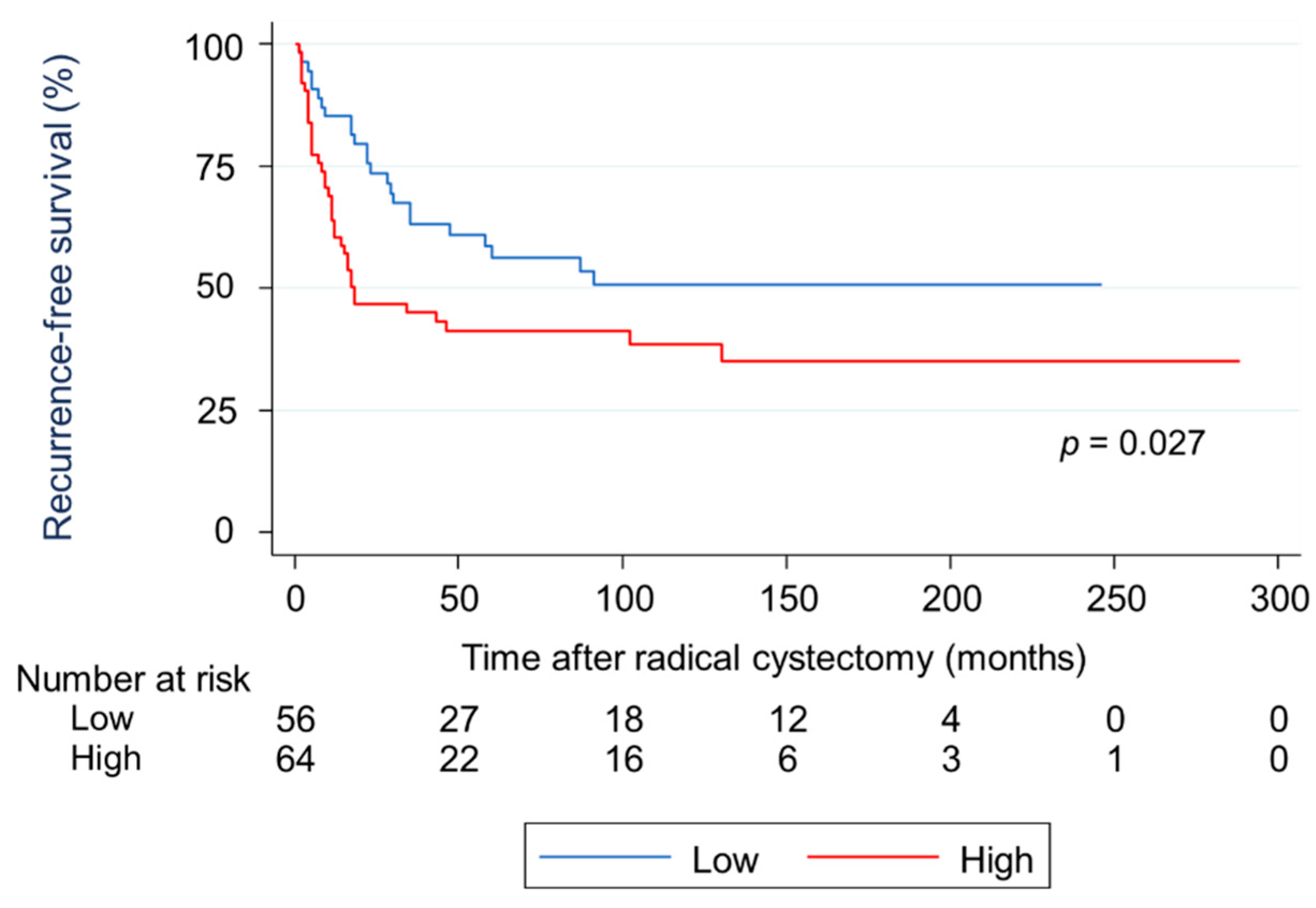
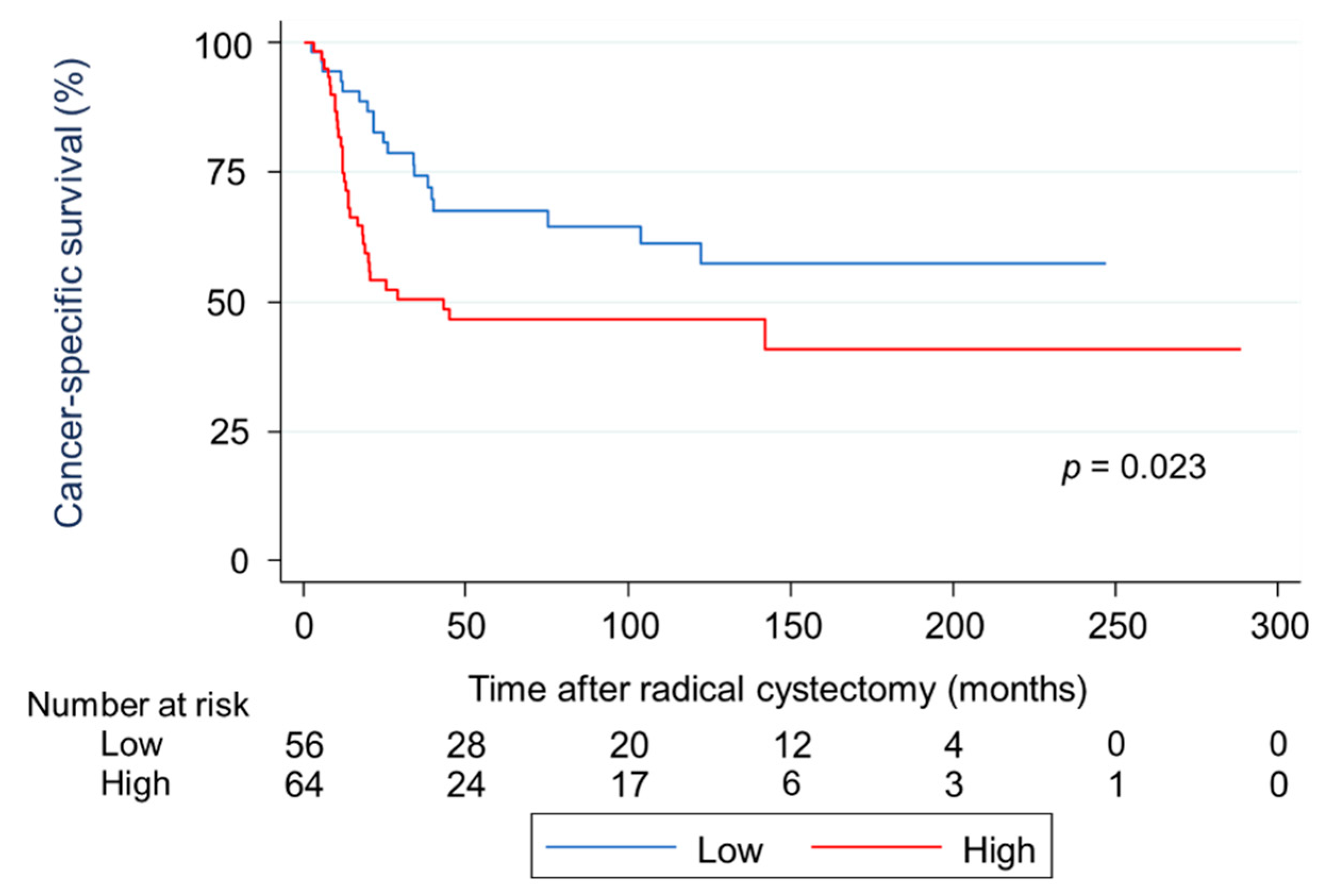
2.3. Survival Analysis Using Kaplan-Meier Methods for RFS and CSS in Terms of Two Types of AHNAK2 Expression
2.4. Univariate and Multivariate Analyses of Prognostic Factors for RFS and CSS
2.5. Subgroup Analysis of Associations between AHNAK2 and Some Proteins
3. Discussion
4. Materials and Methods
4.1. Patient Population
4.2. Patient Characteristics
4.3. Immunohistochemistry and Scoring
4.4. Subgroup Analysis of Associations between AHNAK2 and Some Proteins
4.5. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.; Ma, J.; Zou, Z.; Jemal, A. Cancer Statistics. CA Cancer J. Clin. 2014, 64, 9–29. [Google Scholar] [CrossRef] [Green Version]
- Zehnder, P.; Studer, U.E.; Skinner, E.C.; Thalmann, G.N.; Miranda, G.; Roth, B.; Cai, J.; Birkhäuser, F.D.; Mitra, A.P.; Burkhard, F.C.; et al. Oncological Outcomes of Radical Cystectomy over Three Decades. Bju Int. 2013, 112, 51–58. [Google Scholar] [CrossRef] [Green Version]
- Stein, J.P.; Skinner, D.G. Radical Cystectomy for Invasive Bladder Cancer: Long-Term Results of a Standard Procedure. World J. Urol. 2006, 24, 296–304. [Google Scholar] [CrossRef]
- Mitra, A.P.; Quinn, D.I.; Dorff, T.B.; Skinner, E.C.; Schuckman, A.K.; Miranda, G.; Gill, I.S.; Daneshmand, S. Factors Influencing Post-Recurrence Survival in Bladder Cancer Following Radical Cystectomy. BJU Int. 2012, 109, 846–854. [Google Scholar] [CrossRef]
- Witjes, J.A.; Lebret, T.; Compérat, E.M.; Cowan, N.C.; Santis, M.D.; Bruins, H.M.; Hernández, V.; Espinós, E.L.; Dunn, J.; Rouanne, M.; et al. Updated 2016 EAU Guidelines on Muscle-Invasive and Metastatic Bladder Cancer. Eur. Urol. 2017, 71, 462–475. [Google Scholar] [CrossRef]
- Seiler, R.; Ashab, H.A.D.; Erho, N.; van Rhijn, B.W.G.; Winters, B.; Douglas, J.; Kessel, K.E.V.; van de Putte, E.E.F.; Sommerlad, M.; Wang, N.Q.; et al. Impact of Molecular Subtypes in Muscle-Invasive Bladder Cancer on Predicting Response and Survival after Neoadjuvant Chemotherapy. Eur. Urol. 2017, 72, 544–554. [Google Scholar] [CrossRef] [PubMed]
- Zargar, H.; Espiritu, P.N.; Fairey, A.S.; Mertens, L.S.; Dinney, C.P.; Mir, M.C.; Krabbe, L.-M.; Cookson, M.S.; Jacobsen, N.-E.; Gandhi, N.M.; et al. Multicenter Assessment of Neoadjuvant Chemotherapy for Muscle-Invasive Bladder Cancer. Eur. Urol. 2015, 67, 241–249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosa, M. Advances in the Molecular Analysis of Breast Cancer: Pathway toward Personalized Medicine. Cancer Control 2015, 22, 211–219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Komuro, A.; Masuda, Y.; Kobayashi, K.; Babbitt, R.; Gunel, M.; Flavell, R.A.; Vincent, T.M. The AHNAKs are a Class of Giant Propeller-like Proteins that Associate with Calcium Channel Proteins of Cardiomyocytes and Other Cells. Proc. Natl. Acad. Sci. USA 2004, 102, 4053–4058. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, M.; Li, X.; Zhang, J.; Yang, Q.; Chen, W.; Jin, W.; Huang, Y.-R.; Yang, R.; Gao, W.-Q. AHNAK2 is a Novel Prognostic Marker and Oncogenic Protein for Clear Cell Renal Cell Carcinoma. Theranostics 2017, 7, 1100–1113. [Google Scholar] [CrossRef]
- Lu, D.; Wang, J.; Shi, X.; Yue, B.; Hao, J. AHNAK2 is a Potential Prognostic Biomarker in Patients with PDAC. Oncotarget 2014, 5, 31775–31784. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, M.; Liu, Y.; Meng, Y.; Zhu, Y. AHNAK Nucleoprotein 2 Performs a Promoting Role in the Proliferation and Migration of Uveal Melanoma Cells. Cancer Biother. Radiopharm. 2019, 34, 626–633. [Google Scholar] [CrossRef] [PubMed]
- Xie, Z.; Lun, Y.; Li, X.; He, Y.; Wu, S.; Wang, S.; Sun, J.; He, Y.; Zhang, J. Bioinformatics Analysis of the Clinical Value and Potential Mechanisms of AHNAK2 in Papillary Thyroid Carcinoma. Aging 2020, 12, 18163–18180. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Lu, Y.; Qi, L.; Wang, H.; Wang, Z.; Cai, Z. AHNAK2 is Associated with Poor Prognosis and Cell Migration in Lung Adenocarcinoma. BioMed Res. Int. 2020, 2020, 8571932. [Google Scholar] [CrossRef]
- Wang, D.-W.; Zheng, H.-Z.; Cha, N.; Zhang, X.-J.; Zheng, M.; Chen, M.-M.; Tian, L.-X. Down-Regulation of AHNAK2 Inhibits Cell Proliferation, Migration and Invasion Through Inactivating the MAPK Pathway in Lung Adenocarcinoma. Technol. Cancer Res. Treatment 2020, 19, 153303382095700. [Google Scholar] [CrossRef] [PubMed]
- Liu, G.; Guo, Z.; Zhang, Q.; Liu, Z.; Zhu, D. AHNAK2 Promotes Migration, Invasion, and Epithelial-Mesenchymal Transition in Lung Adenocarcinoma Cells via the TGF-β/Smad3 Pathway. Oncotargets Ther. 2020, 13, 12893–12903. [Google Scholar] [CrossRef]
- Okusa, H.; Kodera, Y.; Oh-Ishi, M.; Minamida, Y.; Tsuchida, M.; Kavoussi, N.; Matsumoto, K.; Sato, T.; Iwamura, M.; Maeda, T.; et al. Searching for New Biomarkers of Bladder Cancer Based on Proteomic Analysis. J. Electrophor. 2008, 52, 19–24. [Google Scholar] [CrossRef] [Green Version]
- Witzke, K.E.; Großerueschkamp, F.; Jütte, H.; Horn, M.; Roghmann, F.; von Landenberg, N.; Bracht, T.; Kallenbach-Thieltges, A.; Käfferlein, H.; Brüning, T.; et al. Integrated Fourier Transform Infrared Imaging and Proteomics for Identification of a Candidate Histochemical Biomarker in Bladder Cancer. Am. J. Pathol. 2019, 189, 619–631. [Google Scholar] [CrossRef] [Green Version]
- Luo, Y.; Zeng, G.; Wu, S. Identification of Microenvironment-Related Prognostic Genes in Bladder Cancer Based on Gene Expression Profile. Front. Genet. 2019, 10, 1187. [Google Scholar] [CrossRef] [Green Version]
- Chen, Z.; He, S.; Zhan, Y.; He, A.; Fang, D.; Gong, Y.; Li, X.; Zhou, L. TGF-β-Induced Transgelin Promotes Bladder Cancer Metastasis by Regulating Epithelial-Mesenchymal Transition and Invadopodia Formation. EBioMedicine 2019, 47, 208–220. [Google Scholar] [CrossRef] [Green Version]
- Al-Ismaeel, Q.; Neal, C.P.; Al-Mahmoodi, H.; Almutairi, Z.; Al-Shamarti, I.; Straatman, K.; Jaunbocus, N.; Irvine, A.; Issa, E.; Moreman, C.; et al. ZEB1 and IL-6/11-STAT3 Signalling Cooperate to Define Invasive Potential of Pancreatic Cancer Cells via Differential Regulation of the Expression of S100 Proteins. Br. J. Cancer 2019, 121, 65–75. [Google Scholar] [CrossRef]
- Scholtes, M.; Akbarzadeh, M.; Zwarthoff, E.; Boormans, J.; Mahmoudi, T.; Zuiverloon, T. Targeted Therapy in Metastatic Bladder Cancer: Present Status and Future Directions. Appl. Sci. 2020, 10, 7102. [Google Scholar] [CrossRef]
- Sluzalska, K.D.; Slawski, J.; Sochacka, M.; Lampart, A.; Otlewski, J.; Zakrzewska, M. Intracellular Partners of Fibroblast Growth Factors 1 and 2—Implications for Functions. Cytokine Growth Facor Rev. 2020, 57, 93–111. [Google Scholar] [CrossRef] [PubMed]
- Kwon, C.H.; Moon, H.J.; Park, H.J.; Choi, J.H.; Park, D.Y. S100A8 and S100A9 Promotes Invasion and Migration through P38 Mitogen-Activated Protein Kinase-Dependent NF-ΚB Activation in Gastric Cancer Cells. Mol. Cell 2013, 35, 226–234. [Google Scholar] [CrossRef] [Green Version]
- Kirov, A.; Kacer, D.; Conley, B.A.; Vary, C.P.H.; Prudovsky, I. AHNAK2 Participates in the Stress-Induced Nonclassical FGF1 Secretion Pathway. J. Cell Biochem. 2015, 116, 1522–1531. [Google Scholar] [CrossRef] [Green Version]
- Eckerdt, F.D.; Bell, J.B.; Gonzalez, C.; Oh, M.S.; Perez, R.E.; Mazewski, C.; Fischietti, M.; Goldman, S.; Nakano, I.; Platanias, L.C. Combined PI3Kα-MTOR Targeting of Glioma Stem Cells. Sci. Rep. 2020, 10, 21873. [Google Scholar] [CrossRef]
- Ashrafizadeh, M.; Zarrabi, A.; Hushmandi, K.; Kalantari, M.; Mohammadinejad, R.; Javaheri, T.; Sethi, G. Association of the Epithelial–Mesenchymal Transition (EMT) with Cisplatin Resistance. Int. J. Mol. Sci. 2020, 21, 4002. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Y.; Zhan, H. Communication between EMT and PD-L1 Signaling: New Insights into Tumor Immune Evasion. Cancer Lett. 2019, 468, 72–81. [Google Scholar] [CrossRef]
- Wang, L.; Saci, A.; Szabo, P.M.; Chasalow, S.D.; Castillo-Martin, M.; Domingo-Domenech, J.; Siefker-Radtke, A.; Sharma, P.; Sfakianos, J.P.; Gong, Y.; et al. EMT- and Stroma-Related Gene Expression and Resistance to PD-1 Blockade in Urothelial Cancer. Nat. Commun. 2018, 9, 3503. [Google Scholar] [CrossRef]
- Matsumoto, K.; Ikeda, M.; Sato, Y.; Kuruma, H.; Kamata, Y.; Nishimori, T.; Tomonaga, T.; Nomura, F.; Egawa, S.; Iwamura, M. Loss of Periplakin Expression is Associated with Pathological Stage and Cancer-Specific Survival in Patients with Urothelial Carcinoma of the Urinary Bladder. BioMed Res. 2014, 35, 201–206. [Google Scholar] [CrossRef] [Green Version]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New Response Evaluation Criteria in Solid Tumours: Revised RECIST Guideline (Version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]
- Amano, N.; Matsumoto, K.; Shimizu, Y.; Nakamura, M.; Tsumura, H.; Ishii, D.; Sato, Y.; Iwamura, M. High HNRNPA3 Expression is Associated with Lymph Node Metastasis and Poor Prognosis in Patients Treated with Radical Cystectomy. Urol. Oncol. Semin. Orig. Investig. 2020, 39, 196. [Google Scholar] [CrossRef]
- Matsumoto, K.; Irie, A.; Satoh, T.; Ishii, J.; Iwabuchi, K.; Iwamura, M.; Egawa, S.; Baba, S. Expression of S100A2 and S100A4 Predicts for Disease Progression and Patient Survival in Bladder Cancer. Urology 2007, 70, 602–607. [Google Scholar] [CrossRef] [PubMed]
- Minami, S.; Sato, Y.; Matsumoto, T.; Kageyama, T.; Kawashima, Y.; Yoshio, K.; Ishii, J.-I.; Matsumoto, K.; Nagashio, R.; Okayasu, I. Proteomic Study of Sera from Patients with Bladder Cancer: Usefulness of S100A8 and S100A9 Proteins. Cancer Genom. Proteom. 2010, 7, 181–189. [Google Scholar]
- Tabata, K.; Matsumoto, K.; Minami, S.; Ishii, D.; Nishi, M.; Fujita, T.; Saegusa, M.; Sato, Y.; Iwamura, M. Nestin is an Independent Predictor of Cancer-Specific Survival after Radical Cystectomy in Patients with Urothelial Carcinoma of the Bladder. PLoS ONE 2014, 9, e91548. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| LE (n = 56) | HE (n = 64) | p-Value | |
|---|---|---|---|
| Age | |||
| ≤65 | 29 (51.8) | 33 (51.6) | 0.98 |
| >65 | 27 (48.2) | 31 (48.4) | |
| Sex | |||
| Male | 51 (91.1) | 46 (71.2) | 0.01 |
| Female | 5 (8.9) | 18 (28.8) | |
| T stage | |||
| pTa | 2 (3.6) | 0 | 0.047 |
| pTis | 2 (3.6) | 1 (1.6) | |
| pT1 | 11 (19.6) | 7 (10.9) | |
| pT2 | 18 (32.1) | 11 (17.2) | |
| pT3 | 16 (28.6) | 30 (46.9) | |
| pT4 | 7 (12.5) | 15 (23.4) | |
| N stage | |||
| pN0 | 45 (80.3) | 43 (67.2) | 0.027 |
| ≥pN1 | 10 (17.8) | 16 (25.0) | |
| Unknown | 1 (1.8) | 5 (7.8) | |
| Grade | |||
| G1/2 | 23 (41.1) | 23 (35.9) | 0.57 |
| G3 | 32 (57.1) | 41 (64.1) | |
| Unknown | 1 (1.8) | 0 | |
| LVI | |||
| Negative | 24 (42.9) | 15 (23.4) | 0.003 |
| Positive | 28 (50.0) | 43 (67.2) | |
| Unknown | 4 (7.1) | 6 (9.4) | |
| CIS | |||
| Negative | 49 (87.5) | 55 (85.9) | 0.97 |
| Positive | 7 (12.5) | 8 (12.5) | |
| Unknown | 0 | 1 (1.6) | |
| Adjuvant chemotherapy | |||
| Yes | 8 (14.3) | 12 (18.8) | 0.51 |
| No | 48 (85.7) | 52 (81.2) | |
| Salvage chemotherapy | |||
| Response | 2 (22.2) | 3 (27.3) | 0.80 |
| No Response | 7 (77.8) | 8 (72.7) | |
| Recurrence | |||
| Yes | 24 (42.9) | 37 (57.8) | 0.027 |
| No | 32 (57.1) | 27 (42.2) | |
| Cancer death | |||
| Yes | 19 (33.9) | 32 (50.0) | 0.023 |
| No | 37 (66.1) | 32 (50.0) | |
| Follow-up, months (IQR) | 51.0 (21–133) | 20.0 (11–98.5) | 0.075 |
| Variable | Category | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | ||
| AHNAK2 | HE | 1.78 | 1.02–2.98 | 0.027 | 1.96 | 1.08–3.53 | 0.026 |
| LE | 1.0 | 1.0 | |||||
| T stage | MIBC | 2.24 | 1.14–4.41 | 0.019 | 1.66 | 0.64–4.28 | 0.30 |
| NMIBC | 1.0 | 1.0 | |||||
| N stage | ≥pN1 | 2.86 | 1.67–4.89 | <0.001 | 2.04 | 1.09–3.84 | 0.026 |
| pN0 | 1.0 | 1.0 | |||||
| Grade | G3 | 1.47 | 0.83–2.60 | 0.18 | 1.12 | 0.55–2.27 | 0.75 |
| G1/2 | 1.0 | 1.0 | |||||
| LVI | Positive | 2.52 | 1.35–4.71 | 0.004 | 1.12 | 0.55–2.27 | 0.75 |
| Negative | 1.0 | 1.0 | |||||
| CIS | Positive | 0.64 | 0.29–1.41 | 0.27 | 1.16 | 0.48–2.84 | 0.73 |
| Negative | 1.0 | 1.0 | |||||
| Variable | Category | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | ||
| AHNAK2 | HE | 1.91 | 1.08–3.38 | 0.023 | 2.22 | 1.14–4.31 | 0.019 |
| LE | 1.0 | 1.0 | |||||
| T stage | MIBC | 2.01 | 0.98–4.13 | 0.057 | 1.44 | 0.50–4.11 | 0.68 |
| NMIBC | 1.0 | 1.0 | |||||
| N stage | ≥pN1 | 3.03 | 1.69–5.45 | <0.001 | 1.19 | 1.25–4.97 | 0.009 |
| pN0 | 1.0 | 1.0 | |||||
| Grade | G3 | 1.65 | 0.87–3.15 | 0.13 | 1.17 | 0.54–2.56 | 0.69 |
| G1/2 | 1.0 | 1.0 | |||||
| LVI | Positive | 2.43 | 1.23–4.80 | 0.01 | 1.19 | 0.53–2.64 | 0.68 |
| Negative | 1.0 | 1.0 | |||||
| CIS | Positive | 0.42 | 0.15–1.18 | 0.101 | 0.57 | 0.17–1.91 | 0.37 |
| Negative | 1.0 | 1.0 | |||||
| Protein | LE (n = 56) | HE (n = 64) | p-Value |
|---|---|---|---|
| S100A2 | |||
| Normal | 16 (28.6) | 12 (18.8) | 0.15 |
| Abnormal | 19 (33.9) | 31 (48.4) | |
| S100A4 | |||
| Normal | 22 (39.3) | 15 (23.4) | 0.022 |
| Abnormal | 13 (23.2) | 28 (43.8) | |
| S100A8 | |||
| Normal | 24 (42.9) | 20 (31.1) | 0.015 |
| Abnormal | 7 (12.5) | 22 (34.4) | |
| S100A9 | |||
| Normal | 28 (50) | 20 (31.1) | <0.001 |
| Abnormal | 3 (5.4) | 22 (34.4) | |
| Nestin | |||
| Negative | 36 (64.3) | 35 (54.6) | 0.005 |
| Positive | 1 (1.8) | 12 (18.8) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koguchi, D.; Matsumoto, K.; Shimizu, Y.; Kobayashi, M.; Hirano, S.; Ikeda, M.; Sato, Y.; Iwamura, M. Prognostic Impact of AHNAK2 Expression in Patients Treated with Radical Cystectomy. Cancers 2021, 13, 1748. https://doi.org/10.3390/cancers13081748
Koguchi D, Matsumoto K, Shimizu Y, Kobayashi M, Hirano S, Ikeda M, Sato Y, Iwamura M. Prognostic Impact of AHNAK2 Expression in Patients Treated with Radical Cystectomy. Cancers. 2021; 13(8):1748. https://doi.org/10.3390/cancers13081748
Chicago/Turabian StyleKoguchi, Dai, Kazumasa Matsumoto, Yuriko Shimizu, Momoko Kobayashi, Shuhei Hirano, Masaomi Ikeda, Yuichi Sato, and Masatsugu Iwamura. 2021. "Prognostic Impact of AHNAK2 Expression in Patients Treated with Radical Cystectomy" Cancers 13, no. 8: 1748. https://doi.org/10.3390/cancers13081748