
Role of Thermal Ablation in Colorectal Cancer Lung Metastases

 ,
,  , and
, and
Abstract
:Simple Summary
Abstract
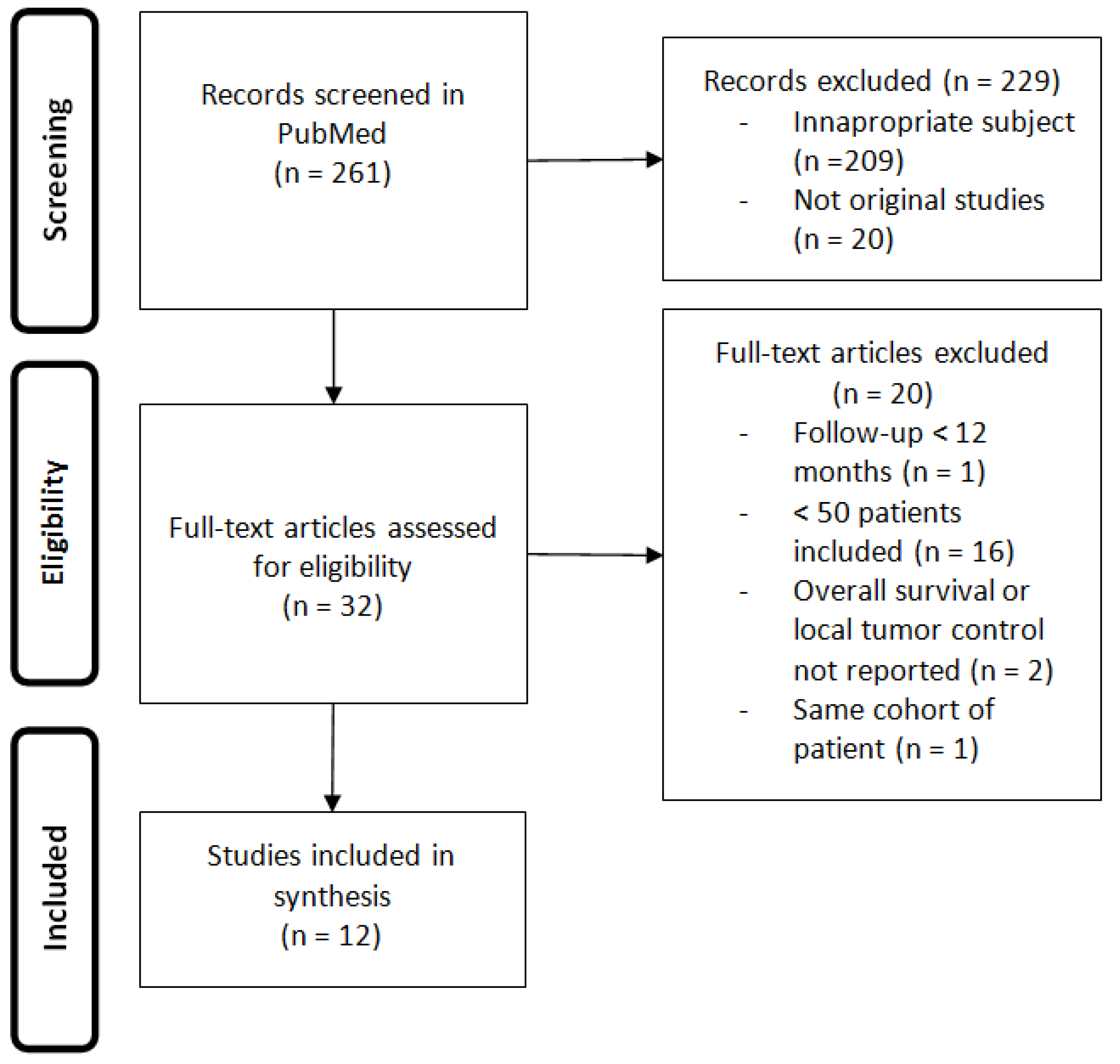
1. Introduction
2. Indications
3. Techniques
4. Oncological Outcomes
4.1. Local Control
4.2. Survival

{kind=link}
| Study | Type of Study | Technique | Number of Patients | Inclusion Dates | Mean Size of Lesions (cm) | Median Follow Up (Months) | LTC | LTP at 1 Year | LTP at 3 Years | Median OS (Months) | OS at 1 Year | OS at 3 Years | OS at 5 Years |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| T.D. Yan (2007) [30] | Retrospective | RFA | 55 | - | 2.1 +/− 1.1 | 24 | 62% | - | - | 33 | 85% | 46% | - |
| K. Yamakado (2009) [36] | Retrospective | RFA | 78 | 2002–2008 | 2.0 +/− 1.0 | 24 | 86% | 10% | 21% | 38 | 84% | 56% | 35% |
| T.C. Chua (2010) [37] | Retrospective | RFA | 100 | 2000–2010 | - | 23 | - | - | - | 36 | 87% | 50% | 30% |
| A. Gillams (2013) [38] | Retrospective | RFA | 122 | 2002–2011 | 1.7 (0.5–4) | 12 | - | - | - | 41 | - | 57% | - |
| T. de Baere (2015) [25] | Retrospective | RFA | 566 (293 mCCR) | 2002–2010 | 1.7 +/− 0.9 | 36 | 92% | 10% | 18% | 62 | 93% | 76% | 56% |
| J. Ferguson (2015) [31] | Retrospective | RFA | 157 | 2000–2013 | 1.6 +/− 0.6 | 28 | 88% | - | - | 33 | 89% | 44% | 20% |
| Y. Matsui (2015) [39] | Retrospective | RFA | 84 | 2001–2012 | 1.5 +/− 0.7 | 38 | 86% | 12% | 18% | 67 | 95% | 65% | 52% |
| I. Kurilova (2018) [32] | Retrospective | MWA | 50 | 2011–2016 | 1.0 (0.3–3.2) | 26 | 90% | 7% | 14% | 59 | 94% | 82% | 61% |
| M. Fonck (2018) [27] | Retrospective | RFA, MWA, CA | 209 | 2002–2013 | 1.0 (0.2–4.6) | 50 | - | - | - | 68 | 95% | - | 55% |
| J. Zhong (2019) [40] | Retrospective | RFA | 70 | 2008–2014 | 1.4 +/− 0.6 | 46 | 90% | 3% | 10% | 52 | 97% | 75% | 44% |
| M.R. Callstrom (2020) [26] | Prospective | CA | 128 (63 mCCR) | 2014–2016 | 1.0 +/− 0.6 | 91% | 9% | 16% | - | 98% | - | - | |
| T. Hasegawa (2020) [23] | Prospective | RFA | 70 | 2008–2014 | 1.0 +/− 0.5 | 57 | 91% | - | 9% | - | - | 84% | - |
4.3. Prognostic Factors
4.3.1. Local Control Factors
4.3.2. Survival Factors
4.3.3. Adverse Events
4.3.4. Overall
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Fedewa, S.A.; Ahnen, D.J.; Meester, R.G.S.; Barzi, A.; Jemal, A. Colorectal cancer statistics, 2017. CA A Cancer J. Clin. 2017, 67, 177–193. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, K.; Saito, N.; Sugito, M.; Ito, M.; Kobayashi, A.; Nishizawa, Y. Incidence and Predictive Factors for Pulmonary Metastases After Curative Resection of Colon Cancer. Ann. Surg. Oncol. 2013, 20, 1374–1380. [Google Scholar] [CrossRef] [PubMed]
- Desch, C.E.; Benson, A.B.; Somerfield, M.R.; Flynn, P.J.; Krause, C.; Loprinzi, C.L.; Minsky, B.D.; Pfister, D.G.; Virgo, K.S.; Petrelli, N.J. Colorectal Cancer Surveillance: 2005 Update of an American Society of Clinical Oncology Practice Guideline. J. Clin. Oncol. 2005, 23, 8512–8519. [Google Scholar] [CrossRef] [PubMed]
- Saito, Y.; Omiya, H.; Kohno, K.; Kobayashi, T.; Itoi, K.; Teramachi, M.; Sasaki, M.; Suzuki, H.; Takao, H.; Nakade, M. Pulmonary metastasectomy for 165 patients with colorectal carcinoma: A prognostic assessment. J. Thorac. Cardiovasc. Surg. 2002, 124, 1007–1013. [Google Scholar] [CrossRef] [Green Version]
- Nakajima, J.; Iida, T.; Okumura, S.; Horio, H.; Asamura, H.; Ozeki, Y.; Ikeda, N.; Matsuguma, H.; Chida, M.; Otsuka, H.; et al. Recent improvement of survival prognosis after pulmonary metastasectomy and advanced chemotherapy for patients with colorectal cancer. Eur. J. Cardio Thorac. Surg. 2017, 51, 869–873. [Google Scholar] [CrossRef]
- Ninomiya, M.; Nakajima, J.; Tanaka, M.; Takeuchi, E.; Murakawa, T.; Fukami, T.; Takamoto, S. Effects of lung metastasectomy on respiratory function. Jpn. J. Thorac. Cardiovasc. Surg. 2001, 49, 17–20. [Google Scholar] [CrossRef] [PubMed]
- Van Cutsem, E.; Cervantes, A.; Adam, R.; Sobrero, A.; Van Krieken, J.H.; Aderka, D.; Aguilar, E.A.; Bardelli, A.; Benson, A.; Bodoky, G.; et al. ESMO consensus guidelines for the management of patients with metastatic colorectal cancer. Ann. Oncol. 2016, 27, 1386–1422. [Google Scholar] [CrossRef] [PubMed]
- Pereira, P.L.; Salvatore, M. Standards of Practice: Guidelines for Thermal Ablation of Primary and Secondary Lung Tumors. Cardiovasc. Interv. Radiol. 2012, 35, 247–254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Detterbeck, F.C.; Grodzki, T.; Gleeson, F.; Robert, J.H. Imaging Requirements in the Practice of Pulmonary Metastasectomy. J. Thorac. Oncol. 2010, 5, S134–S139. [Google Scholar] [CrossRef] [PubMed]
- Bellier, J.; Perentes, J.Y.; Abdelnour-Berchtold, E.; Lopez, B.; Krueger, T.; Beigelman-Aubry, C.; Ris, H.-B.; Gonzalez, M. A plea for thoracoscopic resection of solitary pulmonary nodule in cancer patients. Surg. Endosc. 2017, 31, 4705–4710. [Google Scholar] [CrossRef] [PubMed]
- Tselikas, L.; De Baere, T.; Deschamps, F.; Hakimé, A.; Besse, B.; Teriitehau, C.; De Montpreville, V.; Adam, J. Diagnostic yield of a biopsy performed immediately after lung radiofrequency ablation. Eur. Radiol. 2017, 27, 1211–1217. [Google Scholar] [CrossRef]
- Amouyal, G.; Pernot, S.; Déan, C.; Cholley, B.; Scotté, F.; Sapoval, M.; Pellerin, O. Percutaneous radiofrequency ablation of lung metastases from colorectal carcinoma under C-arm cone beam CT guidance. Diagn. Interv. Imaging 2017, 98, 793–799. [Google Scholar] [CrossRef]
- Ahmed, M.; Liu, Z.; Afzal, K.S.; Weeks, D.; Lobo, S.M.; Kruskal, J.B.; Lenkinski, R.E.; Goldberg, S.N. Radiofrequency Ablation: Effect of Surrounding Tissue Composition on Coagulation Necrosis in a Canine Tumor Model. Radiology 2004, 230, 761–767. [Google Scholar] [CrossRef]
- Dupuy, D.E.; Zagoria, R.J.; Akerley, W.; Mayo-Smith, W.W.; Kavanagh, P.V.; Safran, H. Percutaneous Radiofrequency Ablation of Malignancies in the Lung. Am. J. Roentgenol. 2000, 174, 57–59. [Google Scholar] [CrossRef]
- Jaskolka, J.D.; Kachura, J.R.; Hwang, D.M.; Tsao, M.S.; Waddell, T.K.; Asch, M.R.; Darling, G.E.; Johnston, M.R. Pathologic Assessment of Radiofrequency Ablation of Pulmonary Metastases. J. Vasc. Interv. Radiol. 2010, 21, 1689–1696. [Google Scholar] [CrossRef] [PubMed]
- Steinke, K.; Haghighi, K.S.; Wulf, S.; Morris, D.L. Effect of vessel diameter on the creation of ovine lung radiofrequency lesions in vivo: Preliminary results. J. Surg. Res. 2005, 124, 85–91. [Google Scholar] [CrossRef]
- Prud’Homme, C.; Teriitehau, C.; Adam, J.; Tun, J.K.; Roux, C.; Hakime, A.; Delpla, A.; Deschamps, F.; De Baere, T.; Tselikas, L. Lung microwave ablation—An in vivo swine tumor model experiment to evaluate ablation zones. Int. J. Hyperth. 2020, 37, 879–886. [Google Scholar] [CrossRef] [PubMed]
- Ruiter, S.J.S.; Heerink, W.J.; De Jong, K.P. Liver microwave ablation: A systematic review of various FDA-approved systems. Eur. Radiol. 2019, 29, 4026–4035. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shady, W.; Petre, E.N.; Do, K.G.; Gonen, M.; Yarmohammadi, H.; Brown, K.T.; Kemeny, N.E.; D’Angelica, M.; Kingham, P.T.; Solomon, S.B.; et al. Percutaneous Microwave versus Radiofrequency Ablation of Colorectal Liver Metastases: Ablation with Clear Margins (A0) Provides the Best Local Tumor Control. J. Vasc. Interv. Radiol. 2018, 29, 268–275.e1. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, R.; Jakobs, T.; Lubienski, A.; Schrader, A.; Trumm, C.; Reiser, M.; Helmberger, T. Percutaneous radiofrequency ablation of pulmonary tumors—Is there a difference between treatment under general anaesthesia and under conscious sedation? Eur. J. Radiol. 2006, 59, 168–174. [Google Scholar] [CrossRef]
- De Baere, T.; Tselikas, L.; Woodrum, D.A.; Abtin, F.; Littrup, P.J.; Deschamps, F.; Suh, R.D.; Aoun, H.D.; Callstrom, M.R. Evaluating Cryoablation of Metastatic Lung Tumors in Patients—Safety and Efficacy The ECLIPSE Trial—Interim Analysis at 1 Year. J. Thorac. Oncol. 2015, 10, 1468–1474. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hinshaw, J.L.; Littrup, P.J.; Durick, N.; Leung, W.; Lee, F.T.; Sampson, L.; Brace, C.L. Optimizing the Protocol for Pulmonary Cryoablation: A Comparison of a Dual- and Triple-Freeze Protocol. Cardiovasc. Interv. Radiol. 2010, 33, 1180–1185. [Google Scholar] [CrossRef] [Green Version]
- Hasegawa, T.; Takaki, H.; Kodama, H.; Yamanaka, T.; Nakatsuka, A.; Sato, Y.; Takao, M.; Katayama, Y.; Fukai, I.; Kato, T.; et al. Three-year Survival Rate after Radiofrequency Ablation for Surgically Resectable Colorectal Lung Metastases: A Prospective Multicenter Study. Radiology 2020, 294, 686–695. [Google Scholar] [CrossRef]
- Hiraki, T.; Mimura, H.; Gobara, H.; Sano, Y.; Fujiwara, H.; Date, H.; Kanazawa, S. Repeat Radiofrequency Ablation for Local Progression of Lung Tumors: Does It Have a Role in Local Tumor Control? J. Vasc. Interv. Radiol. 2008, 19, 706–711. [Google Scholar] [CrossRef] [PubMed]
- De Baère, T.; Aupérin, A.; Deschamps, F.; Chevallier, P.; Gaubert, Y.; Boige, V.; Fonck, M.; Escudier, B.; Palussiére, J. Radiofrequency ablation is a valid treatment option for lung metastases: Experience in 566 patients with 1037 metastases. Ann. Oncol. 2015, 26, 987–991. [Google Scholar] [CrossRef]
- Callstrom, M.R.; Woodrum, D.A.; Nichols, F.C.; Palussiere, J.; Buy, X.; Suh, R.D.; Abtin, F.G.; Pua, B.B.; Madoff, D.C.; Bagla, S.L.; et al. Multicenter Study of Metastatic Lung Tumors Targeted by Interventional Cryoablation Evaluation (SOLSTICE). J. Thorac. Oncol. 2020, 15, 1200–1209. [Google Scholar] [CrossRef] [PubMed]
- Fonck, M.; Perez, J.-T.; Catena, V.; Becouarn, Y.; Cany, L.; Brudieux, E.; Vayre, L.; Texereau, P.; Le Brun-Ly, V.; Verger, V.; et al. Pulmonary Thermal Ablation Enables Long Chemotherapy-Free Survival in Metastatic Colorectal Cancer Patients. Cardiovasc. Interv. Radiol. 2018, 41, 1727–1734. [Google Scholar] [CrossRef] [PubMed]
- Embún, R.; Fiorentino, F.; Treasure, T.; Rivas, J.J.; Molins, L. Pulmonary metastasectomy in colorectal cancer: A prospective study of demography and clinical characteristics of 543 patients in the Spanish colorectal metastasectomy registry (GECMP-CCR). BMJ Open 2013, 3. [Google Scholar] [CrossRef] [Green Version]
- Cao, C.; Wang, D.; Tian, D.H.; Wilson-Smith, A.; Huang, J.; Rimner, A. A systematic review and meta-analysis of stereotactic body radiation therapy for colorectal pulmonary metastases. J. Thorac. Dis. 2019, 11, 5187–5198. [Google Scholar] [CrossRef]
- Yan, T.D.; King, J.; Sjarif, A.; Glenn, D.; Steinke, K.; Al-Kindy, A.; Morris, D.L. Treatment Failure After Percutaneous Radiofrequency Ablation for Nonsurgical Candidates With Pulmonary Metastases From Colorectal Carcinoma. Ann. Surg. Oncol. 2007, 14, 1718–1726. [Google Scholar] [CrossRef]
- Ferguson, J.; Alzahrani, N.; Zhao, J.; Glenn, D.; Power, M.; Liauw, W.; Morris, D. Long term results of RFA to lung metastases from colorectal cancer in 157 patients. Eur. J. Surg. Oncol. EJSO 2015, 41, 690–695. [Google Scholar] [CrossRef] [PubMed]
- Kurilova, I.; Gonzalez-Aguirre, A.; Beets-Tan, R.G.; Erinjeri, J.; Petre, E.N.; Gonen, M.; Bains, M.; Kemeny, N.E.; Solomon, S.B.; Sofocleous, C.T. Microwave Ablation in the Management of Colorectal Cancer Pulmonary Metastases. Cardiovasc. Interv. Radiol. 2018, 41, 1530–1544. [Google Scholar] [CrossRef]
- Pagès, P.-B.; Le Pimpec-Barthes, F.; Bernard, A. Chirurgie des métastases pulmonaires des cancers colorectaux: Facteurs prédictifs de survie. Rev. Mal. Respir. 2016, 33, 838–852. [Google Scholar] [CrossRef] [PubMed]
- Iida, T.; Nomori, H.; Shiba, M.; Nakajima, J.; Okumura, S.; Horio, H.; Matsuguma, H.; Ikeda, N.; Yoshino, I.; Ozeki, Y.; et al. Prognostic Factors After Pulmonary Metastasectomy for Colorectal Cancer and Rationale for Determining Surgical Indications: A Retrospective Analysis. Ann. Surg. 2013, 257, 1059–1064. [Google Scholar] [CrossRef]
- Meimarakis, G.; Spelsberg, F.; Angele, M.; Preissler, G.; Fertmann, J.; Crispin, A.; Reu, S.; Kalaitzis, N.; Stemmler, M.; Giessen, C.; et al. Resection of Pulmonary Metastases from Colon and Rectal Cancer: Factors to Predict Survival Differ Regarding to the Origin of the Primary Tumor. Ann. Surg. Oncol. 2014, 21, 2563–2572. [Google Scholar] [CrossRef]
- Yamakado, K.; Inoue, Y.; Takao, M.; Takaki, H.; Nakatsuka, A.; Uraki, J.; Kashima, M.; Kusunoki, M.; Shimpo, H.; Takeda, K. Long-term results of radiofrequency ablation in colorectal lung metastases: Single center experience. Oncol. Rep. 2009, 22, 885–891. [Google Scholar] [CrossRef]
- Chua, T.C.; Thornbury, K.; Saxena, A.; Liauw, W.; Glenn, D.; Zhao, J.; Morris, D.L. Radiofrequency ablation as an adjunct to systemic chemotherapy for colorectal pulmonary metastases. Cancer 2010, 116, 2106–2114. [Google Scholar] [CrossRef]
- Gillams, A.; Khan, Z.; Osborn, P.; Lees, W. Survival after Radiofrequency Ablation in 122 Patients with Inoperable Colorectal Lung Metastases. Cardiovasc. Interv. Radiol. 2013, 36, 724–730. [Google Scholar] [CrossRef] [PubMed]
- Matsui, Y.; Hiraki, T.; Gobara, H.; Iguchi, T.; Fujiwara, H.; Nagasaka, T.; Toyooka, S.; Kanazawa, S. Long-Term Survival following Percutaneous Radiofrequency Ablation of Colorectal Lung Metastases. J. Vasc. Interv. Radiol. 2015, 26, 303–310. [Google Scholar] [CrossRef] [PubMed]
- Zhong, J.; Palkhi, E.; Ng, H.; Wang, K.; Milton, R.; Chaudhuri, N.; Lenton, J.; Smith, J.; Bhartia, B.; Wah, T.M. Long-Term Outcomes in Percutaneous Radiofrequency Ablation for Histologically Proven Colorectal Lung Metastasis. Cardiovasc. Interv. Radiol. 2020, 43, 1900–1907. [Google Scholar] [CrossRef]
- Ruers, T.J.M.; Joosten, J.J.; Wiering, B.; Langenhoff, B.S.; Dekker, H.M.; Wobbes, T.; Oyen, W.J.G.; Krabbe, P.F.M.; Punt, C.J.A. Comparison Between Local Ablative Therapy and Chemotherapy for Non-Resectable Colorectal Liver Metastases: A Prospective Study. Ann. Surg. Oncol. 2007, 14, 1161–1169. [Google Scholar] [CrossRef]
- Cheng, G.; Shi, L.; Qiang, W.; Wu, J.; Ji, M.; Lu, Q.; Li, X.; Xu, B.; Jiang, J.; Wu, C. The safety and efficacy of microwave ablation for the treatment of CRC pulmonary metastases. Int. J. Hyperth. 2018, 34, 486–491. [Google Scholar] [CrossRef] [PubMed]
- Gillams, A.R.; Lees, W.R. Radiofrequency ablation of lung metastases: Factors influencing success. Eur. Radiol. 2008, 18, 672–677. [Google Scholar] [CrossRef]
- Hiraki, T.; Sakurai, J.; Tsuda, T.; Gobara, H.; Sano, Y.; Mukai, T.; Hase, S.; Iguchi, T.; Fujiwara, H.; Date, H.; et al. Risk factors for local progression after percutaneous radiofrequency ablation of lung tumors. Cancer 2006, 107, 2873–2880. [Google Scholar] [CrossRef]
- Yang, Q.; Qi, H.; Zhang, R.; Wan, C.; Song, Z.; Zhang, L.; Fan, W. Risk Factors for Local Progression after Percutaneous Radiofrequency Ablation of Lung Tumors: Evaluation Based on a Review of 147 Tumors. J. Vasc. Interv. Radiol. 2017, 28, 481–489. [Google Scholar] [CrossRef]
- Ridge, C.A.; Solomon, S.B. Percutaneous ablation of colorectal lung metastases. J. Gastrointest. Oncol. 2015, 6, 685–692. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Fuster, A.; Belda-Sanchis, J.; Aguiló, R.; Embun, R.; Mojal, S.; Call, S.; Molins, L.; De Andrés, J.J.R.; Zafra, J.R.; Navarrete, C.P.; et al. Morbidity and mortality in a large series of surgical patients with pulmonary metastases of colorectal carcinoma: A prospective multicentre Spanish study (GECMP-CCR-SEPAR). Eur. J. Cardio Thorac. Surg. 2013, 45, 671–676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steéphan, F.; Boucheseiche, S.; Hollande, J.; Flahault, A.; Cheffi, A.; Bazelly, B.; Bonnet, F. Pulmonary Complications Following Lung Resection: A Comprehensive Analysis of Incidence and Possible Risk Factors. Chest 2000, 118, 1263–1270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peng, Z.; Li, H.; Zhang, C.; Qian, X.; Feng, Z.; Zhu, S. A Retrospective Study of Chronic Post-Surgical Pain following Thoracic Surgery: Prevalence, Risk Factors, Incidence of Neuropathic Component, and Impact on Qualify of Life. PLoS ONE 2014, 9. [Google Scholar] [CrossRef] [Green Version]
- Stone, B.; Mangona, V.S.; Johnson, M.D.; Ye, H.; Grills, I.S. Changes in Pulmonary Function Following Image-Guided Stereotactic Lung Radiotherapy: Neither Lower Baseline Nor Post-SBRT Pulmonary Function Are Associated with Worse Overall Survival. J. Thorac. Oncol. 2015, 10, 1762–1769. [Google Scholar] [CrossRef] [Green Version]
- Lencioni, R.; Crocetti, L.; Cioni, R.; Suh, R.; Glenn, D.; Regge, D.; Helmberger, T.; Gillams, A.R.; Frilling, A.; Ambrogi, M.; et al. Response to radiofrequency ablation of pulmonary tumours: A prospective, intention-to-treat, multicentre clinical trial (the RAPTURE study). Lancet Oncol. 2008, 9, 621–628. [Google Scholar] [CrossRef]
- De Baère, T.; Palussière, J.; Aupérin, A.; Hakime, A.; Abdel-Rehim, M.; Kind, M.; Dromain, C.; Ravaud, A.; Tebboune, N.; Boige, V.; et al. Midterm Local Efficacy and Survival after Radiofrequency Ablation of Lung Tumors with Minimum Follow-up of 1 Year: Prospective Evaluation. Radiology 2006, 240, 587–596. [Google Scholar] [CrossRef] [PubMed]

| Authors | Pneumothorax | Drain | Pleural Effusion | Fistula | Hemorrage | Pneumonia |
|---|---|---|---|---|---|---|
| T.D. Yan [30] | 29% | 16% | 7% | - | 9% | - |
| K. Yamakado [36] | 22% | 13% | 1% | - | - | - |
| T.C. Chua [37] | - | 33% | - | - | - | - |
| A. Gillams [38] | - | - | - | - | - | - |
| T. de Baere [25] | 67% | 39% | 0.2% | |||
| J. Ferguson [31] | 54% | 19% | 1% | 1% | 1% | - |
| Y. Matsui [39] | - | - | - | - | - | - |
| I. Kurilova [32] | 58% | 38% | - | - | - | 2% |
| M. Fonck [27] | 72% | 47% | 2% | - | - | 1% |
| J. Zhong [40] | 60% | 30% | 3% | 3% | - | - |
| M.R. Calslstrom [26] | - | 26% | - | 0% | - | - |
| T. Hasegawa [23] | - | 20% | 1% | - | 1% | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Delpla, A.; de Baere, T.; Varin, E.; Deschamps, F.; Roux, C.; Tselikas, L. Role of Thermal Ablation in Colorectal Cancer Lung Metastases. Cancers 2021, 13, 908. https://doi.org/10.3390/cancers13040908
Delpla A, de Baere T, Varin E, Deschamps F, Roux C, Tselikas L. Role of Thermal Ablation in Colorectal Cancer Lung Metastases. Cancers. 2021; 13(4):908. https://doi.org/10.3390/cancers13040908
Chicago/Turabian StyleDelpla, Alexandre, Thierry de Baere, Eloi Varin, Frederic Deschamps, Charles Roux, and Lambros Tselikas. 2021. "Role of Thermal Ablation in Colorectal Cancer Lung Metastases" Cancers 13, no. 4: 908. https://doi.org/10.3390/cancers13040908