1. Introduction
Epidermal growth factor receptor I (EGFR) is a 170 kDa transmembrane cell-surface glycoprotein which belongs to the ErbB family. EGFR and its family members play a variety of roles in the aberrant growth, oncogenesis and tumor progression in different cancers and cell types [
1,
2]. Overexpression of EGFR is known to drive a subset of aggressive cancers, including squamous cell head and neck [
3], glioma [
4], non-small cell lung, colorectal [
5], ovarian [
2,
6], breast [
7] and cervical cancers. In addition, a crosstalk of this receptor with many other receptors including those from its subfamily causes resistance to targeted therapies [
8,
9]. Structurally, EGFR consists of an extracellular ligand-binding, transmembrane, and intracellular domains. The extracellular binding domain has four subdomains, domains I–IV. Ligands of EGFR (epidermal growth factor, amphiregulin, transforming growth factor receptor α) bind to EGFR initiating a homo- and hetero-dimerization which results in downstream signal activation of the receptor(s) [
2].
Ex vivo quantification of EGFR using biopsy samples are inherently flawed because of the intra-and inter-lesion heterogeneity of tumors. It is also known that EGFR expression of tumors changes over time [
10,
11]. In vivo assessment techniques have several advantages over current ex vivo methods, including measuring EGFR expression over the entire tumor volume rather than just a section of the tumor, assessing the biologic availability of EGFR in vivo, evaluating effects of therapy on EGFR expression, and quantifying EGFR expression of all lesions in real time.
EGFR overexpression in a wide range of cancers makes it a validated target for imaging and therapy using monoclonal antibodies. A few anti-EGFR monoclonal antibodies such as cetuximab, panitumumab, necitumumab and nimotuzumab are approved for treatment in different countries. These antibodies bind to domain III of EGFR [
12,
13,
14,
15]. Some of them have been radiolabeled with different isotopes for use as diagnostics. The clinical utility of
89Zr-cetuximab PET/CT in selecting patients that would benefit from treatment using an EGFR targeted monoclonal antibody was recently demonstrated in colorectal cancer patients by Menke-van der Houven van Oordt et al. [
16]. Only patients with positive
89Zr-cetuximab PET/CT lesions showed clinical benefit with the therapeutic monoclonal antibody cetuximab.
89Zr-cetuximab and other domain III imaging agents can only be used for diagnosis and patient selection. They cannot be used to monitor response to treatment using anti-EGFR monoclonal antibodies, since the imaging probe will compete for binding with the therapeutic antibody.
Therefore, there is strong interest to develop novel imaging agents that bind to epitopes/domains that are different from that of the therapeutic agent. A domain II binder can find applications in patient selection, diagnosis and monitoring of response to anti-EGFR treatments. For the first time, Miersch et al. recently engineered a domain II (8709-scFv-Fc) specific anti-EGFR antibody using phage display [
1]. Anti-EGFR antibody 8709-scFv-Fc inimitably binds to domain II of EGFR with a high affinity and does not interfere with the binding of clinically available anti-EGFR therapeutic antibodies e.g., cetuximab [
17]. The expression, purification and optical imaging of the 8709-scFv-Fc antibody fragment has been published [
17].
Here, we have evaluated the in vitro and in vivo properties of 8709-scFv-Fc fragment radiolabeled with 89Zr via a deferoxamine (p-SCN-Bn-deferoxamine) chelator in EGFR overexpressing cell lines and mouse xenografts and controls. We present the in vitro cell binding characteristics as well as in vivo biodistribution, pharmacokinetics and microPET imaging in tumor-bearing mice. Our results show that 89Zr-8709-scFv-Fc has the potential to be used for diagnosis, patient selection and treatment monitoring of EGFR-positive cancers.
2. Materials and Methods
2.1. Characterization of Antibody
Anti-EGFR antibody 8709-Fab was identified by phage display and converted to an scFv-Fc (8709-scFv-Fc) its expression, purification and fluorescent imaging has been published [
17].
2.2. Cell Lines and Xenografts
EGFR positive DLD-1 (RRID:CVCL_0248) colorectal cancer, breast cancer MDA-MB-231 (RRID:CVCL_0062), and EGFR negative human melanoma MDA-MB-435 (RRID:CVCL_0417) cell lines were obtained from ATCC (Rockville, MD, USA). MDA-MB-435 cells are derived from M14 melanoma cells. Cells were propagated by serial passage in MEM/EBSS medium, supplemented with 10% fetal bovine serum (Biochrom, Sigma-Aldrich, St. Louis, MO, USA) at 37 °C in a humidified atmosphere of 5% CO2. All human cell lines have been authenticated using STR profiling within the last three years. All experiments were performed with mycoplasma-free cells.
All animals used in imaging experiments were cared for and maintained under the supervision and guidelines of the University of Saskatchewan Animal Care Committee (UACC). All animal studies were approved by UACC in accordance with the guidelines set forth on the Use of Laboratory Animals (protocol # 20170084) [
18]. Female CD-1 nude mice were obtained from Charles River Canada (St-Constant, Quebec) at 4 weeks of age and housed in a 12 h light, 12 h dark cycle in a temperature and humidity-controlled vivarium. Animals had libitum access to diet (Lab Diet, St. Louis, MO, USA) and water [
18]. After one week of acclimatization, mice were subcutaneously injected with a suspension of 5–10 × 10
6 DLD-1, MDA-MB-231 or MDA-MB-435 cells in 100 μL of a 1:1 mixture of serum-free MEM/EBSS medium (HyClone Laboratories, Logan, UT, USA) and Matrigel matrix basement membrane (Discovery Laboware, Inc. Bedford, MA, USA) at the hind limb of each mouse. Xenograft was located in the right thigh of the hind leg of the mouse and tumor growth was followed with caliper measurements.
2.3. Conjugation of Antibodies with Bifunctional Chelators
Conjugation of 8709-scFv-Fc (domain I/II binder) was performed as reported earlier [
19]. The excess unreacted chelator was removed by centrifugation using an Amicon Ultra-10 K (Burlington, MA, USA) molecular filtration device. The solution of DFO-8709-scFv-Fc was aliquoted and stored at −80 °C until further use after quality control. 8709-scFv-Fc and DFO-8709-scFv-Fc purities were determined using SEC-HPLC (Waters 2796 Bioseparations Module, Waters 2487 Dual λ Absorbance Detector, XBridge BEH 200A SEC 3.5 µm 7.8 × 300 mm column, Waters Corporation, Milford, MA, USA). The UV-Detector was set at 220 and 280 nm and the solvent system was PBS at a flow rate of 0.6 mL/min. Nimotuzumab (domain III binder) was conjugated with DOTA for labeling with
111In following lab protocol [
18].
The analysis of MW and purity of conjugated antibody was performed on an Agilent 2100 Bioanalyzer using Agilent High Sensitivity Protein 250 Kit using the manufacturer’s protocol. The size and relative peak area were calculated using Agilent 2100 Expert software (Agilent Technologies, Santa Clara, CA, USA, cat # 5067-1575).
Binding kinetics between the antibodies and recombinant monomeric EGFR were measure with ForteBio Octet RED384 (PALL Corporation, NY, USA). Antibodies were immobilized on anti-human FAB-CH1 sensors (18-5104, Forte Bio) according to manufacture’s instructions. The equilibrium dissociation constant (K
D) was obtained using a 1 to 1 binding model with global fitting. Data analysis and curve fitting was performed using data analysis software 7.1.0.33 (Forte Bio, Santa Clara, CA, USA). Saturation binding flow cytometry was performed as described previously [
17].
2.4. Production and Characterization of 89Zr-Oxalate
89Zr-oxalate was produced at the Saskatchewan Centre for Cyclotron Sciences (SCCS), University of Saskatchewan. Yttrium coated (10 mm diameter and 200 µm thickness) on the coin shaped niobium (24 mm diameter and 1 mm thickness) target supplied by ACSI, was irradiated with an incident beam energy of 17.8 MeV providing a degraded transmitted energy through an aluminum degrader of 12.8 MeV and a current of 40 µA for 2 h on an in-house beam-line on TR-24 cyclotron to produce 89Zr via the natY(p, n)89Zr reaction. During irradiation the target was cooled on the frontal side by Helium gas and on the back side by chilled water. After the irradiation, the target left on the target station for 2–3 h to allow decay of short-lived isotopes. Then target was released in the lead pig and transported to the hot cells in the lead shielded cart.
89Zr was separated as
89Zr-oxalate from the irradiated yttrium coin as described by Queern et al. [
20]. Briefly, to a dissolution vessel charged with the irradiated target 2 N trace metal HCl (4 mL) was added slowly. The resulting solution was warmed to 80 °C for 20 min and cooled to room temperature before loading onto a pre-conditioned column of hydroxamate resin (100 mg). A dissolution vessel and target body rinsed with 2 N trace metal HCl (2 mL) and loaded onto hydroxamate resin. Then hydroxamate resin was rinsed with 2N HCl (14 mL) followed by traceselect water (10 mL). Finally,
89Zr was eluted with 1.5 mL of 1.0 M Oxalic acid
89Zr-oxalate was characterized for activity amount, half-life, radionuclidic purity, elemental impurities and specific activity. The final activity of purified
89Zr-oxalate was measured in the Capintec dose calibrator (CRC-55t PET). Specific activity was determined using a published method by Holland et al. [
21] and the specific activity was found to be in the range of 673-1161 MBq/µmol. The
89Zr-oxalate solutions were tested for radionuclidic identity and purity using a high purity germanium (HPGe) detector (Ortec, Oak Ridge, TN, USA). The radiochemical purity was 99.99% and the identity was confirmed by the presence of 909 keV and 511 keV peaks. The ICP-MS analysis of
89Zr-oxalate solutions were performed at Saskatchewan Research Council, Saskatoon and elemental impurity levels were found to be always below 30 ppm and all batches met the QC release specifications.
2.5. Radiolabeling and Characterization of 89Zr-8709-scFv-Fc and 111In-Nimotuzumab
Radiolabeling of DFO-8709 conjugate with
89Zr-oxalate was performed as per the standard lab protocol [
19]. After radiolabeling the reaction mixture was cooled to room temperature and an aliquot was injected onto SEC-HPLC (the same HPLC and solvent system as above) for radiochemical quality control and radiolabeling efficiency determination. Oxalate, HEPES and other impurities (less than 30 kDa) were removed from the crude reaction mixture by single centrifugation in spin columns (Amicon Ultra-4 Centrifugal Filter 30K NMCO, 4 mL, EMD Millipore, Burlington, MA, USA) and sterilized by filtration with 0.22 µm hydrophilic PTFE membrane filter (Ultrafree-CL Centrifugal filter 4 mL, Millipore). The final solution was formulated in PBS. The recovery of the radiolabeled product was 60% for
89Zr-DFO-8709-scFv-Fc with a radiochemical purity of > 95% was used for in vitro and in vivo experiments.
Radiolabeling of DOTA-nimotuzumab conjugate with
111InCl
3 was performed as per the standard lab protocol [
18]. After labeling, the reaction was monitored using iTLC strip with 100 mM sodium citrate buffer (pH 5.0) as the mobile phase and analyzed using ScanRam (LabLogic, Brandon, FL, USA).
111In-labeled conjugates were purified using Amicon Ultra-4 centrifugal filters (10K, EMD Millipore) with PBS. The purity of the radiolabeled immunoconjugates were determined using size exclusion radio-HPLC and iTLC. A radiochemical purity (RCP) of more than 95% was considered good for in vitro and in vivo experiments.
2.6. In Vitro Binding
The in vitro saturation binding, immunoreactivity and domain specific binding of
89Zr-DFO-8709-scFv-Fc was determined in EGFR positive DLD-1 cells. A saturation radioligand binding assay was performed by incubating 0.5 million cells with increasing concentrations of radioimmunoconjugates (0.2–95 nmol/L in 100 μL PBS) for 4 h at 4 °C. Non-specific binding (NSB) was determined in a similar assay but in the presence of a 50-fold molar excess of unlabeled 8709-scFv-Fc (relative to the highest concentration of the radioimmunoconjugates). A non-linear regression analysis with one-site binding equation was used to determine K
D using GraphPad Prism 6 (GraphPad Software, La Jolla, CA, USA). The immunoreactive fraction of the radioimmunoconjugate was determined as described in Lindmo et al. [
22].
Domain II specific binding was determined by a competitive binding experiment. Briefly, one million DLD-1 cells were transferred in 3 vials and incubated with 89Zr-8709-scFv-Fc, but with slight modifications. The first vial was incubated only with 89Zr-8709-scFv-Fc, second vial was initially incubated with cold 8709-scFv-Fc whose concentration was 50× the concentration of radiolabeled 89Zr-8709-scFv-Fc. After 2 h of pre-incubation with unlabeled 8709-scFv-Fc, 89Zr-8709-scFv-Fc was added to these cells. The third vial was incubated with unlabeled nimotuzumab whose concentration was 50 × the concentration of radiolabeled 89Zr8709-scFv-Fc. After 2 h pre-incubation with nimotuzumab, 89Zr-8709-scFv-Fc was added to these cells. After incubation, the cells were centrifuged at 1200 rpm and supernatant was collected separately. This process was repeated 3 times to ensure complete removal of unbound 89Zr-8709-scFv-Fc. After centrifugation the pellet was re-dissolved in PBS and samples were measured using gamma counter. Experiments were performed in triplicate using three different concentrations (50, 5 and 0.5 nM) of 89Zr-8709-scFv-Fc.
2.7. Biodistribution and Pharmacokinetics
Biodistribution studies were performed in athymic CD-1 nude mice bearing EGFR positive DLD-1, and EGFR negative MDA-MB-435 (control) xenografts (n = 3/group). Each mouse received a dose of with 10 ± 0.2 MBq of 89Zr-8709-scFv-Fc (20 µg, specific activity of 0.5 MBq/µg). Animals were sacrificed at 24 and 168 h post injection (p.i.) and different organs were harvested (blood, lungs, liver, spleen, kidneys, bladder, muscle, heart, brain, bones, thymus, pancreas, stomach, small, and large intestine) for biodistribution. The activity in the organs was measured using a gamma counter (2480 Perkin Elmer, Waltham MA, USA) and the tissue uptake was expressed as percentage of injected activity per gram (% IA/g).
The pharmacokinetics was determined in healthy Balb/c mice (n = 5/group). The animals were injected with 10 ± 0.0.1 MBq of the 89Zr-8709-scFv-Fc via a tail vein and blood was collected at various time points from a saphenous vein in heparinized capillary tubes. Activity in the capillary tube was measured using a gamma counter and the blood volume was determined using a digital caliper, assuming the internal diameter of the tube. Radioactivity in blood activity was expressed as % IA/mL). All relevant pharmacokinetic parameters were determined using an exponential decay curve fitting from sigma plot using GraphPad Prism 6.
2.8. EGFR Domain Specific Imaging Using 111In-Nimotuzumab and 89Zr-8709-scFv-Fc
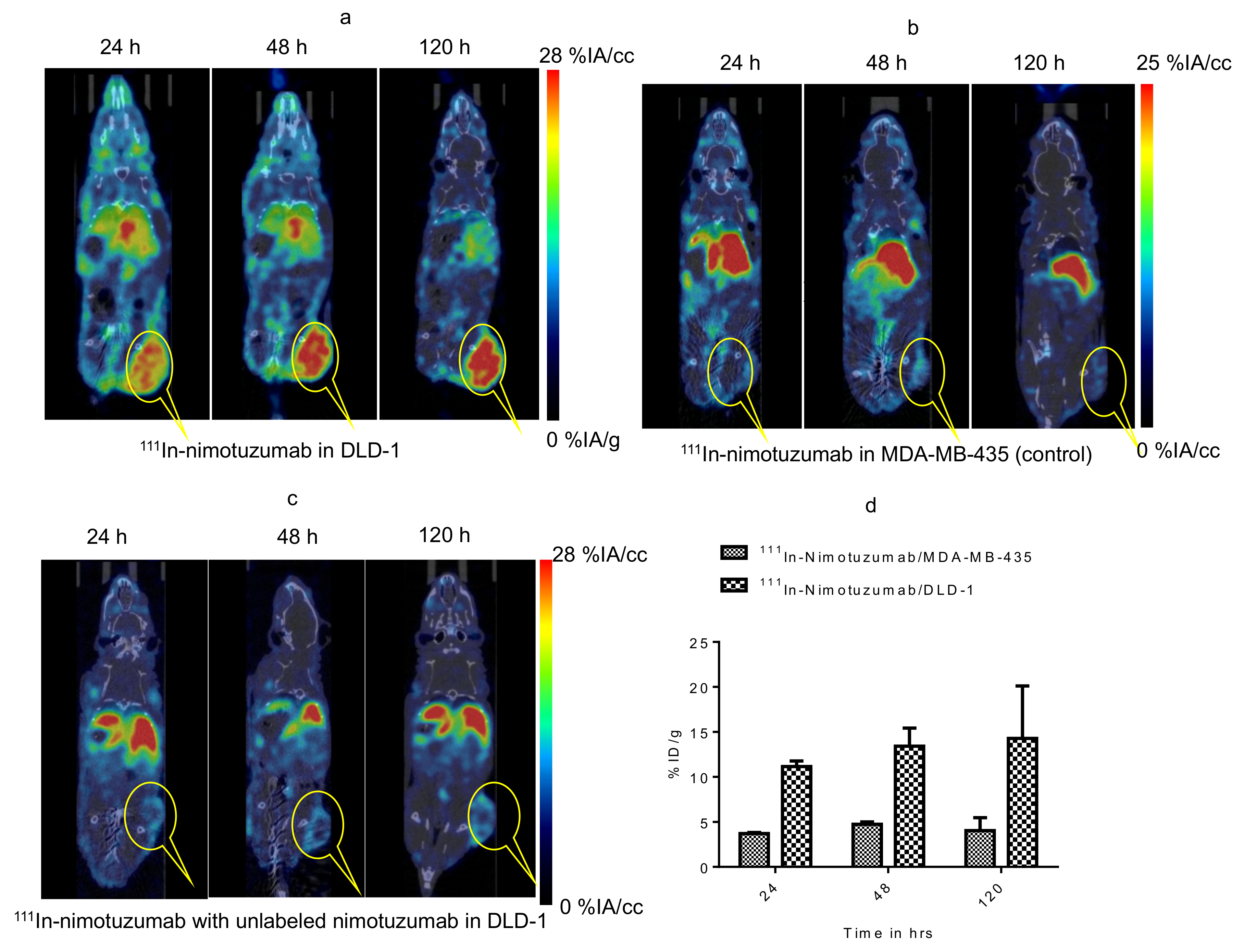
In vivo evaluation of domain III binding of 111In-nimotuzumab was studied with two groups of mice (n = 3), one group bearing EGFR positive DLD-1 xenografts and other bearing EGFR negative MDA-MB-435 xenografts. Mice were injected with 15 ± 0.2 MBq of 111In-nimotuzumab (0.5 MBq/µg) via tail vein injection. Imaging was performed in mice injected with EGFR positive DLD-1 and EGFR negative MDA-MB-435 (control) xenografts. Imaging was performed at three different time points 24 h, 48 h, and 120 h p.i.
In vivo evaluation of domain II binding of 89Zr-8709-scFv-Fc was also studied with two groups of mice (n = 3), one group bearing EGFR positive DLD-1 xenograft and other bearing EGFR negative MDA-MB-435 xenograft. Mice were injected with 9 ± 0.2 MBq of 89Zr-8709-scFv-Fc via a tail vein. Imaging was performed at three different time points 24 h, 48 h, and 120 h p.i.
To understand site-specific domain II binding of 89Zr-8709-scFv-Fc, one group (n = 3) of mice were initially injected with 250 µg of non-radiolabeled nimotuzumab to block the domain III of EGFR leaving domain II available for 89Zr-8709-scFv-Fc binding.
Simultaneously imaging of domain III and domain II was also studied following simultaneous injection of 89Zr-8709-scFv-Fc and 111In-nimotuzumab. Two groups of mice (n = 3) one group bearing EGFR positive DLD-1 xenograft and other bearing EGFR negative MDA-MB-435 xenograft were simultaneously injected with 9 ± 0.2 MBq of 89Zr-8709-scFv-Fc and 15 ± 0.2 MBq of 111In-nimotuzumab via tail vein injection.
To confirm domain II specificity, groups of mice (n = 3) bearing EGFR positive DLD-1 or MDA-MB-231 xenograft was initially injected with 250 ug (therapeutic dose) of unlabeled nimotuzumab to block domain III, followed by simultaneous injection with 9 ± 0.2 MBq of 89Zr-8709-scFv-Fc and/or 15 ± 0.2 MBq of 111In-nimotuzumab and microPET/SPECT/CT imaging.
PET/CT images were acquired at 24 h, 48 h, and 120 h p.i. using the Vector
4CT scanner (MILabs B.V., Utrecht, The Netherlands). PET scans were acquired in a list-mode data format with a high-energy ultra-high resolution (HE-UHR-1.0 mm) mouse/rat pinhole collimator. Corresponding CT scans were acquired and images were reconstructed using a pixel-based order-subset expectation maximization (POS-EM) algorithm that included resolution recovery and compensation for distance-dependent pinhole sensitivity and were registered on CT and quantified using PMOD 3.8 software (PMOD Technologies Ltd., Zurich, Switzerland). SPECT/CT images were acquired using collimator and detector settings as described previously [
19].
Tracer uptake was expressed as percentage injected activity (% IA) per cc of tissue volume (% IA/cc). All quantification data was reported as mean ± standard deviation within one animal study group. After imaging all mice were sacrificed for biodistribution. Activity in the organs was analyzed as percent injected activity per gram (% IA/g).
2.9. Statistical Analysis
All data was expressed as the mean ± SD or SEM of at least three independent experiments. Statistical comparisons between the experimental groups were performed by a t-test. Graphs were prepared and p values were calculated using GraphPad Prism (version 5.03). p values of less than 0.5 were considered significant.
2.10. Data Availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
4. Discussion
Molecular imaging agents such as
89Zr-cetuximab and
89Zr-panitumumab have been developed and evaluated in clinical trials [
16]. However, because these agents bind to the same epitope (mostly domain III) as the anti-EGFR therapeutic antibody, they cannot be used to monitor response to treatment of the same antibody. Approved anti-EGFR antibodies e.g., cetuximab, panitumumab, nimotuzumab and more recently necitumumab bind to domain III leaving the dimerization loop of EGFR (domain II) available for binding to other molecules. Therefore, a monoclonal antibody that binds to a domain other than domain III is needed for comprehensive diagnosis, monitoring of response to anti-EGFR antibody therapy and potentially as a biparatopic anti-EGFR therapeutic agent. For the first time we have developed an immunoPET agent that binds to epitope II of EGFR.
Using phage display we have screened and engineered antibodies and antibody fragments that bind to domain II of EGFR [
1]. We recently reported a near-infrared (NIR) fluorescently labeled IRDye800CW-8909 antibody and antibody fragments of this antibody [
17]. 8907-scFv-Fc emerged as the best fragment for imaging domain II of EGFR [
17]. The expression of 8907-scFv-Fc (50 mg/mL) was at least four-fold better than the other fragments and IgG. In addition, NIR showed that tumor uptake and target to organ ratios of 8907-scFv-Fc was better than all other fragments including the IgG. Here, we report the initial evaluation of a
89Zr-labeled 8907-scFv-Fc fragment of the antibody fragment for potential use in non-invasive diagnosis, patient selection and monitoring of response to anti-EGFR monoclonal antibody treatment by PET.
Conjugation of 8709-scFv-Fc resulted in an average of two molecules of DFO attached to 8709-scFv-Fc which was evident from bioanalyzer. Bioanalyzer results show that there was a slight difference in the molecular weight of 8709-scFv-Fc and DFO-8709-scFv-Fc. Flow cytometry data suggests that, binding affinity of DFO-8709-scFv-Fc was not significantly (72 nM vs 97 nM for 8709-scFv-Fc and DFO-8709-scFv-Fc, respectively in DLD-1 cells) altered by conjugation, indicating conjugation and chemicals used in the reaction did not alter the characteristics of the antibody fragment.
The strategy to develop an antibody imaging agent that binds to a different epitope from the therapeutic antibody has already been investigated using anti-HER2 antibodies pertuzumab (domain II) and trastuzumab (domain IV) [
23,
24,
25]. Pertuzumab (Perjeta) and trastuzumab (Herceptin) are approved for treating HER2 positive breast cancer [
26]. A number of authors have developed radiolabeled derivatives of pertuzumab for imaging and monitoring of response to trastuzumab [
23,
25]. Marquez et al. [
23] evaluated
89Zr-pertuzumab in mice bearing HER2 positive xenografts with or without the administration of unlabeled trastuzumab. It was shown that the administration of unlabeled trastuzumab 5–60 min before the administration of
89Zr-pertuzumab led to an increase in tumor uptake of
89Zr-pertuzumab compared to mice without pre-administration of unlabeled trastuzumab suggesting treatment with unlabeled trastuzumab may affect the quantification of HER2, despite the fact that both antibodies bind to unique epitopes of the receptor. This observation remains unclear and should be interpreted with caution given the large standard deviation seen in that study. On the other hand, Scheuer et al. [
27] showed that the binding of near infrared labeled pertuzumab was not affected by the presence of unlabeled trastuzumab. Assuming this data by Marquez et al. were reliable,
89Zr-pertuzumab would have limited value in monitoring response to trastuzumab treatment. Here, we showed that anti-EGFR nimotuzumab (domain III) did not alter the in vitro binding (
Figure 2) and tumor uptake in vivo (
Figure 5 and
Figure S4) of anti-EGFR
89Zr-8709-scFv-Fc. Similarly, the presence of 8709-scFv-Fc did not alter the binding of
111In-nimotuzumab in vitro and in vivo. We also previously showed using near infrared labeled 8709 antibody fragments did not bind cells overexpressing mutant EGFR
vIII which has all of domain I and most of domain II deleted [
17].
Our in vivo studies show a rather low tumor uptake of the
89Zr-8709-scFv-Fc imaging agent. The highest tumor uptake was 6.5 %IA/cc by microPET which was almost two-fold less that for
89Zr-nimotuzumab seen in this model in a previous study [
19]. This rather low tumor uptake may be attributed to the high K
D of 8709-scFv-Fc fragment (72 nM) compared with nimotuzumab (14 nM). The pharmacokinetics of
89Zr-8709-scFv-Fc was similar to
89Zr-nimotuzumab, indicating that it is not the reason for the observed differences in tumor uptake of
89Zr-8709-scFv-Fc versus
89Zr-nimotuzumab [
19]. In addition, we observed a rather higher than normal kidney uptake for
89Zr-8709-scFv-Fc. Since the size of scFv-Fc is greater than the kidney cutoff this high uptake maybe suggestive of in vivo proteolysis. Additional studies are needed to investigate the stability of this fragment. Strategies such as affinity maturation could be employed in the future to improve the binding and therefore tumor uptake of
89Zr-8709-scFv-Fc.
5. Conclusions
Necitumumab is the first anti-EGFR therapeutic antibody that is indicated only in squamous NSCLC patients whose cancer is positive for EGFR by immunohistochemistry [
28]. Given the inherent issues associated with EGFR determination by immunohistochemistry, better strategies to diagnose, select patients for anti-EGFR treatments and monitor response are needed. Agents that bind to the same epitope as the therapeutic agent would have limited value, hence the need for those that bind to different epitopes. Here, we presented an anti-EGFR domain II PET imaging agent
89Zr-8709-scFv-Fc. The domain specificity of
89Zr-8709-scFv-Fc indicates that this immunoPET agent may find applications for diagnosis, patient selection and monitoring of response to anti-EGFR treatments. In its current form, translation of
89Zr-8709-scFv-Fc will be limited by the rather low tumor uptake shown in these studies, which is due in part by the high K
D (72 nM). Most therapeutic antibodies in this class are pico–low nanomolar affinities. Ongoing engineering studies on affinity maturation of 8709-scFv-Fc/8709-IgG would improve tumor uptake and hence imaging characteristics of the imaging agent(s).

 ,
, 








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}