
Higher Radiation Dose to the Immune Cells Correlates with Worse Tumor Control and Overall Survival in Patients with Stage III NSCLC: A Secondary Analysis of RTOG0617

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Clinical and Dosimetric Patient Data
2.2. EDIC Computation
2.3. Outcomes and Statistical Considerations
3. Results
3.1. Patient Characteristics and the EDIC
3.2. Univariate Analysis of the EDIC and Clinical Factors for OS, PFS and LPFS
3.3. The EDIC in Multivariable Analysis of Factors Associated with OS, PFS and LPFS
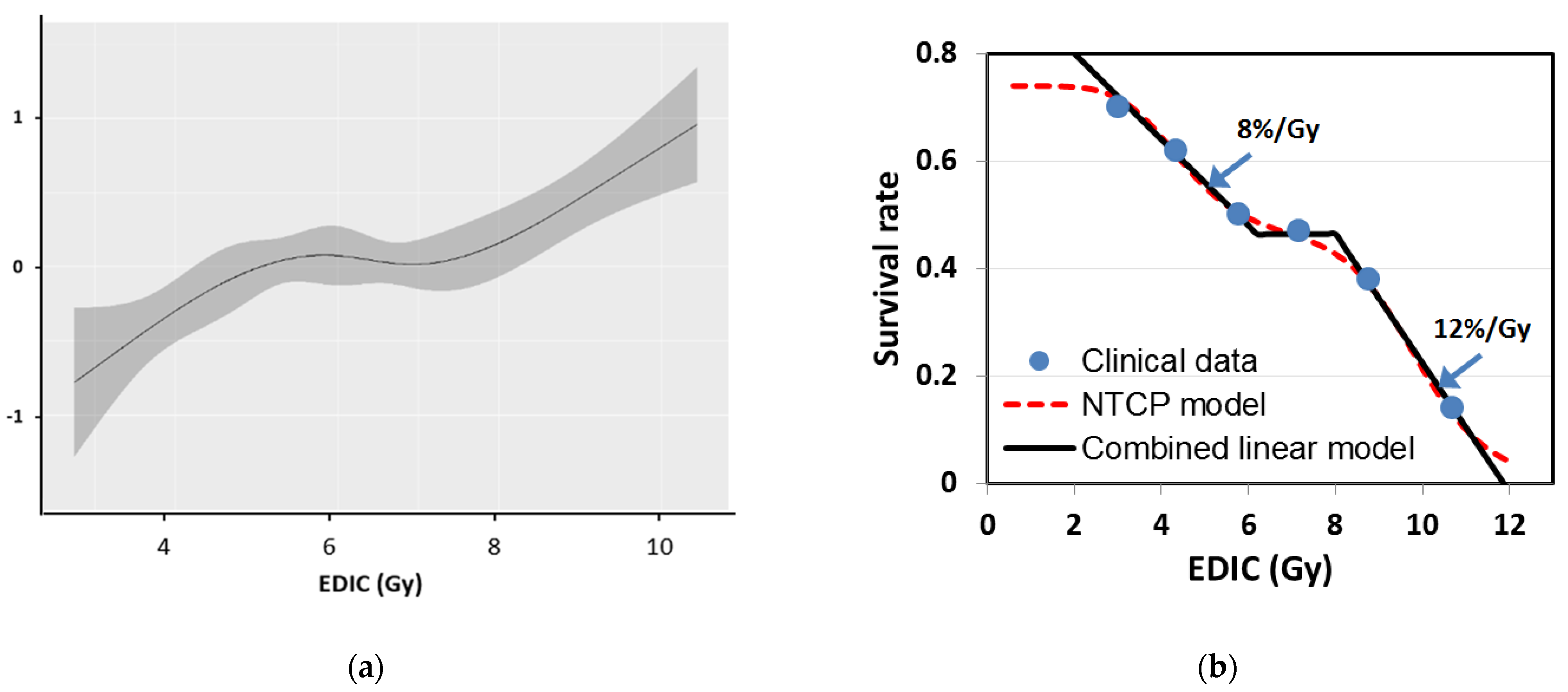
3.4. Non-Linear Relationship between the EDIC and OS
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
References
- Miller, K.D.; Siegel, R.L.; Lin, C.C.; Mariotto, A.B.; Kramer, J.L.; Rowland, J.H.; Stein, K.D.; Alteri, R.; Jemal, A. Cancer treatment and survivorship statistics, 2016. CA Cancer J. Clin. 2016, 66, 271–289. [Google Scholar] [CrossRef] [Green Version]
- Tyldesley, S.; Boyd, C.; Schulze, K.; Walker, H.; MacKillop, W.J. Estimating the need for radiotherapy for lung cancer: An evidence-based, epidemiologic approach. Int. J. Radiat. Oncol. Biol. Phys. 2001, 49, 973–985. [Google Scholar] [CrossRef]
- Furuse, K.; Fukuoka, M.; Kawahara, M.; Nishikawa, H.; Takada, Y.; Kudoh, S.; Katagami, N.; Ariyoshi, Y. Phase III study of concurrent versus sequential thoracic radiotherapy in combination with mitomycin, vindesine, and cisplatin in unresectable stage III non-small-cell lung cancer. J. Clin. Oncol. 1999, 17, 2692. [Google Scholar] [CrossRef]
- Antonia, S.J.; Villegas, A.; Daniel, D.; Vicente, D.; Murakami, S.; Hui, R.; Kurata, T.; Chiappori, A.; Lee, K.H.; De Wit, M.; et al. Overall survival with durvalumab after chemoradiotherapy in stage III NSCLC. N. Engl. J. Med. 2018, 379, 2342–2350. [Google Scholar] [CrossRef] [PubMed]
- Kong, F.-M.; Haken, R.T.; Schipper, M.J.; Sullivan, M.A.; Chen, M.; Lopez, C.; Kalemkerian, G.P.; Hayman, J.A. High-dose radiation improved local tumor control and overall survival in patients with inoperable/unresectable non-small-cell lung cancer: Long-term results of a radiation dose escalation study. Int. J. Radiat. Oncol. 2005, 63, 324–333. [Google Scholar] [CrossRef] [PubMed]
- Bradley, J.D.; Paulus, R.; Komaki, R.; Masters, G.; Blumenschein, G.; Schild, S.; Bogart, J.; Hu, C.; Forster, K.; Magliocco, A.; et al. Standard-dose versus high-dose conformal radiotherapy with concurrent and consolidation carboplatin plus paclitaxel with or without cetuximab for patients with stage IIIA or IIIB non-small-cell lung cancer (RTOG 0617): A randomised, two-by-two factorial phase 3 study. Lancet Oncol. 2015, 16, 187–199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Formenti, S.C. Silvia Formenti on the promise of combining radiotherapy and immunotherapy to treat cancer. Oncology 2016, 30, 289–292. [Google Scholar] [PubMed]
- Lee, Y.; Auh, S.L.; Wang, Y.; Burnette, B.; Meng, Y.; Beckett, M.; Sharma, R.; Chin, R.; Tu, T.; Weichselbaum, R.R.; et al. Therapeutic effects of ablative radiation on local tumor require CD8+ T cells: Changing strategies for cancer treatment. Blood 2009, 114, 589–595. [Google Scholar] [CrossRef]
- Vanpouille-Box, C.; Formenti, S.C.; Demaria, S. Towards precision radiotherapy for use with immune checkpoint blockers. Clin. Cancer Res. 2017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Postow, M.A.; Callahan, M.K.; Barker, C.A.; Yamada, Y.; Yuan, J.; Kitano, S.; Mu, Z.; Rasalan, T.; Adamow, M.; Ritter, E.; et al. Immunologic correlates of the abscopal effect in a patient with melanoma. N. Engl. J. Med. 2012, 366, 925–931. [Google Scholar] [CrossRef] [Green Version]
- Grossman, S.A.; Ye, X.; Lesser, G.; Sloan, A.; Carraway, H.; Desideri, S.; Piantadosi, S. Immunosuppression in patients with high-grade gliomas treated with radiation and temozolomide. Clin. Cancer Res. 2011, 17, 5473–5480. [Google Scholar] [CrossRef] [Green Version]
- Campian, J.L.; Ye, X.; Brock, M.; Grossman, S.A. Treatment-related lymphopenia in patients with stage III non-small-cell lung cancer. Cancer Investig. 2013, 31, 183–188. [Google Scholar] [CrossRef]
- Davuluri, R.; Jiang, W.; Fang, P.; Xu, C.; Komaki, R.; Gomez, D.R.; Welsh, J.; Cox, J.D.; Crane, C.H.; Hsu, C.C.; et al. Lymphocyte nadir and esophageal cancer survival outcomes after chemoradiation therapy. Int. J. Radiat. Oncol. Biol. Phys. 2017, 99, 128–135. [Google Scholar] [CrossRef] [PubMed]
- Wild, A.T.; Ye, X.; Ellsworth, S.G.; Smith, J.A.; Narang, A.K.; Garg, T.; Campian, J.; Laheru, D.A.; Zheng, L.; Wolfgang, C.L.; et al. The association between chemoradiation-related lymphopenia and clinical outcomes in patients with locally advanced pancreatic adenocarcinoma. Am. J. Clin. Oncol. 2015, 38, 259–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wild, A.T.; Herman, J.M.; Dholakia, A.S.; Moningi, S.; Lu, Y.; Rosati, L.M.; Hacker-Prietz, A.; Assadi, R.K.; Saeed, A.M.; Pawlik, T.M.; et al. Lymphocyte-sparing effect of stereotactic body radiation therapy in patients with unresectable pancreatic cancer. Int. J. Radiat. Oncol. Biol. Phys. 2016, 94, 571–579. [Google Scholar] [CrossRef] [Green Version]
- Meyer, K.K. Radiation-induced lymphocyte-immune deficiency. A factor in the increased visceral metastases and decreased hormonal responsiveness of breast cancer. Arch. Surg. 1970, 101, 114–121. [Google Scholar] [CrossRef] [PubMed]
- MacLennan, I.C.; Kay, H.E. Analysis of treatment in childhood leukemia. IV. The critical association between dose fractionation and immunosuppression induced by cranial irradiation. Cancer 1978, 41, 108–111. [Google Scholar]
- Yovino, S.; Kleinberg, L.; Grossman, S.A.; Narayanan, M.; Ford, E. The etiology of treatment-related lymphopenia in patients with malignant gliomas: Modeling radiation dose to circulating lymphocytes explains clinical observations and suggests methods of modifying the impact of radiation on immune cells. Cancer Investig. 2013, 31, 140–144. [Google Scholar] [CrossRef] [Green Version]
- Arina, A.; Beckett, M.; Fernandez, C.; Zheng, W.; Pitroda, S.; Chmura, S.J.; Luke, J.J.; Forde, M.; Hou, Y.; Burnette, B.; et al. Tumor-reprogrammed resident T cells resist radiation to control tumors. Nat. Commun. 2019, 10, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Jin, J.; Hu, C.; Xiao, Y.; Zhang, H.; Ellsworth, S.; Schild, S.; Bogart, J.; Dobelbower, M.; Kavadi, V.; Narayan, S.; et al. Higher radiation dose to immune system is correlated with poorer survival in patients with stage III non-small cell lung cancer: A secondary study of a phase 3 cooperative group trial (NRG oncology RTOG 0617). Int. J. Radiat. Oncol. Biol. Phys. 2017, 99, S151–S152. [Google Scholar] [CrossRef] [Green Version]
- Harre, J.F.E.; Lee, K.L.; Pollock, B.G. Regression models in clinical studies: Determining relationships between predictors and response. J. Natl. Cancer Inst. 1988, 80, 1198–1202. [Google Scholar] [CrossRef]
- Grambsch, P.; Therneau, T. Proportional hazards tests and diagnostics based on weighted residuals. Biometrika 1994, 81, 515–526. [Google Scholar] [CrossRef]
- Tucker, S.L.; Liu, A.; Gomez, D.; Tang, L.L.; Allen, P.; Yang, J.; Liao, Z.; Grosshans, D. Impact of heart and lung dose on early survival in patients with non-small cell lung cancer treated with chemoradiation. Radiother. Oncol. 2016, 119, 495–500. [Google Scholar] [CrossRef]
- Speirs, C.K.; DeWees, T.A.; Rehman, S.; Molotievschi, A.; Velez, M.A.; Mullen, D.; Fergus, S.; Trovo, M.; Bradley, J.D.; Robinson, C.G. Heart dose is an independent dosimetric predictor of overall survival in locally advanced non-small cell lung cancer. J. Thorac. Oncol. 2017, 12, 293–301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ladbury, C.J.; Rusthoven, C.G.; Camidge, D.R.; Kavanagh, B.D.; Nath, S.K. Impact of radiation dose to the host immune system on tumor control and survival for stage III non-small cell lung cancer treated with definitive radiation therapy. Int. J. Radiat. Oncol. 2019, 105, 346–355. [Google Scholar] [CrossRef]
- So, T.H.; Chan, S.K.; Chan, W.L.; Choi, H.; Chiang, C.L.; Lee, V.; Lam, T.C.; Wong, I.; Law, S.; Kwong, D.; et al. Lymphopenia and radiation dose to circulating lymphocytes with neoadjuvant chemoradiation in esophageal squamous cell carcinoma. Adv. Radiat. Oncol. 2020, 5, 880–888. [Google Scholar] [CrossRef]
- Xu, C.; Jin, J.-Y.; Zhang, M.; Liu, A.; Wang, J.; Mohan, R.; Kong, F.-M.; Lin, S.H. The impact of the effective dose to immune cells on lymphopenia and survival of esophageal cancer after chemoradiotherapy. Radiother. Oncol. 2020, 146, 180–186. [Google Scholar] [CrossRef]
- Jin, J.-Y.; Gu, A.; Wang, W.; Oleinick, N.L.; Machtay, M.; Kong, F.-M. Ultra-high dose rate effect on circulating immune cells: A potential mechanism for FLASH effect? Radiother. Oncol. 2020, 149, 55–62. [Google Scholar] [CrossRef]
- Kong, F.-M.; Haken, R.K.T.; Schipper, M.; Frey, K.A.; Hayman, J.; Gross, M.; Ramnath, N.; Hassan, K.A.; Matuszak, M.; Ritter, T.; et al. Effect of midtreatment PET/CT-adapted radiation therapy with concurrent chemotherapy in patients with locally advanced non-small-cell lung cancer: A phase 2 clinical trial. JAMA Oncol. 2017, 3, 1358–1365. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.Y.; Verma, V.; Li, M.; Zhang, W.; Komaki, R.; Lu, C.; Allen, P.K.; Liao, Z.; Welsh, J.; Lin, S.H.; et al. Proton beam radiotherapy and concurrent chemotherapy for unresectable stage III non-small cell lung cancer: Final results of a phase 2 study. JAMA Oncol. 2017, 3, e172032. [Google Scholar] [CrossRef] [PubMed]
- Jin, J.-Y.; Wang, W.; Haken, R.T.; Chen, J.; Bi, N.; Sadek, R.; Zhang, H.; Lawrence, T.S.; Kong, F.-M. Use a survival model to correlate single-nucleotide polymorphisms of DNA repair genes with radiation dose—Response in patients with non-small cell lung cancer. Radiother. Oncol. 2015, 117, 77–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heylmann, D.; Badura, J.; Becker, H.; Fahrer, J.; Kaina, B. Sensitivity of CD3/CD28-stimulated versus non-stimulated lymphocytes to ionizing radiation and genotoxic anticancer drugs: Key role of ATM in the differential radiation response. Cell Death Dis. 2018, 9, 1053. [Google Scholar] [CrossRef] [PubMed]
- Russ, S.; Chambers, H.; Scott, G.; Mottram, J. Experimental studies with small doses of X-rays. Lancet 1919, 193, 692–695. [Google Scholar] [CrossRef] [Green Version]
- Tortora, G.J.; Derrickson, B.H. Principles of Anatomy and Physiology, 14th ed.; Wiley: New York, NY, USA, 2013. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Variables | OS | PFS | LPFS | |||
|---|---|---|---|---|---|---|
| HR (95% CI) | p | HR (95% CI) | p | HR (95% CI) | p | |
| Prescription dose: cont. | 1.31 (1.04, 1.67) | 0.01 | 1.22 (0.98, 1.51) | 0.07 | 1.34 (1.07–1.67) | 0.01 |
| Actual received dose: cont. | 1.22 (0.95, 1.56) | 0.10 | 1.21 (0.98, 1.50) | 0.08 | 1.32 (1.05, 1.65) | 0.017 |
| Age: cont. | 1.01 (0.99, 1.02) | 0.24 | 0.997 (0.99, 1.009) | 0.59 | 1.01 (0.99, 1.02) | 0.26 |
| Gender: Male (RL) vs. Female | 0.83 (0.65, 1.06) | 0.13 | 0.96 (0.77, 1.19) | 0.71 | 0.88 (0.70, 1.10) | 0.27 |
| Zubrod status: 0 (RL) vs. 1 | 1.02 (0.80, 1.30) | 0.86 | 0.95 (0.76, 1.18) | 0.64 | 1.01 (0.81, 1.27) | 0.91 |
| Histology: Non-Sq (RL) vs. Sq | 1.13 (0.88, 1.43) | 0.34 | 1.02 (0.82, 1.26) | 0.87 | 1.19 (0.95, 1.49) | 0.12 |
| Smoking history: Yes (RL) vs. No | 0.72 (0.43, 1.21) | 0.22 | 0.79 (0.50, 1.26) | 0.32 | 0.80 (0.50, 1.30) | 0.37 |
| RT technique: 3D (RL) vs. IMRT | 0.89 (0.70, 1.13) | 0.33 | 1.04 (0.84, 1.28) | 0.74 | 1.06 (0.84, 1.32) | 0.64 |
| PET staging: No (RL) vs. Yes | 0.76 (0.52, 1.11) | 0.16 | 0.87 (0.61, 1.24) | 0.45 | 0.83 (0.58, 1.21) | 0.34 |
| AJCC stage: IIIA (RL) vs. IIIB | 1.03 (0.80, 1.32) | 0.82 | 1.08 (0.86, 1.35) | 0.52 | 1.08 (0.86, 1.37) | 0.49 |
| Tumor location: Not LLL/central (RL) vs. LLL/central | 1.49 (1.06, 2.09) | 0.02 | 1.21 (0.88, 1.66) | 0.25 | 1.33 (0.95, 1.84) | 0.09 |
| Esophagitis grade: <3 (RL) vs. ≥3 | 1.77 (1.30, 2.41) | 0.0003 | 1.72 (1.29, 2.28) | 0.0002 | 1.53 (1/14. 2.06) | 0.005 |
| Received full chemo: No (RL) vs. Yes | 0.64 (0.46, 0.90) | 0.009 | 0.72 (0.53, 0.97) | 0.03 | 0.70 (0.51, 0.97) | 0.03 |
| GTV: cont. | 1.21 (1.07, 1.38) | 0.0026 | 1.13 (1.01, 1.26) | 0.03 | 1.13 (1.01, 1.27) | 0.04 |
| Mean lung dose: cont. | 1.05 (1.02, 1.09) | 0.0004 | 1.04 (1.01, 1.07) | 0.003 | 1.03 (1.004, 1.06) | 0.02 |
| Mean heart dose: cont. | 1.02 (1.01, 1.03) | <0.0001 | 1.01 (1.003, 1.02) | 0.004 | 1.02 (1.007, 1.03) | 0.0007 |
| Integral total dose: cont. | 1.003 (1.001, 1.005) | 0.0004 | 1.001 (1.00, 1.003) | 0.11 | 1.002 (1.00, 1.003) | 0.03 |
| EDIC: cont. | 1.18 (1.10, 1.26) | <0.0001 | 1.10 (1.03, 1.16) | 0.002 | 1.11 (1.05, 1.18) | 0.0009 |
| (a) | ||||
|---|---|---|---|---|
| Variables | OS without EDIC | OS with EDIC | ||
| HR (95% CI) | p | HR (95% CI) | p | |
| Tumor location | 1.42 (0.98, 2.05) | 0.07 | 1.41 (0.98, 2.02) | 0.07 |
| Gross tumor volume | 1.16 (1.00, 1.34) | 0.05 | 1.12 (0.98, 1.28) | 0.09 |
| Esophagitis grade | 1.53 (1.11, 2.11) | 0.01 | 1.52 (1.10, 2.10) | 0.012 |
| Received full chemo | 0.58 (0.41, 0.81) | 0.0015 | 0.59 (0.42, 0.83) | 0.003 |
| Mean lung dose | 1.03 (0.998, 1.070) | 0.07 | ||
| Mean heart dose | 1.008 (0.995, 1.022) | 0.21 | ||
| Integral total dose | 1.000 (0.998, 1.002) | 0.93 | ||
| EDIC | 1.12 (1.03, 1.21) | 0.005 | ||
| (b) | ||||
| Variables | PFS without EDIC | PFS with EDIC | ||
| HR (95% CI) | p | HR (95% CI) | p | |
| Tumor location | 1.19 (0.84, 1.68) | 0.33 | 1.20 (0.85, 1.68) | 0.30 |
| Gross tumor volume | 1.15 (1.01, 1.32) | 0.04 | 1.08 (0.96, 1.21) | 0.20 |
| Esophagitis grade | 1.64 (1.22, 2.21) | 0.001 | 1.60 (1.19, 2.15) | 0.002 |
| Received full chemo | 0.63 (0.46, 0.86) | 0.003 | 0.66 (0.49, 0.90) | 0.009 |
| Mean lung dose | 1.04 (1.006, 1.071) | 0.02 | ||
| Mean heart dose | 1.005 (0.992, 1.017) | 0.47 | ||
| Integral total dose | 0.998 (0.996, 1.000) | 0.10 | ||
| EDIC | 1.05 (0.98, 1.12) | 0.17 | ||
| (c) | ||||
| Variables | LPFS without EDIC | LPFS with EDIC | ||
| HR (95% CI) | p | HR (95% CI) | p | |
| Gross tumor volume | 1.10 (0.96, 1.26) | 0.16 | 1.07 (0.95, 1.20) | 0.29 |
| Esophagitis grade | 1.36 (1.00, 1.85) | 0.05 | 1.37 (1.00, 1.86) | 0.05 |
| Received full chemo | 0.66 (0.48, 0.91) | 0.012 | 0.67 (0.48, 0.92) | 0.013 |
| Mean lung dose | 1.01 (0.98, 1.04) | 0.48 | ||
| Mean heart dose | 1.012 (1.000, 1.024) | 0.044 | ||
| Integral total dose | 1.00 (0.998, 1.002) | 0.81 | ||
| EDIC | 1.09 (1.01, 1.16) | 0.02 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jin, J.-Y.; Hu, C.; Xiao, Y.; Zhang, H.; Paulus, R.; Ellsworth, S.G.; Schild, S.E.; Bogart, J.A.; Dobelbower, M.C.; Kavadi, V.S.; et al. Higher Radiation Dose to the Immune Cells Correlates with Worse Tumor Control and Overall Survival in Patients with Stage III NSCLC: A Secondary Analysis of RTOG0617. Cancers 2021, 13, 6193. https://doi.org/10.3390/cancers13246193
Jin J-Y, Hu C, Xiao Y, Zhang H, Paulus R, Ellsworth SG, Schild SE, Bogart JA, Dobelbower MC, Kavadi VS, et al. Higher Radiation Dose to the Immune Cells Correlates with Worse Tumor Control and Overall Survival in Patients with Stage III NSCLC: A Secondary Analysis of RTOG0617. Cancers. 2021; 13(24):6193. https://doi.org/10.3390/cancers13246193
Chicago/Turabian StyleJin, Jian-Yue, Chen Hu, Ying Xiao, Hong Zhang, Rebecca Paulus, Susannah G. Ellsworth, Steven E. Schild, Jeffrey A. Bogart, Michael Chris Dobelbower, Vivek S. Kavadi, and et al. 2021. "Higher Radiation Dose to the Immune Cells Correlates with Worse Tumor Control and Overall Survival in Patients with Stage III NSCLC: A Secondary Analysis of RTOG0617" Cancers 13, no. 24: 6193. https://doi.org/10.3390/cancers13246193