
Tumor-Infiltrating Lymphocytes and Cancer Markers in Osteosarcoma: Influence on Patient Survival

 , ,
, , 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Tissue Samples
2.2. Immunohistochemical (IHC) Staining
2.3. Histomorphometry
2.4. Data Analysis
3. Results
3.1. Identification of Tumor-Infiltrating Lymphocytes in Osteosarcoma
3.2. Expression of Tumor Markers in Osteosarcoma
3.3. Tumor-Infiltrating CD4 + Cells—A Protective Factor in Osteosarcoma
3.4. OS and PFS Correlated with Infiltrating CD8+ T Cells in OST Patients
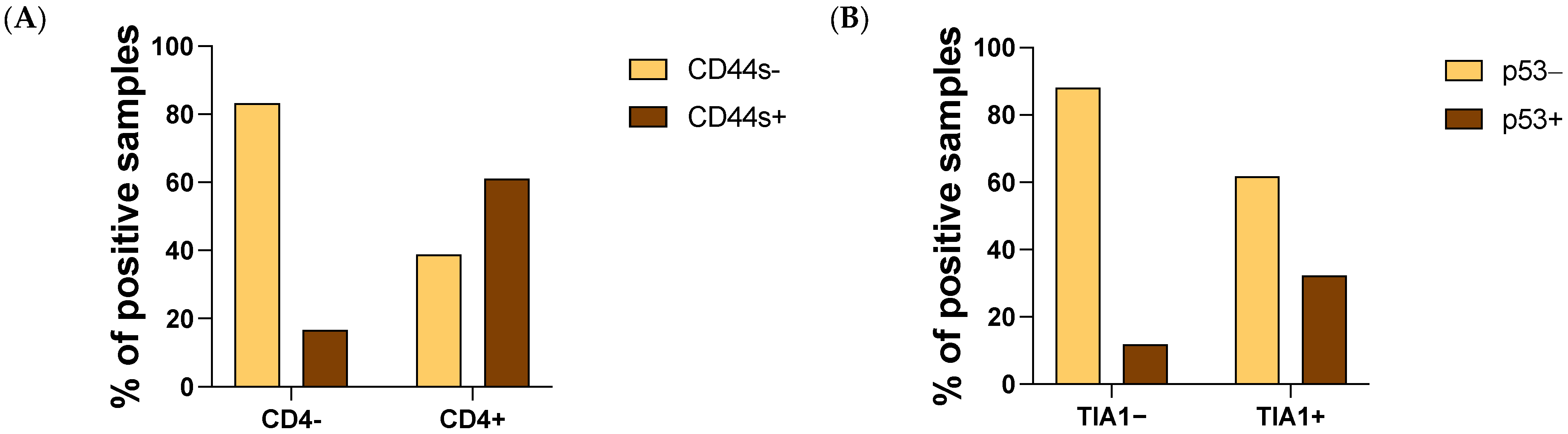
3.5. CD4 T Cells and Tumoral CD44s Expression Were Strongly Associated in OST
3.6. The Influence of Sex, Age, Localization and Neoadjuvant Chemotherapy on the Microenvironment of Tumors in OST Patients
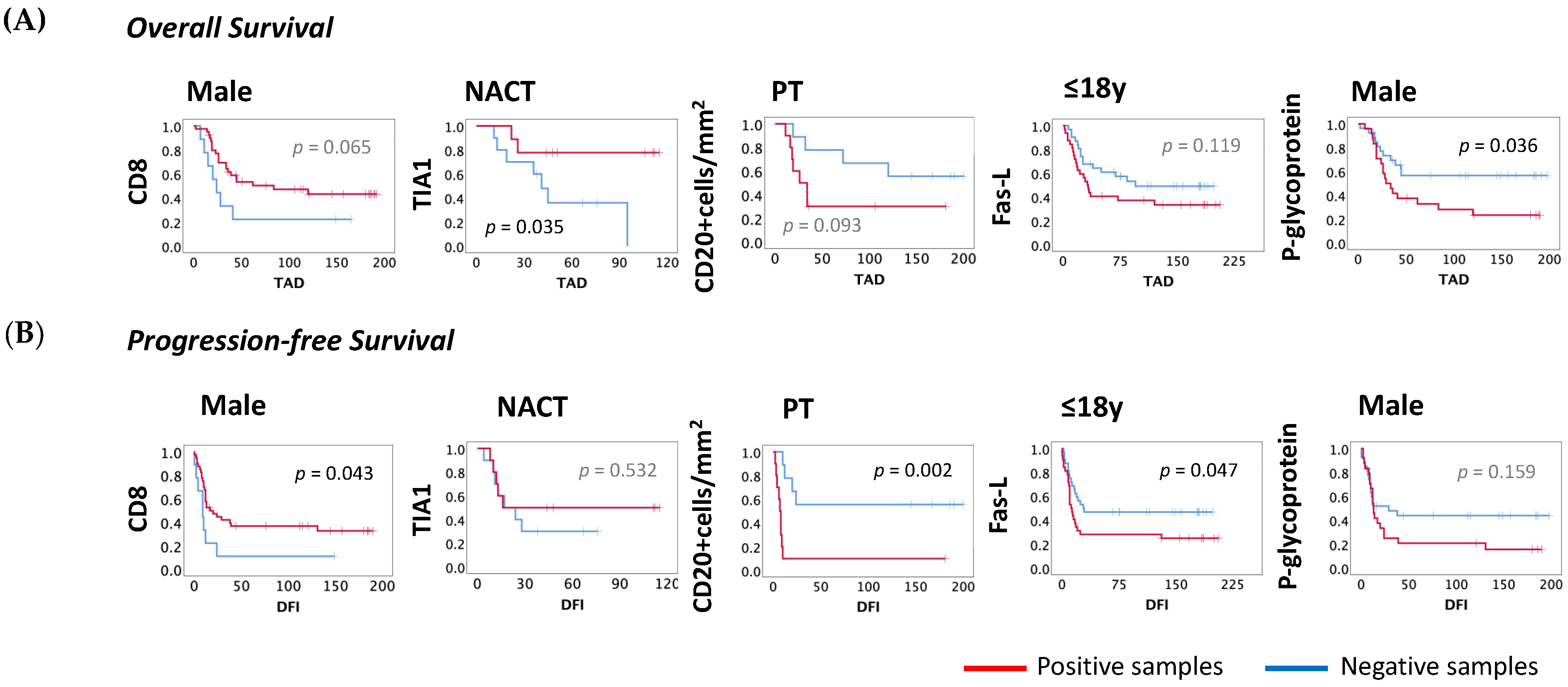
3.7. The Influence of Sex, Age, Localization and Neoadjuvant Chemotherapy on Survival
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kansara, M.; Teng, M.W.; Smyth, M.J.; Thomas, D.M. Translational biology of osteosarcoma. Nat. Rev. Cancer 2014, 14, 722–735. [Google Scholar] [CrossRef] [PubMed]
- Tang, H.; Tang, Z.; Jiang, Y.; Wei, W.; Lu, J. Pathological and therapeutic aspects of matrix metalloproteinases: Implications in osteosarcoma. Asia Pac. J. Clin. Oncol. 2019, 15, 218–224. [Google Scholar] [CrossRef] [Green Version]
- Casali, P.G.; Bielack, S.; Abecassis, N.; Aro, H.T.; Bauer, S.; Biagini, R.; Bonvalot, S.; Boukovinas, I.; Bovee, J.V.M.G.; Brennan, B.; et al. ESMO Guidelines Committee, PaedCan and ERN EURACAN. Bone sarcomas: ESMO-PaedCan-EURACAN Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2018, 29, iv79–iv95. [Google Scholar] [CrossRef] [PubMed]
- Geller, D.S.; Gorlick, R. Osteosarcoma: A review of diagnosis, management, and treatment strategies. Clin. Adv. Hematol. Oncol. 2010, 8, 705–718, PMID: 21317869. [Google Scholar] [PubMed]
- Lindsey, B.A.; Markel, J.E.; Kleinerman, E.S. Osteosarcoma Overview. Rheumatol. Ther. 2017, 4, 25–43. [Google Scholar] [CrossRef] [Green Version]
- Durfee, R.A.; Mohammed, M.; Luu, H.H. Review of Osteosarcoma and Current Management. Rheumatol. Ther. 2016, 3, 221–243. [Google Scholar] [CrossRef] [Green Version]
- ICGC/TCGA Pan-Cancer Analysis of Whole Genomes Consortium. Pan-cancer analysis of whole genomes. Nature 2020, 578, 82–93. [Google Scholar] [CrossRef] [Green Version]
- Cortés-Ciriano, I.; Lee, J.J.; Xi, R.; Jain, D.; Jung, Y.L.; Yang, L.; Gordenin, D.; Klimczak, L.J.; Zhang, C.Z.; Pellman, D.S.; et al. Comprehensive analysis of chromothripsis in 2658 human cancers using whole-genome sequencing. Nat. Genet. 2020, 52, 331–341. [Google Scholar] [CrossRef] [Green Version]
- Xu, H.; Zhu, X.; Bao, H.; Wh Shek, T.; Huang, Z.; Wang, Y.; Wu, X.; Wu, Y.; Chang, Z.; Wu, S.; et al. Genetic and clonal dissection of osteosarcoma progression and lung metastasis. Int. J. Cancer 2018, 143, 1134–1142. [Google Scholar] [CrossRef]
- Chen, C.; Xie, L.; Ren, T.; Huang, Y.; Xu, J.; Guo, W. Immunotherapy for osteosarcoma: Fundamental mechanism, rationale, and recent breakthroughs. Cancer Lett. 2021, 500, 1–10. [Google Scholar] [CrossRef]
- Kelleher, F.C.; O′Sullivan, H. Monocytes, Macrophages and Osteoclasts in Osteosarcoma. J. Adolesc. Young Adult Oncol. 2017, 6, 396–405. [Google Scholar] [CrossRef]
- Cortini, M.; Avnet, S.; Baldini, N. Mesenchymal stroma: Role in osteosarcoma progression. Cancer Lett. 2017, 405, 90–99. [Google Scholar] [CrossRef] [PubMed]
- Heymann, M.F.; Lézot, F.; Heymann, D. The contribution of immune infiltrates and the local microenvironment in the pathogenesis of osteosarcoma. Cell. Immunol. 2019, 343, 103711. [Google Scholar] [CrossRef]
- Koirala, P.; Roth, M.E.; Gill, J.; Piperdi, S.; Chinai, J.M.; Geller, D.S.; Hoang, B.H.; Park, A.; Fremed, M.A.; Zang, X.; et al. Immune infiltration and PD-L1 expression in the tumor microenvironment are prognostic in osteosarcoma. Sci. Rep. 2016, 6, 30093. [Google Scholar] [CrossRef]
- Sundara, Y.T.; Kostine, M.; Cleven, A.H.; Bovée, J.V.; Schilham, M.W.; Cleton-Jansen, A.M. Increased PD-L1 and T-cell infiltration in the presence of HLA class I expression in metastatic high-grade osteosarcoma: A rationale for T-cell-based immunotherapy. Cancer Immunol. Immunother. 2017, 66, 119–128. [Google Scholar] [CrossRef] [Green Version]
- Mori, K.; Rédini, F.; Gouin, F.; Cherrier, B.; Heymann, D. Osteosarcoma: Current status of immunotherapy and future trends (Review). Oncol. Rep. 2006, 15, 693–700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, B.; Huang, Y.; Sun, Y.; Zhang, J.; Yao, Y.; Shen, Z.; Xiang, D.; He, A. Prognostic value of inflammation-based scores in patients with osteosarcoma. Sci. Rep. 2016, 6, 39862. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, T.; Fang, X.C.; Ding, Z.; Sun, Z.G.; Sun, L.M.; Wang, Y.L. Pre-operative lymphocyte-to monocyte ratio as a predictor of overall survival in patients suffering from osteosarcoma. FEBS Open Bio 2015, 5, 682–687. [Google Scholar] [CrossRef] [Green Version]
- Hu, C.; Liu, C.; Tian, S.; Wang, Y.; Shen, R.; Rao, H.; Li, J.; Yang, X.; Chen, B.; Ye, L. Comprehensive analysis of prognostic tumor microenvironment-related genes in osteosarcoma patients. BMC Cancer 2020, 20, 814. [Google Scholar] [CrossRef]
- Liu, W.; Xie, X.; Qi, Y.; Wu, J. Exploration of Immune-Related Gene Expression in Osteosarcoma and Association with Outcomes. JAMA Netw. Open 2021, 4, e2119132. [Google Scholar] [CrossRef]
- Wang, X.; Wang, L.; Xu, W.; Wang, X.; Ke, D.; Lin, J.; Lin, W.; Bai, X. Classification of Osteosarcoma Based on Immunogenomic Profiling. Front. Cell Dev. Biol. 2021, 9, 696878. [Google Scholar] [CrossRef] [PubMed]
- Yang, M.; Cao, Y.; Wang, Z.; Zhang, T.; Hua, Y.; Cai, Z. Identification of two immune subtypes in osteosarcoma based on immune gene sets. Int. Immunopharmacol. 2021, 96, 107799. [Google Scholar] [CrossRef]
- He, L.; Yang, H.; Huang, J. The tumor immune microenvironment and immune-related signature predict the chemotherapy response in patients with osteosarcoma. BMC Cancer 2021, 2, 581. [Google Scholar] [CrossRef]
- Dunn, G.P.; Old, L.J.; Schreiber, R.D. The immunobiology of cancer immunosurveillance and immunoediting. Immunity 2004, 21, 137–148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, W.M.; Gibson, S.J.; Facer, P.; Gu, J.; Polak, J.M. Improved section adhesion for immunocytochemistry using high molecular weight polymers of L-lysine as a slide coating. Histochemistry 1983, 77, 275–279. [Google Scholar] [CrossRef]
- Baldini, N.; Scotlandi, K.; Barbanti-Bròdano, G.; Manara, M.C.; Maurici, D.; Bacci, G.; Bertoni, F.; Picci, P.; Sottili, S.; Campanacci, M.; et al. Expression of P-glycoprotein in high-grade osteosarcomas in relation to clinical outcome. N. Engl. J. Med. 1995, 333, 1380–1385. [Google Scholar] [CrossRef]
- ClustVis: A Web Tool for Visualizing Clustering of Multivariate Data (BETA). Available online: https://biit.cs.ut.ee/clustvis (accessed on 26 October 2021).
- Metsalu, T.; Vilo, J. ClustVis: A web tool for visualizing clustering of multivariate data using Principal Component Analysis and heatmap. Nucleic Acids Res. 2015, 43, W566–W570. [Google Scholar] [CrossRef]
- Théoleyre, S.; Mori, K.; Cherrier, B.; Passuti, N.; Gouin, F.; Rédini, F.; Heymann, D. Phenotypic and functional analysis of lymphocytes infiltrating osteolytic tumors: Use as a possible therapeutic approach of osteosarcoma. BMC Cancer 2005, 5, 123. [Google Scholar] [CrossRef]
- Fritzsching, B.; Fellenberg, J.; Moskovszky, L.; Sápi, Z.; Krenacs, T.; Machado, I.; Poeschl, J.; Lehner, B.; Szendrõi, M.; Bosch, A.L.; et al. CD8+/FOXP3+-ratio in osteosarcoma microenvironment separates survivors from non-survivors: A multicenter validated retrospective study. Oncoimmunology 2015, 4, e990800. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alves, P.M.; de Arruda, J.A.A.; Arantes, D.A.C.; Costa, S.F.S.; Souza, L.L.; Pontes, H.A.R.; Fonseca, F.P.; Mesquita, R.A.; Nonaka, C.F.W.; Mendonça, E.F.; et al. Evaluation of tumor-infiltrating lymphocytes in osteosarcomas of the jaws: A multicenter study. Virchows Arch. 2019, 474, 201–207. [Google Scholar] [CrossRef]
- Song, Y.J.; Xu, Y.; Zhu, X.; Fu, J.; Deng, C.; Chen, H.; Xu, H.; Song, G.; Lu, J.; Tang, Q.; et al. Immune Landscape of the Tumor Microenvironment Identifies Prognostic Gene Signature CD4/CD68/CSF1R in Osteosarcoma. Front. Oncol. 2020, 10, 1198. [Google Scholar] [CrossRef]
- Sun, C.Y.; Zhang, Z.; Tao, L.; Xu, F.F.; Li, H.Y.; Zhang, H.Y.; Liu, W. T cell exhaustion drives osteosarcoma pathogenesis. Ann. Transl. Med. 2021, 18, 1447. [Google Scholar] [CrossRef]
- Gomez-Brouchet, A.; Illac, C.; Gilhodes, J.; Bouvier, C.; Aubert, S.; Guinebretiere, J.M.; Marie, B.; Larousserie, F.; Entz-Werlé, N.; de Pinieux, G.; et al. CD163-positive tumor-associated macrophages and CD8-positive cytotoxic lymphocytes are powerful diagnostic markers for the therapeutic stratification of osteosarcoma patients: An immunohistochemical analysis of the biopsies from the French OS2006 phase 3 trial. Oncoimmunology 2017, 6, e1331193. [Google Scholar] [CrossRef] [PubMed]
- Waghray, D.; Zhang, Q. Inhibit or Evade Multidrug Resistance P-Glycoprotein in Cancer Treatment. J. Med. Chem. 2018, 61, 5108–5121. [Google Scholar] [CrossRef] [PubMed]
- He, C.; Sun, Z.; Hoffman, R.M.; Yang, Z.; Jiang, Y.; Wang, L.; Hao, Y. P-Glycoprotein Overexpression Is Associated with Cisplatin Resistance in Human Osteosarcoma. Anticancer Res. 2019, 39, 1711–1718. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumta, S.M.; Zhu, Q.S.; Lee, K.M.; Griffith, J.; Chow, L.T.; Leung, P.C. Clinical significance of P-glycoprotein immunohistochemistry and doxorubicin binding assay in patients with osteosarcoma. Int. Orthop. 2001, 25, 279–282. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.; Liu, X.; Yang, S. MicroRNA-221 Upregulates the Expression of P-gp and Bcl-2 by Activating the Stat3 Pathway to Promote Doxorubicin Resistance in Osteosarcoma Cells. Biol. Pharm. Bull. 2021, 44, 861–868. [Google Scholar] [CrossRef]
- Gao, Y.; Liao, Y.; Shen, J.K.; Feng, Y.; Choy, E.; Cote, G.; Harmon, D.; Mankin, H.J.; Hornicek, F.J.; Duan, Z. Evaluation of P-glycoprotein (Pgp) expression in human osteosarcoma by high-throughput tissue microarray. J. Orthop. Res. 2016, 34, 1606–1612. [Google Scholar] [CrossRef]
- Hornicek, F.J.; Gebhardt, M.C.; Wolfe, M.W.; Kharrazi, F.D.; Takeshita, H.; Parekh, S.G.; Zurakowski, D.; Mankin, H.J. P-glycoprotein levels predict poor outcome in patients with osteosarcoma. Clin. Orthop. Relat. Res. 2000, 373, 11–17. [Google Scholar] [CrossRef]
- Poulaki, V.; Mitsiades, C.S.; Mitsiades, N. The role of Fas and FasL as mediators of anticancer chemotherapy. Drug Resist. Updat. 2001, 4, 233–242. [Google Scholar] [CrossRef]
- Lafleur, E.A.; Koshkina, N.V.; Stewart, J.; Jia, S.F.; Worth, L.L.; Duan, X.; Kleinerman, E.S. Increased Fas expression reduces the metastatic potential of human osteosarcoma cells. Clin. Cancer Res. 2004, 10, 8114–8119. [Google Scholar] [CrossRef] [Green Version]
- Gordon, N.; Kleinerman, E.S. The role of Fas/FasL in the metastatic potential of osteosarcoma and targeting this pathway for the treatment of osteosarcoma lung metastases. Cancer Treat. Res. 2009, 152, 497–508. [Google Scholar] [CrossRef]
- Xu, L.; Xia, C.; Sun, Q.; Sheng, F.; Xiong, J.; Wang, S. Variants of FasL and ABCC5 are predictive of outcome after chemotherapy-based treatment in osteosarcoma. J. Bone Oncol. 2018, 12, 44–48. [Google Scholar] [CrossRef]
- Koshkina, N.; Yang, Y.; Kleinerman, E.S. The Fas/FasL Signaling Pathway: Its Role in the Metastatic Process and as a Target for Treating Osteosarcoma Lung Metastases. Adv. Exp. Med. Biol. 2020, 1258, 177–187. [Google Scholar] [CrossRef]
- Seiter, S.; Tilgen, W.; Herrmann, K.; Schadendorf, D.; Patzelt, E.; Möller, P.; Zöller, M. Expression of CD44 splice variants in human skin and epidermal tumours. Virchows Arch. 1996, 428, 141–149. [Google Scholar] [CrossRef]
- Picker, L.J.; Nakache, M.; Butcher, E.C. Monoclonal antibodies to human lymphocyte homing receptors define a novel class of adhesion molecules on diverse cell types. J. Cell Biol. 1989, 109, 927–937. [Google Scholar] [CrossRef] [PubMed]
- Afify, A.; Purnell, P.; Nguyen, L. Role of CD44s and CD44v6 on human breast cancer cell adhesion, migration, and invasion. Exp. Mol. Pathol. 2009, 86, 95–100. [Google Scholar] [CrossRef]
- Xiao, Z.; Wan, J.; Nur, A.A.; Dou, P.; Mankin, H.; Liu, T.; Ouyang, Z. Targeting CD44 by CRISPR-Cas9 in Multi-Drug Resistant Osteosarcoma Cells. Cell Physiol. Biochem. 2018, 51, 1879–1893. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.; Feng, Y.; Shen, J.K.; Lin, M.; Choy, E.; Cote, G.M.; Harmon, D.C.; Mankin, H.J.; Hornicek, F.J.; Duan, Z. CD44 is a direct target of miR-199a-3p and contributes to aggressive progression in osteosarcoma. Sci. Rep. 2015, 5, 11365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Y.; Ding, C.; Wang, J.; Sun, G.; Cao, Y.; Xu, L.; Zhou, L.; Chen, X. Prognostic significance of CD44V6 expression in osteosarcoma: A meta-analysis. J. Orthop. Surg. Res. 2015, 10, 187. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.S.; Park, Y.B.; Oh, J.H.; Jeong, J.; Kim, C.J.; Lee, S.H. Expression of CD44 isoforms correlates with the metastatic potential of osteosarcoma. Clin. Orthop. Relat. Res. 2002, 396, 184–190. [Google Scholar] [CrossRef] [PubMed]
- Felgar, R.E.; Macon, W.R.; Kinney, M.C.; Roberts, S.; Pasha, T.; Salhany, K.E. TIA-1 expression in lymphoid neoplasms. Identification of subsets with cytotoxic T lymphocyte or natural killer cell differentiation. Am. J. Pathol. 1997, 150, 1893–1900. [Google Scholar] [PubMed]
- Palmerini, E.; Agostinelli, C.; Picci, P.; Pileri, S.; Marafioti, T.; Lollini, P.L.; Scotlandi, K.; Longhi, A.; Benassi, M.S.; Ferrari, S. Tumoral immune-infiltrate (IF), PD-L1 expression and role of CD8/TIA-1 lymphocytes in localized osteosarcoma patients treated within protocol ISG-OS1. Oncotarget 2017, 8, 111836–111846. [Google Scholar] [CrossRef] [Green Version]
- Velletri, T.; Xie, N.; Wang, Y.; Huang, Y.; Yang, Q.; Chen, X.; Chen, Q.; Shou, P.; Gan, Y.; Cao, G.; et al. P53 functional abnormality in mesenchymal stem cells promotes osteosarcoma development. Cell Death Dis. 2016, 7, e2015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ueda, Y.; Dockhorn-Dworniczak, B.; Blasius, S.; Mellin, W.; Wuisman, P.; Böcker, W.; Roessner, A. Analysis of mutant P53 protein in osteosarcomas and other malignant and benign lesions of bone. J. Cancer Res. Clin. Oncol. 1993, 119, 172–178. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic, Unit | N (%) | Mean (95% CI) |
|---|---|---|
| Samples | 93 | |
| Sex (proportion female) | 39 (41.9%) | |
| Age, years | 18 (17–21) | |
| ≤18 | 65 (70.0%) | |
| >18 | 28 (30.0%) | |
| Localization | ||
| Distal Femur | 62 (66.7%) | |
| Proximal Tibia | 31 (33.3%) | |
| Neoadjuvant Chemotherapy | 20 (21.5%) | |
| Metastasis | 57 (61.3%) | |
| TAD, months | 103 (85–122) | |
| DFI, months | 83 (64–103) |
| Markers | Mortality | Metastization | |||||
|---|---|---|---|---|---|---|---|
| Fisher’s Exact Test | OR | 95% CI | Fisher’s Exact Test | OR | 95% CI | ||
| Tumor-Infiltrating Lymphocytes | CD3 | 0.503 | 0.514 | 0.124–2.138 | 0.734 | 0.623 | 0.150–2.587 |
| CD4 | 0.028 | 0.256 | 0.081–0.806 | 0.177 | 0.433 | 0.152–1.232 | |
| CD8 | 0.183 | 0.420 | 0.135–1.305 | 0.199 | 0.456 | 0.149–1.391 | |
| TIA1 | 0.656 | 0.812 | 0.332–1.986 | 1.000 | 1.056 | 0.434–2.566 | |
| CD20 | 1.000 | 0.995 | 0.417–2.377 | 0.385 | 1.529 | 0.649–3.604 | |
| Tumor Markers | CD44s | 0.226 | 0.526 | 0.201–1.380 | 0.806 | 0.805 | 0.309–2.099 |
| CD44v6 | 1.000 | 1.190 | 0.346–4.093 | 0.756 | 1.391 | 0.386–5.015 | |
| CD95/Fas | 0.105 | 0.305 | 0.073–1.269 | 0.509 | 0.620 | 0.166–2.136 | |
| Fas-L | 0.386 | 1.602 | 0.681–3.768 | 0.289 | 1.624 | 0.693–3.806 | |
| p53 | 0.163 | 0.405 | 0.133–1.236 | 0.271 | 0.500 | 0.173–1.447 | |
| P-glycoprotein | 0.088 | 2.210 | 0.939–5.197 | 0.201 | 1.874 | 0.802–4.379 | |
| Markers | Overall Survival | Progression-Free Survival | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Log-Rank Test | TAD (Months) | HR Exp (B) (pos) | Log-Rank Test | DFI (Months) | HR Exp (B) (pos) | ||||
| neg | pos | neg | pos | ||||||
| Tumor-Infiltrating Lymphocytes | CD3 | 0.201 | 74 | 107 | 0.60 | 0.414 | 66 | 87 | 0.723 |
| CD4 | 0.073 | 94 | 149 | 0.441 | 0.744 | 75 | 114 | 0.590 | |
| CD8 | 0.043 | 61 | 112 | 0.526 | 0.049 | 39 | 91 | 0.561 | |
| TIA1 | 0.794 | 103 | 108 | 0.922 | 0.631 | 85 | 81 | 1.143 | |
| CD20 | 0.773 | 103 | 103 | 0.919 | 0.678 | 89 | 77 | 1.120 | |
| Tumor Markers | CD44s | 0.361 | 100 | 115 | 0.725 | 0.369 | 80 | 92 | 0.756 |
| CD44v6 | 0.389 | 106 | 94 | 1.419 | 0.368 | 86 | 73 | 1.403 | |
| CD95/Fas | 0.084 | 99 | 150 | 0.373 | 0.320 | 81 | 104 | 0.634 | |
| Fas-L | 0.154 | 115 | 94 | 1.513 | 0.158 | 93 | 75 | 1.459 | |
| p53 | 0.200 | 98 | 127 | 0.577 | 0.299 | 76 | 105 | 0.678 | |
| P-glycoprotein | 0.081 | 117 | 87 | 1.638 | 0.258 | 93 | 71 | 1.344 | |
| TIL | Molecule | Pearson Chi-Square | Phi Coefficient | Effect Size |
|---|---|---|---|---|
| CD4 | CD44s | 0.000 | 0.408 | Strong |
| TIA1 | p53 | 0.019 | 0.248 | Moderate |
| CD20 | p53 | 0.076 | 0.188 | Weak |
| CD8 | CD44s | 0.086 | 0.182 | Weak |
| TIA1 | CD44s | 0.087 | 0.180 | Weak |
| CD4 | CD95/Fas | 0.089 | 0.178 | Weak |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Casanova, J.M.; Almeida, J.-S.; Reith, J.D.; Sousa, L.M.; Fonseca, R.; Freitas-Tavares, P.; Santos-Rosa, M.; Rodrigues-Santos, P. Tumor-Infiltrating Lymphocytes and Cancer Markers in Osteosarcoma: Influence on Patient Survival. Cancers 2021, 13, 6075. https://doi.org/10.3390/cancers13236075
Casanova JM, Almeida J-S, Reith JD, Sousa LM, Fonseca R, Freitas-Tavares P, Santos-Rosa M, Rodrigues-Santos P. Tumor-Infiltrating Lymphocytes and Cancer Markers in Osteosarcoma: Influence on Patient Survival. Cancers. 2021; 13(23):6075. https://doi.org/10.3390/cancers13236075
Chicago/Turabian StyleCasanova, José Manuel, Jani-Sofia Almeida, John David Reith, Luana Madalena Sousa, Ruben Fonseca, Paulo Freitas-Tavares, Manuel Santos-Rosa, and Paulo Rodrigues-Santos. 2021. "Tumor-Infiltrating Lymphocytes and Cancer Markers in Osteosarcoma: Influence on Patient Survival" Cancers 13, no. 23: 6075. https://doi.org/10.3390/cancers13236075