
Radiological Patterns of Uveal Melanoma Liver Metastases in Correlation to Genetic Status

 , , , , , ,
, , , , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Inclusion
2.2. Analyses of Metastasis Imaging
2.3. Material and Genetic Analyses
2.4. Statistical Analysis
3. Results
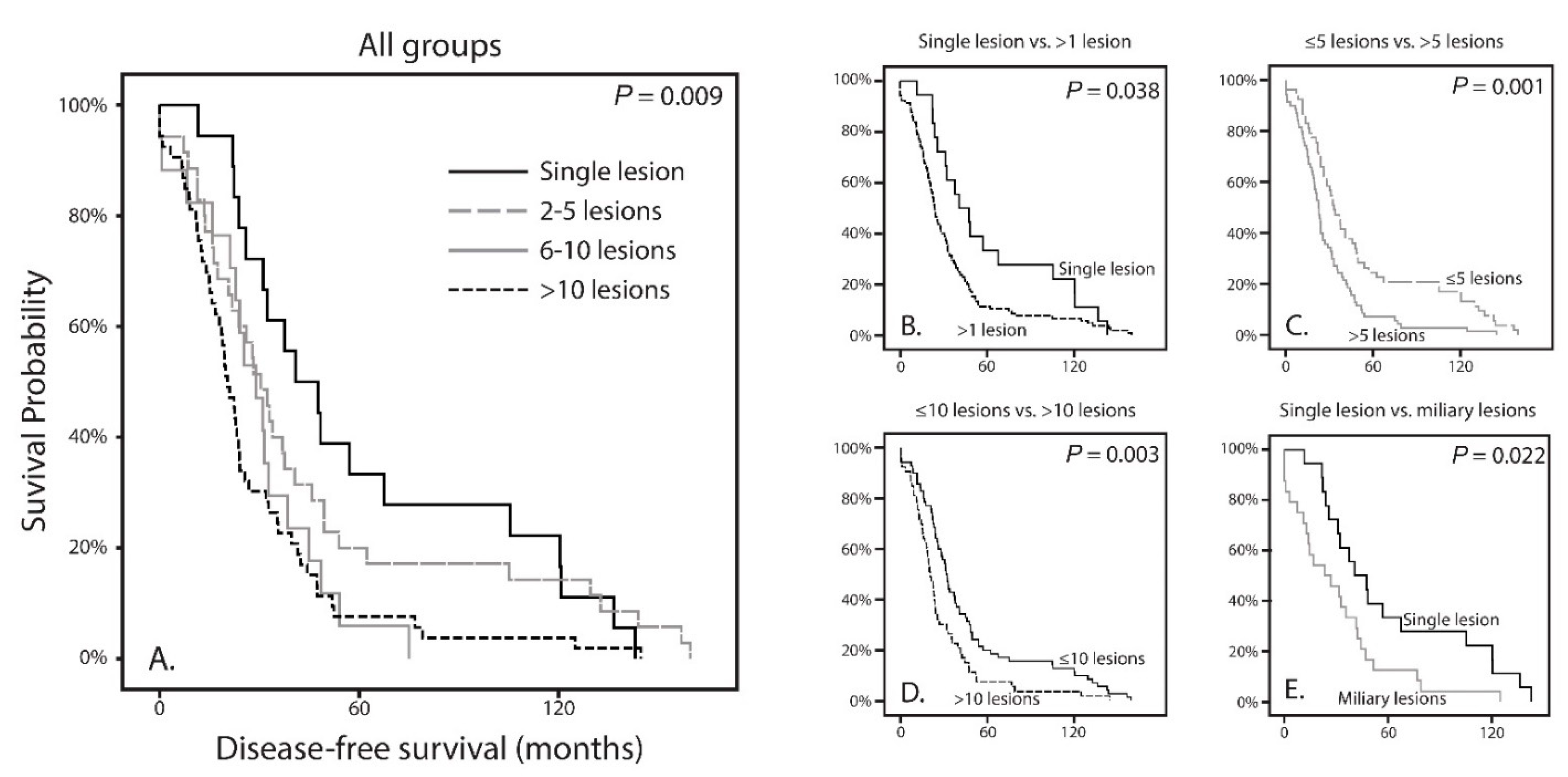
3.1. Survival Analysis
3.2. Correlation with Clinical, Histopathological and Genetic Features of the Primary Tumor
3.3. Differences between Solitary Metastases and Miliary Metastases Pattern
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
List of Abbreviations
| ANOVA | Analysis of variance |
| BAP1 | BRCA1-associated Protein 1 |
| CT | Computed Tomography |
| CYSLTR2 | Cysteinyl Leukotriene Receptor 2 |
| DFS | Disease-free survival |
| EIF1AX | Eukaryotic Translation Initiation Factor 1A, X-linked |
| GEP | Gene Expression Profile |
| GNA11 | Guanine Nucleotide Binding Protein, subunit 11 |
| GNAQ | Guanine Nucleotide Binding Protein, subunit q |
| IHC | Immunohistochemistry |
| MRI | Magnetic Resonance Imaging |
| NRM | No Recurrent Mutation |
| PLCB4 | Phospholipase C Beta 4 |
| SF3B1 | Splicing Factor 3b subunit 1 |
| UM | Uveal Melanoma |
| UMmeta | Uveal Melanoma Metastases |
References
- Singh, A.D.; Turell, M.E.; Topham, A.K. Uveal Melanoma: Trends in Incidence, Treatment, and Survival. Ophthalmology 2011, 118, 1881–1885. [Google Scholar] [CrossRef]
- Hu, D.-N.; Yu, G.-P.; McCormick, S.A.; Schneider, S.; Finger, P.T. Population-Based Incidence of Uveal Melanoma in Various Races and Ethnic Groups. Am. J. Ophthalmol. 2005, 140, 612.e1–612.e8. [Google Scholar] [CrossRef] [PubMed]
- McLaughlin, C.C.; Wu, X.-C.; Jemal, A.; Martin, H.J.; Roche, L.M.; Chen, V.W. Incidence of noncutaneous melanomas in the U.S. Cancer 2005, 103, 1000–1007. [Google Scholar] [CrossRef] [PubMed]
- Kujala, E.; Ma¨kitie, T.; Kivelä, T. Very Long-Term Prognosis of Patients with Malignant Uveal Melanoma. Investig. Opthalmol. Vis. Sci. 2003, 44, 4651–4659. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yavuzyigitoglu, S.; Koopmans, A.E.; Verdijk, R.M.; Vaarwater, J.; Eussen, B.; van Bodegom, A.; Paridaens, D.; Kilic, E.; de Klein, A.; Rotterdam Ocular Melanoma Study, G. Uveal melanomas with sf3b1 mutations: A distinct subclass associated with late-onset metastases. Ophthalmology 2016, 123, 1118–1128. [Google Scholar] [CrossRef] [PubMed]
- Höglund, M.; Gisselsson, D.; Hansen, G.B.; White, V.A.; Säll, T.; Mitelman, F.; Horsman, D. Dissecting karyotypic patterns in malignant melanomas: Temporal clustering of losses and gains in melanoma karyotypic evolution. Int. J. Cancer 2003, 108, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Trolet, J.; Hupe, P.; Huon, I.; Lebigot, I.; Decraene, C.; Delattre, O.; Sastre-Garau, X.; Saule, S.; Thie´ry, J.-P.; Plancher, C.; et al. Genomic Profiling and Identification of High-Risk Uveal Melanoma by Array CGH Analysis of Primary Tumors and Liver Metastases. Investig. Opthalmol. Vis. Sci. 2009, 50, 2572–2580. [Google Scholar] [CrossRef]
- Koopmans, A.; Verdijk, R.M.; Brouwer, R.W.W.; Bosch, T.V.D.; Berg, M.M.P.V.D.; Vaarwater, J.; Kockx, C.; Paridaens, D.; Naus, N.C.; Nellist, M.; et al. Clinical significance of immunohistochemistry for detection of BAP1 mutations in uveal melanoma. Mod. Pathol. 2014, 27, 1321–1330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meir, T.; Dror, R.; Yu, X.; Qian, J.; Simon, I.; Pe’Er, J.; Chowers, I. Molecular Characteristics of Liver Metastases from Uveal Melanoma. Investig. Opthalmol. Vis. Sci. 2007, 48, 4890–4896. [Google Scholar] [CrossRef]
- Yavuzyigitoglu, S.; Drabarek, W.; Smit, K.N.; van Poppelen, N.; Koopmans, A.E.; Vaarwater, J.; Brands, T.; Eussen, B.; Dubbink, H.J.; van Riet, J.; et al. Correlation of Gene Mutation Status with Copy Number Profile in Uveal Melanoma. Ophthalmology 2017, 124, 573–575. [Google Scholar] [CrossRef]
- Griewank, K.; Van De Nes, J.; Schilling, B.; Moll, I.; Sucker, A.; Kakavand, H.; E Haydu, L.; Asher, M.; Zimmer, L.; Hillen, U.; et al. Genetic and clinico-pathologic analysis of metastatic uveal melanoma. Mod. Pathol. 2013, 27, 175–183. [Google Scholar] [CrossRef] [Green Version]
- Luscan, A.; A Just, P.; Briand, A.; Roziers, C.B.D.; Goussard, P.; Nitschké, P.; Vidaud, M.; Avril, M.F.; Terris, B.; Pasmant, E. Uveal melanoma hepatic metastases mutation spectrum analysis using targeted next-generation sequencing of 400 cancer genes. Br. J. Ophthalmol. 2014, 99, 437–439. [Google Scholar] [CrossRef] [Green Version]
- McCarthy, C.; Kalirai, H.; Lake, S.L.; Dodson, A.; Damato, B.E.; Coupland, S.E. Insights into Genetic Alterations of Liver Metastases from Uveal Melanoma. Pigment. Cell Melanoma Res. 2015, 29, 60–67. [Google Scholar] [CrossRef]
- Shain, A.H.; Bagger, M.M.; Yu, R.; Chang, D.; Liu, S.; Vemula, S.; Weier, J.F.; Wadt, K.; Heegaard, S.; Bastian, B.C.; et al. The genetic evolution of metastatic uveal melanoma. Nat. Genet. 2019, 51, 1123–1130. [Google Scholar] [CrossRef]
- Karlsson, J.; Nilsson, L.M.; Mitra, S.; Alsén, S.; Shelke, G.V.; Sah, V.R.; Forsberg, E.M.V.; Stierner, U.; All-Eriksson, C.; Einarsdottir, B.; et al. Molecular profiling of driver events in metastatic uveal melanoma. Nat. Commun. 2020, 11, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Durante, M.A.; Rodriguez, D.A.; Kurtenbach, S.; Kuznetsov, J.N.; Sanchez, M.I.; Decatur, C.L.; Snyder, H.; Feun, L.G.; Livingstone, A.S.; Harbour, J.W. Single-cell analysis reveals new evolutionary complexity in uveal melanoma. Nat. Commun. 2020, 11, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Nielsen, K.; Rolff, H.C.; Eefsen, R.L.; Vainer, B. The morphological growth patterns of colorectal liver metastases are prognostic for overall survival. Mod. Pathol. 2014, 27, 1641–1648. [Google Scholar] [CrossRef] [Green Version]
- Barnhill, R.; Van Dam, P.; Vermeulen, P.; Champenois, G.; Nicolas, A.; Rawson, R.V.; Wilmott, J.; Thompson, J.; Long, G.; Cassoux, N.; et al. Replacement and desmoplastic histopathological growth patterns in cutaneous melanoma liver metastases: Frequency, characteristics, and robust prognostic value. J. Pathol. Clin. Res. 2020, 6, 195–206. [Google Scholar] [CrossRef]
- Frentzas, S.; Simoneau, E.; Bridgeman, V.L.; Vermeulen, P.B.; Foo, S.; Kostaras, E.; Nathan, M.R.; Wotherspoon, A.; Gao, Z.-H.; Shi, Y.; et al. Vessel co-option mediates resistance to anti-angiogenic therapy in liver metastases. Nat. Med. 2016, 22, 1294–1302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, P.; Singh, A. Choroidal melanoma. Oman J. Ophthalmol. 2012, 5, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Henriquez, F.; Janssen, C.; Kemp, E.G.; Roberts, F. The t1799a braf mutation is present in iris melanoma. Investig. Ophthalmol. Vis. Sci. 2007, 48, 4897–4900. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yavuzyigitoglu, S.; Mensink, H.W.; Smit, K.N.; Vaarwater, J.; Verdijk, R.M.; Beverloo, B.; Brüggenwirth, H.T.; Van Marion, R.; Dubbink, H.J.; Paridaens, D.; et al. Metastatic Disease in Polyploid Uveal Melanoma Patients Is Associated With BAP1 Mutations. Investig. Opthalmol. Vis. Sci. 2016, 57, 2232. [Google Scholar] [CrossRef]
- Grossniklaus, H.E. Progression of ocular melanoma metastasis to the liver: The 2012 zimmerman lecture. JAMA Ophthalmol. 2013, 131, 462–469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grossniklaus, H.E.; Zhang, Q.; You, S.; McCarthy, C.; Heegaard, S.; Coupland, S.E. Metastatic ocular melanoma to the liver exhibits infiltrative and nodular growth patterns. Hum. Pathol. 2016, 57, 165–175. [Google Scholar] [CrossRef] [Green Version]
- Liao, A.; Mittal, P.; Lawson, D.H.; Yang, J.J.; Szalai, E.; Grossniklaus, H.E. Radiologic and Histopathologic Correlation of Different Growth Patterns of Metastatic Uveal Melanoma to the Liver. Ophthalmology 2018, 125, 597–605. [Google Scholar] [CrossRef] [PubMed]
- Barnhill, R.; Vermeulen, P.; Daelemans, S.; Van Dam, P.-J.; Roman-Roman, S.; Servois, V.; Hurbain, I.; Gardrat, S.; Raposa, G.; Nicolas, A.; et al. Replacement and desmoplastic histopathological growth patterns: A pilot study of prediction of outcome in patients with uveal melanoma liver metastases. J. Pathol. Clin. Res. 2018, 4, 227–240. [Google Scholar] [CrossRef]
- Robertson, A.G.; Shih, J.; Yau, C.; Gibb, E.A.; Oba, J.; Mungall, K.L.; Hess, J.M.; Uzunangelov, V.; Walter, V.; Danilova, L.; et al. Integrative Analysis Identifies Four Molecular and Clinical Subsets in Uveal Melanoma. Cancer Cell 2018, 33, 151. [Google Scholar] [CrossRef] [Green Version]
- Yu, H.; Pak, H.; Hammond-Martel, I.; Ghram, M.; Rodrigue, A.; Daou, S.; Barbour, H.; Corbeil, L.; Hébert, J.; Drobetsky, E.; et al. Tumor suppressor and deubiquitinase BAP1 promotes DNA double-strand break repair. Proc. Natl. Acad. Sci. USA 2013, 111, 285–290. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, J.Q.; Drabarek, W.; Yavuzyigitoglu, S.; Salsench, E.M.; Verdijk, R.M.; Naus, N.C.; De Klein, A.; Kiliç, E.; Brosens, E. Spliceosome Mutations in Uveal Melanoma. Int. J. Mol. Sci. 2020, 21, 9546. [Google Scholar] [CrossRef]
- Dayani, P.N.; Gould, J.E.; Brown, D.B.; Sharma, K.V.; Linette, G.P.; Harbour, J.W. Hepatic metastasis from uveal melanoma: Angiographic pattern predictive of survival after hepatic arterial chemoembolization. Arch. Ophthalmol. 2009, 127, 628–632. [Google Scholar] [CrossRef] [Green Version]
- Bosch, T.V.D.; Van Beek, J.G.M.; Vaarwater, J.; Verdijk, R.M.; Naus, N.C.; Paridaens, D.; De Klein, A.; Kiliç, E. Higher Percentage of FISH-Determined Monosomy 3 and 8q Amplification in Uveal Melanoma Cells relate to Poor Patient Prognosis. Investig. Opthalmol. Vis. Sci. 2012, 53, 2668–2674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Onken, M.; Worley, L.A.; Harbour, J.W. A Metastasis Modifier Locus on Human Chromosome 8p in Uveal Melanoma Identified by Integrative Genomic Analysis. Clin. Cancer Res. 2008, 14, 3737–3745. [Google Scholar] [CrossRef] [Green Version]
- Halenda, K.M.; Kudchadkar, R.R.; Lawson, D.H.; Kies, D.D.; Zhelnin, K.E.; Krasinskas, A.M.; Grossniklaus, H.E. Reduction of Nodular Growth Pattern of Metastatic Uveal Melanoma after Radioembolization of Hepatic Metastases. Ocul. Oncol. Pathol. 2015, 2, 160–165. [Google Scholar] [CrossRef] [Green Version]
- Field, M.G.; Decatur, C.L.; Kurtenbach, S.; Gezgin, G.; Van Der Velden, P.A.; Jager, M.J.; Kozak, K.N.; Harbour, J.W. PRAME as an Independent Biomarker for Metastasis in Uveal Melanoma. Clin. Cancer Res. 2016, 22, 1234–1242. [Google Scholar] [CrossRef] [Green Version]
- Babchia, N.; Landreville, S.; Clément, B.; Coulouarn, C.; Mouriaux, F. The bidirectional crosstalk between metastatic uveal melanoma cells and hepatic stellate cells engenders an inflammatory microenvironment. Exp. Eye Res. 2019, 181, 213–222. [Google Scholar] [CrossRef] [Green Version]
- Sharma, K.V.; Gould, J.E.; Harbour, J.W.; Linette, G.P.; Pilgram, T.K.; Dayani, P.N.; Brown, D.B. Hepatic Arterial Chemoembolization for Management of Metastatic Melanoma. Am. J. Roentgenol. 2008, 190, 99–104. [Google Scholar] [CrossRef] [PubMed]
- Valpione, S.; Moser, J.C.; Parrozzani, R.; Bazzi, M.; Mansfield, A.S.; Mocellin, S.; Pigozzo, J.; Midena, E.; Markovic, S.N.; Aliberti, C.; et al. Development and External Validation of a Prognostic Nomogram for Metastatic Uveal Melanoma. PLoS ONE 2015, 10, e0120181. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Total |
|---|---|
| Mean (range) | |
| Age (years) | 60.3 (28–87) |
| Largest basal diameter (mm) | 13.7 (5–20) |
| Tumor thickness (mm) | 7.0 (1–22) |
| Gender | n (%) |
| Male | 57/123 (46%) |
| Female | 66/123 (54%) |
| Survival | Median (range) |
| Disease-free survival, months | 25.6 (0–159.6) |
| Survival with metastases, months | 8.0 (0–114.3) |
| No (%) | |
| Alive | 17/123 (14%) |
| Death due to metastasis | 106/123 (86%) |
| Death due to other cause | 0/123 (0%) |
| Primary treatment UM | n (%) |
| Enucleation | 77/123 (63%) |
| Irradiation | 44/123 (36%) |
| Irradiation with secondary treatment | 10/44 (23%) |
| No treatment | 2/123 (2%) |
| Mutation primary UM | n (%) |
| BAP1 aberrant | 73/85 (86%) |
| SF3B1-mutated | 7/85 (8%) |
| No Recurrent Mutation | 5/85 (6%) |
| Hepatic metastatic patterns | n (%) |
| Single lesion | 18/123 (14.6%) |
| 2 to 5 lesions | 35/123 (28.5%) |
| 6 to 10 lesions | 17/123 (13.8%) |
| More than 10 lesions | 53/123 (43.1%) |
| Variables | Hepatic Metastatic Patterns (Number of Metastases) | ||||
|---|---|---|---|---|---|
| 1 Lesion | 2–5 Lesions | 6–10 Lesions | >10 Lesions | p-Value | |
| Mean age (range), yrs | 59.9 (39–81) | 58.4 (28–87) | 62.0 (44–80) | 61.2 (37–83) | 0.599 * |
| Mean largest basal diameter UM (range), mm | 13.2 (9–17) | 12.7 (10–18) | 13.9 (9–19) | 14.3 (5–20) | 0.072 * |
| Mean tumor height UM (range), mm | 6.2 (2–10) | 6.5 (2–12) | 7.0 (1–13) | 7.8 (2–22) | 0.345 * |
| Gender (%), n | |||||
| Male | 7 (39%) | 15 (43%) | 8 (47%) | 27 (51%) | 0.795† |
| Female | 11 (61%) | 20 (57%) | 9 (53%) | 26 (49) | |
| Histopathological features primary UM, n | |||||
| Epitheliod cells | 11/13 | 22/24 | 12/12 | 30/37 | 0.319 † |
| Closed vascular loops | 6/11 | 10/24 | 8/11 | 23/35 | 0.211 † |
| Involvement ciliary body | 4/12 | 8/24 | 5/12 | 13/35 | 0.961 † |
| Extra-ocular extensions | 0/11 | 2/23 | 4/12 | 7/31 | 0.095 † |
| Mutation primary UM, n | |||||
| BAP1 aberrant | 11 | 18 | 10 | 34 | 0.296 † |
| SF3B1-mutated | 1 | 2 | 0 | 4 | |
| No Recurrent Mutation | 0 | 3 | 2 | 0 | |
| Not tested/incomplete | 6 | 12 | 5 | 15 | |
| Mutation primary UM, n | |||||
| GNAQ-mutated | 2 | 9 | 5 | 9 | 0.414 †§ |
| GNA11-mutated | 6 | 6 | 4 | 13 | 0.502 †§ |
| GNAQ/GNA11 wildtype | 2 | 2 | 0 | 1 | |
| Not tested | 8 | 18 | 8 | 30 | |
| Extrahepatic metastases, n | |||||
| Yes | 10 | 13 | 5 | 22 | 0.433 † |
| No | 8 | 22 | 12 | 31 | |
| Hepatic Metastatic Patterns (Number of Metastases) | |||||||
|---|---|---|---|---|---|---|---|
| Variables (n = 83) | 1 Lesion | 2–5 Lesions | 6–10 Lesions | >10 Lesions | p-Value | Miliary | p-Value * |
| Chromosome 1p | |||||||
| Loss | 3 | 7 | 6 | 17 | 0.352 | 12 | 0.026 |
| Normal | 11 | 13 | 6 | 20 | 8 | ||
| Chromosome 3 | |||||||
| Loss | 12 | 17 | 11 | 33 | 0.932 | 18 | 0.703 |
| Normal | 2 | 3 | 1 | 4 | 2 | ||
| Chromosome 6p | |||||||
| Loss | 0 | 0 | 1 | 1 | 0.796 | 15 | 0.816 |
| Normal | 10 | 16 | 8 | 28 | 5 | ||
| Gain | 4 | 4 | 3 | 8 | |||
| Chromosome 6q | |||||||
| Loss | 2 | 4 | 4 | 12 | 0.531 | 6 | 0.305 |
| Normal | 11 | 15 | 8 | 25 | 14 | ||
| Gain | 1 | 1 | 0 | 0 | 0 | ||
| Chromosome 8p | |||||||
| Loss | 0 | 4 | 6 | 13 | 0.045 | 7 | 0.035 |
| Normal | 9 | 13 | 3 | 19 | 10 | ||
| Gain | 5 | 3 | 3 | 5 | 3 | ||
| Chromosome 8q | |||||||
| Normal | 4 | 2 | 1 | 9 | 0.332 | 5 | 0.816 |
| Gain | 10 | 18 | 11 | 28 | 15 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yavuzyigitoglu, S.; Tang, M.C.Y.; Jansen, M.; Geul, K.W.; Dwarkasing, R.S.; Vaarwater, J.; Drabarek, W.; Verdijk, R.M.; Paridaens, D.; Naus, N.C.; et al. Radiological Patterns of Uveal Melanoma Liver Metastases in Correlation to Genetic Status. Cancers 2021, 13, 5316. https://doi.org/10.3390/cancers13215316
Yavuzyigitoglu S, Tang MCY, Jansen M, Geul KW, Dwarkasing RS, Vaarwater J, Drabarek W, Verdijk RM, Paridaens D, Naus NC, et al. Radiological Patterns of Uveal Melanoma Liver Metastases in Correlation to Genetic Status. Cancers. 2021; 13(21):5316. https://doi.org/10.3390/cancers13215316
Chicago/Turabian StyleYavuzyigitoglu, Serdar, Michael C. Y. Tang, Miguel Jansen, Kaspar W. Geul, Roy S. Dwarkasing, Jolanda Vaarwater, Wojtek Drabarek, Robert M. Verdijk, Dion Paridaens, Nicole C. Naus, and et al. 2021. "Radiological Patterns of Uveal Melanoma Liver Metastases in Correlation to Genetic Status" Cancers 13, no. 21: 5316. https://doi.org/10.3390/cancers13215316