
Masaoka-Koga and TNM Staging System in Thymic Epithelial Tumors: Prognostic Comparison and the Role of the Number of Involved Structures

 ,
,  , ,
, ,  , , , and
, , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Clinical and Pathological Records of Patients who Underwent Surgical Treatment for TET in our Institution from 1 January 1985 to 1 January 2018 Were Collected and Retrospectively Reviewed
2.2. Statistical Analysis
3. Results
3.1. Overall
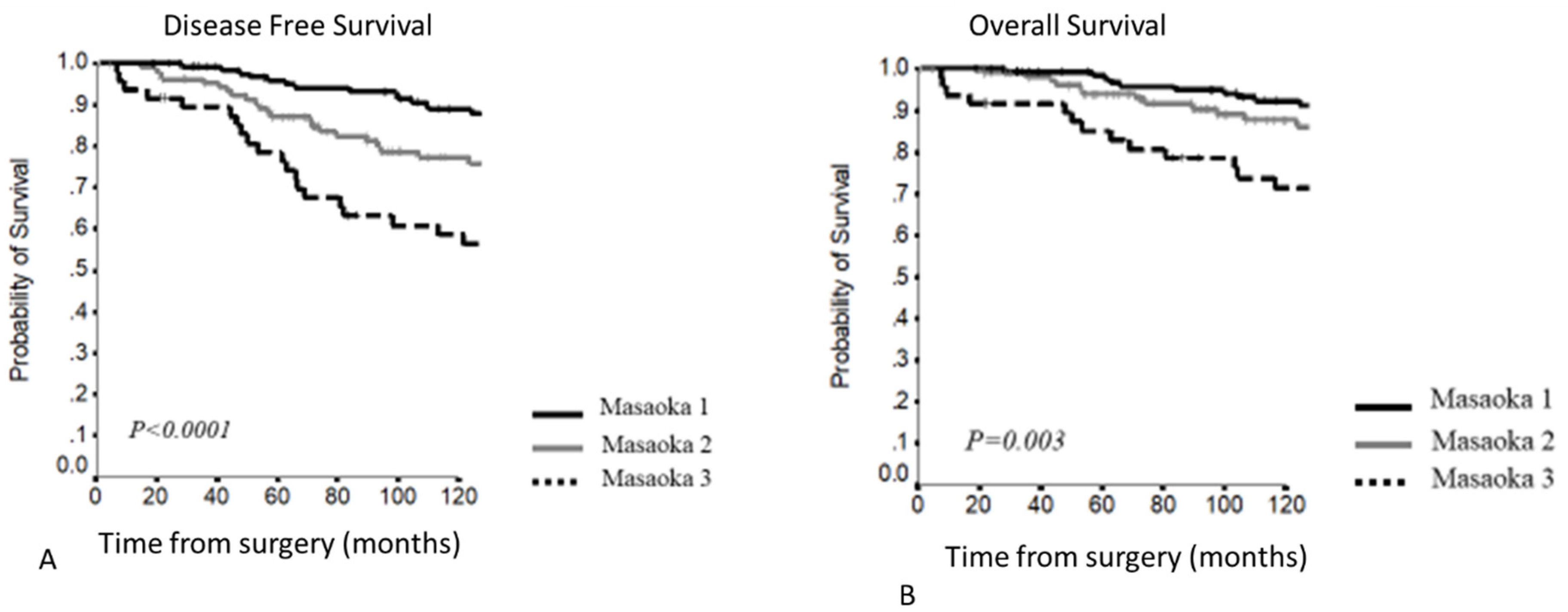
3.2. Masaoka–Koga Staging System
3.3. TNM Staging System
- 5–10YDFS (p < 0.0001)
- T1: 90.13% and 82.1%
- T2: 76% and 56.0%
- T3: 71.6% and 56.5%
- 5–10YOS (p = 0.02)
- T1: 95.5% and 88.8%
- T2: 88% and 70.7%
- T3: 84.8% and 76.3%
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- de Jong, W.K.; Blaauwgeers, J.L.; Schaapveld, M.; Timens, W.; Klinkenberg, T.J.; Groen, H.J. Thymic epithelial tumours: A population-based study of the incidence, diagnostic procedures and therapy. Eur. J. Cancer 2008, 44, 123–130. [Google Scholar] [CrossRef] [PubMed]
- Benjamin, D.J.; Klapheke, A.; Lara, P.N.; Cress, R.D.; Riess, J.W. A Population-Based Study of Incidence and Survival of 1588 Thymic Malignancies: Results from the California Cancer Registry. Clin. Lung Cancer 2019, 20, 477–483. [Google Scholar] [CrossRef] [PubMed]
- Koga, K.; Matsuno, Y.; Noguchi, M.; Mukai, K.; Asamura, H.; Goya, T.; Shimosato, Y. A review of 79 thymomas: Modification of staging system and reappraisal of conventional division into invasive and non-invasive thymoma. Pathol. Int. 1994, 44, 359–367. [Google Scholar] [CrossRef] [PubMed]
- Detterbeck, F.C.; Stratton, K.; Giroux, D.; Asamura, H.; Crowley, J.; Falkson, C.; Filosso, P.L.; Frazier, A.A.; Giaccone, G.; Huang, J.; et al. The IASLC/ITMIG Thymic Epithelial Tumors Staging Project: Proposal for an Evidence-Based Stage Classification System for the Forthcoming (8th) Edition of the TNM Classification of Malignant Tumors. J. Thorac. Oncol. 2014, 9, S65–S72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nicholson, A.G.; Detterbeck, F.C.; Marino, M.; Kim, J.; Stratton, K.; Giroux, D.; Asamura, H.; Crowley, J.; Falkson, C.; Filosso, P.L.; et al. The IASLC/ITMIG Thymic Epithelial Tumors Staging Project: Proposals for the T component for the Forthcoming (8th) Edition of the TNM Classification of Malignant Tumors. J. Thorac. Oncol. 2014, 9, S73–S80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liang, G.; Gu, Z.; Li, Y.; Fu, J.; Shen, Y.; Wei, Y.; Tan, L.; Zhang, P.; Han, Y.; Chen, C.; et al. Comparison of the Masaoka-Koga staging and the International Association for the Study of Lung Cancer/the International Thymic Malignancies Interest Group proposal for the TNM staging systems based on the Chinese Alliance for Research in Thymomas retrospective database. J. Thorac. Dis. 2016, 8, 727–737. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fukui, T.; Fukumoto, K.; Okasaka, T.; Kawaguchi, K.; Nakamura, S.; Hakiri, S.; Ozeki, N.; Hirakawa, A.; Tateyama, H.; Yokoi, K. Clinical evaluation of a new tumour–node–metastasis staging system for thymic malignancies proposed by the International Association for the Study of Lung Cancer Staging and Prognostic Factors Committee and the International Thymic Malignancy Interest Group. Eur. J. Cardio-Thoracic Surg. 2015, 49, 574–579. [Google Scholar] [CrossRef] [Green Version]
- Ried, M.; Eicher, M.-M.; Neu, R.; Sziklavari, Z.; Hofmann, H.-S. Evaluation of the new TNM-staging system for thymic malignancies: Impact on indication and survival. World J. Surg. Oncol. 2017, 15, 214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, Y.; Shi, J.; Fan, L.; Yang, J.; Hu, D.; Zhao, H. Evaluation of the proposed International Association for the Study of Lung Cancer (IASLC)/International Thymic Malignancies Interest Group (ITMIG) staging revisions in thymic well-differentiated neuroendocrine carcinoma patients. Eur. J. Cardio-Thoracic Surg. 2015, 49, 569–573. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marx, A.; Ströbel, P.; Badve, S.; Chalabreysse, L.; Chan, J.K.; Chen, G.; de Leval, L.; Detterbeck, F.; Girard, N.; Huang, J.; et al. ITMIG Consensus Statement on the Use of the WHO Histological Classification of Thymoma and Thymic Carcinoma: Refined Definitions, Histological Criteria, and Reporting. J. Thorac. Oncol. 2014, 9, 596–611. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Girard, N.; Ruffini, E.; Marx, A.; Faivre-Finn, C.; Peters, S. Thymic epithelial tumours: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2015, 26, v40–v55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- NCCN Guide-lines. Available online: https://www.nccn.org/guidelines/category_1 (accessed on 3 August 2021).
- Ruffini, E.; Fang, W.; Guerrera, F.; Huang, J.; Okumura, M.; Kim, D.K.; Girard, N.; Billè, A.; Boubia, S.; Cangir, A.K.; et al. The International Association for the Study of Lung Cancer Thymic Tumors Staging Project: The Impact of the Eighth Edition of the Union for International Cancer Control and American Joint Committee on Cancer TNM Stage Classification of Thymic Tumors. J. Thorac. Oncol. 2019, 15, 436–447. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Gu, Z.; Qiu, B.; Detterbeck, F.C.; Roden, A.C.; Ruffini, E.; Okumura, M.; Girard, N.; Xiang, Y.; Liu, Y.; et al. A Recurrence Predictive Model for Thymic Tumors and Its Implication for Postoperative Management: A Chinese Alliance for Research in Thymomas Database Study. J. Thorac. Oncol. 2019, 15, 448–456. [Google Scholar] [CrossRef] [PubMed]
- Chiappetta, M.; Sperduti, I.; Lococo, F.; Margaritora, S. Does Follow-Up Duration Affect the Effectiveness of a Predictive Nomogram Model for Thymic Malignancy Recurrences? Results from an External Validation. J. Thorac. Oncol. 2020, 15, e137–e139. [Google Scholar] [CrossRef] [PubMed]
- Leuzzi, G.; Rocco, G.; Ruffini, E.; Sperduti, I.; Detterbeck, F.; Weder, W.; Venuta, F.; Van Raemdonck, D.; Thomas, P.; Facciolo, F. Multimodality therapy for locally advanced thymomas: A propensity score–matched cohort study from the European Society of Thoracic Surgeons Database. J. Thorac. Cardiovasc. Surg. 2015, 151, 47–57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruffini, E.; Detterbeck, F.; Van Raemdonck, D.; Rocco, G.; Thomas, P.; Weder, W.; Brunelli, A.; Evangelista, A.; Venuta, F.; Khaled, A.; et al. Tumours of the thymus: A cohort study of prognostic factors from the European Society of Thoracic Surgeons database. Eur. J. Cardio-Thoracic Surg. 2014, 46, 361–368. [Google Scholar] [CrossRef] [PubMed] [Green Version]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N. of Patients | |
|---|---|
| Age (mean and SD) | 51.2 ± 14.65 |
| Gender | |
| Male | 176 (46.4%) |
| Female | 203 (53.6%) |
| Comorbidity | |
| Myasthenia Gravis | 286 (75.5%) |
| Diabetes | 39 (10.3%) |
| Basedow’s disease | 3 (0.8%) |
| Hashimoto’s thyroiditis | 60 (15.8%) |
| Pure red cell aplasia | 18 (4.7%) |
| Other autoimmune disorders | 21 (5.5%) |
| Surgical Radicality | |
| R0 | 375 (98.9%) |
| R1 | 3 (0.8%) |
| R2 | 1 (0.3%) |
| Involved Structures | |
| Pleura | 60 (15.8%) |
| Pericardium | 37 (9.8%) |
| Lung | 26 (6.9%) |
| Great Vessels | 11 (2.9%) |
| N. of infiltrated organs per patients | |
| 0 | 304 (80.2%) |
| 1 | 28 (7.4%) |
| 2 | 35 (9.2%) |
| 3 | 12 (3.2%) |
| Histology | |
| A-AB | 71 (18.8%) |
| B1 | 51 (13.4%) |
| B2 | 194 (51.2%) |
| B3 | 50 (13.2%) |
| C | 13 (3.4%) |
| Masaoka–Koga | ||
|---|---|---|
| Stage | Patients | Rate |
| I | 179 | 47.2% |
| II | 140 | 36.9% |
| IIa | 49 | 12.9% |
| IIb | 91 | 24% |
| III | 57 | 15.1% |
| IV | 3 | 0.8% |
| Stage | Disease Free Survival | Overall Survival | ||
|---|---|---|---|---|
| HR | p Value | HR | p Value | |
| Masaoka–Koga | ||||
| <0.001 | 0.013 | |||
| II vs. I | 1.050 | 0.831 | 0.979 | 0.936 |
| III vs. I | 2.701 | <0.001 | 2.027 | 0.006 |
| II vs. III | 0.389 | <0.001 | 0.483 | 0.015 |
| T TNM | ||||
| <0.001 | 0.019 | |||
| 2 vs. 1 | 1.909 | 0.025 | 1.699 | 0.103 |
| 3 vs. 1 | 3.167 | <0.001 | 2.267 | 0.012 |
| 2 vs. 3 | 0.603 | 0.162 | 0.750 | 0.502 |
| TNM | ||
|---|---|---|
| T | Patients | Rate |
| 1a | 304 | 80.2% |
| 1b | 15 | 4% |
| 2 | 25 | 6.6% |
| 3 | 32 | 8.4% |
| 4 | 3 | 0.8% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chiappetta, M.; Lococo, F.; Pogliani, L.; Sperduti, I.; Tabacco, D.; Bria, E.; D’Argento, E.; Massaccesi, M.; Boldrini, L.; Meacci, E.; et al. Masaoka-Koga and TNM Staging System in Thymic Epithelial Tumors: Prognostic Comparison and the Role of the Number of Involved Structures. Cancers 2021, 13, 5254. https://doi.org/10.3390/cancers13215254
Chiappetta M, Lococo F, Pogliani L, Sperduti I, Tabacco D, Bria E, D’Argento E, Massaccesi M, Boldrini L, Meacci E, et al. Masaoka-Koga and TNM Staging System in Thymic Epithelial Tumors: Prognostic Comparison and the Role of the Number of Involved Structures. Cancers. 2021; 13(21):5254. https://doi.org/10.3390/cancers13215254
Chicago/Turabian StyleChiappetta, Marco, Filippo Lococo, Luca Pogliani, Isabella Sperduti, Diomira Tabacco, Emilio Bria, Ettore D’Argento, Mariangela Massaccesi, Luca Boldrini, Elisa Meacci, and et al. 2021. "Masaoka-Koga and TNM Staging System in Thymic Epithelial Tumors: Prognostic Comparison and the Role of the Number of Involved Structures" Cancers 13, no. 21: 5254. https://doi.org/10.3390/cancers13215254