Treatment of Advanced Gastro-Entero-Pancreatic Neuro-Endocrine Tumors: A Systematic Review and Network Meta-Analysis of Phase III Randomized Controlled Trials

 , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Material and Methods
2.1. Eligibility Criteria
- (a)
- “Population” was represented by the patients having nonresectable GEP–NENs;
- (b)
- “Intervention” arms were any nonsurgical therapy;
- (c)
- the “Control” group was the placebo arm;
- (d)
- all studies reporting at least PFS and grade 3–4 toxicity;
- (e)
- all phase III RCTs included at least two arms.
2.2. Information Source, Search, Study Selection, and Data Collection Process
2.3. Data Items
2.4. Geometries of the Network and Risk of Bias within the Individual Study
2.5. Summary Measurements and Methods of the Analysis
2.6. Inconsistency, Risk of Bias across the Studies, and Meta-Regression Analysis
3. Results
3.1. Studies Selected
3.2. Study Characteristics and Risk of Bias within Studies
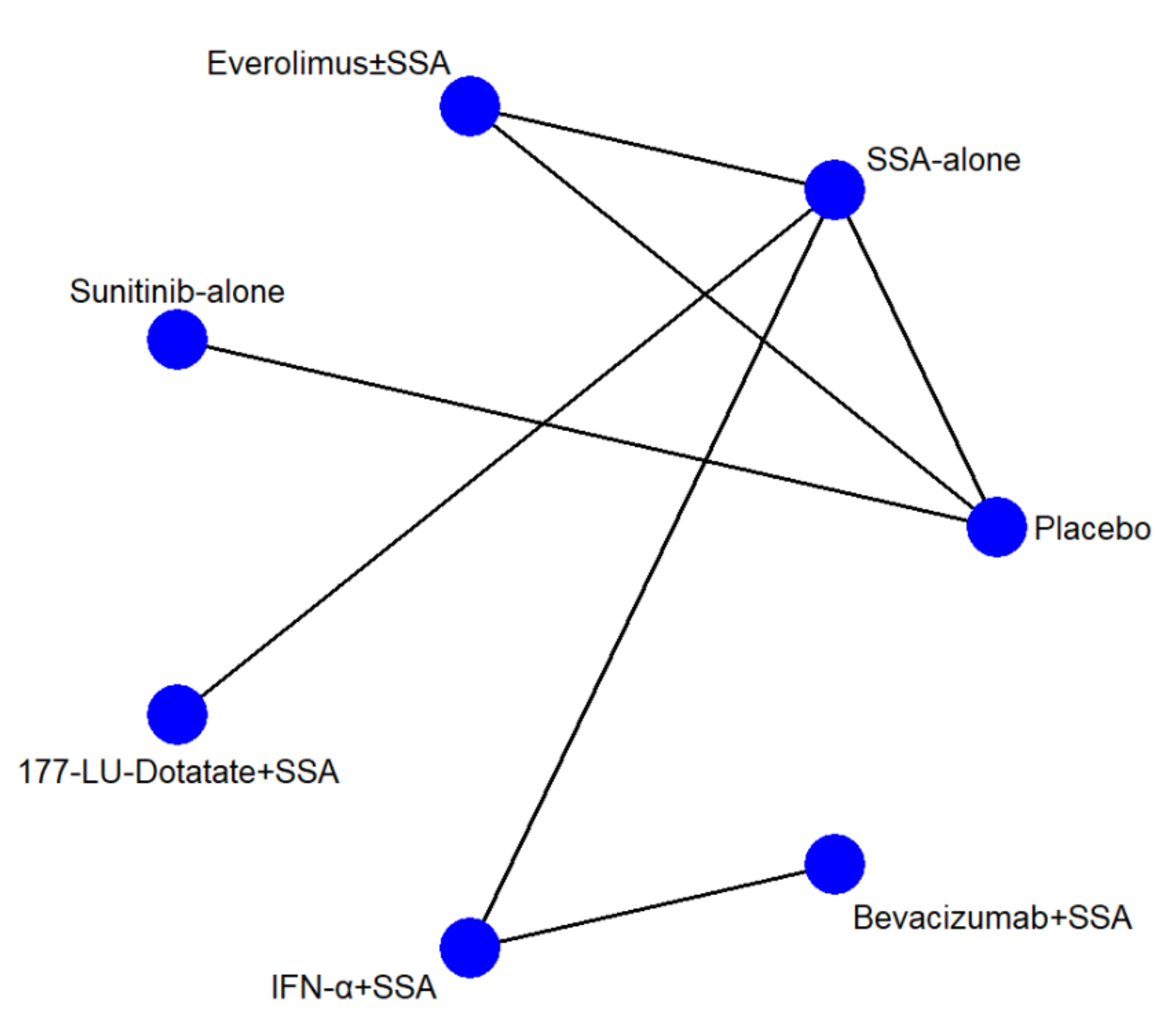
3.3. Network Structures and Geometries
3.4. Synthesis of Results
3.4.1. Efficacy (PFS)
3.4.2. Safety (Toxicity Grade 3 and 4)
3.4.3. Safety/Efficacy Ratio
3.4.4. Secondary Endpoints
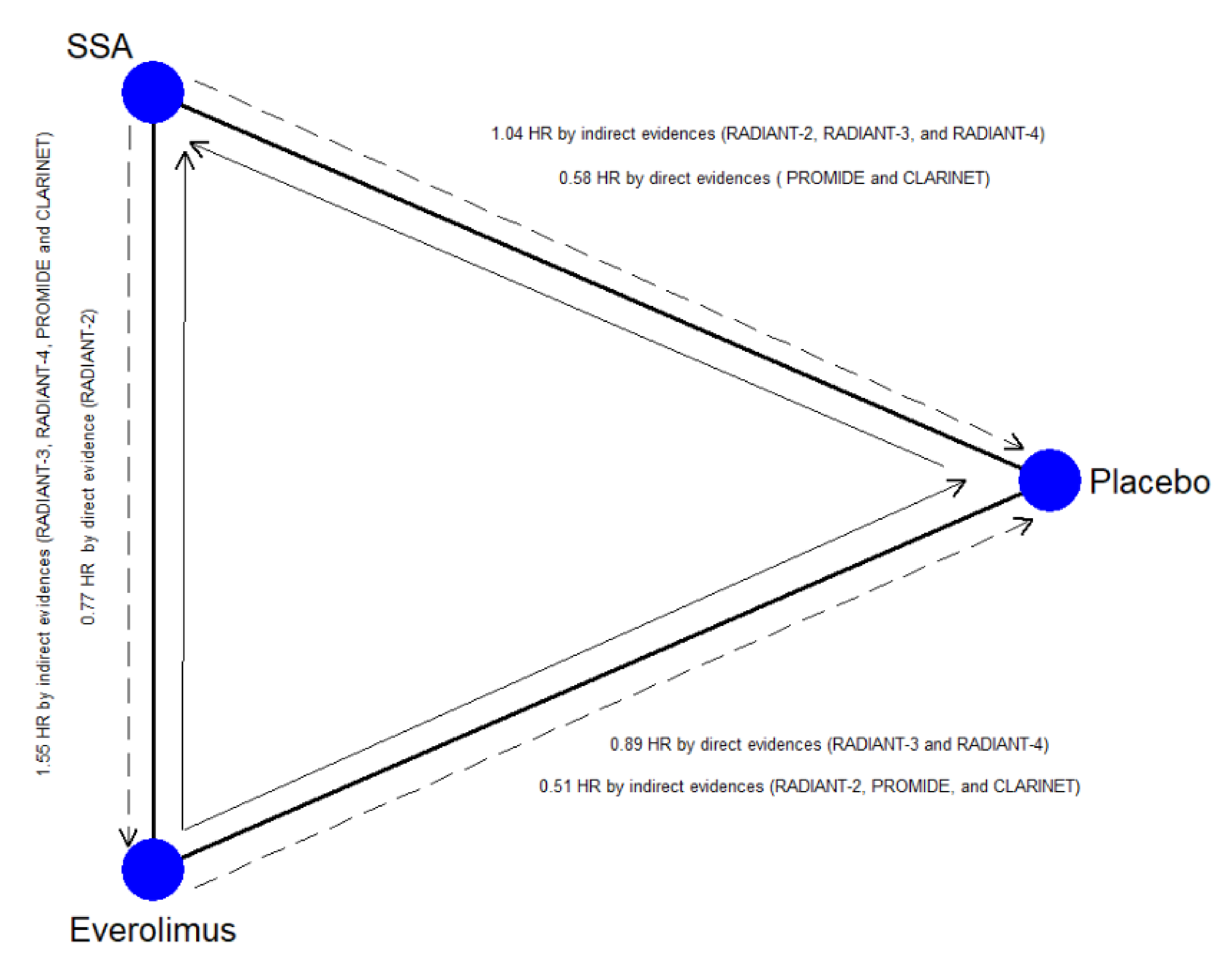
3.4.5. Inconsistency, Heterogeneity, and Publication Bias
3.5. Primary Endpoints
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Declaration of Interest Statement
Conflicts of Interest
References
- Kiesewetter, B.; Raderer, M. How I treat neuroendocrine tumours. ESMO Open 2020, 5, e000811. [Google Scholar] [CrossRef]
- Strosberg, J.R.; Halfdanarson, T.R.; Bellizzi, A.M.; Chan, J.A.; Dillon, J.S.; Heaney, A.P.; Kunz, P.L.; O’Dorisio, T.M.; Salem, R.; Segelov, E.; et al. The North American Neuroendocrine Tumor Society Consensus Guidelines for Surveillance and Medical Management of Midgut Neuroendocrine Tumors. Pancreas 2017, 46, 707–714. [Google Scholar] [CrossRef]
- Halfdanarson, T.R.; Strosberg, J.R.; Tang, L.; Bellizzi, A.M.; Bergsland, E.K.; OʼDorisio, T.M.; Halperin, D.M.; Fishbein, L.; Eads, J.; Hope, T.A.; et al. The North American Neuroendocrine Tumor Society Consensus Guidelines for Surveillance and Medical Management of Pancreatic Neuroendocrine Tumors. Pancreas 2020, 49, 863–881. [Google Scholar] [CrossRef]
- Pavel, M.; O’Toole, D.; Costa, F.; Capdevila, J.; Gross, D.; Kianmanesh, R.; Krenning, E.; Knigge, U.; Salazar, R.; Pape, U.F.; et al. Vienna Consensus Conference participants. ENETS Consensus Guidelines Update for the Management of Distant Metastatic Disease of Intestinal, Pancreatic, Bronchial Neuroendocrine Neoplasms (NEN) and NEN. of Unknown Primary Site. Neuroendocrinology 2016, 103, 172–185. [Google Scholar] [CrossRef]
- Kaderli, R.M.; Spanjol, M.; Kollár, A.; Bütikofer, L.; Gloy, V.; Dumont, R.A.; Seiler, C.A.; Christ, E.R.; Radojewski, P.; Briel, M.; et al. Therapeutic Options for Neuroendocrine Tumors: A Systematic Review and Network Meta-analysis. JAMA Oncol. 2019, 5, 480–489. [Google Scholar] [CrossRef] [PubMed]
- Hutton, B.; Salanti, G.; Caldwell, D.M.; Chaimani, A.; Schmid, C.H.; Cameron, C.; Ioannidis, J.P.A.; Straus, S.; Thorlund, K.; Jansen, J.P.; et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: Checklist and explanations. Ann. Int. Med. 2015, 11, 777–784. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eriksen, M.B.; Frandsen, T.F. The impact of patient, intervention, comparison, outcome (PICO) as a search strategy tool on literature search quality: A systematic review. J. Med. Libr. Assoc. 2018, 106, 420–421. [Google Scholar] [CrossRef] [PubMed]
- Therasse, P.; Arbuck, S.G.; Eisenhauer, E.A.; Wanders, J.; Kaplan, R.S.; Rubinstein, L.; Verweij, J.; Van Glabbeke, M.; van Oosterom, A.T.; Christian, M.C.; et al. New guidelines to evaluate the response to treatment in solid tumors. European Organization for Research and Treatment of Cancer, National Cancer Institute of the United States, National Cancer Institute of Canada. J. Natl. Cancer Inst. 2000, 92, 205–216. [Google Scholar] [CrossRef] [Green Version]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Arbuck, S.; Gwyther, S.; Mooney, M.; Rubinstein, L.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef]
- NCI Guidelines for Investigators: Adverse Event Reporting Requirements for Dctd (Ctep and Cip) and Dcp Inds and IDEs. Available online: https://ctep.cancer.gov/protocolDevelopment/electronic_applications/docs/aeguidelines.pdf (accessed on 15 December 2020).
- Bender, R.; Beckmann, L. Limitations of the incidence density ratio as approximation of the hazard ratio. Trials 2019, 20, 485. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caldwell, D.M.; Ades, A.E.; Higgins, J.P. Simultaneous comparison of multiple treatments: Combining direct and indirect evidence. BMJ 2005, 331, 897–900. [Google Scholar] [CrossRef] [Green Version]
- Mills, E.J.; Ioannidis, J.P.A.; Thorlund, K.; Schünemann, H.J.; Puhan, M.A.; Guyatt, G.H. How to use an article reporting a multiple treatment comparison meta-analysis. JAMA 2012, 308, 1246–1253. [Google Scholar] [CrossRef] [PubMed]
- Chaimani, A.; Higgins, J.P.; Mavridis, D.; Spyridonos, P.; Salanti, G. Graphical tools for network meta-analysis in STATA. PLoS ONE 2013, 8, e76654. [Google Scholar] [CrossRef] [PubMed]
- Bucher, H.C.; Guyatt, G.H.; Griffith, L.E.; Walter, S.D. The results of direct and indirect treatment comparisons in meta-analysis of randomized controlled trials. J. Clin. Epidemiol. 1997, 50, 683–691. [Google Scholar] [CrossRef]
- Shim, S.; Yoon, B.H.; Shin, I.S.; Bae, J.M. Network meta-analysis: Application and practice using Stata. Epidemiol. Health 2017, 27, e2017047. [Google Scholar] [CrossRef]
- Turner, R.M.; Davey, J.; Clarke, M.J.; Thompson, S.G.; Higgins, J.P. Predicting the extent of heterogeneity in meta-analysis, using empirical data from the Cochrane Database of Systematic Reviews. Int. J. Epidemiol. 2012, 41, 818–827. [Google Scholar] [CrossRef] [Green Version]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [Green Version]
- Arnold, R.; Rinke, A.; Klose, K.J.; Müller, H.H.; Wied, M.; Zamzow, K.; Schmidt, C.; Schade-Brittinger, C.; Barth, P.; Moll, R.; et al. Octreotide versus octreotide plus interferon-alpha in endocrine gastroenteropancreatic tumors: A randomized trial. Clin. Gastroenterol. Hepatol. 2005, 3, 761–771. [Google Scholar] [CrossRef]
- Rinke, A.; Müller, H.H.; Schade-Brittinger, C.; Klose, K.J.; Barth, P.; Wied, M.; Mayer, C.; Aminossadati, B.; Pape, U.F.; Bläker, M.; et al. PROMID Study Group. Placebo-controlled, double-blind, prospective, randomized study on the effect of octreotide LAR in the control of tumor growth in patients with metastatic neuroendocrine midgut tumors: A report from the PROMID Study Group. J. Clin. Oncol. 2009, 27, 4656–4663. [Google Scholar] [CrossRef]
- Rinke, A.; Wittenberg, M.; Schade-Brittinger, C.; Aminossadati, B.; Ronicke, E.; Gress, T.M.; Müller, H.H.; Arnold, R. PROMID Study Group. Placebo-Controlled, Double-Blind, Prospective, Randomized Study on the Effect of Octreotide LAR in the Control of Tumor Growth in Patients with Metastatic Neuroendocrine Midgut Tumors (PROMID): Results of Long-Term Survival. Neuroendocrinology 2017, 104, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Pavel, M.E.; Hainsworth, J.D.; Baudin, E.; Peeters, M.; Hörsch, D.; Winkler, R.E.; Klimovsky, J.; Lebwohl, D.; Jehl, V.; Wolin, E.M.; et al. RADIANT-2 Study Group. Everolimus plus octreotide long-acting repeatable for the treatment of advanced neuroendocrine tumours associated with carcinoid syndrome (RADIANT-2): A randomised, placebo-controlled, phase 3 study. Lancet 2011, 10, 2005–2012. [Google Scholar] [CrossRef]
- Pavel, M.E.; Baudin, E.; Öberg, K.E.; Hainsworth, J.D.; Voi, M.; Rouyrre, N.; Peeters, M.; Gross, D.J.; Yao, J.C. Efficacy of Everolimus plus octreotide LAR in patients with advanced neuroendocrine tumor and carcinoid syndrome: Final overall survival from the randomized, placebo-controlled phase 3 RADIANT-2 study. Ann. Oncol. 2017, 28, 1569–1575. [Google Scholar] [CrossRef] [PubMed]
- Yao, J.C.; Shah, M.H.; Ito, T.; Bohas, C.L.; Wolin, E.M.; Van Cutsem, E.; Hobday, T.J.; Okusaka, T.; Capdevila, J.; de Vries, E.G.; et al. RAD001 in Advanced Neuroendocrine Tumors, Third Trial (RADIANT-3) Study Group. Everolimus for advanced pancreatic neuroendocrine tumors. N. Engl. J. Med. 2011, 364, 514–523. [Google Scholar] [CrossRef] [Green Version]
- Yao, J.C.; Pavel, M.; Lombard-Bohas, C.; Van Cutsem, E.; Voi, M.; Brandt, U.; He, W.; Chen, D.; Capdevila, J.; de Vries, E.G.E.; et al. Everolimus for the Treatment of Advanced Pancreatic Neuroendocrine Tumors: Overall Survival and Circulating Biomarkers From the Randomized, Phase III RADIANT-3 Study. J. Clin. Oncol. 2016, 34, 3906–3913. [Google Scholar] [CrossRef]
- Raymond, E.; Dahan, L.; Raoul, J.L.; Bang, Y.J.; Borbath, I.; Lombard-Bohas, C.; Valle, J.; Metrakos, P.; Smith, D.; Vinik, A.; et al. Sunitinib malate for the treatment of pancreatic neuroendocrine tumors. N. Engl. J. Med. 2011, 364, 501–513. [Google Scholar] [CrossRef] [Green Version]
- Caplin, M.E.; Pavel, M.; Ćwikła, J.B.; Phan, A.T.; Raderer, M.; Sedláčková, E.; Cadiot, G.; Wolin, E.M.; Capdevila, J.; Wall, L.; et al. CLARINET Investigators. Lanreotide in metastatic enteropancreatic neuroendocrine tumors. N. Engl. J. Med. 2014, 371, 224–233. [Google Scholar] [CrossRef]
- Yao, J.C.; Fazio, N.; Singh, S.; Buzzoni, R.; Carnaghi, C.; Wolin, E.; Tomasek, J.; Raderer, M.; Lahner, H.; Voi, M.; et al. RAD001 in Advanced Neuroendocrine Tumours, Fourth Trial (RADIANT-4) Study Group. Everolimus for the treatment of advanced, non-functional neuroendocrine tumours of the lung or gastrointestinal tract (RADIANT-4): A randomised, placebo-controlled, phase 3 study. Lancet 2016, 387, 968–977. [Google Scholar]
- Strosberg, J.; El-Haddad, G.; Wolin, E.; Hendifar, A.; Yao, J.; Chasen, B.; Mittra, E.; Kunz, P.L.; Kulke, M.H.; Jacene, H.; et al. NETTER-1 Trial Investigators. Phase 3 Trial of 177Lu-Dotatate for Midgut Neuroendocrine Tumors. N. Engl. J. Med. 2017, 376, 125–135. [Google Scholar] [CrossRef]
- Yao, J.C.; Guthrie, K.A.; Moran, C.; Strosberg, J.R.; Kulke, M.H.; Chan, J.A.; LoConte, N.; McWilliams, R.R.; Wolin, E.M.; Mattar, B.; et al. Phase III Prospective Randomized Comparison Trial of Depot Octreotide Plus Interferon Alfa-2b Versus Depot Octreotide Plus Bevacizumab in Patients With Advanced Carcinoid Tumors: SWOG S0518. J. Clin. Oncol. 2017, 35, 1695–1703. [Google Scholar] [CrossRef]
- Ter Veer, E.; van Oijen, M.G.H.; van Laarhoven, H.W.M. The Use of (Network) Meta-Analysis in Clinical Oncology. Front. Oncol. 2019, 9, 822. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berardi, R.; Partelli, S.; Cascinu, S.; Falconi, M. Somatostatin analogs: Is one better than other? Ther. Adv. Med. Oncol. 2017, 9, 817–819. [Google Scholar] [CrossRef] [PubMed]
- FDA Approves Lutetium Lu 177 Dotatate for Treatment of GEP-NETS. Available online: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-lutetium-lu-177-dotatate-treatment-gep-nets (accessed on 15 December 2020).
- Lutathera. Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/lutathera (accessed on 15 December 2020).
- Study to Evaluate the Efficacy and Safety of Lutathera in Patients With Grade 2 and Grade 3 Advanced GEP-NET (NETTER-2). Available online: https://clinicaltrials.gov/ct2/show/NCT03972488 (accessed on 15 December 2020).
- Mujica-Mota, R.; Varley-Campbell, J.; Tikhonova, I.; Cooper, C.; Griffin, E.; Haasova, M.; Peters, J.; Lucherini, S.; Talens-Bou, J.; Long, L.; et al. Everolimus, lutetium-177 DOTATATE and Sunitinib for advanced, unresectable or metastatic neuroendocrine tumours with disease progression: A systematic review and cost-effectiveness analysis. Health Technol. Assess. 2018, 22, 1–326. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| First Author/Year | Acronyms | Affiliation/Country | Population $ | Pan-NET | Previous SSA Therapy | Previous CHT | Other Therapy | Previous Surgery of Primary Tumor | Design |
|---|---|---|---|---|---|---|---|---|---|
| Arnold et al., 2005 [20] | - | Multicenter | GEP-NET | Yes | Yes | Yes | No | § | Octreotide * vs. Octreotide * + IFN-α |
| Rinke et al., 2009 [21,22] | PROMIDE | Multicenter | Midgut NET | No | Yes # | No | No | Yes | Placebo vs. Octreotide LAR 30 mg |
| Pavel et al., 2011 [23,24] | RADIANT-2 | Multicenter | GEP-NET | Yes | Yes | Yes | Yes ^ | § | Octreotide LAR 30 mg vs. Octretide LAR 30 mg + Everolimus 10 mg |
| Yao et al., 2011 [25,26] | RADIANT-3 | Multicenter | Pan-NET | Yes | Yes | Yes | Yes ^^ | § | Placebo vs. Everolimus 10 mg |
| Raymond et al., 2011 [27] | - | Multicenter | Pan-NET | Yes | Yes | Yes °° | Yes °° | Yes | Placebo vs. Sunitinib 37.5 mg |
| Caplin et al., 2014 [28] | CLARINET | Multicenter | GEP-NET | Yes | Yes £ | Yes £ | Yes £ | Yes £ | Placebo vs. Lanreotide 120 mg |
| Yao et al., 2016 [29] | RADIANT-4 | Multicenter | Lung or Midgut NET | No | Yes | Yes | Yes | Yes | Placebo vs. Everolimus 10 mg |
| Strosberg et al., 2017 [30] | NETTER-1 | Multicenter | Midgut NET | No | Yes ** | Yes ** | Yes ** | Yes | 177 Lu-Dotate + Octreotide LAR 30 mg vs. Octreotide LAR 60 mg |
| Yao et al., 2017 [31] | SWOG S0518 | Multicenter | Midgut NET | No | Yes £ | Yes | Yes £ | Yes £ | depot Octreotide 20 mg + Bevacizumab vs. depot Octreotide 20 mg + IFN-α |
| First Author/Year | Clusters | Endpoints | Rob2 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Placebo (Arm A) | SSA-Based (Arm B) | Everolimus-Based (Arm C) | Sunitinib -Based (Arm D) | 177Lu-Dotatate-Based (Arm E) | IFN-α-Based (Arm F) | BevacizumaB-Based (Arm G) | |||
| Arnold et al., 2005 [20] | - | 51 | - | - | - | 54 | - | PFS, grade 3–4 toxicity, OS, ORR, PD, SAEs, OTD, DDR, DDAEs | Low risk |
| Rinke et al., 2009 [21,22] | 43 | 42 | - | - | - | - | - | PFS, grade 3–4 toxicity, OS, ORR, PD, SAEs, OTD, DDR, DDAEs | Some Comcerns |
| Pavel et al., 2011 [23,24] | - | 213 | 216 | - | - | - | - | PFS, grade 3–4 toxicity, OS, ORR, PD, SAEs, OTD, DDR, DDAEs | Some Comcerns |
| Yao et al., 2011 [25,26] | 203 | - | 207 | - | - | - | - | PFS, grade 3–4 toxicity, OS, ORR, PD, AEs, SAEs, OTD, DDR, DDAEs | Low risk |
| Raymond et al., 2011 [27] | 85 | - | - | 86 | - | - | - | PFS, grade 3–4 toxicity, OS, ORR, PD, AEs, SAEs, OTD, DDR, DDAEs | Low risk |
| Caplin et al., 2014 [28] | 103 | 101 | - | - | - | - | - | PFS, grade 3–4 toxicity, OS, PD, AEs, SAEs, OTD, DDR, DDAEs | Low risk |
| Yao et al., 2016 [29] | 97 | - | 205 | - | - | - | - | PFS, grade 3–4 toxicity, OS, ORR, PD, AEs, SAEs, OTD, DDR, DDAEs | Low risk |
| Strosberg et al., 2017 [30] | - | 113 | - | - | 116 | - | - | PFS, grade 3–4 toxicity, OS, ORR, PD, AEs, SAEs, DDR, DDAEs | Low Risk |
| Yao et al., 2017 [31] | - | - | - | - | - | 213 | 214 | PFS, grade 3–4 toxicity, OS, ORR, PD, SAEs, OTD, DDR, DDAEs | Low Risk |
| Total | 531 | 520 | 628 | 86 | 116 | 267 | 214 | ||
| Outcomes of Interest | Studies | SUCRA (%) and Rank (Mean) for Arm | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Placebo | SSA Alone | Everolimus ± SSA | Sunitinib Alone | 177Lu-Dotatate + SSA | IFN-α + SSA | Bevacizumab + SSA | |||||||||
| SUCRA | Rank | SUCRA | Rank | SUCRA | Rank | SUCRA | Rank | SUCRA | Rank | SUCRA | Rank | SUCRA | Rank | ||
| Progression-Free Survival | 9 | 7.6 | 6.5 | 46.6 | 4.2 | 33.6 | 5.0 | 64.5 | 3.1 | 99.6 | 1.0 | 53.0 | 3.8 | 45.0 | 4.3 |
| Grade 3–4 toxicity ° | 9 | 73.7 | 2.4 | 65.0 | 3.1 | 3.9 | 6.8 | 28.8 | 5.3 | 49.4 | 4.0 | 52.4 | 3.9 | 76.7 | 2.4 |
| Overall Survival | 9 | 32.6 | 5.0 | 48.9 | 4.1 | 43.4 | 4.4 | 93.6 | 1.4 | 87.7 | 1.7 | 31.8 | 5.1 | 11.9 | 6.3 |
| ORR (CR+PR) § | 8 | 6.9 | 5.8 | 20.0 | 5.8 | 32.0 | 5.1 | 74.2 | 2.5 | 68.6 | 2.8 | 59.0 | 3.5 | 88.3 | 1.7 |
| PD § | 9 | 2.6 | 6.8 | 22.8 | 5.6 | 56.9 | 3.6 | 35.0 | 4.9 | 90.6 | 1.6 | 61.3 | 3.3 | 80.8 | 2.2 |
| AEs | 6 | 74.1 | 2.0 | 96.3 | 1.1 | 27.6 | 3.9 | 33.7 | 3.7 | 18.3 | 4.3 | * | * | * | * |
| SAEs | 9 | 60.6 | 3.4 | 76.4 | 2.4 | 31 | 5.1 | 96.5 | 1.2 | 65.6 | 3.1 | 19.9 | 5.8 | 0 | 7.0 |
| On Treatment Deaths | 8 | 61.2 | 2.9 | 56.8 | 3.2 | 15.9 | 5.2 | 87.3 | 1.6 | 34.9 | 4.3 | 43.8 | 3.8 | * | * |
| Deaths Drug-related | 9 | 64.3 | 3.1 | 58.5 | 3.5 | 42.0 | 4.5 | 58.5 | 3.5 | 56.7 | 3.6 | 37.7 | 4.7 | 32.4 | 5.1 |
| Discontinuation for SAE | 9 | 85.7 | 1.9 | 71 | 2.7 | 19.5 | 5.8 | 52.1 | 3.9 | 86.7 | 1.8 | 25 | 5.5 | 10 | 6.4 |
| Outcomes of Interest | Inconsistency | τ Value | Adjusted SUCRA and Rank Values | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Global | Local | Placebo | SSA Alone | Everolimus ± SSA | Sunitinib Alone | 177Lu-Dotatate + SSA | IFN-α + SSA | BevacizumaB + SSA | ||||||||||||
| Chi-Square | p-Value | Loop | RoR | p-Value | SUCRA | Rank | SUCRA | Rank | SUCRA | Rank | SUCRA | Rank | SUCRA | Rank | SUCRA | Rank | SUCRA | Rank | ||
| PFS | 4.86 | 0.027 | ABC | 1.78 | 0.016 | 0.2 | 26.1 | 5.4 | 45.5 | 4.3 | 43.1 | 4.4 | 58.1 | 3.5 | 75.0 | 2.6 | 51.7 | 3.9 | 49.1 | 4.1 |
| Grade 3–4 toxicity | 0.03 | 0.853 | ABC | 1.28 | 0.628 | 0.3 | - | - | - | - | - | - | - | - | - | - | - | - | - | - |
| OS | 0.52 | 0.470 | ABC | 1.27 | 0.443 | 0.1 | - | - | - | - | - | - | - | - | - | - | - | - | - | - |
| ORR (CR + PR) § | 0.14 | 0.707 | ABC | 1.84 | 0.713 | <0.1 | - | - | - | - | - | - | - | - | - | - | - | - | - | - |
| PD § | 1.17 | 0.279 | ABC | 2.26 | 0.144 | 0.4 | - | - | - | - | - | - | - | - | - | - | - | - | - | - |
| AE | 1.75 | 0.185 | ABC | 1.30 | 0.185 | <0.1 | - | - | - | - | - | - | - | - | - | - | - | - | - | - |
| SAE | 0.01 | 0.927 | ABC | 1.04 | 0.928 | <0.1 | - | - | - | - | - | - | - | - | - | - | - | - | - | - |
| On treatment deaths | 0.02 | 0.883 | ABC | 1.18 | 0.877 | <0.1 | - | - | - | - | - | - | - | - | - | - | - | - | - | - |
| Deaths Drug-related | 0.09 | 0.768 | ABC | 2.13 | 0.770 | 0.5 | - | - | - | - | - | - | - | - | - | - | - | - | - | - |
| Discontinuation for SAE | 0.30 | 0.585 | ABC | 1.72 | 0.600 | <0.1 | - | - | - | - | - | - | - | - | - | - | - | - | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ricci, C.; Lamberti, G.; Ingaldi, C.; Mosconi, C.; Pagano, N.; Alberici, L.; Ambrosini, V.; Manuzzi, L.; Monari, F.; Malvi, D.; et al. Treatment of Advanced Gastro-Entero-Pancreatic Neuro-Endocrine Tumors: A Systematic Review and Network Meta-Analysis of Phase III Randomized Controlled Trials. Cancers 2021, 13, 358. https://doi.org/10.3390/cancers13020358
Ricci C, Lamberti G, Ingaldi C, Mosconi C, Pagano N, Alberici L, Ambrosini V, Manuzzi L, Monari F, Malvi D, et al. Treatment of Advanced Gastro-Entero-Pancreatic Neuro-Endocrine Tumors: A Systematic Review and Network Meta-Analysis of Phase III Randomized Controlled Trials. Cancers. 2021; 13(2):358. https://doi.org/10.3390/cancers13020358
Chicago/Turabian StyleRicci, Claudio, Giuseppe Lamberti, Carlo Ingaldi, Cristina Mosconi, Nico Pagano, Laura Alberici, Valentina Ambrosini, Lisa Manuzzi, Fabio Monari, Deborah Malvi, and et al. 2021. "Treatment of Advanced Gastro-Entero-Pancreatic Neuro-Endocrine Tumors: A Systematic Review and Network Meta-Analysis of Phase III Randomized Controlled Trials" Cancers 13, no. 2: 358. https://doi.org/10.3390/cancers13020358