
Immunonutritive Scoring for Patients with Hepatocellular Carcinoma Undergoing Transarterial Chemoembolization: Evaluation of the CALLY Index

 ,
,  , ,
, ,  , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
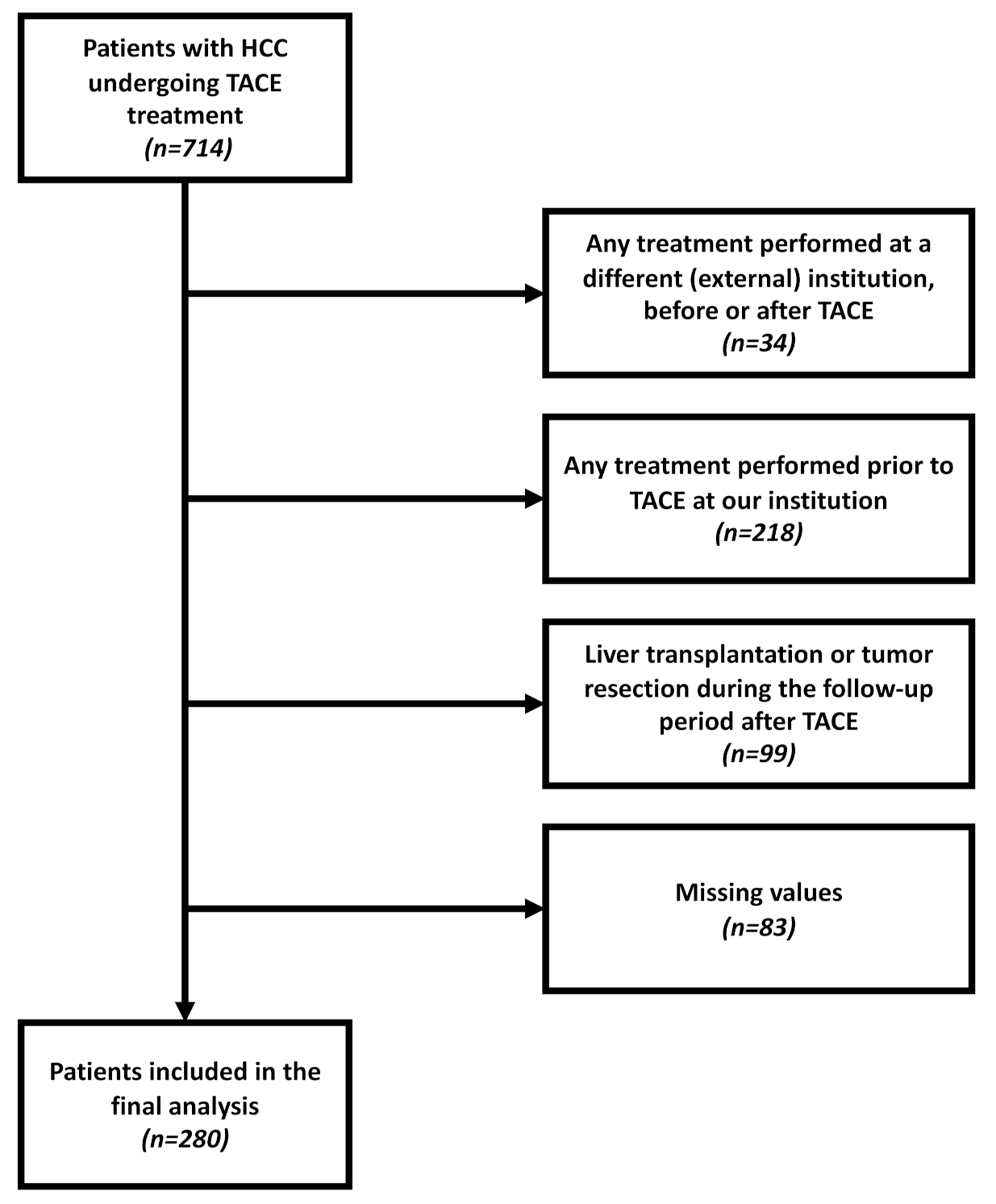
2.1. Patients
2.2. Diagnosis, Treatment, and Follow-Up
2.3. Data Acquisition
2.4. Calculation of the CALLY Index
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Survival Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Global Burden of Disease Liver Cancer Collaboration. The Burden of Primary Liver Cancer and Underlying Etiologies from 1990 to 2015 at the Global, Regional, and National Level: Results From the Global Burden of Disease Study 2015. JAMA Oncol. 2017, 3, 1683–1691. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; Zucman-Rossi, J.; Pikarsky, E.; Sangro, B.; Schwartz, M.; Sherman, M.; Gores, G. Hepatocellular carcinoma. Nat. Rev. Dis. Prim. 2016, 2, 16018. [Google Scholar] [CrossRef] [PubMed]
- Galle, P.R.; Forner, A.; Llovet, J.M.; Mazzaferro, V.; Piscaglia, F.; Raoul, J.-L.; Schirmacher, P.; Vilgrain, V. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heimbach, J.K.; Kulik, L.M.; Finn, R.S.; Sirlin, C.B.; Abecassis, M.M.; Roberts, L.R.; Zhu, A.X.; Murad, M.H.; Marrero, J.A. AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology 2018, 67, 358–380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Llovet, J.M.; Brú, C.; Bruix, J. Prognosis of hepatocellular carcinoma: The BCLC staging classification. In Seminars in Liver Disease; Thieme Medical Publishers, Inc.: New York, NY, USA, 1999; Volume 19, pp. 329–338. [Google Scholar]
- Forner, A.; Reig, M.; Bruix, J. Hepatocellular carcinoma. Lancet 2018, 391, 1301–1314. [Google Scholar] [CrossRef]
- Bolondi, L.; Burroughs, A.; Dufour, J.-F.; Galle, P.R.; Mazzaferro, V.; Piscaglia, F.; Raoul, J.L.; Sangro, B. Heterogeneity of patients with intermediate (BCLC B) Hepatocellular Carcinoma: Proposal for a subclassification to facilitate treatment decisions. In Seminars in Liver Disease; Thieme Medical Publishers: New York, NY, USA, 2012; Volume 32, pp. 348–359. [Google Scholar]
- Chow, P.K.H.; Choo, S.P.; Ng, D.C.E.; Lo, R.H.G.; Wang, M.L.C.; Toh, H.C.; Tai, D.W.M.; Goh, B.K.P.; San Wong, J.; Tay, K.H.; et al. Heterogeneity and subclassification of barcelona clinic liver cancer stage B. Liver Cancer 2016, 5, 91–96. [Google Scholar]
- Hucke, F.; Pinter, M.; Graziadei, I.; Bota, S.; Vogel, W.; Müller, C.; Heinzl, H.; Waneck, F.; Trauner, M.; Peck-Radosavljevic, M.; et al. How to STATE suitability and START transarterial chemoembolization in patients with intermediate stage hepatocellular carcinoma. J. Hepatol. 2014, 61, 1287–1296. [Google Scholar] [CrossRef] [PubMed]
- Kadalayil, L.; Benini, R.; Pallan, L.; O’Beirne, J.; Marelli, L.; Yu, D.; Hackshaw, A.; Fox, R.; Johnson, P.; Burroughs, A.K.; et al. A simple prognostic scoring system for patients receiving transarterial embolisation for hepatocellular cancer. Ann. Oncol. 2013, 24, 2565–2570. [Google Scholar] [CrossRef] [PubMed]
- Park, Y.; Kim, S.U.; Kim, B.K.; Park, J.Y.; Kim, D.Y.; Ahn, S.H.; Park, Y.E.; Park, J.H.; Lee, Y.I.; Yun, H.R.; et al. Addition of tumor multiplicity improves the prognostic performance of the hepatoma arterial-embolization prognostic score. Liver Int. 2016, 36, 100–107. [Google Scholar] [CrossRef]
- Mähringer-Kunz, A.; Wagner, F.; Hahn, F.; Weinmann, A.; Brodehl, S.; Schotten, S.; Hinrichs, J.B.; Düber, C.; Galle, P.R.; Pinto dos Santos, D.; et al. Predicting survival after transarterial chemoembolization for hepatocellular carcinoma using a neural network: A Pilot Study. Liver Int. 2020, 40, 694–703. [Google Scholar] [CrossRef] [Green Version]
- Pinato, D.J.; Arizumi, T.; Jang, J.W.; Allara, E.; Suppiah, P.I.; Smirne, C.; Tait, P.; Pai, M.; Grossi, G.; Kim, Y.W.; et al. Combined sequential use of HAP and ART scores to predict survival outcome and treatment failure following chemoembolization in hepatocellular carcinoma: A multi-center comparative study. Oncotarget 2016, 7, 44705. [Google Scholar] [CrossRef] [Green Version]
- Refolo, M.G.; Messa, C.; Guerra, V.; Carr, B.I.; D’Alessandro, R. Inflammatory mechanisms of HCC development. Cancers 2020, 12, 641. [Google Scholar] [CrossRef] [Green Version]
- Buzby, G.P.; Mullen, J.L.; Matthews, D.C.; Hobbs, C.L.; Rosato, E.F. Prognostic nutritional index in gastrointestinal surgery. Am. J. Surg. 1980, 139, 160–167. [Google Scholar] [CrossRef]
- Sun, K.; Chen, S.; Xu, J.; Li, G.; He, Y. The prognostic significance of the prognostic nutritional index in cancer: A systematic review and meta-analysis. J. Cancer Res. Clin. Oncol. 2014, 140, 1537–1549. [Google Scholar] [CrossRef]
- Müller, L.; Hahn, F.; Mähringer-Kunz, A.; Stoehr, F.; Gairing, S.J.; Foerster, F.; Weinmann, A.; Galle, P.R.; Mittler, J.; Pinto dos Santos, D.; et al. Immunonutritive Scoring in Patients With Hepatocellular Carcinoma Undergoing Transarterial Chemoembolization: Prognostic Nutritional Index or Controlling Nutritional Status Score? Front. Oncol. 2021, 11, 2205. [Google Scholar] [CrossRef]
- Rekik, S.; Guyot, E.; Bhais, M.; Ajavon, Y.; Grando, V.; Bourcier, V.; Nkontchou, G.; Nahon, P.; Sellier, N.; Seror, O.; et al. The CRP level and STATE score predict survival in cirrhotic patients with hepatocellular carcinoma treated by transarterial embolization. Dig. Liver Dis. 2016, 48, 1088–1092. [Google Scholar] [CrossRef]
- Iida, H.; Tani, M.; Komeda, K.; Nomi, T.; Matsushima, H.; Tanaka, S.; Ueno, M.; Nakai, T.; Maehira, H.; Mori, H.; et al. Superiority of CRP-Albumin-Lymphocyte index (CALLY index) as a non-invasive prognostic biomarker after hepatectomy for hepatocellular carcinoma. HPB 2021, in press. [Google Scholar] [CrossRef]
- Kloeckner, R.; Galle, P.R.; Bruix, J. Local and Regional Therapies for Hepatocellular Carcinoma. Hepatology 2021, 73, 137–149. [Google Scholar] [CrossRef]
- Lammer, J.; Malagari, K.; Vogl, T.; Pilleul, F.; Denys, A.; Watkinson, A.; Pitton, M.; Sergent, G.; Pfammatter, T.; Terraz, S.; et al. Prospective Randomized Study of Doxorubicin-Eluting-Bead Embolization in the Treatment of Hepatocellular Carcinoma: Results of the PRECISION V Study. Cardiovasc. Interv. Radiol. 2010, 33, 41–52. [Google Scholar] [CrossRef] [Green Version]
- Lencioni, R.; De Baere, T.; Burrel, M.; Caridi, J.G.; Lammer, J.; Malagari, K.; Martin, R.C.G.; O’Grady, E.; Real, M.I.; Vogl, T.J.; et al. Transcatheter treatment of hepatocellular carcinoma with Doxorubicin-loaded DC Bead (DEBDOX): Technical recommendations. Cardiovasc. Interv. Radiol. 2012, 35, 980–985. [Google Scholar] [CrossRef] [Green Version]
- Weinmann, A.; Koch, S.; Niederle, I.M.; Schulze-Bergkamen, H.; König, J.; Hoppe-Lotichius, M.; Hansen, T.; Pitton, M.B.; Düber, C.; Otto, G.; et al. Trends in epidemiology, treatment, and survival of hepatocellular carcinoma patients between 1998 and 2009: An analysis of 1066 cases of a German HCC Registry. J. Clin. Gastroenterol. 2014, 48, 279–289. [Google Scholar] [CrossRef]
- Huang, Z.-L.; Luo, J.; Chen, M.-S.; Li, J.-Q.; Shi, M. Blood neutrophil-to-lymphocyte ratio predicts survival in patients with unresectable hepatocellular carcinoma undergoing transarterial chemoembolization. J. Vasc. Interv. Radiol. 2011, 22, 702–709. [Google Scholar] [CrossRef]
- Zheng, J.; Cai, J.; Li, H.; Zeng, K.; He, L.; Fu, H.; Zhang, J.; Chen, L.; Yao, J.; Zhang, Y.; et al. Neutrophil to lymphocyte ratio and platelet to lymphocyte ratio as prognostic predictors for hepatocellular carcinoma patients with various treatments: A meta-analysis and systematic review. Cell. Physiol. Biochem. 2017, 44, 967–981. [Google Scholar] [CrossRef]
- Wang, B.; Huang, Y.; Lin, T. Prognostic impact of elevated pre-treatment systemic immune-inflammation index (SII) in hepatocellular carcinoma: A meta-analysis. Medicine 2020, 99, e18571. [Google Scholar] [CrossRef]
- Chan, S.L.; Wong, L.-L.; Chan, K.-C.A.; Chow, C.; Tong, J.H.-M.; Yip, T.C.-F.; Wong, G.L.-H.; Chong, C.C.-N.; Liu, P.-H.; Chu, C.-M.; et al. Development of a novel inflammation-based index for hepatocellular carcinoma. Liver Cancer 2020, 9, 167–181. [Google Scholar] [CrossRef]
- Yang, Z.; Zhang, J.; Lu, Y.; Xu, Q.; Tang, B.; Wang, Q.; Zhang, W.; Chen, S.; Lu, L.; Chen, X. Aspartate aminotransferase-lymphocyte ratio index and systemic immune-inflammation index predict overall survival in HBV-related hepatocellular carcinoma patients after transcatheter arterial chemoembolization. Oncotarget 2015, 6, 43090. [Google Scholar] [CrossRef] [Green Version]
- Uno, H.; Cai, T.; Pencina, M.J.; D’Agostino, R.B.; Wei, L.-J. On the C-statistics for evaluating overall adequacy of risk prediction procedures with censored survival data. Stat. Med. 2011, 30, 1105–1117. [Google Scholar] [CrossRef] [Green Version]
- Yu, L.-X.; Ling, Y.; Wang, H.-Y. Role of nonresolving inflammation in hepatocellular carcinoma development and progression. NPJ Precis. Oncol. 2018, 2, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El–Serag, H.B.; Rudolph, K.L. Hepatocellular Carcinoma: Epidemiology and Molecular Carcinogenesis. Gastroenterology 2007, 132, 2557–2576. [Google Scholar] [CrossRef] [PubMed]
- Coussens, L.M.; Werb, Z. Inflammation and cancer. Nature 2002, 420, 860–867. [Google Scholar] [CrossRef] [PubMed]
- He, C.-B.; Lin, X.-J. Inflammation scores predict the survival of patients with hepatocellular carcinoma who were treated with transarterial chemoembolization and recombinant human type-5 adenovirus H101. PLoS ONE 2017, 12, e0174769. [Google Scholar] [CrossRef]
- Liu, Y.; Shi, M.; Chen, S.; Wan, W.; Shen, L.; Shen, B.; Qi, H.; Cao, F.; Wu, Y.; Huang, T.; et al. Intermediate stage hepatocellular carcinoma: Comparison of the value of inflammation-based scores in predicting progression-free survival of patients receiving transarterial chemoembolization. J. Cancer Res. Ther. 2021, 17, 740. [Google Scholar]
- Li, S.; Feng, X.; Cao, G.; Wang, Q.; Wang, L. Prognostic significance of inflammatory indices in hepatocellular carcinoma treated with transarterial chemoembolization: A systematic review and meta-analysis. PLoS ONE 2020, 15, e0230879. [Google Scholar] [CrossRef] [Green Version]
- Walsh, S.R.; Cook, E.J.; Goulder, F.; Justin, T.A.; Keeling, N.J. Neutrophil-lymphocyte ratio as a prognostic factor in colorectal cancer. J. Surg. Oncol. 2005, 91, 181–184. [Google Scholar] [CrossRef]
- Smith, R.A.; Bosonnet, L.; Raraty, M.; Sutton, R.; Neoptolemos, J.P.; Campbell, F.; Ghaneh, P. Preoperative platelet-lymphocyte ratio is an independent significant prognostic marker in resected pancreatic ductal adenocarcinoma. Am. J. Surg. 2009, 197, 466–472. [Google Scholar] [CrossRef]
- Hu, B.; Yang, X.-R.; Xu, Y.; Sun, Y.-F.; Sun, C.; Guo, W.; Zhang, X.; Wang, W.-M.; Qiu, S.-J.; Zhou, J.; et al. Systemic immune-inflammation index predicts prognosis of patients after curative resection for hepatocellular carcinoma. Clin. Cancer Res. 2014, 20, 6212–6222. [Google Scholar] [CrossRef] [Green Version]
- Müller, L.; Stoehr, F.; Mähringer-Kunz, A.; Hahn, F.; Weinmann, A.; Kloeckner, R. Current Strategies to Identify Patients that Will Benefit from TACE Treatment and Future Directions a Practical Step-by-Step Guide. J. Hepatocell. Carcinoma 2021, 8, 403. [Google Scholar] [CrossRef]
- Pugh, R.N.H.; Murray-Lyon, I.M.; Dawson, J.L.; Pietroni, M.C.; Williams, R. Transection of the oesophagus for bleeding oesophageal varices. Br. J. Surg. 1973, 60, 646–649. [Google Scholar] [CrossRef]
- Johnson, P.J.; Berhane, S.; Kagebayashi, C.; Satomura, S.; Teng, M.; Reeves, H.L.; O’Beirne, J.; Fox, R.; Skowronska, A.; Palmer, D.; et al. Assessment of liver function in patients with hepatocellular carcinoma: A new evidence-based approach—The ALBI grade. J. Clin. Oncol. 2015, 33, 550. [Google Scholar] [CrossRef]
- Pinato, D.J.; Sharma, R.; Allara, E.; Yen, C.; Arizumi, T.; Kubota, K.; Bettinger, D.; Jang, J.W.; Smirne, C.; Kim, Y.W.; et al. The ALBI grade provides objective hepatic reserve estimation across each BCLC stage of hepatocellular carcinoma. J. Hepatol. 2017, 66, 338–346. [Google Scholar] [CrossRef] [Green Version]
- Vogeler, M.; Mohr, I.; Pfeiffenberger, J.; Sprengel, S.D.; Klauss, M.; Teufel, A.; Chang, D.-H.; Springfeld, C.; Longerich, T.; Merle, U.; et al. Applicability of scoring systems predicting outcome of transarterial chemoembolization for hepatocellular carcinoma. J. Cancer Res. Clin. Oncol. 2020, 146, 1033–1050. [Google Scholar] [CrossRef] [Green Version]
- Zheng, Z.; Zhou, L.; Gao, S.; Yang, Z. Prognostic role of C-reactive protein in hepatocellular carcinoma: A systematic review and meta-analysis. Int. J. Med. Sci. 2013, 10, 653. [Google Scholar] [CrossRef] [Green Version]
- Pan, J.; Chen, S.; Tian, G.; Jiang, T. Preoperative Albumin–Bilirubin Grade With Prognostic Nutritional Index Predicts the Outcome of Patients With Early-Stage Hepatocellular Carcinoma After Percutaneous Radiofrequency Ablation. Front. Med. 2020, 7, 584871. [Google Scholar] [CrossRef] [PubMed]
- Müller, L.; Hahn, F.; Mähringer-Kunz, A.; Stoehr, F.; Gairing, S.J.; Foerster, F.; Weinmann, A.; Galle, P.R.; Mittler, J.; Pinto dos Santos, D.; et al. Refining Prognosis in Chemoembolization for Hepatocellular Carcinoma: Immunonutrition and Liver Function. Cancers 2021, 13, 3961. [Google Scholar] [CrossRef]
- Fujiwara, N.; Nakagawa, H.; Kudo, Y.; Tateishi, R.; Taguri, M.; Watadani, T.; Nakagomi, R.; Kondo, M.; Nakatsuka, T.; Minami, T.; et al. Sarcopenia, intramuscular fat deposition, and visceral adiposity independently predict the outcomes of hepatocellular carcinoma. J. Hepatol. 2015, 63, 131–140. [Google Scholar] [CrossRef] [Green Version]
- Imai, K.; Takai, K.; Watanabe, S.; Hanai, T.; Suetsugu, A.; Shiraki, M.; Shimizu, M. Sarcopenia Impairs Prognosis of Patients with Hepatocellular Carcinoma: The Role of Liver Functional Reserve and Tumor-Related Factors in Loss of Skeletal Muscle Volume. Nutrients 2017, 9, 1054. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variable | All Patients (n = 280) | Patients Classified as BCLC B (n = 154) |
|---|---|---|
| Age, years | 69.5 (62.5–75.4) | 70.2 (63.3–75.6) |
| Sex, n (%) | ||
| Female | 46 (16.4) | 23 (14.9) |
| Male | 234 (83.6) | 131 (85.1) |
| Etiology, n (%) | ||
| Alcohol | 131 (46.8) | 70 (45.5) |
| Hepatitis C | 46 (16.4) | 25 (16.2) |
| Hepatitis B | 26 (9.3) | 17 (11.0) |
| NASH | 27 (9.6) | 15 (9.7) |
| Hemochromatosis | 5 (1.8) | 3 (2.0) |
| AIH/PBC/PSC | 5 (1.8) | 3 (2.0) |
| Unknown/Other | 29 (10.4) | 13 (8.4) |
| None | 11 (3.9) | 8 (5.2) |
| Child–Pugh stage, n (%) | ||
| A | 104 (37.2) | 60 (39.0) |
| B | 116 (41.4) | 74 (48.0) |
| C | 25 (8.9) | 0 |
| No cirrhosis | 35 (12.5) | 20 (13.0) |
| BCLC stage, n (%) | ||
| 0 | 0 | 0 |
| A | 45 (16.1) | 0 |
| B | 154 (55.0) | 154 (100) |
| C | 58 (20.7) | 0 |
| D | 23 (8.2) | 0 |
| Max. tumor size, cm | 4.2 (2.9–6.4) | 4.3 (3.2–6.1) |
| Tumor number, n (%) | ||
| Unifocal | 55 (19.6) | 0 |
| Multifocal | 203 (72.5) | 146 (94.8) |
| Diffuse growth pattern | 22 (7.9) | 8 (5.2) |
| Albumin level, g/L | 31 (27–35) | 31 (28–35) |
| Lymphocyte count, per mm3 | 1214 (83–1558) | 1263 (841–1660) |
| Bilirubin level, mg/dL | 1.3 (0.8–2.2) | 1.3 (0.9–2.0) |
| Platelet count, per nL | 128 (87–193) | 119 (84–194) |
| AST level, U/L | 64.5 (47.0–95.5) | 63.0 (47.0–88.5) |
| ALT level, U/L | 41.5 (28.0–61.0) | 42.0 (28.0–62.0) |
| AP level, U/L | 156.0 (114.0–212.3) | 146.5 (104.0–201.8) |
| CRP level, mg/L | 9.0 (3.6–18.0) | 8.0 (3.6–15.8) |
| INR | 1.2 (1.1–1.3) | 1.1 (1.0–1.3) |
| AFP level, ng/mL | 45.0 (8.1–777.0) | 48.0 (7.6–593.5) |
| Analysis | Univariate | Multivariate | |||||
|---|---|---|---|---|---|---|---|
| Covariate | Cut-Off | HR | 95% CI | p-Value | HR | 95% CI | p-Value |
| CALLY | <1 point | 1.9 | 1.4–2.6 | <0.001 | 1.5 | 1.1–2.1 | 0.008 |
| Age | ≥70 years | 1.0 | 0.8–1.3 | 0.960 | |||
| AFP | >400 ng/mL | 0.9 | 0.7–1.2 | 0.620 | |||
| Bilirubin level | ≥1.2 mg/dL | 2.1 | 1.6–2.7 | <0.001 | 1.8 | 1.4–2.5 | <0.001 |
| AST level | >31 U/L | 2.0 | 1.1–3.7 | 0.025 | 2.0 | 1.1–3.6 | 0.033 |
| ALT level | ≥35 U/L | 1.2 | 0.9–1.6 | 0.200 | |||
| INR level | >1.2 | 1.1 | 0.8–1.5 | 0.460 | |||
| Platelet count | >150/nL | 1.3 | 0.9–1.7 | 0.140 | |||
| Tumor number | ≥2 | 1.5 | 1.0–2.1 | 0.027 | 1.2 | 0.8–1.6 | 0.388 |
| Max. lesion size | >5.0 cm | 1.3 | 1.0–1.7 | 0.058 | |||
| Analysis | Univariate | Multivariate | |||||
|---|---|---|---|---|---|---|---|
| Covariate | Cut-off | HR | 95% CI | p-Value | HR | 95% CI | p-Value |
| CALLY | <1 point | 1.9 | 1.3–2.9 | 0.002 | 1.5 | 1.1–2.1 | 0.010 |
| Age | ≥70 years | 1.0 | 0.7–1.5 | 0.930 | |||
| AFP | >400 ng/mL | 1.0 | 0.7–1.4 | 0.790 | |||
| Bilirubin level | ≥1.2 mg/dL | 1.9 | 1.3–2.8 | <0.001 | 1.9 | 1.4–2.5 | <0.001 |
| AST level | >31 U/L | 1.5 | 0.7–2.9 | 0.280 | |||
| ALT level | ≥35 U/L | 1.3 | 0.9–1.9 | 0.230 | |||
| INR level | >1.2 | 1.1 | 0.7–1.6 | 0.770 | |||
| Platelet count | >150/nL | 1.1 | 0.7–1.7 | 0.720 | |||
| Max. lesion size | >5.0 cm | 1.5 | 1.0–2.3 | 0.035 | 1.3 | 1.0–1.7 | 0.069 |
| Analysis | Univariate | Multivariate | ||||
|---|---|---|---|---|---|---|
| Covariate | HR | 95% CI | p-Value | HR | 95% CI | p-Value |
| All patients (n = 280) | ||||||
| Serum albumin level ≤ 31 g/L | 2.5 | 1.9–3.3 | <0.001 | 1.9 | 1.4–2.6 | <0.001 |
| Total lymphocyte count ≤ 647.9/mm3 | 1.7 | 1.2–2.5 | 0.005 | 1.5 | 1.0–2.2 | 0.036 |
| Serum CRP level ≤ 12 mg/L | 3.7 | 2.8–5.0 | <0.001 | 3.0 | 2.2–4.1 | <0.001 |
| BCLC B subgroup (n = 164) | ||||||
| Serum albumin level ≤29 g/L | 2.6 | 1.7–3.8 | <0.001 | 2.4 | 1.6–3.6 | <0.001 |
| Total lymphocyte count ≤ 727/mm3 | 2.2 | 1.4–3.5 | <0.001 | 1.7 | 1.0–2.7 | 0.038 |
| Serum CRP level ≤ 4 mg/L | 2.0 | 1.3–3.1 | <0.001 | 2.0 | 1.3–3.0 | 0.001 |
| Score | Median OS | HR | 95% CI | p-Value | C-Index | |
|---|---|---|---|---|---|---|
| All Patients (n = 280) | ||||||
| CALLY | ≥1 | 24.0 | Reference | 0.60 | ||
| <1 | 9.0 | 1.9 | 1.4–2.6 | <0.001 | ||
| NLR | ≤3 | 16.5 | Reference | 0.59 | ||
| >3 | 7.6 | 1.8 | 1.4–2.4 | <0.001 | ||
| PLR | <164 | 12.8 | Reference | 0.54 | ||
| ≥164 | 10.2 | 1.3 | 1.0–1.8 | 0.082 | ||
| PNI | >36 | 18.8 | Reference | 0.63 | ||
| ≤36 | 6.5 | 2.4 | 1.8–3.2 | <0.001 | ||
| SII | <664 | 13.8 | Reference | 0.56 | ||
| ≥664 | 8.6 | 1.5 | 1.1–2.1 | 0.006 | ||
| ILIS | <11 | 18.8 | Reference | 0.57 | ||
| ≥11 | 10.2 | 1.5 | 1.3–2.5 | <0.001 | ||
| BLCL B subgroup (n = 164) | ||||||
| CALLY | ≥1 | 26.2 | Reference | 0.61 | ||
| <1 | 13.1 | 1.9 | 1.3–2.9 | 0.002 | ||
| NLR | ≤3 | 18.3 | Reference | 0.59 | ||
| >3 | 9.0 | 2.5 | 1.6–3.8 | <0.001 | ||
| PLR | <214 | 16.5 | Reference | 0.55 | ||
| ≥214 | 7.5 | 2.5 | 1.4–4.4 | 0.002 | ||
| PNI | >39 | 20.9 | Reference | 0.63 | ||
| ≤39 | 10.3 | 1.9 | 1.3–2.8 | <0.001 | ||
| SII | <622 | 16.7 | Reference | 0.55 | ||
| ≥622 | 10.0 | 1.9 | 1.2–3.1 | 0.007 | ||
| ILIS | <31 | 17.9 | Reference | 0.58 | ||
| ≥31 | 10.4 | 2.0 | 1.4–3.0 | <0.001 | ||
| Index | Concept and Characteristics | Included Parameters | Pros | Cons | Current Research Status | Future Research Strategies |
|---|---|---|---|---|---|---|
| Immunonutritive Indices | ||||||
| CALLY | - combines inflammation, immune response, and nutritional status markers (aspects of the PNI) - for liver disease, albumin functions as an indicator of liver function | - CRP - albumin - lymphocyte count | - novel combination of inflammation, immune response, nutritional status, and liver function markers provides a more holistic assessment | - scarce literature available - in this study, CALLY was not superior to previously established scoring systems | - designed for a cohort of patients with HCC undergoing resections [19] - only validated in this study for patients with HCC undergoing TACE | - further validation needed for patients with HCC undergoing TACE - validation for assessing other HCC treatment options - efficacy of CALLY combined with bilirubin - the mathematical calculation may require improvement |
| PNI | - combines immune response and nutritional status markers | - albumin - lymphocyte count | - combination of immune response and nutritional status markers | - few studies available on patients with HCC undergoing TACE - divergent results regarding the predictive ability of PNI - the mathematical calculation may require improvement | - designed for patients with gastric cancer [15] - extensively validated for various cancer entities - few studies available for patients with HCC undergoing TACE - divergent results on its predictive ability - PNI combined with ALBI was identified as a novel, feasible stratification system for patients with HCC undergoing TACE | - further, large-scale validation needed for patients with HCC undergoing TACE - the integration of immunonutrition into existing stratification systems |
| Other Immune-Based Indices | ||||||
| NLR | - captures shifts in the relationships between blood cells, due to immune response effects | - neutrophil count - lymphocyte count | - simple calculation - well investigated | - nutritional status not included - divergent results in studies that compared NLR to other immune-based indices | - designed for the stratification of critically ill patients, and validated in patients with colorectal cancer, in an oncologic context [36] - extensively validated for various cancer entities, including patients with HCC undergoing TACE | - NLR combined with nutritional status markers - NLR combined with liver function markers - large-scale validation for patients with HCC undergoing TACE - integration into existing stratification tools |
| PLR | - captures shifts in the relationships between blood cells, due to immune response effects | - platelet count - lymphocyte count | - simple calculation - well investigated | - nutritional status not included - divergent results in studies that compared PLR to other immune-based indices | - designed for the stratification of patients with pancreatic cancer [37] - extensively validated for patients with HCC undergoing TACE | - PLR combined with nutritional status markers - PLR combined with liver function markers - further large-scale validation for patients with HCC undergoing TACE - integration into existing stratification tools |
| SII | - combines inflammation and immune response markers | - lymphocyte count - neutrophil count - platelet count | - extensively validated for patients with HCC | - nutritional status not included - literature is scarce for patients undergoing TACE | - designed for the stratification of patients with HCC undergoing resections [38] - extensively validated for various cancer entities - few studies on the role of the SII in patients undergoing TACE | - SII combined with nutritional status markers - SII combined with liver function markers - further large-scale validation for patients with HCC undergoing TACE - integration into existing stratification tools |
| ILIS | - combines inflammation, liver function, and tumor markers - specifically developed for patients with HCC | - albumin - bilirubin - alkaline phosphatase - neutrophil count | - index is specific for HCC - includes tumor and liver function markers | - complex calculation - scarce literature for patients with HCC, particularly for patients undergoing TACE | - specifically designed for patients with HCC [27] - only one external validation study available | - large-scale validation is mandatory - integration into existing stratification tools |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Müller, L.; Hahn, F.; Mähringer-Kunz, A.; Stoehr, F.; Gairing, S.J.; Michel, M.; Foerster, F.; Weinmann, A.; Galle, P.R.; Mittler, J.; et al. Immunonutritive Scoring for Patients with Hepatocellular Carcinoma Undergoing Transarterial Chemoembolization: Evaluation of the CALLY Index. Cancers 2021, 13, 5018. https://doi.org/10.3390/cancers13195018
Müller L, Hahn F, Mähringer-Kunz A, Stoehr F, Gairing SJ, Michel M, Foerster F, Weinmann A, Galle PR, Mittler J, et al. Immunonutritive Scoring for Patients with Hepatocellular Carcinoma Undergoing Transarterial Chemoembolization: Evaluation of the CALLY Index. Cancers. 2021; 13(19):5018. https://doi.org/10.3390/cancers13195018
Chicago/Turabian StyleMüller, Lukas, Felix Hahn, Aline Mähringer-Kunz, Fabian Stoehr, Simon Johannes Gairing, Maurice Michel, Friedrich Foerster, Arndt Weinmann, Peter Robert Galle, Jens Mittler, and et al. 2021. "Immunonutritive Scoring for Patients with Hepatocellular Carcinoma Undergoing Transarterial Chemoembolization: Evaluation of the CALLY Index" Cancers 13, no. 19: 5018. https://doi.org/10.3390/cancers13195018