
Reproducibility of mRNA-Based Testing of ESR1, PGR, ERBB2, and MKI67 Expression in Invasive Breast Cancer—A Europe-Wide External Quality Assessment

 , , , , , add
Show full author list
, , , , , add
Show full author list
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Sample Cohort
2.2. Immunohistochemical (IHC) Expression of ER, PgR, HER2, and Ki-67 and IHC Subtyping
- Samples with ER or PgR IHC ≥1% positive stained cells, regardless of staining intensity, were classified as positive (<10% as low positive); samples with <1% cells staining at any intensity were classified as negative [8,9,20,21]. ER and/or PgR positivity were summarized as hormone receptor positivity (HR+).
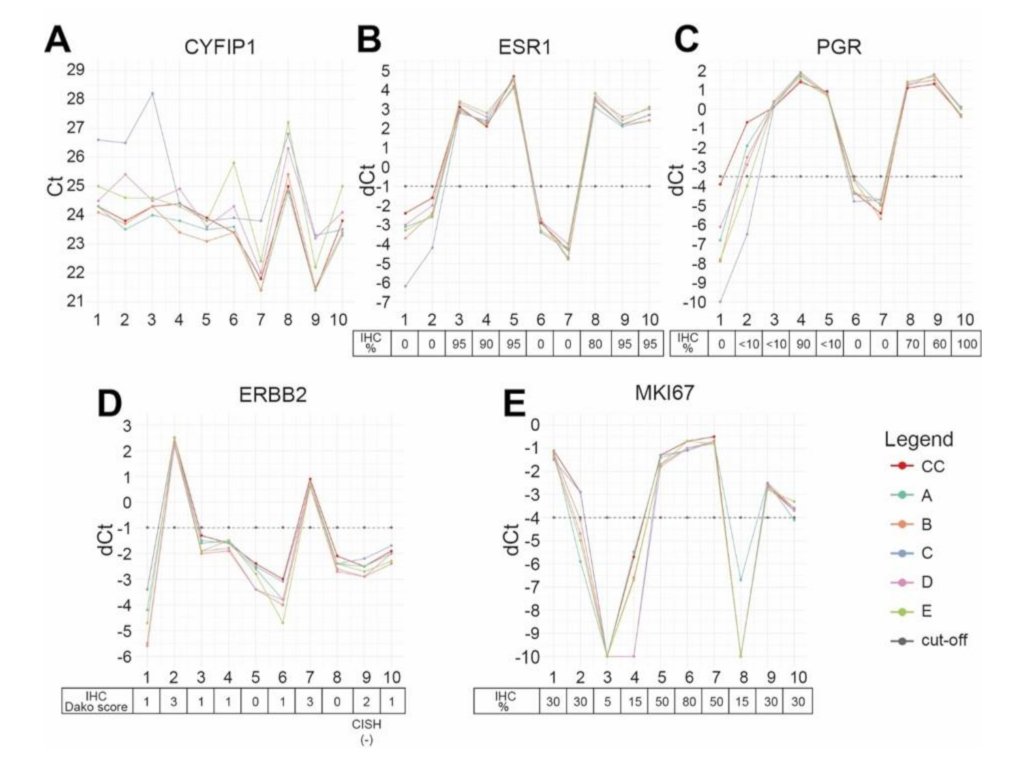
2.3. mRNA-Based Testing of ESR1, PGR, ERBB2, and MKI67 in the Coordinating Center
2.4. EQA Implementation
2.5. Re-Evaluation of Discrepant Cases
2.6. Statistical Analysis
3. Results
3.1. Comparison of Binary STRAT4 Results
3.2. Re-Evaluation of Discrepant Cases
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Perou, C.M.; Sorlie, T.; Eisen, M.B.; van de Rijn, M.; Jeffrey, S.S.; Rees, C.A.; Pollack, J.R.; Ross, D.T.; Johnsen, H.; Akslen, L.A.; et al. Molecular portraits of human breast tumours. Nature 2000, 406, 747–752. [Google Scholar] [CrossRef] [PubMed]
- Sorlie, T.; Perou, C.M.; Tibshirani, R.; Aas, T.; Geisler, S.; Johnsen, H.; Hastie, T.; Eisen, M.B.; van de Rijn, M.; Jeffrey, S.S.; et al. Gene expression patterns of breast carcinomas distinguish tumor subclasses with clinical implications. Proc. Natl. Acad. Sci. USA 2001, 98, 10869–10874. [Google Scholar] [CrossRef] [Green Version]
- Paik, S.; Shak, S.; Tang, G.; Kim, C.; Baker, J.; Cronin, M.; Baehner, F.L.; Walker, M.G.; Watson, D.; Park, T.; et al. A Multigene Assay to Predict Recurrence of Tamoxifen-Treated, Node-Negative Breast Cancer. N. Engl. J. Med. 2004, 351, 2817–2826. [Google Scholar] [CrossRef] [Green Version]
- Curigliano, G.; Burstein, H.J.; Winer, E.P.; Gnant, M.; Dubsky, P.; Loibl, S.; Colleoni, M.; Regan, M.M.; Piccart-Gebhart, M.; Senn, H.J.; et al. De-escalating and escalating treatments for early-stage breast cancer: The St. Gallen International Expert Consensus Conference on the Primary Therapy of Early Breast Cancer 2017. Ann. Oncol. 2017, 28, 1700–1712. [Google Scholar] [CrossRef] [PubMed]
- Goldhirsch, A.; Winer, E.P.; Coates, A.S.; Gelber, R.D.; Piccart-Gebhart, M.; Thurlimann, B.; Senn, H.J.; Panel, M. Personalizing the treatment of women with early breast cancer: Highlights of the St Gallen International Expert Consensus on the Primary Therapy of Early Breast Cancer 2013. Ann. Oncol. Off. J. Eur. Soc. Med Oncol. 2013, 24, 2206–2223. [Google Scholar] [CrossRef]
- Dowsett, M.; Nielsen, T.O.; A’Hern, R.; Bartlett, J.; Coombes, R.C.; Cuzick, J.; Ellis, M.; Henry, N.L.; Hugh, J.C.; Lively, T.; et al. Assessment of Ki67 in breast cancer: Recommendations from the International Ki67 in Breast Cancer working group. J. Natl. Cancer Inst. 2011, 103, 1656–1664. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gonzalez-Ericsson, P.I.; Stovgaard, E.S.; Sua, L.F.; Reisenbichler, E.; Kos, Z.; Carter, J.M.; Michiels, S.; Le Quesne, J.; Nielsen, T.O.; Lænkholm, A.-V.; et al. The path to a better biomarker: Application of a risk management framework for the implementation of PD-L1 and TILs as immuno-oncology biomarkers into breast cancer clinical trials and daily practice. J. Pathol. 2020, 250, 667–684. [Google Scholar] [CrossRef] [Green Version]
- Hammond, M.E.; Hayes, D.F.; Dowsett, M.; Allred, D.C.; Hagerty, K.L.; Badve, S.; Fitzgibbons, P.L.; Francis, G.; Goldstein, N.S.; Hayes, M.; et al. American Society of Clinical Oncology/College of American Pathologists guideline recommendations for immunohistochemical testing of estrogen and progesterone receptors in breast cancer (unabridged version). Arch. Pathol. Lab. Med. 2010, 134, e48–e72. [Google Scholar] [CrossRef]
- Allison, K.H.; Hammond, M.E.H.; Dowsett, M.; McKernin, S.E.; Carey, L.A.; Fitzgibbons, P.L.; Hayes, D.F.; Lakhani, S.R.; Chavez-MacGregor, M.; Perlmutter, J.; et al. Estrogen and Progesterone Receptor Testing in Breast Cancer: ASCO/CAP Guideline Update. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2020, 38, 1346–1366. [Google Scholar] [CrossRef]
- Wolff, A.C.; Hammond, M.E.; Schwartz, J.N.; Hagerty, K.L.; Allred, D.C.; Cote, R.J.; Dowsett, M.; Fitzgibbons, P.L.; Hanna, W.M.; Langer, A.; et al. American Society of Clinical Oncology/College of American Pathologists guideline recommendations for human epidermal growth factor receptor 2 testing in breast cancer. Arch. Pathol. Lab. Med. 2007, 131, 18–43. [Google Scholar] [CrossRef]
- Wolff, A.C.; Hammond, M.E.; Hicks, D.G.; Dowsett, M.; McShane, L.M.; Allison, K.H.; Allred, D.C.; Bartlett, J.M.; Bilous, M.; Fitzgibbons, P.; et al. Recommendations for human epidermal growth factor receptor 2 testing in breast cancer: American Society of Clinical Oncology/College of American Pathologists clinical practice guideline update. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2013, 31, 3997–4013. [Google Scholar] [CrossRef] [PubMed]
- Wolff, A.C.; Hammond, M.E.H.; Allison, K.H.; Harvey, B.E.; Mangu, P.B.; Bartlett, J.M.S.; Bilous, M.; Ellis, I.O.; Fitzgibbons, P.; Hanna, W.; et al. Human Epidermal Growth Factor Receptor 2 Testing in Breast Cancer: American Society of Clinical Oncology/College of American Pathologists Clinical Practice Guideline Focused Update. Arch. Pathol. Lab. Med. 2018, 142, 1364–1382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Viale, G.; Giobbie-Hurder, A.; Regan, M.M.; Coates, A.S.; Mastropasqua, M.G.; Dell’Orto, P.; Maiorano, E.; MacGrogan, G.; Braye, S.G.; Ohlschlegel, C.; et al. Prognostic and predictive value of centrally reviewed Ki-67 labeling index in postmenopausal women with endocrine-responsive breast cancer: Results from Breast International Group Trial 1-98 comparing adjuvant tamoxifen with letrozole. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2008, 26, 5569–5575. [Google Scholar] [CrossRef] [PubMed]
- Erber, R.; Gluz, O.; Brunner, N.; Kreipe, H.H.; Pelz, E.; Kates, R.; Bartels, A.; Huober, J.; Mohrmann, S.; Moustafa, Z.; et al. Predictive role of HER2/neu, topoisomerase-II-alpha, and tissue inhibitor of metalloproteinases (TIMP-1) for response to adjuvant taxane-based chemotherapy in patients with intermediate-risk breast cancer: Results from the WSG-AGO EC-Doc trial. Breast Cancer Res. Treat. 2015, 150, 279–288. [Google Scholar] [CrossRef] [PubMed]
- Polley, M.Y.; Leung, S.C.; McShane, L.M.; Gao, D.; Hugh, J.C.; Mastropasqua, M.G.; Viale, G.; Zabaglo, L.A.; Penault-Llorca, F.; Bartlett, J.M.; et al. An international Ki67 reproducibility study. J. Natl. Cancer Inst. 2013, 105, 1897–1906. [Google Scholar] [CrossRef] [PubMed]
- Hammond, M.E.; Hayes, D.F.; Dowsett, M.; Allred, D.C.; Hagerty, K.L.; Badve, S.; Fitzgibbons, P.L.; Francis, G.; Goldstein, N.S.; Hayes, M.; et al. American Society of Clinical Oncology/College Of American Pathologists guideline recommendations for immunohistochemical testing of estrogen and progesterone receptors in breast cancer. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2010, 28, 2784–2795. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldhirsch, A.; Wood, W.C.; Gelber, R.D.; Coates, A.S.; Thurlimann, B.; Senn, H.J. Meeting highlights: Updated international expert consensus on the primary therapy of early breast cancer. J. Clin. Oncol. 2003, 21, 3357–3365. [Google Scholar] [CrossRef]
- Goldhirsch, A.; Glick, J.H.; Gelber, R.D.; Coates, A.S.; Thurlimann, B.; Senn, H.J. Meeting highlights: International expert consensus on the primary therapy of early breast cancer 2005. Ann. Oncol. Off. J. Eur. Soc. Med Oncol. 2005, 16, 1569–1583. [Google Scholar] [CrossRef]
- Cheang, M.C.U.; Chia, S.K.; Voduc, D.; Gao, D.; Leung, S.; Snider, J.; Watson, M.; Davies, S.; Bernard, P.S.; Parker, J.S.; et al. Ki67 index, HER2 status, and prognosis of patients with luminal B breast cancer. J. Natl. Cancer Inst. 2009, 101, 736–750. [Google Scholar] [CrossRef] [Green Version]
- Landmann, A.; Farrugia, D.J.; Zhu, L.; Diego, E.J.; Johnson, R.R.; Soran, A.; Dabbs, D.J.; Clark, B.Z.; Puhalla, S.L.; Jankowitz, R.C.; et al. Low Estrogen Receptor (ER)-Positive Breast Cancer and Neoadjuvant Systemic Chemotherapy: Is Response Similar to Typical ER-Positive or ER-Negative Disease? Am. J. Clin. Pathol. 2018, 150, 34–42. [Google Scholar] [CrossRef]
- Chen, T.; Zhang, N.; Moran, M.S.; Su, P.; Haffty, B.G.; Yang, Q. Borderline ER-Positive Primary Breast Cancer Gains No Significant Survival Benefit From Endocrine Therapy: A Systematic Review and Meta-Analysis. Clin. Breast Cancer 2018, 18, 1–8. [Google Scholar] [CrossRef]
- AGOEV. Guidelines Breast Version 2020 1D. Available online: https://www.ago-online.de/fileadmin/ago-online/downloads/_leitlinien/kommission_mamma/2020/PDF_DE/2020D%2004_Pathologie_mit%20Literatur.pdf (accessed on 21 February 2021).
- Nielsen, T.O.; Leung, S.C.Y.; Rimm, D.L.; Dodson, A.; Acs, B.; Badve, S.; Denkert, C.; Ellis, M.J.; Fineberg, S.; Flowers, M.; et al. Assessment of Ki67 in Breast Cancer: Updated Recommendations from the International Ki67 in Breast Cancer Working Group. J. Natl. Cancer Inst. 2021, 113, 808–819. [Google Scholar] [CrossRef] [PubMed]
- Laible, M.; Schlombs, K.; Kaiser, K.; Veltrup, E.; Herlein, S.; Lakis, S.; Stöhr, R.; Eidt, S.; Hartmann, A.; Wirtz, R.M.; et al. Technical validation of an RT-qPCR in vitro diagnostic test system for the determination of breast cancer molecular subtypes by quantification of ERBB2, ESR1, PGR and MKI67 mRNA levels from formalin-fixed paraffin-embedded breast tumor specimens. BMC Cancer 2016, 16, 398. [Google Scholar] [CrossRef] [Green Version]
- Gupta, S.; Mani, N.R.; Carvajal-Hausdorf, D.E.; Bossuyt, V.; Ho, K.; Weidler, J.; Wong, W.; Rhees, B.; Bates, M.; Rimm, D.L. Macrodissection prior to closed system RT-qPCR is not necessary for estrogen receptor and HER2 concordance with IHC/FISH in breast cancer. Lab. Investig. 2018, 98, 1076–1083. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, N.C.; Wong, W.; Ho, K.E.; Chu, V.C.; Rizo, A.; Davenport, S.; Kelly, D.; Makar, R.; Jassem, J.; Duchnowska, R.; et al. Comparison of central laboratory assessments of ER, PR, HER2, and Ki67 by IHC/FISH and the corresponding mRNAs (ESR1, PGR, ERBB2, and MKi67) by RT-qPCR on an automated, broadly deployed diagnostic platform. Breast Cancer Res. Treat. 2018, 172, 327–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Filipits, M.; Rudas, M.; Singer, C.; Bago-Horvath, Z.; Greil, R.; Balic, M.; Lax, S.; Wu, N.; Zhao, S.; Weidler, J.; et al. mRNA Expression of ER, PR, HER2 and Ki67 are Concordant with Central IHC and Predict Clinical Outcome: A Validation Study from the ABCSG-6 Biomarker Cohort. Ann. Oncol. 2018, 29 (Suppl. 8), 1339. [Google Scholar] [CrossRef]
- Remmele, W.; Stegner, H.E. Recommendation for uniform definition of an immunoreactive score (IRS) for immunohistochemical estrogen receptor detection (ER-ICA) in breast cancer tissue. Pathologe 1987, 8, 138–140. [Google Scholar] [PubMed]
- Bethune, G.C.; Veldhuijzen van Zanten, D.; MacIntosh, R.F.; Rayson, D.; Younis, T.; Thompson, K.; Barnes, P.J. Impact of the 2013 American Society of Clinical Oncology/College of American Pathologists guideline recommendations for human epidermal growth factor receptor 2 (HER2) testing of invasive breast carcinoma: A focus on tumours assessed as ‘equivocal’ for HER2 gene amplification by fluorescence in-situ hybridization. Histopathology 2015, 67, 880–887. [Google Scholar] [CrossRef] [PubMed]
- Viale, G.; On the behalf of the International Breast Cancer Study Group; Regan, M.M.; Mastropasqua, M.G.; Maffini, F.; Maiorano, E. Predictive Value of Tumor Ki-67 Expression in Two Randomized Trials of Adjuvant Chemoendocrine Therapy for Node-Negative Breast Cancer. JNCI J. Natl. Cancer Inst. 2008, 100, 207–212. [Google Scholar] [CrossRef] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing: Vienna, Austria, 2019. Available online: https://www.R-project.org/ (accessed on 21 February 2021).
- Xpert Breast Cancer STRAT4 (CE-IVD) package insert. 301-4981, Rev. C March 2020.
- Wirtz, R.M.; Sihto, H.; Isola, J.; Heikkilä, P.; Kellokumpu-Lehtinen, P.L.; Auvinen, P.; Turpeenniemi-Hujanen, T.; Jyrkkiö, S.; Lakis, S.; Schlombs, K.; et al. Biological subtyping of early breast cancer: A study comparing RT-qPCR with immunohistochemistry. Breast Cancer Res. Treat. 2016, 157, 437–446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harris, L.; Fritsche, H.; Mennel, R.; Norton, L.; Ravdin, P.; Taube, S.; Somerfield, M.R.; Hayes, D.F.; Bast, R.C., Jr. American Society of Clinical Oncology 2007 update of recommendations for the use of tumor markers in breast cancer. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2007, 25, 5287–5312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirchner, M.; Glade, J.; Lehmann, U.; Merkelbach-Bruse, S.; Hummel, M.; Lehmann, A.; Trautmann, M.; Kumbrink, J.; Jung, A.; Dietmaier, W.; et al. NTRK testing: First results of the QuiP-EQA scheme and a comprehensive map of NTRK fusion variants and their diagnostic coverage by targeted RNA-based NGS assays. Genes Chromosomes Cancer 2020, 59, 445–453. [Google Scholar] [CrossRef]
- Jöhrens, K.; von Wasielewski, R.; Kreipe, H.H.; Forberger, A.; Jurmeister, P.; Dietel, M.; Stenzinger, A.; Fischer, J. Quality assurance in diagnostic in situ hybridization-experience of QuIP. Pathologe 2020, 41, 614–620. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Sample Information | ER IHC | PgR IHC | HER2 IHC/CISH | Ki-67 IHC | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| EQA Sample ID | Subtype by IHC | ER IHC Status | ER IHC Percentage | ER IHC IRS | PgR IHC Status | PgR IHC Percentage | PgR IHC IRS | HER2 IHC/CISH Status | HER2 Dako Score (IHC) | HER2 CISH | Ki-67 IHC Status | Ki-67 IHC Percentage (%) |
| 1 | TNBC | negative | 0 | 0 | negative | 0 | 0 | negative | 1 | n.p. | positive | 30 |
| 2 | HER2+ | negative | 0 | 0 | positive (low) | <10 | 3 | positive | 3 | n.p. | positive | 30 |
| 3 | HR+, Ki-67 low | positive | 95 | 12 | positive (low) | <10 | 1 | negative | 1 | n.p. | negative | 5 |
| 4 | HR+, Ki-67 low | positive | 90 | 12 | positive | 90 | 12 | negative | 1 | n.p. | negative | 15 |
| 5 | HR+, Ki-67 high | positive | 95 | 12 | positive (low) | <10 | 3 | negative | 0 | n.p. | positive | 50 |
| 6 | TNBC | negative | 0 | 0 | negative | 0 | 0 | negative | 1 | n.p. | positive | 80 |
| 7 | HER2+ | negative | 0 | 0 | negative | 0 | 0 | positive | 3 | n.p. | positive | 50 |
| 8 | HR+, Ki-67 low | positive | 80 | 12 | positive | 70 | 6 | negative | 0 | n.p. | negative | 15 |
| 9 | HR+, Ki-67 high | positive | 95 | 12 | positive | 60 | 9 | negative | 2 | Negative (HER2/ CEN17 ratio = 0.87) | positive | 30 |
| 10 | HR+, Ki-67 high | positive | 95 | 12 | positive | 100 | 12 | negative | 1 | n.p. | positive | 30 |
| Performance Index | ER | PgR | HER2 | Ki-67 |
|---|---|---|---|---|
| Sensitivity | 1 (1–1) | 0.94 (0.87–1) | 1 (1–1) | 0.86 (0.76–0.95) |
| Specificity | 1 (1–1) | 1 (1–1) | 1 (1–1) | 1 (1–1) |
| Precision (PPV) | 1 (1–1) | 1 (1–1) | 1 (1–1) | 1 (1–1) |
| Accuracy | 1 (1–1) | 0.96 (0.91–1) | 1 (1–1) | 0.9 (0.83–0.97) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Erber, R.; Hartmann, A.; Fasching, P.A.; Ruebner, M.; Stöhr, R.; Beckmann, M.W.; Zentgraf, M.; Popp, V.; Weidler, J.; Simon, I.; et al. Reproducibility of mRNA-Based Testing of ESR1, PGR, ERBB2, and MKI67 Expression in Invasive Breast Cancer—A Europe-Wide External Quality Assessment. Cancers 2021, 13, 4718. https://doi.org/10.3390/cancers13184718
Erber R, Hartmann A, Fasching PA, Ruebner M, Stöhr R, Beckmann MW, Zentgraf M, Popp V, Weidler J, Simon I, et al. Reproducibility of mRNA-Based Testing of ESR1, PGR, ERBB2, and MKI67 Expression in Invasive Breast Cancer—A Europe-Wide External Quality Assessment. Cancers. 2021; 13(18):4718. https://doi.org/10.3390/cancers13184718
Chicago/Turabian StyleErber, Ramona, Arndt Hartmann, Peter Andreas Fasching, Matthias Ruebner, Robert Stöhr, Matthias Wilhelm Beckmann, Miriam Zentgraf, Verena Popp, Jodi Weidler, Iris Simon, and et al. 2021. "Reproducibility of mRNA-Based Testing of ESR1, PGR, ERBB2, and MKI67 Expression in Invasive Breast Cancer—A Europe-Wide External Quality Assessment" Cancers 13, no. 18: 4718. https://doi.org/10.3390/cancers13184718