
Statin Use and Long-Term Mortality after Rectal Cancer Surgery

 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Study Setting
2.2. Statin Therapy
2.3. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef]
- Howlader, N.; Noone, A.M.; Krapcho, M.; Miller, D.; Brest, A.; Yu, M.; Ruhl, J.; Tatalovich, Z.; Mariotto, A.; Lewis, D.R.; et al. SEER Cancer Statistics Review 1975–2017; Howlader, N., Noone, A.M., Krapcho, M., Miller, D., Brest, A., Yu, M., Ruhl, J., Tatalovich, Z., Mariotto, A., Lewis, D.R., et al., Eds.; National Cancer Institute: Bethesda, MD, USA, 2020. Available online: https://seer.cancer.gov/csr/1975_2017/ (accessed on 14 May 2021).
- Sido, B.; Teklote, J.-R.; Hartel, M.; Friess, H.; Büchler, M.W. Inflammatory response after abdominal surgery. Best Pract. Res. Clin. Anaesthesiol. 2004, 18, 439–454. [Google Scholar] [CrossRef]
- Dekker, J.W.T.; Gooiker, G.A.; Bastiaannet, E.; van den Broek, C.B.M.; van der Geest, L.G.M.; van de Velde, C.J.; Tollenaar, R.A.E.M.; Liefers, G.J. Cause of death the first year after curative colorectal cancer surgery; a prolonged impact of the surgery in elderly colorectal cancer patients. Eur. J. Surg. Oncol. 2014, 40, 1481–1487. [Google Scholar] [CrossRef]
- Smit, L.C.; Bruins, M.J.; Patijn, G.A.; Ruijs, G.J.H.M. Infectious Complications after Major Abdominal Cancer Surgery: In Search of Improvable Risk Factors. Surg. Infect. 2016, 17, 683–693. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smilowitz, N.R.; Berger, J.S. Perioperative Cardiovascular Risk Assessment and Management for Noncardiac Surgery: A Review. JAMA 2020, 324, 279–290. [Google Scholar] [CrossRef] [PubMed]
- Ferreyra, G.; Long, Y.; Ranieri, V.M. Respiratory complications after major surgery. Curr. Opin. Crit. Care 2009, 15, 342–348. [Google Scholar] [CrossRef]
- Skrlin, S.; Hou, V. A Review of Perioperative Statin Therapy for Noncardiac Surgery. Semin. Cardiothorac. Vasc. Anesth. 2010, 14, 283–290. [Google Scholar] [CrossRef]
- Laufs, U.; Liao, J.K. Isoprenoid metabolism and the pleiotropic effects of statins. Curr. Atheroscler. Rep. 2003, 5, 372–378. [Google Scholar] [CrossRef] [Green Version]
- Demierre, M.-F.; Higgins, P.D.R.; Gruber, S.B.; Hawk, E.; Lippman, S.M. Statins and cancer prevention. Nat. Rev. Cancer 2005, 5, 930–942. [Google Scholar] [CrossRef]
- Disbrow, D.; Seelbach, C.L.; Albright, J.; Ferraro, J.; Wu, J.; Hain, J.M.; Shanker, B.-A.; Cleary, R.K. Statin medications are associated with decreased risk of sepsis and anastomotic leaks after rectal resections. Am. J. Surg. 2018, 216, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Singh, P.P.; Srinivasa, S.; Bambarawana, S.; Lemanu, D.P.; Kahokehr, A.A.; Zargar-Shoshtari, K.; Hill, A.G. Perioperative use of statins in elective colectomy. Dis. Colon Rectum 2012, 55, 205–210. [Google Scholar] [CrossRef]
- Battersby, C.L.F.; Green, P.; Vyapury, V.; Rooney, P.; Hunt, J. PTU-227 Statins may modify colorectal anastomotic leak risk in high risk patients. Gut 2015, 64, A162–A163. [Google Scholar] [CrossRef]
- Bisgård, A.S.; Noack, M.W.; Klein, M.; Rosenberg, J.; Gögenur, I. Perioperative Statin Therapy Is Not Associated With Reduced Risk of Anastomotic Leakage After Colorectal Resection. Dis. Colon Rectum 2013, 56, 980–986. [Google Scholar] [CrossRef]
- Fransgaard, T.; Thygesen, L.C.; Gögenur, I. Statin use is not associated with improved 30-day survival in patients undergoing surgery for colorectal cancer. Int. J. Colorectal Dis. 2018, 33, 199–207. [Google Scholar] [CrossRef]
- Singh, P.P.; Lemanu, D.P.; Soop, M.; Bissett, I.P.; Harrison, J.; Hill, A.G. Perioperative Simvastatin Therapy in Major Colorectal Surgery: A Prospective, Double-Blind Randomized Controlled Trial. J. Am. Coll. Surg. 2016, 223, 308–320.e1. [Google Scholar] [CrossRef] [PubMed]
- Pourlotfi, A.; Ahl, R.; Bass, G.A.; Sjolin, G.; Cao, Y.; Matthiessen, P.; Mohseni, S. Statin therapy is associated with decreased 90-day post-operative mortality after colon cancer surgery. Dis. Colon Rectum. (Forthcoming, Accepted Dec 2020). [CrossRef]
- Pourlotfi, A.; Ahl, R.; Sjolin, G.; Forssten, M.P.; Bass, G.A.; Cao, Y.; Matthiessen, P.; Mohseni, S. Statin therapy and postoperative short-term mortality after rectal cancer surgery. Colorectal. Dis. 2021, 23, 875–881. [Google Scholar] [CrossRef]
- Shao, Y.-Y.; Hsu, C.-H.; Yeh, K.-H.; Chen, H.-M.; Yeh, Y.-C.; Lai, C.-L.; Lin, Z.-Z.; Cheng, A.-L.; Lai, M.-S. Statin Use Is Associated with Improved Prognosis of Colorectal Cancer in Taiwan. Clin. Colorectal Cancer 2015, 14, 177–184.e4. [Google Scholar] [CrossRef] [PubMed]
- Swedish Colorectal Cancer Registry (SCRCR). Nationella Kvalitetsregister. Available online: https://kvalitetsregister.se/englishpages/findaregistry/registerarkivenglish/swedishcolorectalcancerregistryscrcr.2156.html (accessed on 22 February 2021).
- Swedish Colorectal Cancer Registry (SCRCR). National Quality Registry for Rectal Cancer (2007–2016). Available online: https://statistik.incanet.se/kolorektal/rektum/ (accessed on 4 May 2021).
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Swedish National Board of Health and Welfare. (2007–2016). Statin Prescription: Residents 55–84 Years of Age. National Prescribed Drug Register. Available online: https://sdb.socialstyrelsen.se/if_lak/val.aspx (accessed on 21 July 2020).
- Li, Y.; He, X.; Ding, Y.; Chen, H.; Sun, L. Statin uses and mortality in colorectal cancer patients: An updated systematic review and meta-analysis. Cancer Med. 2019, 8, 3305–3313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Konishi, T.; Watanabe, T.; Kishimoto, J.; Nagawa, H. Elective Colon and Rectal Surgery Differ in Risk Factors for Wound Infection. Ann. Surg. 2006, 244, 758–763. [Google Scholar] [CrossRef] [PubMed]
- Kotti, A.; Holmqvist, A.; Albertsson, M.; Sun, X.-F. Survival benefit of statins in older patients with rectal cancer: A Swedish population-based cohort study. J. Geriatr. Oncol. 2019, 10, 690–697. [Google Scholar] [CrossRef] [PubMed]
- Katz, M.S.; Minsky, B.D.; Saltz, L.B.; Riedel, E.; Chessin, D.B.; Guillem, J.G. Association of statin use with a pathologic complete response to neoadjuvant chemoradiation for rectal cancer. Int. J. Radiat. Oncol. Biol. Phys. 2005, 62, 1363–1370. [Google Scholar] [CrossRef]
- Mace, A.G.; Gantt, G.A.; Skacel, M.; Pai, R.; Hammel, J.P.; Kalady, M.F. Statin therapy is associated with improved pathologic response to neoadjuvant chemoradiation in rectal cancer. Dis. Colon Rectum 2013, 56, 1217–1227. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, D.; Raissouni, S.; Price Hiller, J.; Mercer, J.; Powell, E.; MacLean, A.; Jiang, M.; Doll, C.; Goodwin, R.; Batuyong, E.; et al. Predictors of Pathologic Complete Response After Neoadjuvant Treatment for Rectal Cancer: A Multicenter Study. Clin. Colorectal Cancer 2015, 14, 291–295. [Google Scholar] [CrossRef] [PubMed]
- Jameson, M.B.; Gormly, K.; Espinoza, D.; Hague, W.; Asghari, G.; Jeffery, G.M.; Price, T.J.; Karapetis, C.S.; Arendse, M.; Armstrong, J.; et al. SPAR-a randomised, placebo-controlled phase II trial of simvastatin in addition to standard chemotherapy and radiation in preoperative treatment for rectal cancer: An AGITG clinical trial. BMC Cancer 2019, 19, 1229. [Google Scholar] [CrossRef]
- Botto, F.; Alonso-Coello, P.; Chan, M.T.V.; Villar, J.C.; Xavier, D.; Srinathan, S.; Guyatt, G.; Cruz, P.; Graham, M.; Wang, C.Y.; et al. Myocardial injury after noncardiac surgery: A large, international, prospective cohort study establishing diagnostic criteria, characteristics, predictors, and 30-day outcomes. Anesthesiology 2014, 120, 564–578. [Google Scholar] [CrossRef]
- Baker, E.A.; El-Gaddal, S.; Williams, L.; Leaper, D.J. Profiles of inflammatory cytokines following colorectal surgery: Relationship with wound healing and outcome. Wound Repair Regen. 2006, 14, 566–572. [Google Scholar] [CrossRef]
- Dimopoulou, I.; Armaganidis, A.; Douka, E.; Mavrou, I.; Augustatou, C.; Kopterides, P.; Lyberopoulos, P.; Tzanela, M.; Orfanos, S.E.; Pelekanou, E.; et al. Tumour necrosis factor-alpha (TNFα) and interleukin-10 are crucial mediators in post-operative systemic inflammatory response and determine the occurrence of complications after major abdominal surgery. Cytokine 2007, 37, 55–61. [Google Scholar] [CrossRef]
- Scott, F.I.; Vajravelu, R.K.; Mamtani, R.; Bianchina, N.; Mahmoud, N.; Hou, J.K.; Wu, Q.; Wang, X.; Haynes, K.; Lewis, J.D. Association Between Statin Use at the Time of Intra-abdominal Surgery and Postoperative Adhesion-Related Complications and Small-Bowel Obstruction. JAMA Netw. Open 2021, 4, e2036315. [Google Scholar] [CrossRef]
- Lochhead, P.; Chan, A.T. Statins and colorectal cancer. Clin. Gastroenterol. Hepatol. 2013, 11, 109-e14. [Google Scholar] [CrossRef] [Green Version]
- Ogino, S.; Chan, A.T.; Fuchs, C.S.; Giovannucci, E. Molecular pathological epidemiology of colorectal neoplasia: An emerging transdisciplinary and interdisciplinary field. Gut 2011, 60, 397–411. [Google Scholar] [CrossRef] [PubMed]
- Ng, K.; Ogino, S.; Meyerhardt, J.A.; Chan, J.A.; Chan, A.T.; Niedzwiecki, D.; Hollis, D.; Saltz, L.B.; Mayer, R.J.; Benson, A.B.; et al. Relationship Between Statin Use and Colon Cancer Recurrence and Survival: Results from CALGB 89803. J. Natl. Cancer Inst. 2011, 103, 1540–1551. [Google Scholar] [CrossRef] [PubMed]
- Lash, T.L.; Riis, A.H.; Ostenfeld, E.B.; Erichsen, R.; Vyberg, M.; Ahern, T.P.; Thorlacius-Ussing, O. Associations of Statin Use with Colorectal Cancer Recurrence and Mortality in a Danish Cohort. Am. J. Epidemiol. 2017, 186, 679–687. [Google Scholar] [CrossRef] [PubMed]
- Alves, A.; Panis, Y.; Mathieu, P.; Mantion, G.; Kwiatkowski, F.; Slim, K. Postoperative Mortality and Morbidity in French Patients Undergoing Colorectal Surgery: Results of a Prospective Multicenter Study. Arch. Surg. 2005, 140, 278–283. [Google Scholar] [CrossRef] [Green Version]
- Arnaboldi, L.; Corsini, A. Do structural differences in statins correlate with clinical efficacy? Curr. Opin. Lipidol. 2010, 21, 298–304. [Google Scholar] [CrossRef] [PubMed]



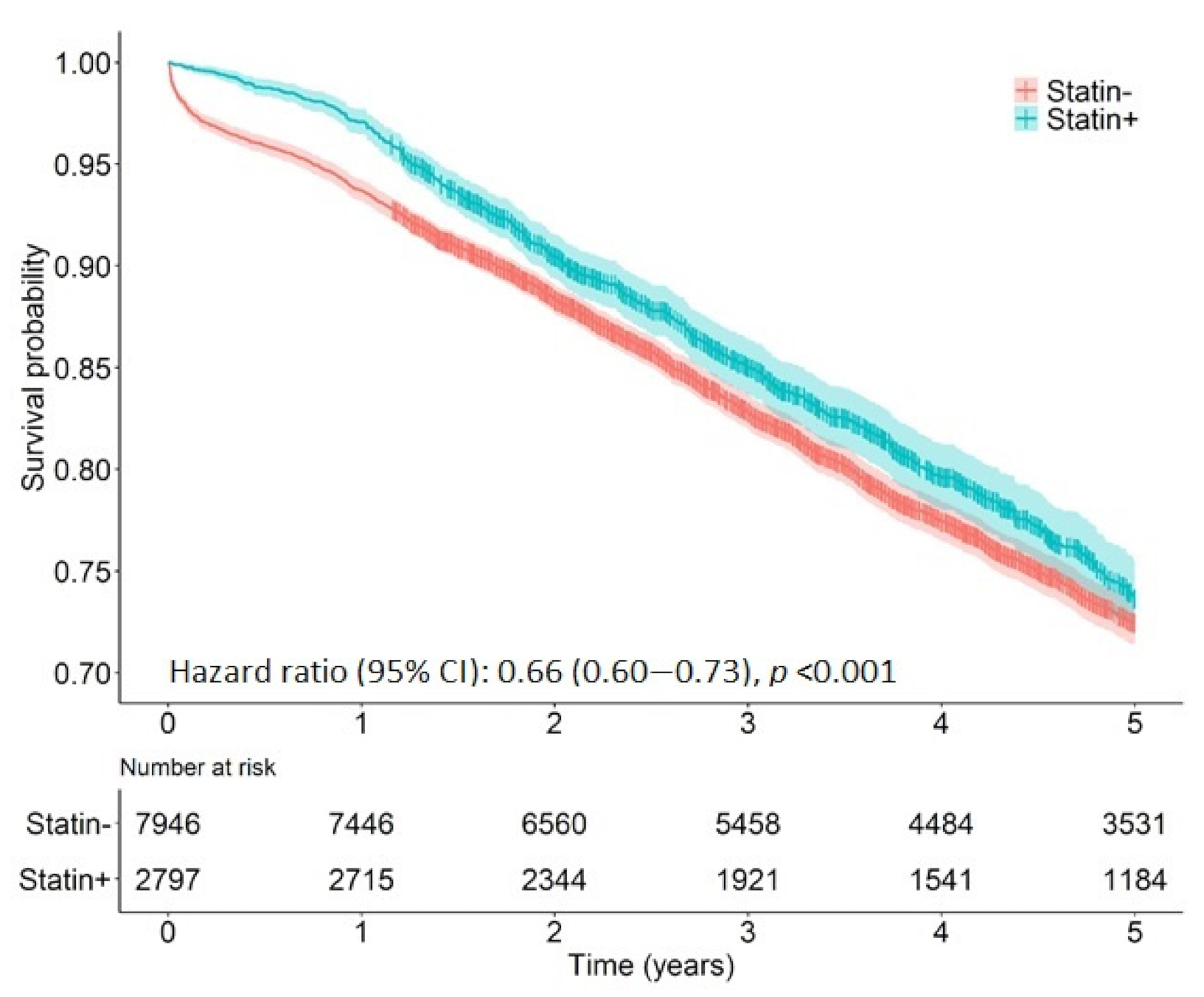{kind=link}
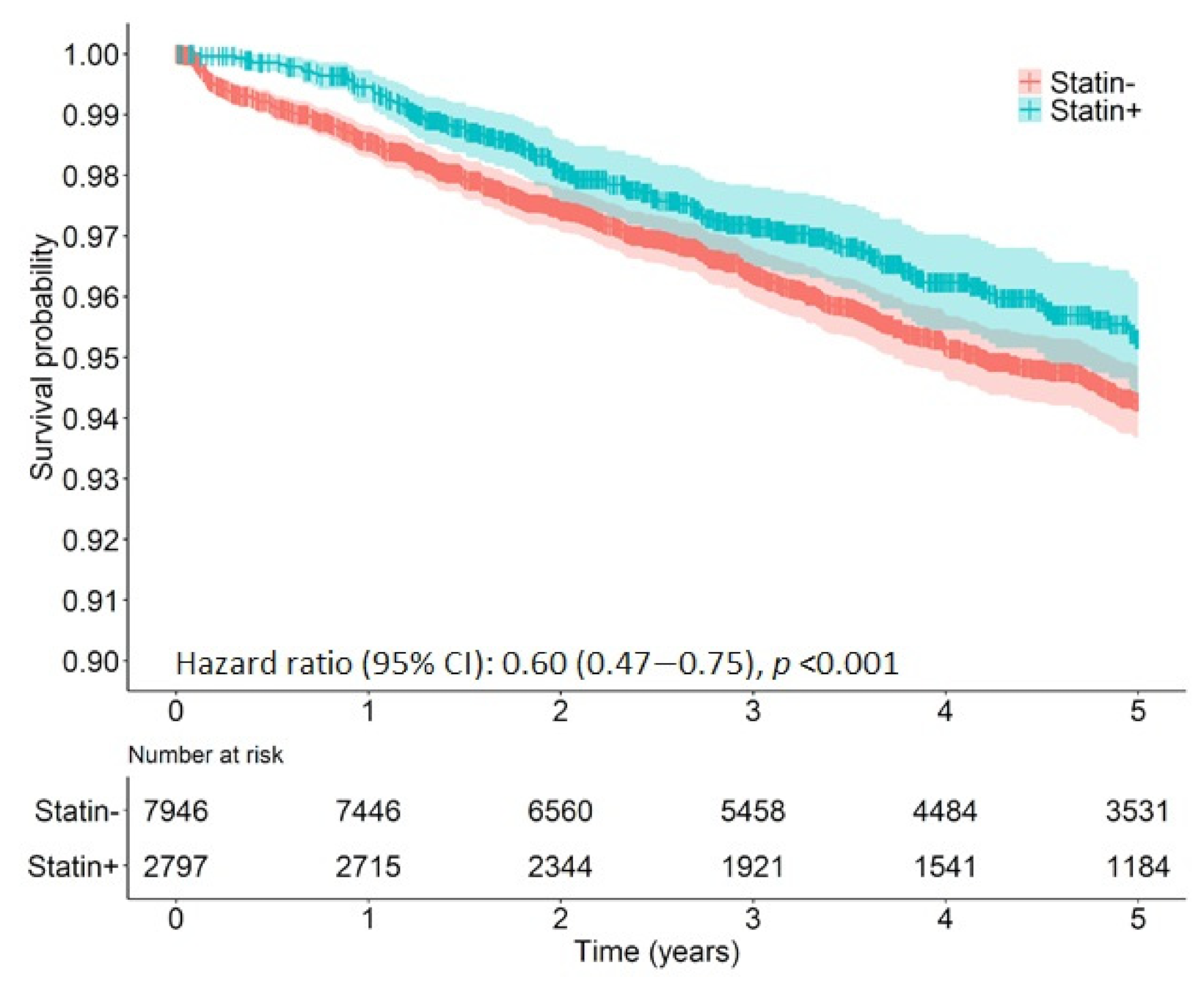{kind=link}
| Variable | Statin− (N = 7946) | Statin+ (N = 2797) | p-Value |
|---|---|---|---|
| Age, mean (±SD) | 67.7 (±11.7) | 71.2 (±8.2) | <0.001 |
| Sex, n (%) | <0.001 | ||
| Male | 4549 (57.2) | 1921 (68.7) | |
| Female | 3397 (42.8) | 876 (31.3) | |
| ASA classification, n (%) | <0.001 | ||
| 1 | 2113 (26.6) | 139 (5.0) | |
| 2 | 4351 (54.8) | 1580 (56.5) | |
| 3 | 1303 (16.4) | 993 (35.5) | |
| 4 | 58 (0.7) | 53 (1.9) | |
| Missing | 121 (1.5) | 32 (1.1) | |
| Cancer stage, n (%) | 0.002 | ||
| I | 2300 (28.9) | 907 (32.4) | |
| II | 2546 (32.0) | 875 (31.3) | |
| III | 3100 (39.0) | 1015 (36.3) | |
| Neoadjuvant therapy, n (%) | 1092 (13.7) | 232 (8.3) | <0.001 |
| Missing | 2873 (36.2) | 1113 (39.8) | |
| Adjuvant therapy, n (%) | 1644 (20.7) | 452 (16.2) | <0.001 |
| Surgical technique, n (%) | 0.099 | ||
| Open surgery | 6682 (84.1) | 2314 (82.7) | |
| Laparoscopic surgery | 1264 (15.9) | 483 (17.3) | |
| Type of surgery, n (%) | 0.040 | ||
| Anterior resection | 4175 (52.5) | 1435 (51.3) | |
| Abdominoperineal excision | 2900 (36.5) | 1006 (36.0) | |
| Hartmann’s operation | 871 (11.0) | 356 (12.7) |
| Variable | Statin− (N = 7946) | Statin+ (N = 2797) | p-Value |
|---|---|---|---|
| Arrhythmia, n (%) | 644 (8.1) | 401 (14.3) | <0.001 |
| Hypertension, n (%) | 1469 (18.5) | 1261 (45.1) | <0.001 |
| Myocardial infarction, n (%) | 136 (1.7) | 443 (15.8) | <0.001 |
| Congestive heart failure, n (%) | 240 (3.0) | 198 (7.1) | <0.001 |
| Peripheral vascular disease, n (%) | 132 (1.7) | 186 (6.6) | <0.001 |
| Cerebrovascular disease, n (%) | 274 (3.4) | 342 (12.2) | <0.001 |
| Dementia, n (%) | 85 (1.1) | 29 (1.0) | 0.969 |
| COPD, n (%) | 337 (4.2) | 181 (6.5) | <0.001 |
| Connective tissue disease, n (%) | 131 (1.6) | 62 (2.2) | 0.063 |
| Peptic ulcer disease, n (%) | 122 (1.5) | 60 (2.1) | 0.039 |
| Liver disease, n (%) | 56 (0.7) | 14 (0.5) | 0.309 |
| Diabetes, n (%) | 394 (5.0) | 661 (23.6) | <0.001 |
| Hemiplegia, n (%) | 36 (0.5) | 36 (1.3) | <0.001 |
| Chronic kidney disease, n (%) | 83 (1.0) | 70 (2.5) | <0.001 |
| Charlson comorbidity index, n (%) | <0.001 | ||
| ≤4 | 3785 (47.6) | 646 (23.1) | |
| 5–6 | 3251 (40.9) | 1447 (51.7) | |
| ≥7 | 910 (11.5) | 704 (25.2) |
| Variable | Statin− (N = 7946) | Statin+ (N = 2797) | p-Value |
|---|---|---|---|
| Length of stay (days), median [IQR] | 9.0 [7.0–14] | 10 [7.0–15] | 0.002 |
| Missing, n (%) | 67 (0.8) | 25 (0.9) | |
| 1-year mortality, n (%) | |||
| All-cause | 500 (6.3) | 82 (2.9) | <0.001 |
| Cancer-specific | 111 (1.4) | 15 (0.5) | <0.001 |
| Statin− (N = 7474) | Statin+ (N = 2606) | ||
| 2-year mortality, n (%) | |||
| All-cause | 917 (12.3) | 262 (10.1) | 0.003 |
| Cancer-specific | 194 (2.6) | 51 (2.0) | 0.080 |
| Statin− (N = 6756) | Statin+ (N = 2315) | ||
| 3-year mortality, n (%) | |||
| All-cause | 1304 (19.3) | 394 (17.0) | 0.016 |
| Cancer-specific | 259 (3.8) | 71 (3.1) | 0.102 |
| Statin− (N = 6119) | Statin+ (N = 2048) | ||
| 4-year mortality, n (%) | |||
| All-cause | 1635 (26.7) | 507 (24.8) | 0.085 |
| Cancer-specific | 319 (5.2) | 87 (4.2) | 0.093 |
| Statin− (N = 5430) | Statin+ (N = 1796) | ||
| 5-year mortality, n (%) | |||
| All-cause | 1899 (35.0) | 612 (34.1) | 0.507 |
| Cancer-specific | 357 (6.6) | 100 (5.6) | 0.143 |
| Variable | All-Cause Mortality | Cancer-Specific Mortality | ||
|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| Statin therapy | ||||
| No | ref. | ref. | ||
| Yes | 0.66 (0.60–0.73) | <0.001 | 0.60 (0.47–0.75) | <0.001 |
| Age | 1.03 (1.02–1.04) | <0.001 | 1.04 (1.02–1.05) | <0.001 |
| Sex | ||||
| Male | ref. | ref. | ||
| Female | 0.81 (0.74–0.88) | <0.001 | 1.05 (0.87–1.26) | 0.633 |
| ASA classification | ||||
| 1 | ref. | ref. | ||
| 2 | 1.29 (1.12–1.47) | <0.001 | 1.28 (0.93–1.76) | 0.136 |
| 3 | 2.07 (1.78–2.41) | <0.001 | 2.38 (1.67–3.38) | <0.001 |
| 4 | 3.01 (2.23–4.05) | <0.001 | 3.33 (1.64–6.76) | <0.001 |
| Charlson Comorbidity Index | ||||
| ≤4 | ref. | ref. | ||
| 5–6 | 1.37 (1.20–1.57) | <0.001 | 1.48 (1.07–2.04) | 0.018 |
| ≥7 | 2.04 (1.74–2.40) | <0.001 | 2.06 (1.40–3.02) | <0.001 |
| Cancer stage | ||||
| I | ref. | ref. | ||
| II | 1.42 (1.26–1.59) | <0.001 | 1.52 (1.16–2.00) | 0.003 |
| III | 2.47 (2.21–2.75) | <0.001 | 2.51 (1.93–3.26) | <0.001 |
| Neoadjuvant therapy | ||||
| No | ref. | ref. | ||
| Yes | 1.36 (1.16–1.60) | <0.001 | 1.77 (1.31–2.39) | <0.001 |
| Adjuvant therapy | ||||
| No | ref. | ref. | ||
| Yes | 0.93 (0.82–1.05) | 0.221 | 0.93 (0.70–1.25) | 0.646 |
| Surgical technique | ||||
| Open surgery | ref. | ref. | ||
| Laparoscopic surgery | 0.91 (0.79–1.04) | 0.157 | 0.93 (0.67–1.28) | 0.651 |
| Type of surgery | ||||
| Anterior resection | ref. | ref. | ||
| Abdominoperineal excision | 1.53 (1.40–1.68) | <0.001 | 1.72 (1.39–2.14) | <0.001 |
| Hartmann’s operation | 1.77 (1.58–1.98) | <0.001 | 1.84 (1.40–2.42) | <0.001 |
| Surgery year | ||||
| 2007 | ref. | ref. | ||
| 2008 | 0.90 (0.77–1.05) | 0.170 | 0.85 (0.60–1.20) | 0.349 |
| 2009 | 0.90 (0.77–1.04) | 0.158 | 0.87 (0.62–1.22) | 0.420 |
| 2010 | 0.78 (0.67–0.92) | 0.003 | 0.66 (0.46–0.96) | 0.029 |
| 2011 | 0.80 (0.68–0.94) | 0.006 | 0.85 (0.60–1.20) | 0.347 |
| 2012 | 0.67 (0.57–0.79) | <0.001 | 0.53 (0.36–0.77) | 0.001 |
| 2013 | 0.68 (0.57–0.81) | <0.001 | 0.52 (0.34–0.78) | 0.002 |
| 2014 | 0.67 (0.56–0.81) | <0.001 | 0.49 (0.32–0.77) | 0.002 |
| 2015 | 0.68 (0.55–0.83) | <0.001 | 0.35 (0.20–0.61) | <0.001 |
| 2016 | 0.62 (0.44–0.87) | 0.005 | 0.36 (0.15–0.84) | 0.019 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pourlotfi, A.; Bass, G.A.; Ahl Hulme, R.; Forssten, M.P.; Sjolin, G.; Cao, Y.; Matthiessen, P.; Mohseni, S. Statin Use and Long-Term Mortality after Rectal Cancer Surgery. Cancers 2021, 13, 4288. https://doi.org/10.3390/cancers13174288
Pourlotfi A, Bass GA, Ahl Hulme R, Forssten MP, Sjolin G, Cao Y, Matthiessen P, Mohseni S. Statin Use and Long-Term Mortality after Rectal Cancer Surgery. Cancers. 2021; 13(17):4288. https://doi.org/10.3390/cancers13174288
Chicago/Turabian StylePourlotfi, Arvid, Gary Alan Bass, Rebecka Ahl Hulme, Maximilian Peter Forssten, Gabriel Sjolin, Yang Cao, Peter Matthiessen, and Shahin Mohseni. 2021. "Statin Use and Long-Term Mortality after Rectal Cancer Surgery" Cancers 13, no. 17: 4288. https://doi.org/10.3390/cancers13174288