External Validation of a Nomogram to Predict Survival and Benefit of Concurrent Chemoradiation for Stage II Nasopharyngeal Carcinoma

 , , , and
, , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Treatment
2.2. Statistical Analysis
3. Results
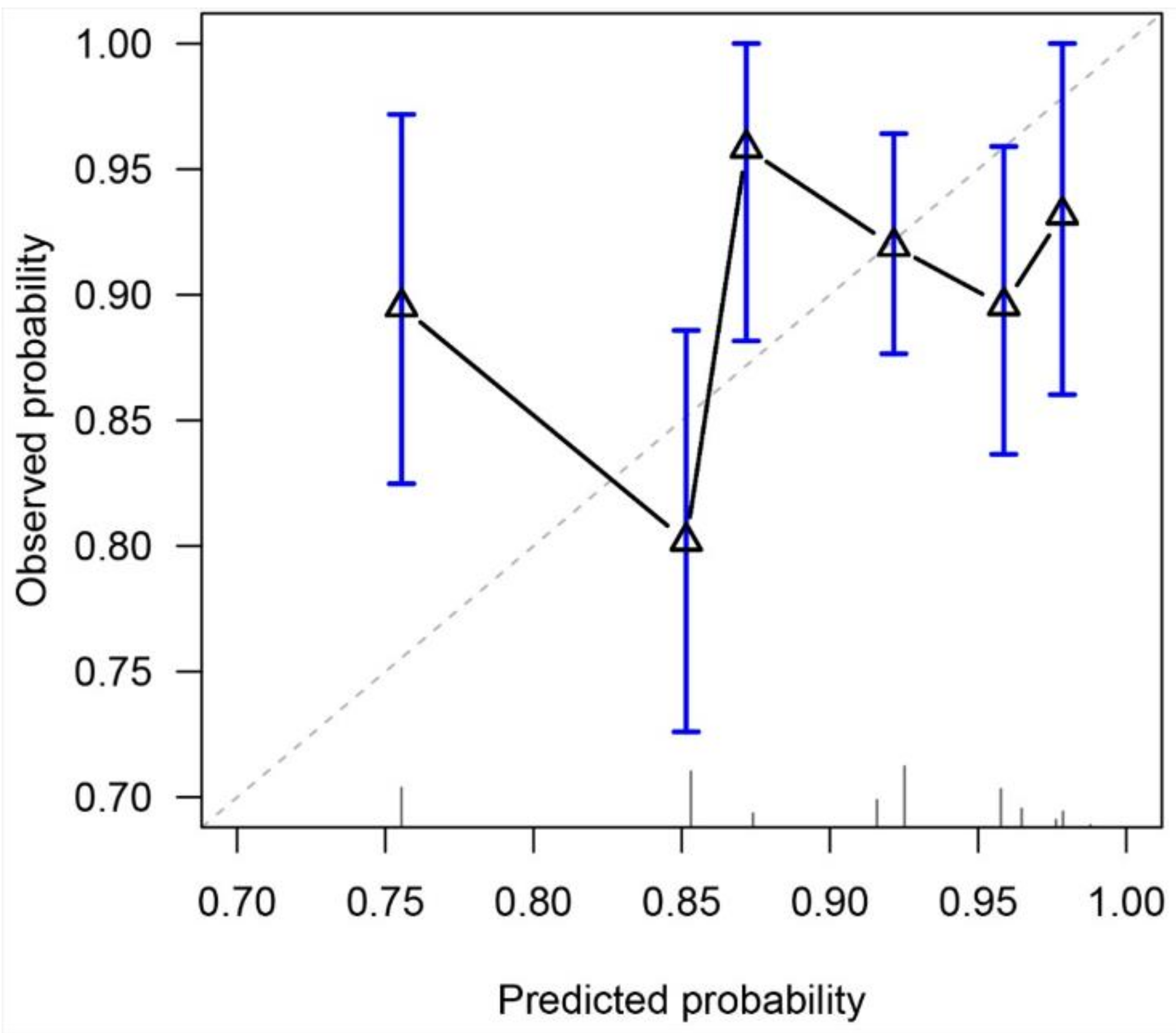
Discrimination and Accuracy
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nasopharynx. Available online: https://gco.iarc.fr/today/data/factsheets/cancers/4-Nasopharynx-fact-sheet.pdf (accessed on 21 February 2021).
- Hong Kong Cancer Registry, H.A. Nasopharyngeal Cancer in 2017. Available online: https://www3.ha.org.hk/cancereg/pdf/factsheet/2017/npc_2017.pdf (accessed on 21 February 2021).
- Hong Kong Cancer Registry, H.A. Nasopharyngeal Cancer in 2018. Available online: https://www3.ha.org.hk/cancereg/pdf/factsheet/2018/npc_2018.pdf (accessed on 21 February 2021).
- Wu, P.; Zhao, Y.; Xiang, L.; Yang, L. Management of Chemotherapy for Stage II Nasopharyngeal Carcinoma in the Intensity-Modulated Radiotherapy Era: A Review. Cancer Manag. Res. 2020, 12, 957–963. [Google Scholar] [CrossRef] [PubMed]
- Lee, V.H.; Lam, K.O.; Chang, A.T.; Lam, T.C.; Chiang, C.L.; So, T.H.; Choi, C.W.; Lee, A.W. Management of Nasopharyngeal Carcinoma: Is Adjuvant Therapy Needed? J. Oncol. Pract. 2018, 14, 594–602. [Google Scholar] [CrossRef] [PubMed]
- Liu, F.; Jin, T.; Liu, L.; Xiang, Z.; Yan, R.; Yang, H. The role of concurrent chemotherapy for stage II nasopharyngeal carcinoma in the intensity-modulated radiotherapy era: A systematic review and meta-analysis. PLoS ONE 2018, 13, e0194733. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Su, Z.; Mao, Y.P.; Tang, J.; Lan, X.W.; OuYang, P.Y.; Xie, F.Y. Long-term outcomes of concurrent chemoradiotherapy versus radiotherapy alone in stage II nasopharyngeal carcinoma treated with IMRT: A retrospective study. Tumour Biol. J. Int. Soc. Oncodevelopmental Biol. Med. 2016, 37, 4429–4438. [Google Scholar] [CrossRef] [PubMed]
- NCCN Clinical Practice Guidelines in Oncology. Head and Neck Cancers. Version 1.2021. Available online: https://www.nccn.org/professionals/physician_gls/pdf/head-and-neck.pdf (accessed on 26 February 2021).
- Chen, Y.-P.; Ismaila, N.; Chua, M.L.K.; Colevas, A.D.; Haddad, R.; Huang, S.H.; Wee, J.T.S.; Whitley, A.C.; Yi, J.-L.; Yom, S.S.; et al. Chemotherapy in Combination With Radiotherapy for Definitive-Intent Treatment of Stage II-IVA Nasopharyngeal Carcinoma: CSCO and ASCO Guideline. J. Clin. Oncol. 2021, 39, 840–859. [Google Scholar] [CrossRef]
- Bossi, P.; Chan, A.T.; Licitra, L.; Trama, A.; Orlandi, E.; Hui, E.P.; Halámková, J.; Mattheis, S.; Baujat, B.; Hardillo, J.; et al. Nasopharyngeal carcinoma: ESMO-EURACAN Clinical Practice Guidelines for diagnosis, treatment and follow-up(†). Ann. Oncol. Off. J. Eur. Soc. Med Oncol. 2020, 32, 452–465. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Miao, J.; Huang, H.; Chen, B.; Xiao, X.; Zhu, M.; Liang, Y.; Xiao, W.; Huang, S.; Peng, Y.; et al. Long-term Survivals, Toxicities and the Role of Chemotherapy in Early-Stage Nasopharyngeal Carcinoma Patients Treated with Intensity-modulated Radiation Therapy: A Retrospective Study with 15-year Follow-up. Cancer Res. Treat. 2021. [Google Scholar] [CrossRef]
- Chua, D.T.; Sham, J.S.; Kwong, D.L.; Au, G.K. Treatment outcome after radiotherapy alone for patients with Stage I-II nasopharyngeal carcinoma. Cancer 2003, 98, 74–80. [Google Scholar] [CrossRef] [PubMed]
- Cho, B. Intensity-modulated radiation therapy: A review with a physics perspective. Radiat. Oncol. J. 2018, 36, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, X.S.; Li, X.Y.; Xiao, B.B.; Liu, S.L.; Chen, Q.Y.; Tang, L.Q.; Mai, H.Q. Establishment and validation of a nomogram for predicting the benefit of concurrent chemotherapy in stage II nasopharyngeal carcinoma: A study based on a phase III randomized clinical trial with 10-year follow-up. Oral Oncol. 2020, 100, 104490. [Google Scholar] [CrossRef]
- Chen, Q.-Y.; Wen, Y.-F.; Guo, L.; Liu, H.; Huang, P.-Y.; Mo, H.-Y.; Li, N.-W.; Xiang, Y.-Q.; Luo, D.-H.; Qiu, F.; et al. Concurrent Chemoradiotherapy vs Radiotherapy Alone in Stage II Nasopharyngeal Carcinoma: Phase III Randomized Trial. JNCI J. Natl. Cancer Inst. 2011, 103, 1761–1770. [Google Scholar] [CrossRef] [Green Version]
- Au, K.H.; Ngan, R.K.C.; Ng, A.W.Y.; Poon, D.M.C.; Ng, W.T.; Yuen, K.T.; Lee, V.H.F.; Tung, S.Y.; Chan, A.T.C.; Sze, H.C.K.; et al. Treatment outcomes of nasopharyngeal carcinoma in modern era after intensity modulated radiotherapy (IMRT) in Hong Kong: A report of 3328 patients (HKNPCSG 1301 study). Oral Oncol. 2018, 77, 16–21. [Google Scholar] [CrossRef]
- Edge, S.B.; Compton, C.C. The American Joint Committee on Cancer: The 7th Edition of the AJCC Cancer Staging Manual and the Future of TNM. Ann. Surg. Oncol. 2010, 17, 1471–1474. [Google Scholar] [CrossRef] [PubMed]
- Noronha, V.; Joshi, A.; Patil, V.M.; Agarwal, J.; Ghosh-Laskar, S.; Budrukkar, A.; Murthy, V.; Gupta, T.; D’Cruz, A.K.; Banavali, S.; et al. Once-a-Week Versus Once-Every-3-Weeks Cisplatin Chemoradiation for Locally Advanced Head and Neck Cancer: A Phase III Randomized Noninferiority Trial. J. Clin. Oncol. 2017, 36, 1064–1072. [Google Scholar] [CrossRef] [PubMed]
- Kwong, D.L.; Sham, J.S.; Au, G.K.; Chua, D.T.; Kwong, P.W.; Cheng, A.C.; Wu, P.M.; Law, M.W.; Kwok, C.C.; Yau, C.C.; et al. Concurrent and adjuvant chemotherapy for nasopharyngeal carcinoma: A factorial study. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2004, 22, 2643–2653. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.W.M.; Ngan, R.K.C.; Ng, W.T.; Tung, S.Y.; Cheng, A.A.C.; Kwong, D.L.W.; Lu, T.X.; Chan, A.T.C.; Sze, H.C.K.; Yiu, H.H.Y.; et al. NPC-0501 trial on the value of changing chemoradiotherapy sequence, replacing 5-fluorouracil with capecitabine, and altering fractionation for patients with advanced nasopharyngeal carcinoma. Cancer 2020, 126, 3674–3688. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Chen, L.; Hu, G.Q.; Zhang, N.; Zhu, X.D.; Yang, K.Y.; Jin, F.; Shi, M.; Chen, Y.P.; Hu, W.H.; et al. Gemcitabine and Cisplatin Induction Chemotherapy in Nasopharyngeal Carcinoma. N. Engl. J. Med. 2019, 381, 1124–1135. [Google Scholar] [CrossRef]
- Peng, G.; Wang, T.; Yang, K.Y.; Zhang, S.; Zhang, T.; Li, Q.; Han, J.; Wu, G. A prospective, randomized study comparing outcomes and toxicities of intensity-modulated radiotherapy vs. conventional two-dimensional radiotherapy for the treatment of nasopharyngeal carcinoma. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2012, 104, 286–293. [Google Scholar] [CrossRef]
- Zhang, B.; Mo, Z.; Du, W.; Wang, Y.; Liu, L.; Wei, Y. Intensity-modulated radiation therapy versus 2D-RT or 3D-CRT for the treatment of nasopharyngeal carcinoma: A systematic review and meta-analysis. Oral Oncol. 2015, 51, 1041–1046. [Google Scholar] [CrossRef]
- Co, J.; Mejia, M.B.; Dizon, J.M. Evidence on effectiveness of intensity-modulated radiotherapy versus 2-dimensional radiotherapy in the treatment of nasopharyngeal carcinoma: Meta-analysis and a systematic review of the literature. Head Neck 2016, 38 (Suppl. 1), E2130–E2142. [Google Scholar] [CrossRef]
- Luo, S.; Zhao, L.; Wang, J.; Xu, M.; Li, J.; Zhou, B.; Xiao, F.; Long, X.; Shi, M. Clinical outcomes for early-stage nasopharyngeal carcinoma with predominantly WHO II histology treated by intensity-modulated radiation therapy with or without chemotherapy in nonendemic region of China. Head Neck 2014, 36, 841–847. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.; Chen, X.; Zhao, C.; Wang, J.; Wang, K.; Wang, L.; Miao, J.; Cao, C.; Jin, T.; Zhang, Y.; et al. Adding Concurrent Chemotherapy to Intensity-Modulated Radiotherapy Does Not Improve Treatment Outcomes for Stage II Nasopharyngeal Carcinoma: A Phase 2 Multicenter Clinical Trial. Front. Oncol. 2020, 10. [Google Scholar] [CrossRef]
- Zhang, L.N.; Gao, Y.H.; Lan, X.W.; Tang, J.; Su, Z.; Ma, J.; Deng, W.; OuYang, P.Y.; Xie, F.Y. Propensity score matching analysis of cisplatin-based concurrent chemotherapy in low risk nasopharyngeal carcinoma in the intensity-modulated radiotherapy era. Oncotarget 2015, 6, 44019–44029. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, K.-H.; Zhu, X.-D.; Li, L.; Qu, S.; Liang, Z.-Q.; Liang, X.; Pan, X.-B.; Liang, Z.-G.; Jiang, Y.-M. Comparison of the efficacy between concurrent chemoradiotherapy with or without adjuvant chemotherapy and intensity-modulated radiotherapy alone for stage II nasopharyngeal carcinoma. Oncotarget 2016, 7, 69041. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guo, Q.; Lu, T.; Lin, S.; Zong, J.; Chen, Z.; Cui, X.; Zhang, Y.; Pan, J. Long-term survival of nasopharyngeal carcinoma patients with Stage II in intensity-modulated radiation therapy era. Jpn. J. Clin. Oncol. 2016, 46, 241–247. [Google Scholar] [CrossRef] [Green Version]
- Xu, T.; Shen, C.; Zhu, G.; Hu, C. Omission of Chemotherapy in Early Stage Nasopharyngeal Carcinoma Treated with IMRT: A Paired Cohort Study. Medicine 2015, 94, e1457. [Google Scholar] [CrossRef]
- Ding, X.C.; Fan, P.P.; Xie, P.; Fan, B.J.; Yang, J.; Jiang, L.Y.; Bai, X.B.; Yu, J.M.; Hu, M. Ten-Year Outcomes Of Intensity-Modulated Radiotherapy (IMRT) Combine With Chemotherapy Versus IMRT Alone For Stage II Nasopharyngeal Carcinoma In The Real-World Study (RWD). Cancer Manag. Res. 2019, 11, 8893–8903. [Google Scholar] [CrossRef] [Green Version]
- Xu, C.; Zhang, L.H.; Chen, Y.P.; Liu, X.; Zhou, G.Q.; Lin, A.H.; Sun, Y.; Ma, J. Chemoradiotherapy Versus Radiotherapy Alone in Stage II Nasopharyngeal Carcinoma: A Systemic Review and Meta-analysis of 2138 Patients. J. Cancer 2017, 8, 287–297. [Google Scholar] [CrossRef] [Green Version]
- Su, S.F.; Han, F.; Zhao, C.; Chen, C.Y.; Xiao, W.W.; Li, J.X.; Lu, T.X. Long-term outcomes of early-stage nasopharyngeal carcinoma patients treated with intensity-modulated radiotherapy alone. Int. J. Radiat. Oncol. Biol. Phys. 2012, 82, 327–333. [Google Scholar] [CrossRef] [PubMed]
- Yao, J.J.; Zhou, G.Q.; Wang, Y.Q.; Wang, S.Y.; Zhang, W.J.; Jin, Y.N.; Zhang, F.; Li, L.; Liu, L.Z.; Cheng, Z.B.; et al. Prognostic values of the integrated model incorporating the volume of metastatic regional cervical lymph node and pretreatment serum Epstein-Barr virus DNA copy number in predicting distant metastasis in patients with N1 nasopharyngeal carcinoma. Chin. J. Cancer 2017, 36, 98. [Google Scholar] [CrossRef]
- Leung, S.F.; Chan, A.T.; Zee, B.; Ma, B.; Chan, L.Y.; Johnson, P.J.; Lo, Y.M. Pretherapy quantitative measurement of circulating Epstein-Barr virus DNA is predictive of posttherapy distant failure in patients with early-stage nasopharyngeal carcinoma of undifferentiated type. Cancer 2003, 98, 288–291. [Google Scholar] [CrossRef]
- He, S.-S.; Wang, C.-T.; Peng, Z.-W.; Ren, Y.-F.; Lu, L.-X.; Chen, R.-W.; Liang, S.-B.; Wang, Y.; Chen, Y. Development and external validation of a nomogram for predicting the overall survival of patients with stage II nasopharyngeal carcinoma after curative treatment. Cancer Manag. Res. 2019, 11, 4403–4412. [Google Scholar] [CrossRef] [Green Version]
- Chen, Q.Y.; Guo, S.Y.; Tang, L.Q.; Lu, T.Y.; Chen, B.L.; Zhong, Q.Y.; Zou, M.S.; Tang, Q.N.; Chen, W.H.; Guo, S.S.; et al. Combination of Tumor Volume and Epstein-Barr Virus DNA Improved Prognostic Stratification of Stage II Nasopharyngeal Carcinoma in the Intensity Modulated Radiotherapy Era: A Large-Scale Cohort Study. Cancer Res. Treat. 2018, 50, 861–871. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Min, H.; Hong, M.; Ma, J.; Zhang, E.; Zheng, Q.; Zhang, J.; Zhang, J.; Zhang, F.; Su, Y.; Qiu, F. A new staging system for nasopharyngeal carcinoma in China. Int. J. Radiat. Oncol. Biol. Phys. 1994, 30, 1037–1042. [Google Scholar] [PubMed]
- Balachandran, V.P.; Gonen, M.; Smith, J.J.; DeMatteo, R.P. Nomograms in oncology: More than meets the eye. Lancet Oncol. 2015, 16, e173–e180. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total (n = 482) | CCRT (n = 176) | RT Alone (n = 306) | p |
|---|---|---|---|---|
| Age | ||||
| Mean, SD, (range, IQR) | 48, 8 (20–68, 43–53) | 50, 10 (23–70, 44–57) | 0.02 | |
| Age ≤ 45, n (%) | 158 | 63 (35.8%) | 95 (31.1%) | 0.29 |
| Age > 45, n (%) | 324 | 113 (64.2%) | 211 (69.0%) | |
| Sex | ||||
| Male, n (%) | 337 | 128 (72.7%) | 209 (68.3%) | 0.31 |
| Female, n (%) | 145 | 48 (27.3%) | 97 (31.7%) | |
| T category | 0.10 | |||
| T1, n (%) | 210 | 68 (38.6%) | 142 (46.4%) | |
| T2, n (%) | 272 | 108 (61.4%) | 164 (53.6%) | |
| N category | ||||
| N0, n (%) | 89 | 17 (9.7%) | 72 (23.5%) | <0.01 |
| N1, n (%) | 393 | 159 (90.3%) | 234 (76.5%) | |
| TN category | <0.01 | |||
| T2N0, n (%) | 89 | 17 (9.7%) | 72 (23.5%) | |
| T1N1, n (%) | 210 | 68 (38.6%) | 142 (46.4%) | |
| T2N1, n (%) | 183 | 91 (51.7%) | 92 (30.1%) | |
| Concurrent chemotherapy | ||||
| 3-weekly cisplatin, n (%) | 62 (35.2%) | |||
| Weekly cisplatin, n (%) | 108 (61.4%) | |||
| Carboplatin, n (%) | 6 (3.4%) | |||
| Total score by nomogram, mean, SD | 198.5, 58.9 | 143.5, 39.1 | 230.2, 42.9 | <0.01 |
| Follow-up, median, months, IQR | 86, 68–106 | 85, 69–104 | 86, 68–107 | 0.66 |
| OS, event | 28 | 51 | 0.90 | |
| 5-year OS | 90.8% | 88.4% | ||
| 8-year OS | 84.9% | 83.7% |
| Clinical Factors | HR | 95% CI | p |
|---|---|---|---|
| Age | |||
| ≤45 years | reference | ||
| >45 years | 1.97 | 1.13–3.40 | 0.02 |
| Age (continuous by year) | 1.05 | 1.02–1.07 | <0.01 |
| Sex | |||
| Male | reference | ||
| Female | 0.77 | 0.46–1.28 | 0.31 |
| T Category | |||
| T1 | reference | ||
| T2 | 0.73 | 0.47–1.14 | 0.17 |
| N Category | |||
| N0 | reference | ||
| N1 | 1.46 | 0.77–2.75 | 0.25 |
| TN Category | |||
| T2N0 | reference | 0.31 | |
| T1N1 | 1.62 | 0.83–3.15 | 0.16 |
| T2N1 | 1.28 | 0.64–2.56 | 0.50 |
| Treatment Group | |||
| RT alone | reference | ||
| CCRT | 0.97 | 0.61–1.54 | 0.90 |
| Clinical Factors | HR | 95% CI | p |
|---|---|---|---|
| Age | |||
| ≤45 years | reference | ||
| >45 years | 1.98 | 1.15–3.44 | 0.02 |
| T Category | |||
| T1 | reference | ||
| T2 | 0.77 | 0.47–1.25 | 0.29 |
| N Category | |||
| N0 | reference | ||
| N1 | 1.26 | 0.62–2.55 | 0.53 |
| Treatment Group | |||
| RT alone | reference | ||
| CCRT | 0.99 | 0.62–1.58 | 0.96 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yip, P.-L.; Lee, S.-F.; Choi, C.-W.H.; Chan, P.-C.S.; Cheung, K.-W.A.; Chow, C.-H.J.; Cheung, K.-M.; Lai, W.-Y.J.; Lee, H.-F.V.; Lam, K.-O.; et al. External Validation of a Nomogram to Predict Survival and Benefit of Concurrent Chemoradiation for Stage II Nasopharyngeal Carcinoma. Cancers 2021, 13, 4286. https://doi.org/10.3390/cancers13174286
Yip P-L, Lee S-F, Choi C-WH, Chan P-CS, Cheung K-WA, Chow C-HJ, Cheung K-M, Lai W-YJ, Lee H-FV, Lam K-O, et al. External Validation of a Nomogram to Predict Survival and Benefit of Concurrent Chemoradiation for Stage II Nasopharyngeal Carcinoma. Cancers. 2021; 13(17):4286. https://doi.org/10.3390/cancers13174286
Chicago/Turabian StyleYip, Pui-Lam, Shing-Fung Lee, Cheuk-Wai Horace Choi, Po-Chung Sunny Chan, Ka-Wai Alice Cheung, Chung-Hang James Chow, Ka-Man Cheung, Wing-Yu Jessica Lai, Ho-Fun Victor Lee, Ka-On Lam, and et al. 2021. "External Validation of a Nomogram to Predict Survival and Benefit of Concurrent Chemoradiation for Stage II Nasopharyngeal Carcinoma" Cancers 13, no. 17: 4286. https://doi.org/10.3390/cancers13174286