
Different Approaches for Case-Mix Adjustment of Patient-Reported Outcomes to Compare Healthcare Providers—Methodological Results of a Systematic Review


 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Studies and Methodological Decisions of Interest
- Risk of what outcome?
- Over what time frame?
- For what population?
- For what purpose?
2.2. Eligibility Criteria and Information Sources
2.3. Search and Study Selection
2.4. Data Collection Process, Data Items, and Risk of Bias in Individual Studies
2.5. Summary Measures and Synthesis of Results
2.6. Risk of Bias across Studies
3. Results
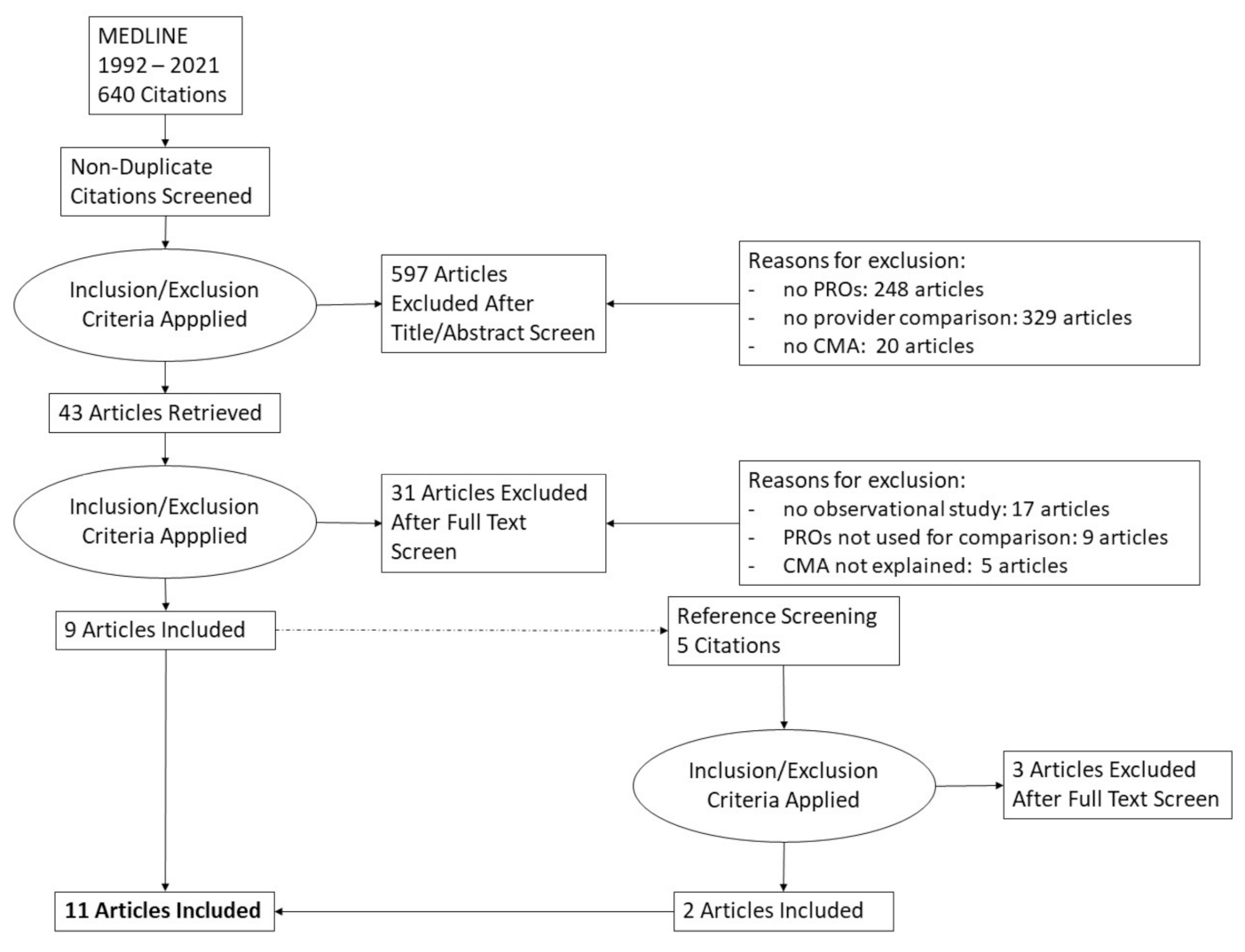
3.1. Study Selection and Characteristics
3.2. Quality of Included Studies (CASP Evaluation)
3.3. Provider Settings
3.4. “Iezzoni’s Four”
3.4.1. Risk of What Outcome?
3.4.2. For What Population?
3.4.3. Over What Time Period?
3.4.4. For What Purpose?
3.5. Selection of Adjustors
3.6. Patient Characteristics Included in the CMA Models
3.7. Provider Characteristics
3.8. Statistical Approaches
3.8.1. Calculation of Transformed Adjusted Scores (Unit/Scale-Preserving Approaches)
3.8.2. Calculation of Transformed Adjusted Scores (Unit/Scale-Aberrant Approaches)
3.8.3. Other
3.8.4. Minimum Case Number Requirements for Statistical Modeling/Adjustment
4. Discussion
Limitations
5. Conclusions and Recommendations
Author Contributions
Funding
Conflicts of Interest
Appendix A. Search String for MEDLine, Including Number of Hits of MEDLine Search
Appendix B

{kind=link}
| Author | Clearly Focused | Recruitement Acceptable | Exposure Accuartely Measured | Outcome Accurately Measured | Identified Confounding | Accounted for Confounding | Subject Follow-Up Complete Enough | Subject Follow-Up Long Enough | Results Precise | Believe Results | Applicable Results | Fit with Other Evidence | Implications for Practice |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Deutscher et al., 2018 [25] | x | can’t tell | x | x | x | x | can’t tell | can’t tell | x | x | x | x | x |
| Farin et al., 2009 [20] | x | x | can’t tell | x | can’t tell | can’t tell | can’t tell | can’t tell | x | x | x | x | x |
| Gozalo et al., [29] | x | can’t tell | x | x | x | x | can’t tell | x | x | x | x | x | x |
| Gutacker et al., 2013 [21] | x | x | x | x | x | x | x | x | x | x | x | x | x |
| Hendryx et al., 1999 [26] | x | x | x | x | can’t tell | x | x | can’t tell | x | x | can’t tell | x | x |
| Khor et al., 2020 [22] | x | x | x | x | x | x | x | x | x | x | x | x | x |
| Lutz et al., 2020 [27] | x | x | x | x | x | x | x | can’t tell | x | x | x | x | x |
| Nuttall et al., 2015 [23] | x | can’t tell | x | x | x | x | can’t tell | x | x | x | x | x | x |
| Resnik & Hart 2003 [28] | x | can’t tell | x | x | x | x | can’t tell | x | x | x | x | x | x |
| Sivaganesan et al., 2018 [24] | x | can’t tell | x | x | x | x | x | x | x | x | x | x | x |
| Varagunam et al., 2015 [30] | x | can’t tell | x | x | x | x | can’t tell | x | x | x | x | x | x |
References
- Klinkhammer-Schalke, M.; Koller, M.; Steinger, B.; Ehret, C.; Ernst, B.; Wyatt, J.C.; Hofstadter, F.; Lorenz, W.; Regensburg Qo, L.S.G. Direct improvement of quality of life using a tailored quality of life diagnosis and therapy pathway: Randomised trial in 200 women with breast cancer. Br. J. Cancer 2012, 106, 826–838. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klinkhammer-Schalke, M.; Steinger, B.; Koller, M.; Zeman, F.; Fürst, A.; Gumpp, J.; Obermaier, R.; Piso, P.; Lindberg-Scharf, P.; Altendorfer, A.; et al. Diagnosing deficits in quality of life and providing tailored therapeutic options: Results of a randomised trial in 220 patients with colorectal cancer. Eur. J. Cancer 2020, 130, 102–113. [Google Scholar] [CrossRef] [PubMed]
- Fromme, E.K.; Eilers, K.M.; Mori, M.; Hsieh, Y.C.; Beer, T.M. How accurate is clinician reporting of chemotherapy adverse effects? A comparison with patient-reported symptoms from the Quality-of-Life Questionnaire C30. J. Clin. Oncol. 2004, 22, 3485–3490. [Google Scholar] [CrossRef] [PubMed]
- Laugsand, E.A.; Sprangers, M.A.; Bjordal, K.; Skorpen, F.; Kaasa, S.; Klepstad, P. Health care providers underestimate symptom intensities of cancer patients: A multicenter European study. Health Qual. Life Outcomes 2010, 8, 104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Basch, E.; Deal, A.M.; Kris, M.G.; Scher, H.I.; Hudis, C.A.; Sabbatini, P.; Rogak, L.; Bennett, A.V.; Dueck, A.C.; Atkinson, T.M.; et al. Symptom Monitoring with Patient-Reported Outcomes during Routine Cancer Treatment: A Randomized Controlled Trial. J. Clin. Oncol. 2015, 34, 557. [Google Scholar] [CrossRef]
- Basch, E.; Deal, A.M.; Dueck, A.C.; Scher, H.I.; Kris, M.G.; Hudis, C.; Schrag, D. Overall Survival Results of a Trial Assessing Patient-Reported Outcomes for Symptom Monitoring During Routine Cancer Treatment. JAMA 2017, 318, 197–198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Denis, F.; Yossi, S.; Septans, A.-L.; Charron, A.; Voog, E.; Dupuis, O.; Ganem, G.; Pointreau, Y.; Letellier, C. Improving survival in patients treated for a lung cancer using self-evaluated symptoms reported through a web application. Am. J. Clin. Oncol. 2017, 40, 464–469. [Google Scholar] [CrossRef]
- Zeegers, M.P.; Bryan, R.T.; Langford, C.; Billingham, L.; Murray, P.; Deshmukh, N.S.; Hussain, S.; James, N.; Wallace, D.M.A.; Cheng, K.K. The West Midlands Bladder Cancer Prognosis Programme: Rationale and design. BJU Int. 2010, 105, 784–788. [Google Scholar] [CrossRef]
- Engelen, V.; Detmar, S.; Koopman, H.; Maurice-Stam, H.; Caron, H.; Hoogerbrugge, P.; Egeler, R.M.; Kaspers, G.; Grootenhuis, M. Reporting health-related quality of life scores to physicians during routine follow-up visits of pediatric oncology patients: Is it effective?: Patient Reported Outcomes in Pediatric Clinic. Pediatr. Blood Cancer 2012, 58, 766–774. [Google Scholar] [CrossRef]
- Trautmann, F.; Hentschel, L.; Hornemann, B.; Rentsch, A.; Baumann, M.; Ehninger, G.; Schmitt, J.; Schuler, M. Electronic real-time assessment of patient-reported outcomes in routine care—First findings and experiences from the implementation in a comprehensive cancer center. Support. Care Cancer 2016, 24, 3047–3056. [Google Scholar] [CrossRef]
- Slovenian National Institute of Public Health. Report on the Basis of the Analysis of Data from the Survey on National Cancer Control. Programmes/Cancer Documents in EU—An IPAAC Report; Ljublja. 2019. Available online: https://www.ipaac.eu/res/file/outputs/wp10/national-cancer-control-plans-survey.pdf (accessed on 2 August 2021).
- ICHOM—International Consortium for Health Outcomes Measurement Localized Prostate Cancer Data Collection Reference Guide. Localized Prostate Cancer Data Collection Reference Guide. 2015. Available online: http://ichom.org/files/medical-conditions/localized-prostate-cancer/localized-prostate-cancer-reference-guide.pdf (accessed on 4 August 2021).
- Evans, S.M.; Millar, J.L.; Moore, C.M.; Lewis, J.D.; Huland, H.; Sampurno, F.; Connor, S.E.; Villanti, P.; Litwin, M.S. Cohort profile: The TrueNTH Global Registry—An international registry to monitor and improve localised prostate cancer health outcomes. BMJ Open 2017, 7, e017006. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kowalski, C.; Roth, R.; Carl, G.; Feick, G.; Oesterle, A.; Hinkel, A.; Steiner, T.; Brock, M.; Kaftan, B.; Borowitz, R.; et al. A multicenter paper-based and web-based system for collecting patient-reported outcome measures in patients undergoing local treatment for prostate cancer: First experiences. J. Patient-Rep. Outcomes 2020, 4, 56. [Google Scholar] [CrossRef] [PubMed]
- Scheibe, M.; Herrmann, A.; Schmitt, J.; Einhart, N.; Sedlmayr, B.; Kowalski, C. Implementation of patient-reported outcome assessment in routine cancer care: A systematic review of multicentric programs in Europe. Z. Für Evidenz Fortbild. Qual. Im Gesundheitswesen 2020, 156–157, 11–23. [Google Scholar] [CrossRef] [PubMed]
- Iezzoni, L. Risk Adjustment for Measuring Healthcare Outcomes, 4th ed.; Health Administration Press: Chicago, IL, USA, 2012. [Google Scholar]
- OECD. Measuring What Matters: The Patient-Reported Indicator Surveys; OECD: Paris, France, 2019. [Google Scholar]
- McGowan, J.; Sampson, M.; Salzwedel, D.M.; Cogo, E.; Foerster, V.; Lefebvre, C. PRESS Peer Review of Electronic Search Strategies: 2015 Guideline Statement. J. Clin. Epidemiol. 2016, 75, 40–46. [Google Scholar] [CrossRef] [Green Version]
- Critical Appraisal Skills Programme CASP Cohort Study Checklist. 2018. Available online: https://casp-uk.net/wp-content/uploads/2018/01/CASP-Cohort-Study-Checklist_2018.pdf (accessed on 18 March 2021).
- Farin, E.; Jäckel, W.H.; Schalaster, V. Projektgruppe QS-Reha-Verfahren in der AQMS The quality assurance programme of the statutory health insurance funds in medical rehabilitation: Results and further developments. Gesundh. Bundesverb. Arzte Offentlichen Gesundh. 2009, 71, 163–174. [Google Scholar] [CrossRef]
- Gutacker, N.; Bojke, C.; Daidone, S.; Devlin, N.; Street, A. Hospital variation in patient-reported outcomes at the level of EQ-5D dimensions: Evidence from England. Med. Decis. Mak. Int. J. Soc. Med. Decis. Mak. 2013, 33, 804–818. [Google Scholar] [CrossRef] [Green Version]
- Khor, S.; Lavallee, D.C.; Cizik, A.M.; Bellabarba, C.; Dagal, A.; Hart, R.A.; Howe, C.R.; Martz, R.D.; Shonnard, N.; Flum, D.R. Hospital and Surgeon Variation in Patient-reported Functional Outcomes After Lumbar Spine Fusion: A Statewide Evaluation. Spine 2020, 45, 465–472. [Google Scholar] [CrossRef]
- Nuttall, D.; Parkin, D.; Devlin, N. Inter-provider comparison of patient-reported outcomes: Developing an adjustment to account for differences in patient case mix. Health Econ. 2015, 24, 41–54. [Google Scholar] [CrossRef]
- Sivaganesan, A.; Asher, A.L.; Bydon, M.; Khan, I.; Kerezoudis, P.; Foley, K.T.; Nian, H.; Harrell, F.E.; Archer, K.R.; Devin, C.J. A Strategy for Risk-adjusted Ranking of Surgeons and Practices Based on Patient-reported Outcomes after Elective Lumbar Surgery. Spine 2019, 44, 670–677. [Google Scholar] [CrossRef]
- Deutscher, D.; Werneke, M.W.; Hayes, D.; Mioduski, J.E.; Cook, K.F.; Fritz, J.M.; Woodhouse, L.J.; Stratford, P.W. Impact of Risk Adjustment on Provider Ranking for Patients With Low Back Pain Receiving Physical Therapy. J. Orthop. Sports Phys. Ther. 2018, 48, 637–648. [Google Scholar] [CrossRef]
- Hendryx, M.S.; Dyck, D.G.; Srebnik, D. Risk-adjusted outcome models for public mental health outpatient programs. Health Serv. Res. 1999, 34, 171–195. [Google Scholar] [PubMed]
- Lutz, A.D.; Brooks, J.M.; Chapman, C.G.; Shanley, E.; Stout, C.E.; Thigpen, C.A. Risk Adjustment of the Modified Low Back Pain Disability Questionnaire and Neck Disability Index to Benchmark Physical Therapist Performance: Analysis From an Outcomes Registry. Phys. Ther. 2020, 100, 609–620. [Google Scholar] [CrossRef]
- Resnik, L.; Hart, D.L. Using clinical outcomes to identify expert physical therapists. Phys. Ther. 2003, 83, 990–1002. [Google Scholar] [CrossRef] [Green Version]
- Gozalo, P.L.; Resnik, L.J.; Silver, B. Benchmarking Outpatient Rehabilitation Clinics Using Functional Status Outcomes. Health Serv. Res. 2016, 51, 768–789. [Google Scholar] [CrossRef] [Green Version]
- Varagunam, M.; Hutchings, A.; Black, N. Do patient-reported outcomes offer a more sensitive method for comparing the outcomes of consultants than mortality? A multilevel analysis of routine data. BMJ Qual. Saf. 2015, 24, 195–202. [Google Scholar] [CrossRef] [PubMed]
- Ware, J.; Kosinski, M.; Keller, S.D. A 12-Item Short-Form Health Survey: Construction of scales and preliminary tests of reliability and validity. Med. Care 1996, 34, 220–233. [Google Scholar] [CrossRef] [Green Version]
- Haley, S.M.; McHorney, C.A.; Ware, J.E. Evaluation of the MOS SF-36 physical functioning scale (PF-10): I. Unidimensionality and reproducibility of the Rasch item scale. J. Clin. Epidemiol. 1994, 47, 671–684. [Google Scholar] [CrossRef]
- McGee, J.; Goldfield, N.; Riley, K.; Morton, J. Collecting Information from Health Care Consumers: A Resource Manual of Tested Questionnaires and Practical Advice; Apsen Publications: Gaithersburg, MD, USA, 1996. [Google Scholar]
- Lehman, A.F.; Postrado, L.T.; Rachuba, L.T. Convergent validation of quality of life assessments for persons with severe mental illnesses. Qual. Life Res. Int. J. Qual. Life Asp. Treat. Care Rehabil. 1993, 2, 327–333. [Google Scholar] [CrossRef] [PubMed]
- Rabin, R.; de Charro, F. EQ-5D: A measure of health status from the EuroQol Group. Ann. Med. 2001, 33, 337–343. [Google Scholar] [CrossRef] [PubMed]
- Bührlen, B.; Gerdes, N.; Jäckel, W.H. Development and psychometric testing of a patient questionnaire for medical rehabilitation (IRES-3). Die Rehabil. 2005, 44, 63–74. [Google Scholar] [CrossRef]
- Chiarotto, A.; Maxwell, L.J.; Ostelo, R.W.; Boers, M.; Tugwell, P.; Terwee, C.B. Measurement Properties of Visual Analogue Scale, Numeric Rating Scale, and Pain Severity Subscale of the Brief Pain Inventory in Patients With Low Back Pain: A Systematic Review. J. Pain 2019, 20, 245–263. [Google Scholar] [CrossRef]
- Murray, D.W.; Fitzpatrick, R.; Rogers, K.; Pandit, H.; Beard, D.J.; Carr, A.J.; Dawson, J. The use of the Oxford hip and knee scores. J. Bone Jt. Surg. Br. 2007, 89, 1010–1014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fritz, J.M.; Irrgang, J.J. A comparison of a modified Oswestry Low Back Pain Disability Questionnaire and the Quebec Back Pain Disability Scale. Phys. Ther. 2001, 81, 776–788. [Google Scholar] [CrossRef] [PubMed]
- Vernon, H.; Mior, S. The Neck Disability Index: A study of reliability and validity. J. Manip. Physiol. Ther. 1991, 14, 409–415. [Google Scholar]
- Fairbank, J.C.; Pynsent, P.B. The Oswestry Disability Index. Spine 2000, 25, 2940–2952. [Google Scholar] [CrossRef]
- Dempster, M.; Donnelly, M.; O′Loughlin, C. The validity of the MacNew Quality of Life in heart disease questionnaire. Health Qual. Life Outcomes 2004, 2, 6. [Google Scholar] [CrossRef] [Green Version]
- Swiontkowski, M.F.; Engelberg, R.; Martin, D.P.; Agel, J. Short musculoskeletal function assessment questionnaire: Validity, reliability, and responsiveness. J. Bone Jt. Surg. Am. 1999, 81, 1245–1260. [Google Scholar] [CrossRef] [PubMed]
- Hart, D.L.; Werneke, M.W.; Wang, Y.-C.; Stratford, P.W.; Mioduski, J.E. Computerized adaptive test for patients with lumbar spine impairments produced valid and responsive measures of function. Spine 2010, 35, 2157–2164. [Google Scholar] [CrossRef]
- Schokkaert, E.; Van de Voorde, C. Direct versus indirect standardization in risk adjustment. J. Health Econ. 2009, 28, 361–374. [Google Scholar] [CrossRef]
- Sibert, N.T.; Dieng, S.; Oesterle, A.; Feick, G.; Carl, G.; Steiner, T.; Minner, J.; Roghmann, F.; Kaftan, B.; Zengerling, F.; et al. Psychometric validation of the German version of the EPIC-26 questionnaire for patients with localized and locally advanced prostate cancer. World J. Urol. 2019, 39, 11–25. [Google Scholar] [CrossRef]
- Skolarus, T.A.; Dunn, R.L.; Sanda, M.G.; Chang, P.; Greenfield, T.K.; Litwin, M.S.; Wei, J.T. Minimally important difference for the Expanded Prostate Cancer Index Composite Short Form. Urology 2015, 85, 101–105. [Google Scholar] [CrossRef] [Green Version]
- Farin, E.; Follert, P.; Gerdes, N.; Jäckel, W.H.; Thalau, J. Quality assessment in rehabilitation centres: The indicator system “Quality Profile”. Disabil. Rehabil. 2004, 26, 1096–1104. [Google Scholar] [CrossRef]
- Roth, R.; Dieng, S.; Oesterle, A.; Feick, G.; Carl, G.; Hinkel, A.; Steiner, T.; Kaftan, B.T.; Kunath, F.; Hadaschik, B.; et al. Determinants of self-reported functional status (EPIC-26) in prostate cancer patients prior to treatment. World J. Urol. 2021, 39, 27–36. [Google Scholar] [CrossRef] [Green Version]
- The Royal College of Surgeons of England. National Prostate Cancer Audit Annual Report 2020. 2021. Available online: https://www.npca.org.uk/content/uploads/2021/01/NPCA-Annual-Report-2020_Final_140121.pdf (accessed on 2 August 2021).
- Neuburger, J.; Cromwell, D.A.; Hutchings, A.; Black, N.; van der Meulen, J.H. Funnel plots for comparing provider performance based on patient-reported outcome measures. BMJ Qual. Saf. 2011, 20, 1020–1026. [Google Scholar] [CrossRef]
- Waljee, J.F.; Ghaferi, A.; Cassidy, R.; Varban, O.; Finks, J.; Chung, K.C.; Carlozzi, N.E.; Dimick, J.B. Are Patient-reported Outcomes Correlated With Clinical Outcomes After Surgery?: A Population-based Study. Ann. Surg. 2016, 264, 682–689. [Google Scholar] [CrossRef] [PubMed]
- Waljee, J.F.; Ghaferi, A.; Finks, J.F.; Cassidy, R.; Varban, O.; Carlin, A.; Carlozzi, N.; Dimick, J. Variation in Patient-reported Outcomes Across Hospitals Following Surgery. Med. Care 2015, 53, 960–966. [Google Scholar] [CrossRef] [PubMed]
- Desai, A.; Bekelis, K.; Ball, P.A.; Lurie, J.; Mirza, S.K.; Tosteson, T.D.; Zhao, W.; Weinstein, J.N. Outcome Variation Across Centers after Surgery for Lumbar Stenosis and Degenerative Spondylolisthesis. Spine 2013, 38, 678–691. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yen, S.-C.; Corkery, M.B.; Chui, K.K.; Manjourides, J.; Wang, Y.-C.; Resnik, L.J. Risk Adjustment for Lumbar Dysfunction: Comparison of Linear Mixed Models With and Without Inclusion of Between-Clinic Variation as a Random Effect. Phys. Ther. 2015, 95, 1692–1702. [Google Scholar] [CrossRef] [Green Version]
- Brundage, M.D.; Smith, K.C.; Little, E.A.; Bantug, E.T.; Snyder, C.F. The PRO Data Presentation Stakeholder Advisory Board Communicating patient-reported outcome scores using graphic formats: Results from a mixed-methods evaluation. Qual. Life Res. 2015, 24, 2457–2472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sibert, N.T.; Kowalski, C.; Pfaff, H.; Wesselmann, S.; Breidenbach, C. Clinicians’ knowledge and attitudes towards patient reported outcomes in colorectal cancer care—Insights from qualitative interviews. BMC Health Serv. Res. 2021, 21, 366. [Google Scholar] [CrossRef]
- Nguyen, H.; Butow, P.; Dhillon, H.; Sundaresan, P. A review of the barriers to using Patient-Reported Outcomes (PROs) and Patient-Reported Outcome Measures (PROMs) in routine cancer care. J. Med. Radiat. Sci. 2021, 68, 186–195. [Google Scholar] [CrossRef] [PubMed]
- Luque Ramos, A.; Redeker, I.; Hoffmann, F.; Callhoff, J.; Zink, A.; Albrecht, K. Comorbidities in Patients with Rheumatoid Arthritis and Their Association with Patient-reported Outcomes: Results of Claims Data Linked to Questionnaire Survey. J. Rheumatol. 2019, 46, 564–571. [Google Scholar] [CrossRef] [PubMed]

| Author | Study Design | Participants/Setting | Data Sources | Study Size (Complete/Included Datasets) | Outcome (PRO) | No. of Variables Used for Case-Mix Adjustment (and Specific Adjustors) | Model R2 |
|---|---|---|---|---|---|---|---|
| Deutscher et al., 2018 [25] | Retrospective analysis of prospectively collected data | Adult patients with lower back pain treated in outpatient physical therapy clinics (2014–2016) | FOTO | n = 341,642 patients n = 6934 clinicians n = 2107 hospitals | LCAT | 11: LCAT score at admission, age, sex, acuity, payer, surgical history, physical exercise history, medication/previous treatment, type of surgery, comorbidities | 0.373 |
| Farin et al., 2009 [20] | Analysis of quality assurance data | Quality assurance report for statutory rehabilitation institutions in Germany on: 1, musculoskeletal; 2, cardiological; and 3, neurological diseases | QS Reha® | 1: n = 4045 patients in n = 27 hospitals 2: n = 2503 patients in n = 25 hospitals 3: n = 1477 patients in n = 12 hospitals | 1: IRES 2: SMFA 3: MacNew | Reported elsewhere [48]: 10: age, sex, somatic, functional and psychosocial status at admission, diagnosis, multimorbidity, treatment motivation, application for pension, education | Not reported |
| Gozalo et al., [29] | Retrospective analysis of prospectively collected data | Outpatient rehabilitation clinics for patients with lower back pain | FOTO | n = 90,392 patients n = 2040 therapists n = 538 clinics | FOTO overall health status measure: OHS, PCS, PF-10 | 8: PRO at intake, age, gender, onset, surgery count, functional comorbidity index, fear avoidance level, payer type | OHS: 0.416 PCS: 0.345 PF-10: 0.421 |
| Gutacker et al., 2013 [21] | Retrospective analysis of prospectively collected data | Analysis of hospital performance variation in hip replacement surgery | NHS PROMs and routinely collected inpatient data (HES) | n = 21,565 patients n = 153 hospitals | EQ-5D | 10: pre-treatment PROs, age, gender, deprivation index, weighted Charlson Index of comorbidities, number of additional comorbidities (not included in Charlson Index), time between pre-operative assessment and admission, primary surgery, revision surgery, treatment | Not reported |
| Hendryx et al., 1999 [26] | Retrospective analysis of prospectively collected data | Development of outcome risk adjustment models for public mental health outpatient treatment programs | Patient-reported, case manager ratings, management information system data | n = 289 patients n = 6 mental health agencies | SF-12, ADL, Lehman Quality of Life Interviews | 8: sex, age, race, presence of severe primary diagnosis (major depression, schizophrenia, bipolar disorder), baseline levels of substance abuse, baseline PRO, baseline quality of life, baseline satisfaction with services | 0.34 |
| Khor et al., 2020 [22] | Retrospective analysis of prospectively collected data | Analysis of variation in PROs 1 year after elective lumbar fusion surgery across surgeons and hospitals | Spine Care and Outcomes Assessment Program (Washington State, USA) | n = 737 patients n = 17 hospitals n = 58 surgeons | ODI | 11: age, sex, insurance status, race, ASA, smoking status, prior spine surgery, diagnosis, opiate use, asthma, baseline PRO | Not reported |
| Lutz et al., 2020 [27] | Retrospective analysis of prospectively collected data | Benchmarking physical therapist study | ATI Patient Outcomes Registry | n = 182,276 patients n = 2799 physical therapists | MDQ, NDI | 10: sex, age, BMI, initial PRO, payer type, physical component score and mental component score of the Veterans RAND 12-Item Health Survey, state of physical therapy services, type of pain (acute/chronic), comorbidities | MDQ: 0.19 NDI: 0.19 |
| Nuttall et al., 2015 [23] | Retrospective analysis of prospectively collected data | Feasibility study to analyze case-mix adjustment methodology for elective surgery | NHS PROMs and HES | n = 30,555 patients n = 237 providers | OKS | 11: baseline PRO, sex, ethnicity, age, deprivation index, assistance for completing questionnaires (baseline and follow-up), disability, previous surgery, comorbidities, type of surgery, length of post-operative stay | 0.258 (ordinary least square model) 0.257 (fixed effects model) |
| Resnik & Hart 2003 [28] | Retrospective analysis of prospectively collected data | Outpatient rehabilitation clinics for patients with lower back pain | FOTO | n = 24,276 patients n = 930 therapists n = 354 hospitals | FOTO overall health status measure (OHS), PCS, PF--10 | 8: age, employment, exercise history, sex, intake PRO, onset, reimbursement, surgery | OHS: 0.416 PCS: 0.345 PF-10: 0.421 |
| Sivaganesan et al., 2018 [24] | Retrospective analysis of prospectively collected data | Report of a risk-adjusted ranking of spine surgeons and sites performing elective lumbar surgery | Quality and Outcome Database (QOD) | n = 8834 patients n = 124 surgeons n = 21 sites | ODI, EQ-5D, VAS-BP/VAS-LP | 22 (19 at patient level: age, BMI, ethnicity, education, smoking status, opioid use, comorbidities, pre-operative symptoms, motor deficit, ASA, symptom duration, interbody graft placement, worker’s compensation, liability claims, insurance status, employment, baseline PRO); 3 constructs at surgeon level: site ID, years in practice, fellowship training) | Not applicable (Bayesian model) |
| Varagunam et al., 2015 [30] | Retrospective analysis of prospectively collected data | Feasibility study analyzing different approaches on how to adjust PROM scores for individual consultant comparison for elective surgery | NHS PROMs | N = 65,465 (hip), 68,107 (knee) and 38,965 (hernia) patients N = 948 (hip), 1130 (knee) and 974 (hernia) consultants N = 183 (hip), 188 (knee) and 197 (hernia) clinics | OHS, OKS, EQ-5D | 6: age, sex, deprivation index, comorbidities, previous surgery, baseline PRO | Not reported |
| Author | What Type of Provider? | Iezzoni’s Four | Which Adjustors? | Are Criteria for the Selection of Adjustors Met? 1 | How is Case-Mix Adjustment Statistically Performed? | How are Case-Mix Adjustment Results Reported? | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Risk of What Outcome? | For What Population? | Over What Time Period? | For What Purpose? | Socio-Economic Information? | Baseline PROM Included? | Comor-Bidities? | Adjustment for ProVider Characteristics? | Are the Adjustors Associated with the Outcome? | Do Adjustors Vary Across Providers? | ||||
| Deutscher et al., 2018 [25] | Outpatient physical therapist clinics (US) | LCAT | Lower back pain patients treated in outpatient setting | Time between admission and discharge | Clinical ranking for performance measuring | x | x | x | – | Yes, assessed via back-step regression model approach | Not analyzed | Multiple regression, >50% complete patients per hospital and ≥10 complete cases per clinician per year required | Comparison between adjusted and unadjusted scores (agreement: 30%), ranking changed 70% of the hospitals, reported as percentile ranking |
| Farin et al., 2009 [20] | In- and outpatient rehab. institutions (Germany) | IRES, SMFA, MacNew | Patients in statutory rehab. institutions | Time between start and end of rehab. | Quality assurance | x | x | x | – | Not reported | Not reported | Multilevel regression, taking the standardized residuals in the prediction as the case-mix-adjusted outcome, >199 patients per institution required | 95% confidence intervals reported graphically |
| Gozalo et al., 2016 [29] | Outpatient rehabilitation clinics (US) | FOTO CATs, either generic or body impairment specific | Patients treated in outpatient rehabilitation clinics (for orthopedic conditions) | At intake and discharge from outpatient rehabilitation | Identify expert physical therapists | x | x | x | - | Not assessed | Not reported | Generalized linear model with >7 patients per clinic required | Ranking of clinics based on predicted clinic random intercept (including 95% confidence interval) |
| Gutacker et al., 2013 [21] | NHS-funded hospitals (UK) | EQ-5D | Patients receiving hip replacement in an NHS-funded hospital | Time between before/day of admission and 6 months after surgery | Inter-provider comparison for performance measuring | x | x | x | – | Yes, assessed via regression modeling | Not reported | Multilevel linear regression and probit model, no minimum number of patients per hospital required | 95% confidence intervals reported graphically |
| Hendryx et al., 1999 [26] | Outpatient mental health services (US) | SF-12 (functional status domain), Lehman Quality of Life Interview (Quality of Life domain) | Adult patients treated in outpatient mental health agencies | At baseline, 5 and 10 months | Inter-provider comparison for performance measuring | x | x | x | – | Not reported | Not assessed | Multiple linear regression, then calculating the ratio: observed/expected, no minimum number of patients per agency required | Observed score ranks and observed/expected ratio ranks are compared |
| Khor et al., 2020 [22] | In-patient hospitals performing elective spine surgery (USA) | ODI (probability of improvement beyond MID and reaching minimal disability level) | Adults treated with elective lumbar fusion surgery | At 0–60 days before surgery and at 12-month follow-up | Inter-provider comparison for performance measuring | x | x | x | – | Yes (association based on findings from earlier studies by the research group) | For all adjustors except for age, sex, and smoking status | 1. Multiple logistic model 2. Calculation of an expected number of events per provider based on a previously published risk calculator 3. Calculation of observed/expected ratio 4. Calculation of a case-mix-adjusted event rate by multiplying the O/E ratio by the overall state-wide average; >9 patients per provider required | Adjusted and unadjusted scores, ICCs to describe the proportion of total variability accounted for by between-provider variance |
| Lutz et al., 2020 [27] | Outpatient physical therapists (USA) | MDQ, NDI | Adults with episodes related to the lower back and neck with no history of related surgery | Not specified | Benchmarking physical therapists | x | x | x | x (state of physical therapy services) | Not reported | Not assessed | 1. Multiple linear regression 2. Calculation of an observed/expected ratio; >39 patients per physical therapist required | Reporting of counts of “outperforming, meeting, and underperforming” physical therapists (adjusted and unadjusted) based on 95% confidence intervals |
| Nuttall et al., 2015 [23] | NHS-funded hospitals (UK) | OKS | Patients treated by NHS providers for unilateral knee replacement | Before and 3 or 6 months after surgery | Inter-provider comparison for performance measuring | x | x | x | – | Yes (association based on findings from earlier studies) | Not analyzed | Multilevel linear regression: generalized least squares with fixed effects, general least squares with random effects, ordinary least squares, then calculating: (observed/expected) * observed mean overall; no minimum number of patients per hospital required | Differences between different adjustment scores reported, ranking reported as funnel plots |
| Resnik & Hart 2003 [28] | Outpatient rehab. clinics (USA) | OHS, PCS, PF-10 | Patients treated in outpatient rehab. clinics for lower back pain | At intake and discharge from outpatient rehabilitation | Identify expert physical therapists | x | x | x | – | Yes, bivariate analysis to identify adjustors | Not reported | Generalized linear model with >7 patients per therapist required, then calculating the difference: observed—expected; no minimum number of patients per clinic required | Percentiles of differences reported |
| Sivaganesan et al., 2018 [24] | Sites performing spine surgery (USA) | ODI, EQ-5D, VAS-BP/VAS-LP | Patients treated with spine surgery | Before and 1 year after surgery | Inter-provider comparison for performance measuring | x | x | x | x | Yes, but no association coefficients are reported | Not reported | Random effects regression models and multilevel hierarchical Bayesian models (3 levels); no minimum number of patients per hospital required | Box plots for adjusted ranks per surgeon per site reported |
| Varagunam et al., 2015 [30] | NHS-funded hospitals (UK) | OHS, OKS, EQ-5D | Patients treated by consultant in NHS providers | Before and three or six months after surgery | Inter-consultant comparison for performance measuring | x | x | x | - | Not assessed | Not reported | Multiple linear regression, >39 patients per NHS provider and >9 patients per consultant required; multilevel models | Number of consultants reported that perform better than expected, as expected, and worse than expected |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sibert, N.T.; Pfaff, H.; Breidenbach, C.; Wesselmann, S.; Kowalski, C. Different Approaches for Case-Mix Adjustment of Patient-Reported Outcomes to Compare Healthcare Providers—Methodological Results of a Systematic Review. Cancers 2021, 13, 3964. https://doi.org/10.3390/cancers13163964
Sibert NT, Pfaff H, Breidenbach C, Wesselmann S, Kowalski C. Different Approaches for Case-Mix Adjustment of Patient-Reported Outcomes to Compare Healthcare Providers—Methodological Results of a Systematic Review. Cancers. 2021; 13(16):3964. https://doi.org/10.3390/cancers13163964
Chicago/Turabian StyleSibert, Nora Tabea, Holger Pfaff, Clara Breidenbach, Simone Wesselmann, and Christoph Kowalski. 2021. "Different Approaches for Case-Mix Adjustment of Patient-Reported Outcomes to Compare Healthcare Providers—Methodological Results of a Systematic Review" Cancers 13, no. 16: 3964. https://doi.org/10.3390/cancers13163964