
ALBI Score Is a Strong Predictor of Toxicity Following SIRT for Hepatocellular Carcinoma

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Therapy Protocol
2.3. Assessments
2.4. Calculation of Liver Function Scores
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
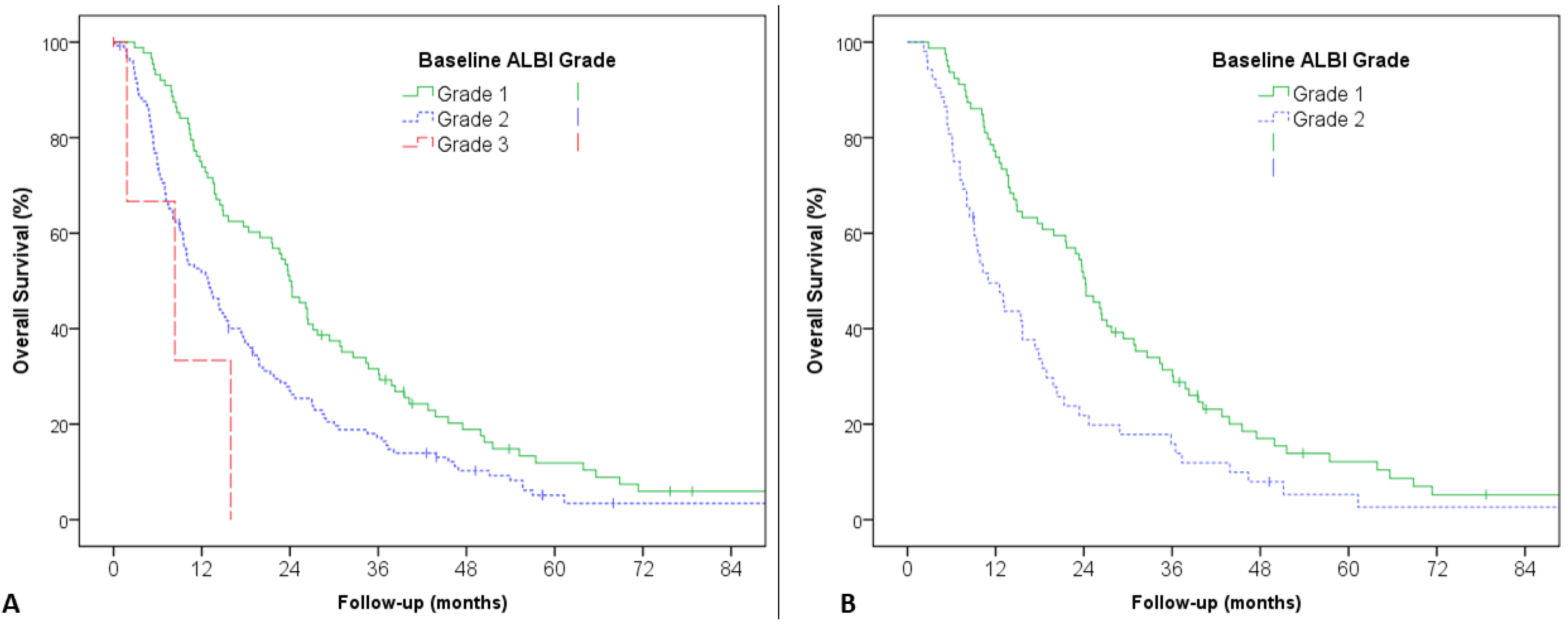
3.2. Prognostic Value of Baseline ALBI Score
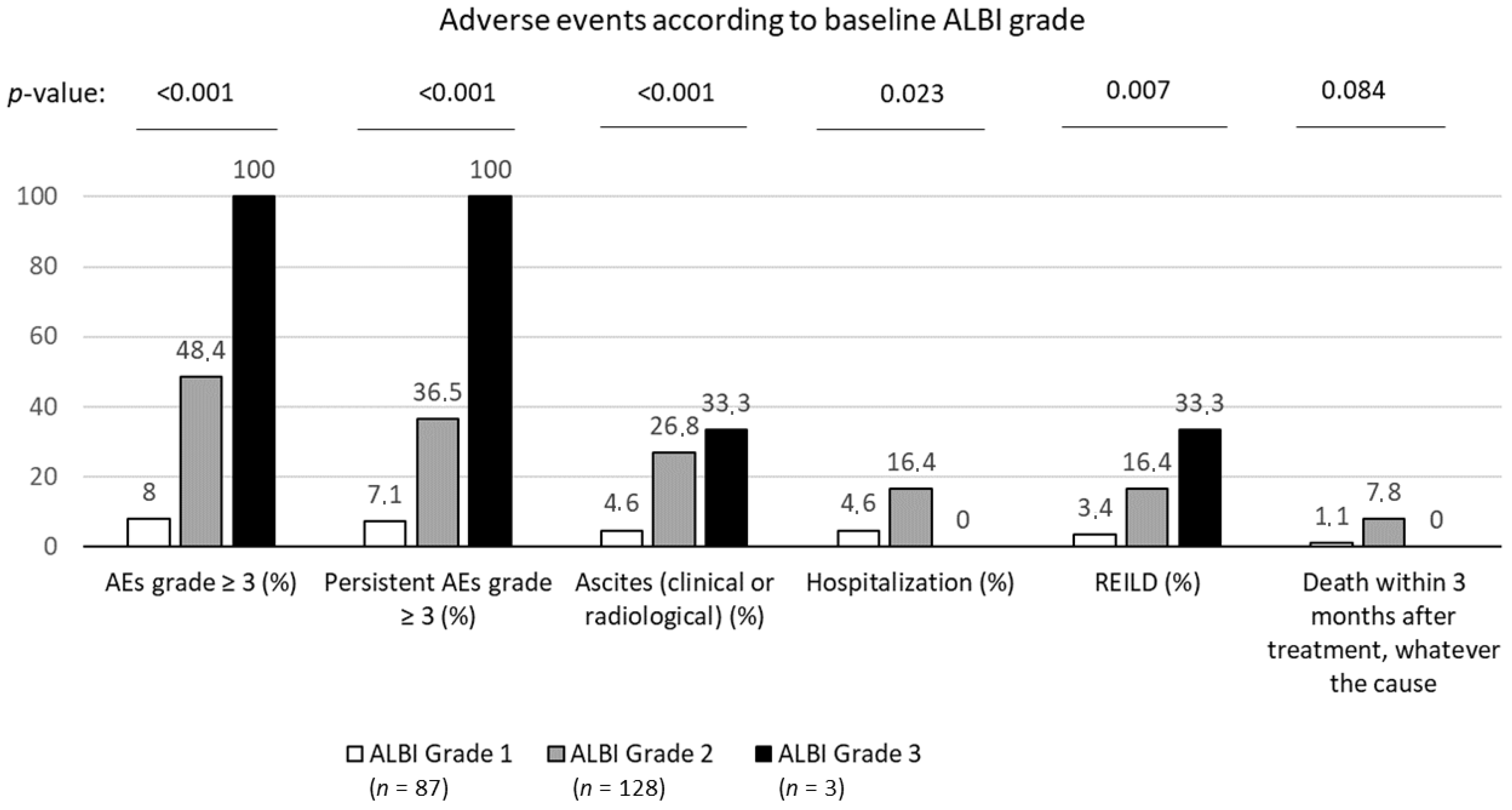
3.3. Baseline ALBI Grade Was Strongly Associated with Toxicity, Including REILD, after First SIRT
3.4. ALBI Score Variation Following SIRT
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Global Burden of Disease Cancer Collaboration; Fitzmaurice, C.; Abate, D.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdel-Rahman, O.; Abdelalim, A.; Abdoli, A.; Abdollahpour, I.; et al. Global, regional, and national cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life-years for 29 cancer groups, 1990 to 2017: A systematic analysis for the global burden of disease study. JAMA Oncol. 2019. [Google Scholar] [CrossRef] [Green Version]
- European Association for the Study of the Liver. EASL Clinical practice guidelines management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inghilesi, A.L.; Gallori, D.; Antonuzzo, L.; Forte, P.; Tomcikova, D.; Arena, U.; Colagrande, S.; Pradella, S.; Fani, B.; Gianni, E.; et al. Predictors of survival in patients with established cirrhosis and hepatocellular carcinoma treated with sorafenib. World J. Gastroenterol. 2014, 20, 786–794. [Google Scholar] [CrossRef] [PubMed]
- Child, C.G.; Turcotte, J.G. Surgery and portal hypertension. Major Probl. Clin. Surg. 1964, 1, 1–85. [Google Scholar] [PubMed]
- Pugh, R.N.; Murray-Lyon, I.M.; Dawson, J.L.; Pietroni, M.C.; Williams, R. Transection of the oesophagus for bleeding oesophageal varices. Br. J. Surg. 1973, 60, 646–649. [Google Scholar] [CrossRef]
- Johnson, P.J.; Berhane, S.; Kagebayashi, C.; Satomura, S.; Teng, M.; Reeves, H.L.; O’Beirne, J.; Fox, R.; Skowronska, A.; Palmer, D.; et al. Assessment of liver function in patients with hepatocellular carcinoma: A new evidence-based approach-the ALBI GRADE. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2015, 33, 550–558. [Google Scholar] [CrossRef]
- Toyoda, H.; Lai, P.B.S.; O’Beirne, J.; Chong, C.C.; Berhane, S.; Reeves, H.; Manas, D.; Fox, R.P.; Yeo, W.; Mo, F.; et al. Long-term impact of liver function on curative therapy for hepatocellular carcinoma: Application of the ALBI grade. Br. J. Cancer 2016, 114, 744–750. [Google Scholar] [CrossRef]
- Edeline, J.; Blanc, J.-F.; Johnson, P.; Campillo-Gimenez, B.; Ross, P.; Ma, Y.T.; King, J.; Hubner, R.A.; Sumpter, K.; Darby, S.; et al. A multicentre comparison between child pugh and albumin-bilirubin scores in patients treated with sorafenib for hepatocellular carcinoma. Liver Int. Off. J. Int. Assoc. Study Liver 2016, 36, 1821–1828. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edeline, J.; Crouzet, L.; Campillo-Gimenez, B.; Rolland, Y.; Pracht, M.; Guillygomarc’h, A.; Boudjema, K.; Lenoir, L.; Adhoute, X.; Rohou, T.; et al. Selective internal radiation therapy compared with sorafenib for hepatocellular carcinoma with portal vein thrombosis. Eur. J. Nucl. Med. Mol. Imaging 2016, 43, 635–643. [Google Scholar] [CrossRef]
- Sangro, B.; Iñarrairaegui, M.; Bilbao, J.I. Radioembolization for hepatocellular carcinoma. J. Hepatol. 2012, 56, 464–473. [Google Scholar] [CrossRef]
- Chow, P.K.H.; Gandhi, M.; Tan, S.-B.; Khin, M.W.; Khasbazar, A.; Ong, J.; Choo, S.P.; Cheow, P.C.; Chotipanich, C.; Lim, K.; et al. SIRveNIB: Selective internal radiation therapy versus sorafenib in Asia-Pacific patients with hepatocellular carcinoma. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2018, 36, 1913–1921. [Google Scholar] [CrossRef]
- Vilgrain, V.; Pereira, H.; Assenat, E.; Guiu, B.; Ilonca, A.D.; Pageaux, G.-P.; Sibert, A.; Bouattour, M.; Lebtahi, R.; Allaham, W.; et al. Efficacy and safety of selective internal radiotherapy with yttrium-90 Resin Microspheres Compared with Sorafenib in Locally Advanced and Inoperable Hepatocellular Carcinoma (SARAH): An open-label randomised controlled phase 3 trial. Lancet Oncol. 2017, 18, 1624–1636. [Google Scholar] [CrossRef]
- Ricke, J.; Klümpen, H.J.; Amthauer, H.; Bargellini, I.; Bartenstein, P.; de Toni, E.N.; Gasbarrini, A.; Pech, M.; Peck-Radosavljevic, M.; Popovič, P.; et al. Impact of combined selective internal radiation therapy and sorafenib on survival in advanced hepatocellular carcinoma. J. Hepatol. 2019, 71, 1164–1174. [Google Scholar] [CrossRef]
- Garin, E.; Tselikas, L.; Guiu, B.; Chalaye, J.; Edeline, J.; de Baere, T.; Assenat, E.; Tacher, V.; Robert, C.; Terroir-Cassou-Mounat, M.; et al. Personalised versus Standard Dosimetry Approach of Selective Internal Radiation Therapy in Patients with Locally Advanced Hepatocellular Carcinoma (DOSISPHERE-01): A randomised, multicentre, open-label phase 2 trial. Lancet Gastroenterol. Hepatol. 2021, 6, 17–29. [Google Scholar] [CrossRef]
- Garin, E.; Rolland, Y.; Campillo-Gimenez, B.; Edeline, J. Negative phase 3 study of 90Y microspheres versus sorafenib in HCC. Lancet Oncol. 2018, 19, e70. [Google Scholar] [CrossRef] [Green Version]
- Hickey, R.; Mouli, S.; Kulik, L.; Desai, K.; Thornburg, B.; Ganger, D.; Baker, T.; Abecassis, M.; Ralph Kallini, J.; Gabr, A.; et al. Independent analysis of albumin-bilirubin grade in a 765-patient cohort treated with transarterial locoregional therapy for hepatocellular carcinoma. J. Vasc. Interv. Radiol. JVIR 2016, 27, 795–802. [Google Scholar] [CrossRef]
- Antkowiak, M.; Gabr, A.; Das, A.; Ali, R.; Kulik, L.; Ganger, D.; Moore, C.; Abecassis, M.; Katariya, N.; Mouli, S.; et al. Prognostic role of albumin, bilirubin, and ALBI scores: Analysis of 1000 patients with hepatocellular carcinoma undergoing radioembolization. Cancers 2019, 11, 879. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gui, B.; Weiner, A.A.; Nosher, J.; Lu, S.-E.; Foltz, G.M.; Hasan, O.; Kim, S.K.; Gendel, V.; Mani, N.B.; Carpizo, D.R.; et al. Assessment of the Albumin-Bilirubin (ALBI) grade as a prognostic indicator for hepatocellular carcinoma patients treated with radioembolization. Am. J. Clin. Oncol. 2018, 41, 861–866. [Google Scholar] [CrossRef] [PubMed]
- Azar, A.; Devcic, Z.; Paz-Fumagalli, R.; Vidal, L.L.C.; McKinney, J.M.; Frey, G.; Lewis, A.R.; Ritchie, C.; Starr, J.S.; Mody, K.; et al. Albumin-bilirubin grade as a prognostic indicator for patients with non-hepatocellular primary and metastatic liver malignancy undergoing yttrium-90 radioembolization using resin microspheres. J. Gastrointest. Oncol. 2020, 11, 715–723. [Google Scholar] [CrossRef]
- Salem, R.; Thurston, K.G. Radioembolization with 90yttrium microspheres: A state-of-the-art brachytherapy treatment for primary and secondary liver malignancies. Part 1: Technical and methodologic considerations. J. Vasc. Interv. Radiol. JVIR 2006, 17, 1251–1278. [Google Scholar] [CrossRef] [Green Version]
- Salem, R.; Padia, S.A.; Lam, M.; Bell, J.; Chiesa, C.; Fowers, K.; Hamilton, B.; Herman, J.; Kappadath, S.C.; Leung, T.; et al. Clinical and dosimetric considerations for Y90: Recommendations from an international multidisciplinary working group. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 1695–1704. [Google Scholar] [CrossRef] [PubMed]
- Sangro, B.; Gil-Alzugaray, B.; Rodriguez, J.; Sola, I.; Martinez-Cuesta, A.; Viudez, A.; Chopitea, A.; Iñarrairaegui, M.; Arbizu, J.; Bilbao, J.I. Liver disease induced by radioembolization of liver tumors. Cancer 2008, 112, 1538–1546. [Google Scholar] [CrossRef]
- Gil-Alzugaray, B.; Chopitea, A.; Iñarrairaegui, M.; Bilbao, J.I.; Rodriguez-Fraile, M.; Rodriguez, J.; Benito, A.; Dominguez, I.; D’Avola, D.; Herrero, J.I.; et al. Prognostic factors and prevention of radioembolization-induced liver disease. Hepatology 2013, 57, 1078–1087. [Google Scholar] [CrossRef]
- Vilgrain, V.; Abdel-Rehim, M.; Sibert, A.; Ronot, M.; Lebtahi, R.; Castéra, L.; Chatellier, G.; SARAH Trial Group. Radioembolisation with Yttrium‒90 microspheres versus Sorafenib for Treatment of Advanced Hepatocellular Carcinoma (SARAH): Study protocol for a randomised controlled trial. Trials 2014, 15, 474. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garin, E.; Rolland, Y.; Pracht, M.; Le Sourd, S.; Laffont, S.; Mesbah, H.; Haumont, L.; Lenoir, L.; Rohou, T.; Brun, V.; et al. High impact of macroaggregated albumin-based tumour dose on response and overall survival in hepatocellular carcinoma patients treated with 90Y-loaded glass microsphere radioembolization. Liver Int. 2017, 37, 101–110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raoul, J.-L.; Kudo, M.; Finn, R.S.; Edeline, J.; Reig, M.; Galle, P.R. Systemic therapy for intermediate and advanced hepatocellular carcinoma: Sorafenib and beyond. Cancer Treat. Rev. 2018, 68, 16–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | n = 222 | |
|---|---|---|
| Age, median | 66.4 ± 8.9 | |
| Gender | Female | 28 (12.6%) |
| Male | 194 (87.4%) | |
| Performance Status | 0 | 149 (67.1%) |
| 1 or 2 | 73 (32.9%) | |
| Cirrhosis | 189 (85.1%) | |
| Alcohol consumption | 140 (63.1%) | |
| Hepatitis infection B | 10 (4.5%) | |
| Hepatitis infection C | 31 (14.0%) | |
| Previous treatment for HCC before SIRT | 121 (54.5%) | |
| Surgery | 41 (18.5%) | |
| Radiofrequency ablation | 23 (10.4%) | |
| Trans-arterial chemoembolization (TACE) | 59 (26.6%) | |
| I131-lipiodol | 21 (9.5%) | |
| Macrovascular invasion | 109 (49.0%) | |
| Main portal vein or hepatic vei | 21 (9.5%) | |
| Branch portal vein | 88 (39.6%) | |
| ALBI score, median (range) | −2.49 (−3.51; −1.17) | |
| ALBI Grade | 1 | 88 (39.6%) |
| 2 | 130 (58.6%) | |
| 3 | 4 (1.8%) | |
| Child−Pugh Score | A5 | 131 (59%) |
| A6 | 70 (31.5%) | |
| B7 | 18 (8.1%) | |
| B8 | 3 (1.4%) | |
| Number of liver tumors | 1 | 75 (33.8%) |
| 2 | 31 (14.0%) | |
| 3 or more | 116 (52.3%) | |
| Median size of the lesion, in mm (range) | 67 (10–170) | |
| Median alpha-fetoprotein, median (range) | 19 (1–235,700) | |
| Barcelona clinic civer cancer (BCLC) stage | A | 1 (0.5%) |
| B | 67 (30.2%) | |
| C | 154 (68.4%) | |
| D | 0 (0%) | |
| Overall delivered activity, in GBq, median (range) | 4.3 (0.23–350) | |
| Dose delivered to tumor, in Gy, median (range) | 322.6 (119.3–880) | |
| Lung dose, in Gy, median (range) | 4 (0–32) | |
| Nontumoral liver dose, in Gy, median (range) | 85.4 (0–221) | |
| Average dose to treated liver, in Gy, median (range) | 126.7 (16–252) | |
| First SIRT localization, n (%) | Left liver | 62 (28%) |
| Right liver | 151 (68%) | |
| Bilateral | 9 (4%) | |
| Second SIRT, n (%) | 55 (25%) | |
| Second SIRT localization, n (%) | Left liver | 27 (12%) |
| Right liver | 25 (11%) | |
| Bilateral | 3 (11%) | |
| Dose ≥ 205 Gy, n (%) | 174 (78%) | |
| Glass microspheres, n (%) | 210 (95%) | |
| Resin microspheres, n (%) | 12 (5%) | |
| Variables | Univariate Analysis | ||
|---|---|---|---|
| HR (95% CI) | p-Value | ||
| Age (continuous) | 0.99 (0.98–1.01) | 0.54 | |
| Gender (male vs. female) | 1.07 (0.75–1.72) | 0.75 | |
| Cirrhosis (yes vs. no) | 1.23 (0.83–1.82) | 0.31 | |
| Etiology of cirrhosis: | Alcohol | 1.01 (0.76–1.35) | 0.93 |
| Hepatitis B infection | 1.02 (0.52–1.99) | 0.95 | |
| Hepatitis C infection | 1.43 (0.96–2.12) | 0.08 | |
| NASH/others | 1.11 (0.84–1.46) | 0.46 | |
| Treatment before SIRT | 0.95 (0.72–1.25) | 0.54 | |
| —TACE | 1.19 (0.97–1.45) | 0.09 | |
| —Sorafenib | 0.92 (0.62–1.34) | 0.65 | |
| Macrovascular invasion | 1.34 (1.01–1.76) | 0.04 | |
| Bigger tumor size | 1.00 (0.99–1.01) | 0.16 | |
| Performance status (0 vs. 1 or 2) | 1.37 (1.02–1.76) | 0.16 | |
| Child−Pugh score (points) | 1.27 (1.04–1.56) | 0.02 | |
| Child−Pugh score (A vs. B or C) | 0.54 (0.34–0.87) | 0.01 | |
| ALBI score | 1.89 (1.39–2.56) | <0.001 | |
| ALBI grade (2 or 3 vs. 1) | 1.64 (1.23–2.18) | 0.001 | |
| Multifocal | 1.34 (0.99–1.80) | 0.05 | |
| Baseline alpha-fetoprotein | 1 (1–1) | 0.03 | |
| BCLC (A/B/C/D) | 1.47 (1.08–1.99) | 0.01 | |
| Baseline albumin | 0.95 (0.92–0.97) | <0.001 | |
| Baseline bilirubin | 1.01 (1–1.02) | 0.11 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lescure, C.; Estrade, F.; Pedrono, M.; Campillo-Gimenez, B.; Le Sourd, S.; Pracht, M.; Palard, X.; Bourien, H.; Muzellec, L.; Uguen, T.; et al. ALBI Score Is a Strong Predictor of Toxicity Following SIRT for Hepatocellular Carcinoma. Cancers 2021, 13, 3794. https://doi.org/10.3390/cancers13153794
Lescure C, Estrade F, Pedrono M, Campillo-Gimenez B, Le Sourd S, Pracht M, Palard X, Bourien H, Muzellec L, Uguen T, et al. ALBI Score Is a Strong Predictor of Toxicity Following SIRT for Hepatocellular Carcinoma. Cancers. 2021; 13(15):3794. https://doi.org/10.3390/cancers13153794
Chicago/Turabian StyleLescure, Céline, Florian Estrade, Maud Pedrono, Boris Campillo-Gimenez, Samuel Le Sourd, Marc Pracht, Xavier Palard, Héloïse Bourien, Léa Muzellec, Thomas Uguen, and et al. 2021. "ALBI Score Is a Strong Predictor of Toxicity Following SIRT for Hepatocellular Carcinoma" Cancers 13, no. 15: 3794. https://doi.org/10.3390/cancers13153794