
Adjuvant Radiotherapy Significantly Increases Neck Control and Survival in Early Oral Cancer Patients with Solitary Nodal Involvement: A National Cancer Registry Database Analysis


Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Patient Demographics and Measurements
2.3. Statistical Analysis
3. Results
3.1. Clinicopathological Characteristics
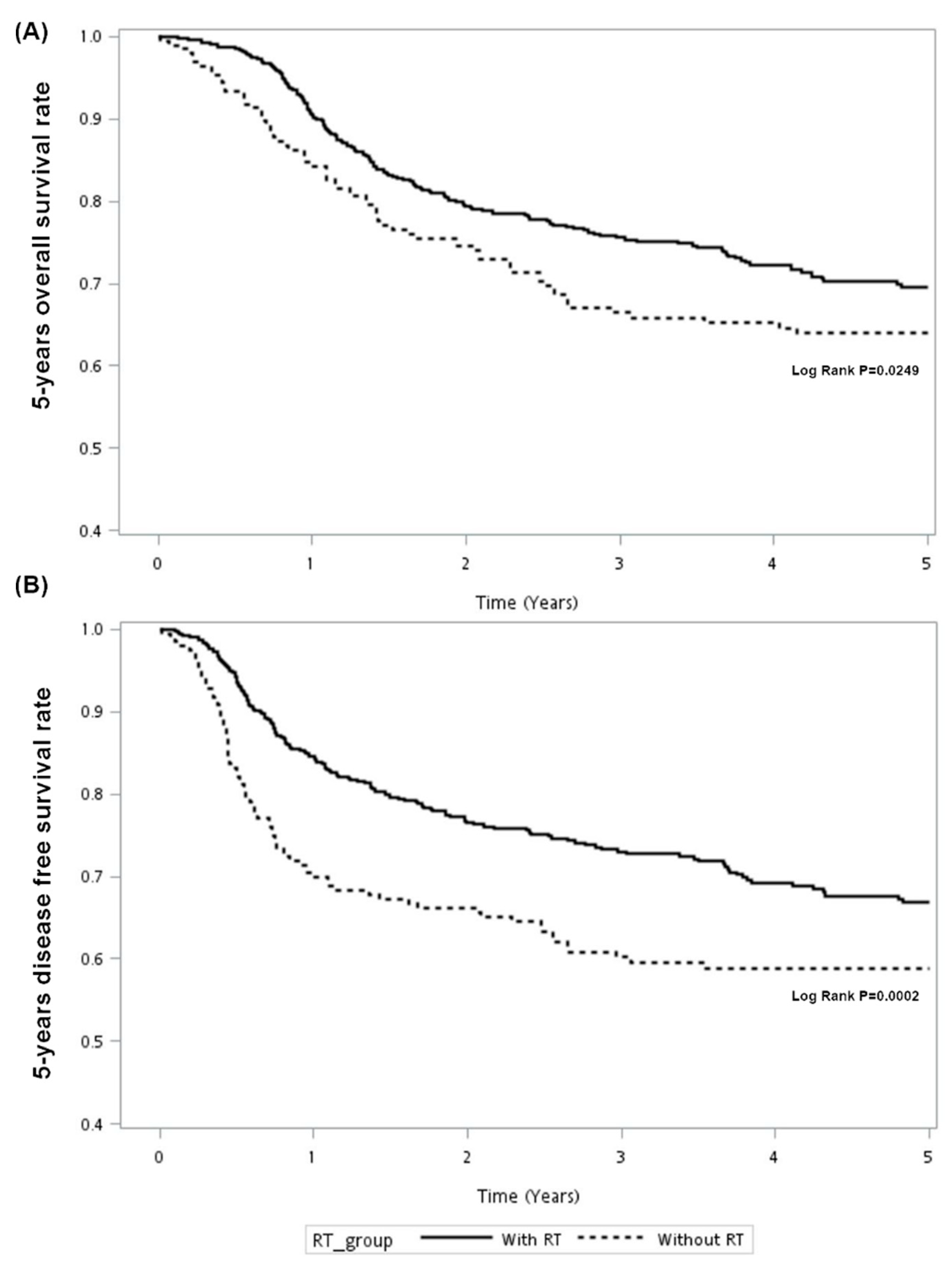
3.2. Analysis for Survival and Neck Control
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| TCR | Taiwan Cancer Registry |
| NHI | National Health Insurance |
| CCI | Charlson Comorbidity Index |
| TNM | tumor-node-metastasis |
| LN | lymph node |
| OS | overall survival |
| DFS | disease-free survival |
| HR | hazard ratio |
| CI | Confidence Interval |
| aHR | adjusted hazard ratio |
| NCDB | National Cancer Database |
References
- Ghantous, Y.; Abu Elnaaj, I. Global Incidence and Risk Factors of Oral Cancer. Harefuah 2017, 156, 645–649. [Google Scholar]
- Hung, L.C.; Kung, P.T.; Lung, C.H.; Tsai, M.H.; Liu, S.A.; Chiu, L.T.; Huang, K.H.; Tsai, W.C. Assessment of the Risk of Oral Cancer Incidence in A High-Risk Population and Establishment of A Predictive Model for Oral Cancer Incidence Using A Population-Based Cohort in Taiwan. Int. J. Environ. Res. Public Health 2020, 17, 665. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheraghlou, S.; Schettino, A.; Zogg, C.K.; Judson, B.L. Changing prognosis of oral cancer: An analysis of survival and treatment between 1973 and 2014. Laryngoscope 2018, 128, 2762–2769. [Google Scholar] [CrossRef] [PubMed]
- Myers, J.N.; Elkins, T.; Roberts, D.; Byers, R.M. Squamous cell carcinoma of the tongue in young adults: Increasing incidence and factors that predict treatment outcomes. Otolaryngol. Head Neck Surg. 2000, 122, 44–51. [Google Scholar] [CrossRef]
- Koyfman, S.A.; Ismaila, N.; Crook, D.; D’Cruz, A.; Rodriguez, C.P.; Sher, D.J.; Silbermins, D.; Sturgis, E.M.; Tsue, T.T.; Weiss, J.; et al. Management of the Neck in Squamous Cell Carcinoma of the Oral Cavity and Oropharynx: ASCO Clinical Practice Guideline. J. Clin. Oncol. 2019, 37, 1753–1774. [Google Scholar] [CrossRef]
- Pfister, D.G.; Spencer, S.; Adelstein, D.; Adkins, D.; Anzai, Y.; Brizel, D.M.; Bruce, J.Y.; Busse, P.M.; Caudell, J.J.; Cmelak, A.J.; et al. Head and Neck Cancers, Version 2.2020, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2020, 18, 873–898. [Google Scholar] [CrossRef]
- Schiff, B.A.; Roberts, D.B.; El-Naggar, A.; Garden, A.S.; Myers, J.N. Selective vs Modified Radical Neck Dissection and Postoperative Radiotherapy vs Observation in the Treatment of Squamous Cell Carcinoma of the Oral Tongue. Arch. Otolaryngol. Head Neck Surg. 2005, 131, 874–878. [Google Scholar] [CrossRef] [Green Version]
- Jackel, M.C.; Ambrosch, P.; Christiansen, H.; Martin, A.; Steiner, W. Value of postoperative radiotherapy in patients with pathologic N1 neck disease. Head Neck 2008, 30, 875–882. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.C.; Wang, C.T.; Ko, J.Y.; Lou, P.J.; Yang, T.L.; Ting, L.L.; Wang, C.W.; Hu, Y.L.; Wang, C.P. Postoperative radiotherapy for primary early oral tongue cancer with pathologic N1 neck. Head Neck 2010, 32, 555–561. [Google Scholar] [CrossRef]
- Bray, F.; Parkin, D.M. Evaluation of data quality in the cancer registry: Principles and methods. Part I: Comparability, validity and timeliness. Eur. J. Cancer 2009, 45, 747–755. [Google Scholar] [CrossRef] [PubMed]
- Chiang, C.J.; Lo, W.C.; Yang, Y.W.; You, S.L.; Chen, C.J.; Lai, M.S. Incidence and survival of adult cancer patients in Taiwan, 2002–2012. J. Formos. Med. Assoc. 2016, 115, 1076–1088. [Google Scholar] [CrossRef] [Green Version]
- Chang, H.J.; Chen, P.C.; Yang, C.C.; Su, Y.C.; Lee, C.C. Comparison of Elixhauser and Charlson Methods for Predicting Oral Cancer Survival. Medicine 2016, 95, e2861. [Google Scholar] [CrossRef]
- Divi, V.; Chen, M.M.; Nussenbaum, B.; Rhoads, K.F.; Sirjani, D.B.; Holsinger, F.C.; Shah, J.L.; Hara, W. Lymph Node Count From Neck Dissection Predicts Mortality in Head and Neck Cancer. J. Clin. Oncol. 2016, 34, 3892–3897. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.C.; Su, Y.C.; Hung, S.K.; Chen, P.C.; Huang, C.I.; Huang, W.L.; Lin, Y.W.; Yang, C.C. Recommendation for incorporation of a different lymph node scoring system in future AJCC N category for oral cancer. Sci. Rep. 2017, 7, 14117. [Google Scholar] [CrossRef]
- Ettinger, K.S.; Ganry, L.; Fernandes, R.P. Oral Cavity Cancer. Oral Maxillofac. Surg. Clin. N. Am. 2019, 31, 13–29. [Google Scholar] [CrossRef]
- Shrime, M.G.; Gullane, P.J.; Dawson, L.; Kim, J.; Gilbert, R.W.; Irish, J.C.; Brown, D.H.; Goldstein, D.P. The impact of adjuvant radiotherapy on survival in T1-2N1 squamous cell carcinoma of the oral cavity. Arch. Otolaryngol. Head Neck Surg. 2010, 136, 225–228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rajappa, S.K.; Maheshwari, U.; Ram, D.; Koyyala, V.P.B.; Mandal, G.; Goyal, S.; Kumar, R.; Dewan, A.K. Early oral cavity cancer: The prognostic factors and impact of adjuvant radiation on survival. Head Neck 2019, 41, 3577–3583. [Google Scholar] [CrossRef] [PubMed]
- Ivaldi, E.; Di Mario, D.; Paderno, A.; Piazza, C.; Bossi, P.; Iacovelli, N.A.; Incandela, F.; Locati, L.; Fallai, C.; Orlandi, E. Postoperative radiotherapy (PORT) for early oral cavity cancer (pT1-2,N0-1): A review. Crit. Rev. Oncol. Hematol. 2019, 143, 67–75. [Google Scholar] [CrossRef]
- Moergel, M.; Meurer, P.; Ingel, K.; Wendt, T.G.; Al-Nawas, B. Effectiveness of postoperative radiotherapy in patients with small oral and oropharyngeal squamous cell carcinoma and concomitant ipsilateral singular cervical lymph node metastasis (pN1): A meta-analysis. Strahlenther. Onkol. 2011, 187, 337–343. [Google Scholar] [CrossRef] [PubMed]
- Qian, X.; Sinikovic, B.; Schreiber, F.; Ochsenreither, S.; Klinghammer, K.; Wollenberg, B.; Kaufmann, A.M.; Albers, A.E. pN status predicts outcomes in surgically treated pT1-pT2 patients of various disease stages with squamous cell carcinoma of the head and neck: A 17-year retrospective single center cohort study. Eur. Arch. Otorhinolaryngol. 2018, 275, 2787–2795. [Google Scholar] [CrossRef]
- Torrecillas, V.; Shepherd, H.M.; Francis, S.; Buchmann, L.O.; Monroe, M.M.; Lloyd, S.; Cannon, D.; Hitchcock, Y.J.; Weis, J.R.; Hunt, J.P.; et al. Adjuvant radiation for T1-2N1 oral cavity cancer survival outcomes and utilization treatment trends: Analysis of the SEER database. Oral Oncol. 2018, 85, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.M.; Harris, J.P.; Hara, W.; Sirjani, D.; Divi, V. Association of Postoperative Radiotherapy with Survival in Patients With N1 Oral Cavity and Oropharyngeal Squamous Cell Carcinoma. JAMA Otolaryngol. Head Neck Surg. 2016, 142, 1224–1230. [Google Scholar] [CrossRef]
- Suresh, K.; Cramer, J.D. Postoperative radiation therapy vs observation for pN1 oral cavity squamous cell carcinoma. Head Neck 2019, 41, 4136–4142. [Google Scholar] [CrossRef] [PubMed]
- Xiang, M.; Holsinger, F.C.; Gensheimer, M.F.; Divi, V.; Pollom, E.L.; Colevas, A.D.; Le, Q.T.; Beadle, B.M. Postoperative Observation Versus Radiotherapy for Pathologic N1 Oral Cavity Squamous Cell Carcinoma. Am. J. Clin. Oncol. 2021, 44, 99–104. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.C.; Su, Y.C.; Lin, Y.W.; Huang, C.I.; Lee, C.C. Differential impact of age on survival in head and neck cancer according to classic Cox regression and decision tree analysis. Clin. Otolaryngol. 2019, 44, 244–253. [Google Scholar] [CrossRef]
- Rusthoven, K.; Ballonoff, A.; Raben, D.; Chen, C. Poor prognosis in patients with stage I and II oral tongue squamous cell carcinoma. Cancer 2008, 112, 345–351. [Google Scholar] [CrossRef]
- Weiss, B.G.; Anczykowski, M.Z.; Flach, S.; Spiegel, J.L.; Kitz, J.; Bertlich, M.; Canis, M.; Jakob, M.; Ihler, F. Benefit of postoperative radiotherapy for early tumors with single ipsilateral lymph node metastasis. Laryngoscope 2020, 130, E530–E538. [Google Scholar] [CrossRef] [Green Version]
- de Abreu, P.M.; Co, A.C.G.; Azevedo, P.L.; do Valle, I.B.; de Oliveira, K.G.; Gouvea, S.A.; Cordeiro-Silva, M.F.; Louro, I.D.; de Podesta, J.R.V.; Lenzi, J.; et al. Frequency of HPV in oral cavity squamous cell carcinoma. BMC Cancer 2018, 18, 324. [Google Scholar] [CrossRef] [PubMed]
- Lee, L.A.; Huang, C.G.; Liao, C.T.; Lee, L.Y.; Hsueh, C.; Chen, T.C.; Lin, C.Y.; Fan, K.H.; Wang, H.M.; Huang, S.F.; et al. Human papillomavirus-16 infection in advanced oral cavity cancer patients is related to an increased risk of distant metastases and poor survival. PLoS ONE 2012, 7, e40767. [Google Scholar] [CrossRef]
- Chang, K.C.; Su, I.J.; Tsai, S.T.; Shieh, D.B.; Jin, Y.T. Pathological features of betel quid-related oral epithelial lesions in taiwan with special emphasis on the tumor progression and human papillomavirus association. Oncology 2002, 63, 362–369. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variation | RT | p Value * | |
|---|---|---|---|
| No (n = 196) | Yes (n = 505) | ||
| n (%) | n (%) | ||
| Gender | |||
| Female | 20 (10.20) | 53 (10.50) | 0.9099 |
| Male | 176 (89.80) | 452 (89.50) | |
| Age, years | |||
| <65 | 155 (79.08) | 448 (88.71) | 0.0010 |
| ≥65 | 41 (20.92) | 57 (11.29) | |
| AJCC pT | |||
| T1 | 76 (38.78) | 144 (28.51) | 0.0086 |
| T2 | 120 (61.22) | 361 (71.49) | |
| Grade | |||
| Well/moderately | 179 (91.33) | 425 (84.16) | 0.0136 |
| Poorly/undifferentiated | 17 (8.67) | 80 (15.84) | |
| Site | |||
| Tongue | 85 (43.37) | 250 (49.50) | 0.1443 |
| Other | 111 (56.63) | 255 (50.50) | |
| CCI group | |||
| 0 | 133 (67.86) | 387 (76.63) | 0.0383 |
| 1 | 37 (18.88) | 77 (15.25) | |
| ≥2 | 26 (13.27) | 41 (8.12) | |
| Hospital level | |||
| Medical center | 150 (76.53) | 359 (71.09) | 0.1471 |
| Non-medical center | 46 (23.47) | 146 (28.91) | |
| Mortality | 76 (38.78) | 157 (31.09) | 0.0525 |
| Variation | N | % |
|---|---|---|
| RT dose, missing (n = 9) | ||
| ≤50 Gy | 14 | 2.82 |
| 50–60 Gy | 154 | 31.05 |
| 60–70 Gy | 319 | 64.31 |
| >70 Gy | 9 | 1.81 |
| RT techniques, missing (n = 11) | ||
| 3D | 28 | 5.67 |
| IMRT | 422 | 85.43 |
| VMAT | 44 | 8.91 |
| RT fields, missing (n = 9) | ||
| Primary only | 3 | 0.60 |
| Neck only | 3 | 0.60 |
| Primary + neck | 490 | 98.80 |
| Variation | 5-Year DFS | 5-Year DFS | ||||||
|---|---|---|---|---|---|---|---|---|
| Crude HR (95% C.I) | p Value | Adjusted HR (95% C.I) | p Value | Crude HR (95% C.I) | p Value | Adjusted HR (95% C.I) | p Value | |
| All | ||||||||
| RT | 0.76 (0.57–1.01) | 0.0596 | 0.72 (0.54–0.97) | 0.0288 | 0.66 (0.50–0.87) | 0.0030 | 0.64 (0.48–0.84) | 0.0016 |
| Age, ≥65 | 1.30 (0.90–1.88) | 0.1570 | 1.25 (0.85–1.84) | 0.2591 | 1.35 (0.95–1.91) | 0.0986 | 1.30 (0.90–1.87) | 0.1681 |
| Male | 1.17 (0.73–1.88) | 0.5064 | 1.27 (0.78–2.08) | 0.3447 | 1.27 (0.80–2.04) | 0.3131 | 1.38 (0.85–2.25) | 0.1960 |
| pT2 | 1.81 (1.31–2.51) | 0.0004 | 1.79 (1.29–2.50) | 0.0006 | 1.61 (1.18–2.19) | 0.0026 | 1.63 (1.19–2.23) | 0.0024 |
| Grade (Well/moderately) | 0.62 (0.44–0.87) | 0.0055 | 0.65 (0.46–0.91) | 0.0135 | 0.67 (0.48–0.93) | 0.0186 | 0.69 (0.49–0.98) | 0.0369 |
| CCI group | ||||||||
| 0 | Ref. | Ref. | Ref. | Ref. | ||||
| 1 | 1.16 (0.81–1.67) | 0.4181 | 1.14 (0.78–1.66) | 0.4937 | 1.05 (0.73–1.51) | 0.7789 | 1.01 (0.70–1.46) | 0.9531 |
| ≥2 | 1.88 (1.28–2.77) | 0.0014 | 1.75 (1.18–2.60) | 0.0056 | 1.71 (1.16–2.51) | 0.0064 | 1.58 (1.06–2.34) | 0.0233 |
| Hospital level, medical center | 1.08 (0.79–1.46) | 0.6347 | 1.06 (0.78–1.44) | 0.7337 | 1.10 (0.81–1.47) | 0.5464 | 1.06 (0.78–1.43) | 0.7105 |
| Site | ||||||||
| Tongue | 1.04 (0.80–1.36) | 0.7668 | 1.07 (0.81–1.40) | 0.6423 | 1.10 (0.85–1.43) | 0.4830 | 1.14 (0.88–1.49) | 0.3244 |
| Other | Ref. | Ref. | Ref. | Ref. | ||||
| RT vs. Non-RT | 5-Year OS | 5-Year DFS | ||||||
|---|---|---|---|---|---|---|---|---|
| Crude HR (95% C.I) | p Value | Adjusted HR (95% C.I) | p Value | Crude HR (95% C.I) | p Value | Adjusted HR (95% C.I) | p Value | |
| Gender | ||||||||
| Male | 0.83 (0.62–1.13) | 0.2419 | 0.80 (0.59–1.09) | 0.1588 | 0.73 (0.55–0.98) | 0.0349 | 0.71 (0.52–0.95) | 0.0221 |
| Female | 0.32 (0.13–0.78) | 0.0128 | 0.31 (0.12–0.84) | 0.0206 | 0.25 (0.10–0.62) | 0.0028 | 0.23 (0.09–0.61) | 0.0033 |
| Age, years | ||||||||
| <65 | 0.93 (0.67–1.30) | 0.6734 | 0.88 (0.63–1.23) | 0.4597 | 0.74 (0.54–1.01) | 0.0560 | 0.70 (0.51–0.96) | 0.0257 |
| ≥65 | 0.35 (0.17–0.70) | 0.0028 | 0.29 (0.14–0.62) | 0.0012 | 0.45 (0.23–0.86) | 0.0160 | 0.42 (0.21–0.84) | 0.0145 |
| AJCC pT | ||||||||
| T1 | 1.00 (0.55–1.84) | 0.9902 | 0.97 (0.51–1.83) | 0.9230 | 0.79 (0.45–1.39) | 0.4193 | 0.80 (0.44–1.44) | 0.4509 |
| T2 | 0.63 (0.45–0.87) | 0.0053 | 0.65 (0.46–0.90) | 0.0097 | 0.57 (0.41–0.77) | 0.0004 | 0.58 (0.42–0.80) | 0.0009 |
| Site | ||||||||
| Tongue | 0.86 (0.56–1.33) | 0.5097 | 0.95 (0.61–1.49) | 0.8288 | 0.65 (0.44–0.97) | 0.0337 | 0.72 (0.48–1.09) | 0.1194 |
| Other | 0.68 (0.46–1.00) | 0.0491 | 0.62 (0.41–0.93) | 0.0195 | 0.66 (0.45–0.97) | 0.0328 | 0.61 (0.41–0.91) | 0.0158 |
| Variation | Crude HR (95% C.I) | p Value | Adjusted HR (95% C.I) | p Value |
|---|---|---|---|---|
| All | ||||
| RT | 0.29 (0.18–0.49) | <0.0001 | 0.30 (0.18–0.51) | <0.0001 |
| Age, ≥65 | 1.89 (1.03–3.50) | 0.0415 | 1.63 (0.86–3.10) | 0.1333 |
| Male | 1.58 (0.57–4.35) | 0.3788 | 1.86 (0.66–5.22) | 0.2371 |
| pT2 | 0.97 (0.56–1.65) | 0.8968 | 1.10 (0.65–1.90) | 0.7291 |
| Grade (Well/moderately) | 0.80 (0.41–1.59) | 0.5282 | 0.88 (0.44–1.77) | 0.7262 |
| CCI group | ||||
| 0 | Ref. | Ref. | ||
| 1 | 1.25 (0.64–2.43) | 0.5159 | 1.08 (0.55–2.13) | 0.8297 |
| ≥2 | 1.59 (0.75–3.40) | 0.2281 | 1.40 (0.64–3.04) | 0.3962 |
| Hospital level, medical center | 1.48 (0.78–2.78) | 0.2283 | 1.40 (0.74–2.66) | 0.3010 |
| Site | ||||
| Tongue | 1.89 (1.12–3.19) | 0.0176 | 2.10 (1.23–3.58) | 0.0066 |
| Other | Ref. | Ref. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsai, C.-J.; Kuo, Y.-H.; Wu, H.-C.; Ho, C.-H.; Chen, Y.-C.; Yang, C.-C. Adjuvant Radiotherapy Significantly Increases Neck Control and Survival in Early Oral Cancer Patients with Solitary Nodal Involvement: A National Cancer Registry Database Analysis. Cancers 2021, 13, 3742. https://doi.org/10.3390/cancers13153742
Tsai C-J, Kuo Y-H, Wu H-C, Ho C-H, Chen Y-C, Yang C-C. Adjuvant Radiotherapy Significantly Increases Neck Control and Survival in Early Oral Cancer Patients with Solitary Nodal Involvement: A National Cancer Registry Database Analysis. Cancers. 2021; 13(15):3742. https://doi.org/10.3390/cancers13153742
Chicago/Turabian StyleTsai, Chia-Jen, Yu-Hsuan Kuo, Hung-Chang Wu, Chung-Han Ho, Yi-Chen Chen, and Ching-Chieh Yang. 2021. "Adjuvant Radiotherapy Significantly Increases Neck Control and Survival in Early Oral Cancer Patients with Solitary Nodal Involvement: A National Cancer Registry Database Analysis" Cancers 13, no. 15: 3742. https://doi.org/10.3390/cancers13153742