
Treatment and Survival of Malignant Extracranial Germ Cell Tumours in the Paediatric Population: A Systematic Review and Meta-Analysis

 , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Results
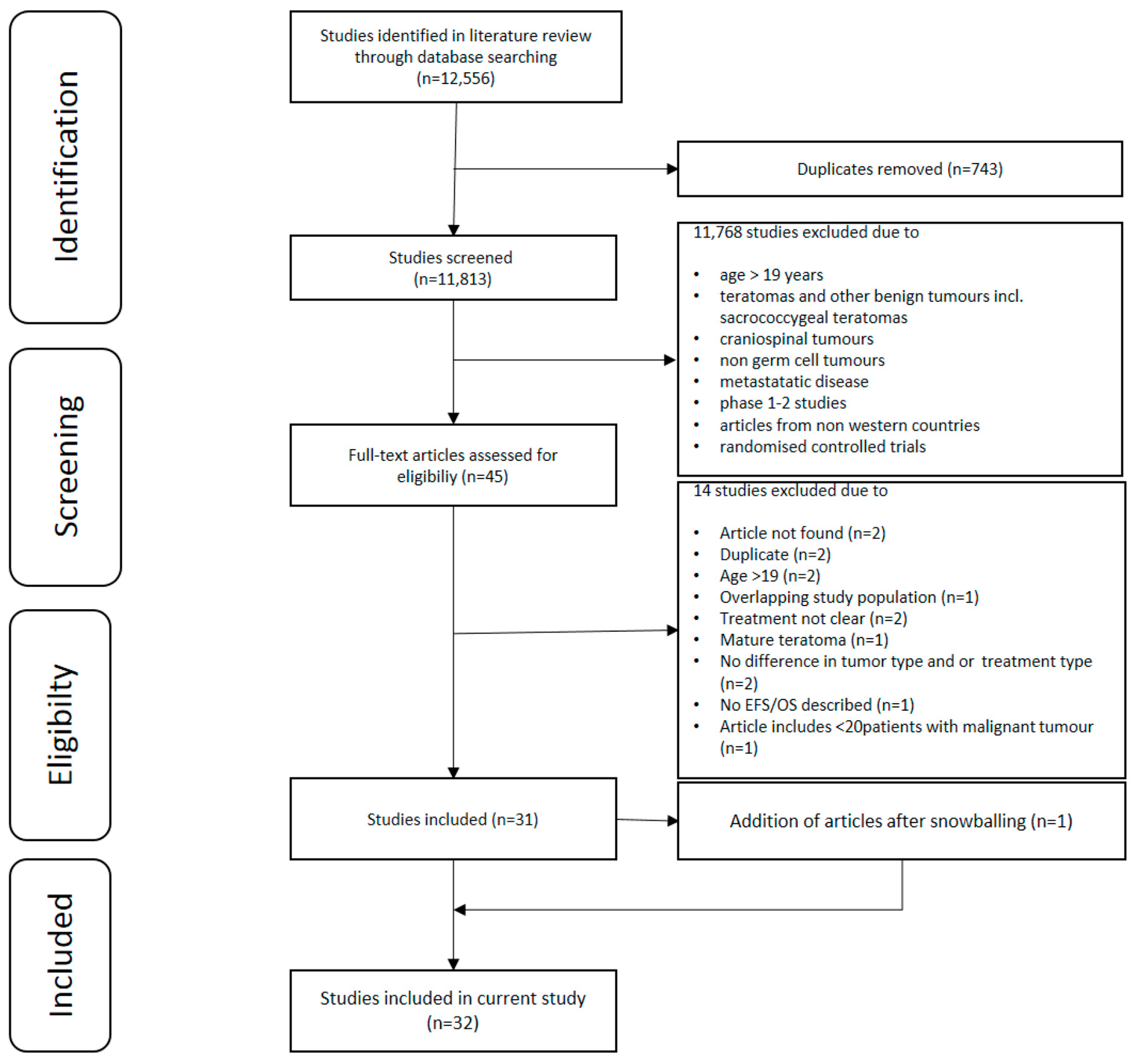
2.1. Search Outcomes
2.2. Overview of Studies
3. Overall Survival Data
3.1. Anatomical Locations
3.2. Age
3.3. Serum Tumour Markers
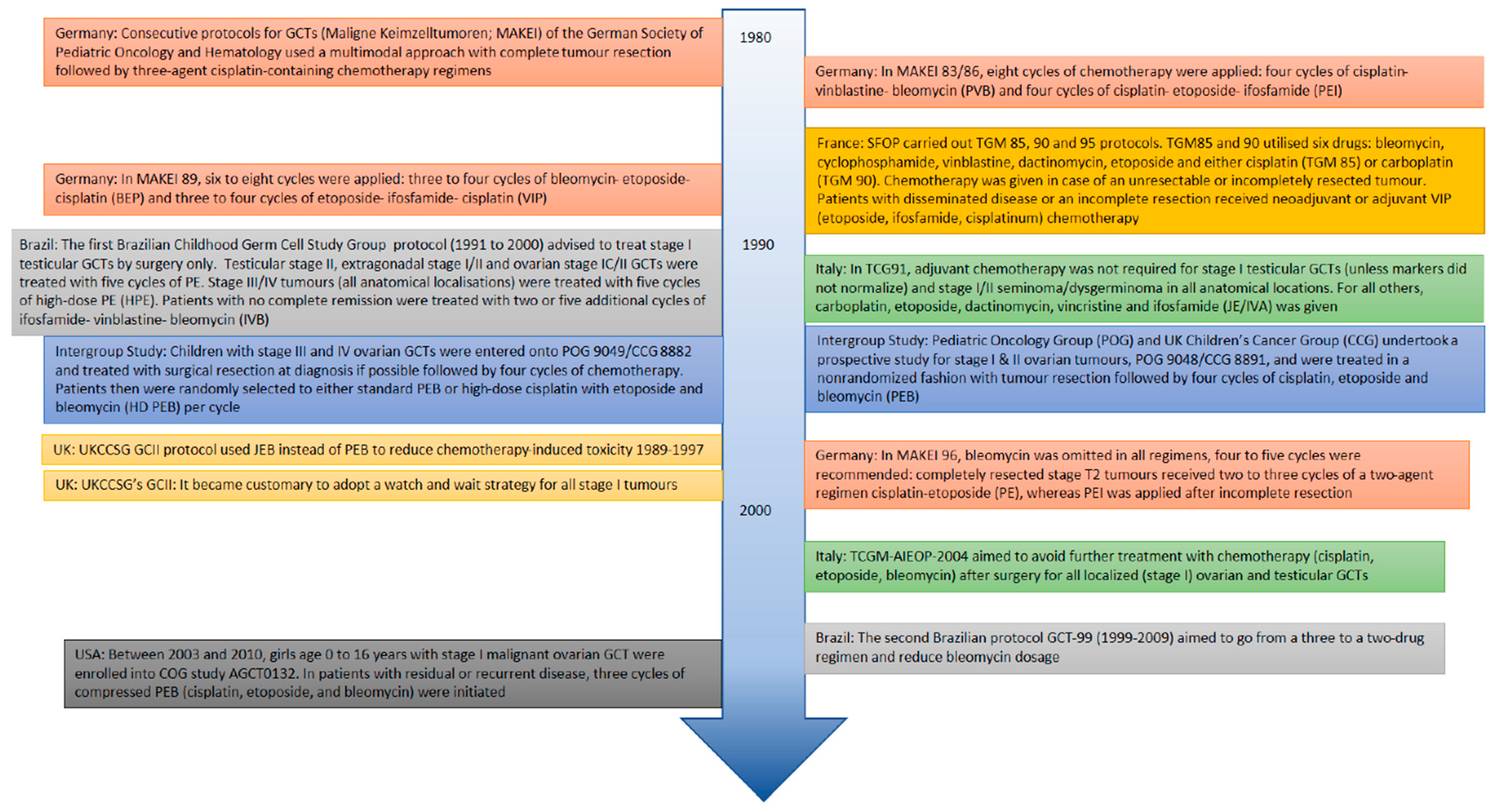
3.4. Chemotherapy Regimens
3.5. Stage
4. Individual Anatomical Localisations
4.1. Study Characteristics
4.2. Clinical Presentation
4.3. Staging
4.4. Histopathology
4.5. Treatment
4.6. Survival
5. Testis
5.1. Study Characteristics
5.2. Clinical Presentation
5.3. Staging
5.4. Histopathology
5.5. Treatment
5.6. Survival
6. Mediastinum
6.1. Study Characteristics
6.2. Clinical Presentation
6.3. Staging
6.4. Histopathology
6.5. Treatment
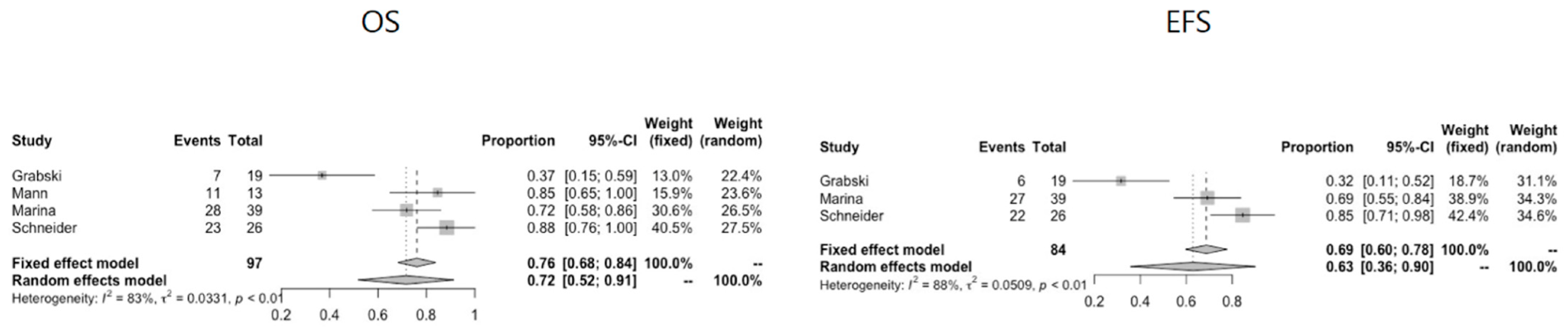
6.6. Survival
7. Sacrococcygeal
7.1. Study Characteristics
7.2. Clinical Presentation
7.3. Staging
7.4. Histopathology
7.5. Treatment
7.6. Survival
8. Discussion
9. Materials and Methods
9.1. Search Strategy
9.2. Study Selection
9.3. Data Extraction and Analysis
9.4. Statistical Analysis
10. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Murray, M.J.; Nicholson, J.C. Germ cell tumours in children and adolescents. Paediatr. Child Health 2010, 20, 109–116. [Google Scholar] [CrossRef]
- Shaikh, F.; Murray, M.J.; Amatruda, J.F.; Coleman, N.; Nicholson, J.C.; Hale, J.P.; Pashankar, F.; Stoneham, S.J.; Poynter, J.N.; Olson, T.A.; et al. Paediatric extracranial germ-cell tumours. Lancet Oncol. 2016, 17, e149–e162. [Google Scholar] [CrossRef] [Green Version]
- Kops, A.L.; Hulsker, C.C.; Fiocco, M.; Zsiros, J.; Mavinkurve-Groothuis, A.M.C.; Looijenga, L.H.; van der Steeg, A.F.; Wijnen, M.H. Malignant Recurrence after Mature Sacrococcygeal Teratoma: A Meta-Analysis and Review of the Literature. Crit. Rev. Oncol. Hematol. 2020, 103140. [Google Scholar] [CrossRef] [PubMed]
- Seydoux, G.; Braun, R.E. Pathway to Totipotency: Lessons from Germ Cells. Cell 2006. [Google Scholar] [CrossRef] [PubMed]
- De Felici, M.; Klinger, F.G.; Campolo, F.; Balistreri, C.R.; Barchi, M.; Dolci, S. To Be or Not to Be a Germ Cell: The Extragonadal Germ Cell Tumor Paradigm. Int. J. Mol. Sci. 2021, 22, 5982. [Google Scholar] [CrossRef] [PubMed]
- Zambrano, E.; De Stefano, D.V.; Reyes-Múgica, M. Pediatric germ cell tumors. In Pathology and Biology of Human Germ Cell Tumors; Springer: Berlin/Heidelberg, Germany, 2017; pp. 381–395. ISBN 9783662537756. [Google Scholar]
- Fonseca, A.; Frazier, A.L.; Shaikh, F. Germ Cell Tumors in Adolescents and Young Adults. J. Oncol. Pract. 2019, 15. [Google Scholar] [CrossRef] [PubMed]
- Calaminus, G.; Schneider, D.T.; von Schweinitz, D.; Jürgens, H.; Infed, N.; Schönberger, S.; Olson, T.A.; Albers, P.; Vokuhl, C.; Stein, R.; et al. Age-Dependent Presentation and Clinical Course of 1465 Patients Aged 0 to Less than 18 Years with Ovarian or Testicular Germ Cell Tumors; Data of the MAKEI 96 Protocol Revisited in the Light of Prenatal Germ Cell Biology. Cancers 2020, 12, 611. [Google Scholar] [CrossRef] [Green Version]
- Kaatsch, P.; Häfner, C.; Calaminus, G.; Blettner, M.; Tulla, M. Pediatric germ cell tumors from 1987 to 2011: Incidence rates, time trends, and survival. Pediatrics 2015, 135, e136–e143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kramarova, E.; Mann, J.; Magnani, C.; Corraziari, I.; Berrino, F. EUROCARE Working Group: Survival of children with malignant germ cell, trophoblastic and other gonadal tumours in Europe. Eur. J. Cancer 2001, 37, 750–759. [Google Scholar] [CrossRef]
- Billmire, D.F.; Cullen, J.W.; Rescorla, F.J.; Davis, M.; Schlatter, M.G.; Olson, T.A.; Malogolowkin, M.H.; Pashankar, F.; Villaluna, D.; Krailo, M.; et al. Surveillance after initial surgery for pediatric and adolescent girls with stage I ovarian germ cell tumors: Report from the children’s oncology group. J. Clin. Oncol. 2014, 32, 465–470. [Google Scholar] [CrossRef] [Green Version]
- Rescorla, F.J.; Ross, J.H.; Billmire, D.F.; Dicken, B.J.; Villaluna, D.; Davis, M.M.; Krailo, M.; Cullen, J.W.; Olson, T.A.; Egler, R.A.; et al. Surveillance after initial surgery for Stage I pediatric and adolescent boys with malignant testicular germ cell tumors: Report from the Children’s Oncology Group. J. Pediatr. Surg. 2015, 50, 1000–1003. [Google Scholar] [CrossRef] [PubMed]
- Schlatter, M.; Rescorla, F.; Giller, R.; Cushing, B.; Vinocur, C.; Colombani, P.; Cullen, J.; London, W.; Davis, M.; Lauer, S.; et al. Excellent outcome in patients with stage I germ cell tumors of the testes: A study of the Children’s Cancer Group/Pediatric Oncology Group. J. Pediatr. Surg. 2003, 38, 319–324. [Google Scholar] [CrossRef]
- Taskinen, S.; Fagerholm, R.; Lohi, J.; Taskinen, M. Pediatric ovarian neoplastic tumors: Incidence, age at presentation, tumor markers and outcome. Acta Obstet. Gynecol. Scand. 2015, 94, 425–429. [Google Scholar] [CrossRef] [PubMed]
- Frazier, A.L.; Hale, J.P.; Rodriguez-Galindo, C.; Dang, H.; Olson, T.; Murray, M.J.; Amatruda, J.F.; Thornton, C.; Arul, G.S.; Billmire, D.; et al. Revised Risk classification for pediatric extracranial germ cell tumors based on 25 years of clinical trial data from the United Kingdom and United States. J. Clin. Oncol. 2015, 33, 195–201. [Google Scholar] [CrossRef] [PubMed]
- Billmire, D.; Vinocur, C.; Rescorla, F.; Colombani, P.; Cushing, B.; Hawkins, E.; Davis, M.; London, W.B.; Lauer, S.; Giller, R.; et al. Malignant retroperitoneal and abdominal germ cell tumors: An intergroup study. J. Pediatr. Surg. 2003, 38, 315–318. [Google Scholar] [CrossRef]
- Goebel, U.; Calaminus, G.; Schneider, D.T.; Schmidt, P.; Haas, R.J. Management of germ cell tumors in children: Approaches to cure. Onkologie 2002, 25, 14–22. [Google Scholar] [CrossRef] [Green Version]
- Vaysse, C.; Delsol, M.; Carfagna, L.; Bouali, O.; Combelles, S.; Lemasson, F.; Le Mandat, A.; Castex, M.P.; Pasquet, M.; Moscovici, J.; et al. Ovarian germ cell tumors in children. Management, survival and ovarian prognosis. A report of 75 cases. J. Pediatr. Surg. 2010, 45, 1484–1490. [Google Scholar] [CrossRef]
- Schneider, D.T.; Calaminus, G.; Reinhard, H.; Gutjahr, P.; Kremens, B.; Harms, D.; Göbel, U. Primary Mediastinal Germ Cell Tumors in Children and Adolescents: Results of the German Cooperative Protocols MAKEI 83/86, 89, and 96. J. Clin. Oncol. 2000, 18, 832–839. [Google Scholar] [CrossRef]
- Schneider, D.T.; Calaminus, G.; Wessalowksi, R.; Pathmanathan, R.; Selle, B.; Sternschulte, W.; Harms, D.; Göbel, U. Ovarian sex cord-stromal tumors in children and adolescents. J. Clin. Oncol. 2003, 21, 2357–2363. [Google Scholar] [CrossRef]
- Baranzelli, M.C.; Bouffet, E.; Quintana, E.; Portas, M.; Thyss, A.; Patte, C. Non-seminomatous ovarian germ cell tumours in children. Eur. J. Cancer 2000, 36, 376–383. Available online: www.elsevier.com/locate/ejconline (accessed on 16 July 2021). [CrossRef]
- Duhil de Bénazé, G.; Pacquement, H.; Faure-Conter, C.; Patte, C.; Orbach, D.; Corradini, N.; Berger, C.; Sudour-Bonnange, H.; Vérité, C.; Martelli, H.; et al. Paediatric dysgerminoma: Results of three consecutive French germ cell tumours clinical studies (TGM-85/90/95) with late effects study. Eur. J. Cancer 2018, 91, 30–37. [Google Scholar] [CrossRef]
- Fresneau, B.; Orbach, D.; Faure-Conter, C.; Verité, C.; Castex, M.P.; Kalfa, N.; Martelli, H.; Patte, C. Sex-Cord Stromal Tumors in Children and Teenagers: Results of the TGM-95 Study. Pediatr. Blood Cancer 2015, 62, 2114–2119. [Google Scholar] [CrossRef]
- Terenziani, M.; Bisogno, G.; Boldrini, R.; Cecchetto, G.; Conte, M.; Boschetti, L.; De Pasquale, M.D.; Biasoni, D.; Inserra, A.; Siracusa, F.; et al. Malignant ovarian germ cell tumors in pediatric patients: The AIEOP (Associazione Italiana Ematologia Oncologia Pediatrica) study. Pediatr. Blood Cancer 2017, 64. [Google Scholar] [CrossRef] [Green Version]
- Terenziani, M.; De Pasquale, M.D.; Bisogno, G.; Biasoni, D.; Boldrini, R.; Collini, P.; Conte, M.; Dall’Igna, P.; Inserra, A.; Melchionda, F.; et al. Malignant testicular germ cell tumors in children and adolescents: The AIEOP (Associazione Italiana Ematologia Oncologia Pediatrica) protocol. Urol. Oncol. Semin. Orig. Investig. 2018, 36, 502.e7–502.e13. [Google Scholar] [CrossRef] [PubMed]
- Curto, M.L.; Lumia, F.; Alaggio, R.; Cecchetto, G.; Almasio, P.; Indolfi, P.; Siracusa, F.; Bagnulo, S.; De Bernardi, B.; De Laurentis, T.; et al. Malignant germ cell tumors in childhood: Results of the first Italian cooperative study “TCG 91”. Med. Pediatr. Oncol. 2003, 41, 417–425. [Google Scholar] [CrossRef]
- Lopes, L.F.; Sonaglio, V.; Ribeiro, K.C.B.; Schneider, D.T.; De Camargo, B. Improvement in the outcome of children with germ cell tumors. Pediatr. Blood Cancer 2008, 50, 250–253. [Google Scholar] [CrossRef] [PubMed]
- Lopes, L.F.; Macedo, C.R.P.; Pontes, E.M.; Aguiar, S.D.S.; Mastellaro, M.J.; Melaragno, R.; Vianna, S.M.R.; Lopes, P.A.A.; Mendonça, N.; De Almeida, M.T.A.; et al. Cisplatin and etoposide in childhood germ cell tumor: Brazilian pediatric oncology society protocol GCT-91. J. Clin. Oncol. 2009, 27, 1297–1303. [Google Scholar] [CrossRef] [PubMed]
- Lopes, L.F.; Macedo, C.R.P.D.; Dos Santos Aguiar, S.; Barreto, J.H.S.; Martins, G.E.; Sonaglio, V.; Milone, M.; Lima, E.R.; De Assis Almeida, M.T.; Lopes, P.M.A.A.; et al. Lowered cisplatin dose and no bleomycin in the treatment of pediatric germ cell tumors: Results of the GCT-99 protocol from the brazilian germ cell pediatric oncology cooperative group. J. Clin. Oncol. 2016, 34, 603–610. [Google Scholar] [CrossRef]
- Billmire, D.F.; Vinocur, C.; Rescorla, F.; Cushing, B.; London, W.; Schlatter, M.; Davis, M.; Giller, R.; Lauer, S.; Olson, T.; et al. Outcome and Staging Evaluation in Malignant Germ Cell Tumors of the Ovary in Children and Adolescents: An Intergroup Study. J. Pediatric Surg. 2004, 39, 424–429. [Google Scholar] [CrossRef]
- Rogers, P.C.; Olson, T.A.; Cullen, J.W.; Billmire, D.F.; Marina, N.; Rescorla, F.; Davis, M.M.; London, W.B.; Latter, S.J.; Giller, R.H.; et al. Treatment of children and adolescents with stage II testicular and stages I and II ovarian malignant germ cell tumors: A Pediatric Intergroup study-Pediatric Oncology Group 9048 and Children’s Cancer Group 8891. J. Clin. Oncol. 2004, 22, 3563–3569. [Google Scholar] [CrossRef]
- Marina, N.; London, W.B.; Frazier, A.L.; Lauer, S.; Rescorla, F.; Cushing, B.; Malogolowkin, M.H.; Castleberry, R.P.; Womer, R.B.; Olson, T. Prognostic factors in children with extragonadal malignant germ cell tumors: A pediatric intergroup study. J. Clin. Oncol. 2006, 24, 2544–2548. [Google Scholar] [CrossRef] [PubMed]
- Mann, J.R.; Raafat, F.; Robinson, K.; Imeson, J.; Gornall, P.; Sokal, M.; Gray, E.; Mckeever, P.; Hale, J.; Bailey, S.; et al. The United Kingdom Children’s Cancer Study Group’s Second Germ Cell Tumor Study: Carboplatin, Etoposide, and Bleomycin Are Effective Treatment for Children With Malignant Extracranial Germ Cell Tumors, With Acceptable Toxicity. J. Clin. Oncol. 2000, 18, 3809–3818. [Google Scholar] [CrossRef] [PubMed]
- Akyüz, C.; Varan, A.; Büyükpamukçu, N.; Kutluk, T.; Büyükpamukçu, M. Malignant Ovarian Tumors in Children: 22 Years of Experience at a Single Institution. J. Pediatr. Hematol. Oncol. 2000, 22, 422–427. [Google Scholar] [CrossRef] [PubMed]
- Amini, A.; Waxweiler, T.V.; Maroni, P.D.; Kessler, E.R.; Cost, C.R.; Greffe, B.S.; Garrington, T.P.; Liu, A.K.; Cost, N.G. Survival outcomes of adolescent and adult patients with non-seminomatous testicular germ-cell tumors: A population-based study. J. Pediatr. Urol. 2016, 12, 405.e1–405.e9. [Google Scholar] [CrossRef] [PubMed]
- Andrés, M.D.M.; Costa, E.; Cañete, A.; Moreno, L.; Castel, V. Solid ovarian tumours in childhood: A 35-year review in a single institution. Clin. Transl. Oncol. 2010, 12, 287–291. [Google Scholar] [CrossRef] [PubMed]
- Frazier, A.L.; Stoneham, S.; Rodriguez-Galindo, C.; Dang, H.; Xia, C.; Olson, T.A.; Murray, M.J.; Amatruda, J.F.; Shaikh, F.; Pashankar, F.; et al. Comparison of carboplatin versus cisplatin in the treatment of paediatric extracranial malignant germ cell tumours: A report of the Malignant Germ Cell International Consortium. Eur. J. Cancer 2018, 98, 30–37. [Google Scholar] [CrossRef] [PubMed]
- Grabski, D.F.; Pappo, A.S.; Krasin, M.J.; Davidoff, A.M.; Rao, B.N.; Fernandez-Pineda, I. Long-term outcomes of pediatric and adolescent mediastinal germ cell tumors: A single pediatric oncology institutional experience. Pediatr. Surg. Int. 2017, 33, 235–244. [Google Scholar] [CrossRef]
- Güler, E.; Kutluk, M.T.; Büyükpamukçu, N.; Çaǧlar, M.; Varan, A.; Akyüz, C.; Büyükpamukçu, M. Testicular germ cell tumors in childhood: Treatment results of 52 patients. Pediatr. Hematol. Oncol. 2004, 21, 49–56. [Google Scholar] [CrossRef]
- Suita, S.; Shono, K.; Tajiri, T.; Takamatsu, T.; Mizote, H.; Nagasaki, A.; Inomata, Y.; Hara, T.; Okamura, J.; Miyazaki, S.; et al. Malignant germ cell tumors: Clinical characteristics, treatment, and outcome. A report from the study group for pediatric solid malignant tumors in the Kyushu area, Japan. J. Pediatr. Surg. 2002, 37, 1703–1706. [Google Scholar] [CrossRef]
- Terenziani, M.; Massimino, M.; Casanova, M.; Cefalo, G.; Ferrari, A.; Luksch, R.; Spreafico, F.; Polastri, D.; Fontanelli, R.; Piva, L.; et al. Childhood malignant ovarian germ cell tumors: A monoinstitutional experience. Gynecol. Oncol. 2001, 81, 436–440. [Google Scholar] [CrossRef]
- Terenziani, M.; Piva, L.; Spreafico, F.; Salvioni, R.; Massimino, M.; Luksch, R.; Cefalo, G.; Casanova, M.; Ferrari, A.; Polastri, D.; et al. Clinical Stage I Nonseminomatous Germ Cell Tumors of the Testis in Childhood and Adolescence: An Analysis of 31 Cases. J. Pediatr. Hematol. Oncol. 2002, 24, 454–458. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: Guidelines for reporting observational studies. Int. J. Surg. 2014, 12, 1495–1499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shaikh, F.; Cullen, J.W.; Olson, T.A.; Pashankar, F.; Malogolowkin, M.H.; Amatruda, J.F.; Villaluna, D.; Krailo, M.; Billmire, D.F.; Rescorla, F.J.; et al. Reduced and compressed cisplatin-based chemotherapy in children and adolescents with intermediate-risk extracranial malignant germ cell tumors: A report from the children’s oncology group. J. Clin. Oncol. 2017, 35, 1203–1210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stern, J.W.; Bunin, N. Prospective study of carboplatin-based chemotherapy for pediatric germ cell tumors. Med. Pediatr. Oncol. 2002, 39, 163–167. [Google Scholar] [CrossRef] [PubMed]
- Faure Conter, C.; Xia, C.; Gershenson, D.; Hurteau, J.; Covens, A.; Pashankar, F.; Krailo, M.; Billmire, D.; Patte, C.; Fresneau, B.; et al. Ovarian yolk sac tumors; does age matter? Int. J. Gynecol. Cancer 2018, 28, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Oosterhuis, J.W.; Looijenga, L.H.J. Testicular germ-cell tumours in a broader perspective. Nat. Rev. Cancer 2005, 5, 210–222. [Google Scholar] [CrossRef]
- Oosterhuis, J.W.; Looijenga, L.H.J. Human germ cell tumours from a developmental perspective. Nat. Rev. Cancer 2019, 19, 522–537. [Google Scholar] [CrossRef]
- Scully, R.E. A Gonadal Tumor Related to the Dysgerminoma (Seminoma) and Capable of Sex-Hormone Production. Cancer 1953, 6, 455–463. [Google Scholar] [CrossRef]
- Cools, M.; Stoop, H.; Kersemaekers, A.M.F.; Drop, S.L.S.; Wolffenbuttel, K.P.; Bourguignon, J.P.; Slowikowska-Hilczer, J.; Kula, K.; Faradz, S.M.H.; Oosterhuis, J.W.; et al. Gonadoblastoma arising in undifferentiated gonadal tissue within dysgenetic gonads. J. Clin. Endocrinol. Metab. 2006, 91, 2404–2413. [Google Scholar] [CrossRef] [Green Version]
- Cost, N.G.; Lubahn, J.D.; Adibi, M.; Romman, A.; Wickiser, J.E.; Raj, G.V.; Sagalowsky, A.I.; Margulis, V. A comparison of pediatric, adolescent, and adult testicular germ cell malignancy. Pediatr. Blood Cancer 2014, 61, 446–451. [Google Scholar] [CrossRef]
- Fox, E.P.; Loehrer, P.J. Chemotherapy for advanced testicular cancer. Hematol. Oncol. Clin. N. Am. 1991, 5, 1173–1187. [Google Scholar] [CrossRef]
- Kapoor, G.; Advani, S.H.; Nair, C.N.; Pai, K.; Kurkure, P.A.; Nair, R.; Saikia, T.K.; Vege, D.; Desai, P.B. Pediatric Germ Cell Tumor; an experience with BEP. J. Pediatr. Hematol. Oncol. 1995, 17, 318–324. [Google Scholar] [CrossRef]
- Einhorn, L.H.; Donohue, J.P. Improved chemotherapy in disseminated testicular cancer. J. Urol. 1977, 117, 65–69. [Google Scholar] [CrossRef]
- Cheng, L.; Albers, P.; Berney, D.M.; Feldman, D.R.; Daugaard, G.; Gilligan, T.; Looijenga, L.H.J. Testicular cancer. Nat. Rev. Dis. Prim. 2018, 4. [Google Scholar] [CrossRef] [PubMed]
- Schneider, D.T.; Schuster, A.E.; Fritsch, M.K.; Calaminus, G.; Göbel, U.; Harms, D.; Lauer, S.; Olson, T.; Perlman, E.J. Genetic analysis of mediastinal nonseminomatous germ cell tumors in children and adolescents. Genes Chromosom. Cancer 2002, 34, 115–125. [Google Scholar] [CrossRef] [PubMed]
- Oosterhuis, J.W.; Looijenga, L.H.J. Mediastinal germ cell tumors: Many questions and perhaps an answer. J. Clin. Investig. 2020, 130, 6238–6241. [Google Scholar] [CrossRef] [PubMed]
- Taylor, J.; Donoghue, M.T.A.; Ho, C.; Petrova-Drus, K.; Al-Ahmadie, H.A.; Funt, S.A.; Zhang, Y.; Aypar, U.; Rao, P.; Chavan, S.S.; et al. Germ cell tumors and associated hematologic malignancies evolve from a common shared precursor. J. Clin. Investig. 2020, 130, 6668–6676. [Google Scholar] [CrossRef] [PubMed]
- Bagrodia, A.; Lee, B.H.; Lee, W.; Cha, E.K.; Sfakianos, J.P.; Iyer, G.; Pietzak, E.J.; Gao, S.P.; Zabor, E.C.; Ostrovnaya, I.; et al. Genetic determinants of cisplatin resistance in patients with advanced germ cell tumors. J. Clin. Oncol. 2016, 34, 4000–4007. [Google Scholar] [CrossRef]
- Dieckmann, K.P.; Richter-Simonsen, H.; Kulejewski, M.; Ikogho, R.; Zecha, H.; Anheuser, P.; Pichlmeier, U.; Isbarn, H. Testicular germ-cell tumours: A descriptive analysis of clinical characteristics at first presentation. Urol. Int. 2018, 100, 409–419. [Google Scholar] [CrossRef]
- Escudero-Ávila, R.; Rodríguez-Castaño, J.D.; Osman, I.; Fernandez, F.; Medina, R.; Vargas, B.; Japón-Rodríguez, M.; Sancho, P.; Perez-Valderrama, B.; Praena-Fernández, J.M.; et al. Active surveillance as a successful management strategy for patients with clinical stage I germ cell testicular cancer. Clin. Transl. Oncol. 2019, 21, 796–804. [Google Scholar] [CrossRef]
- Lobo, J.; Gillis, A.J.M.; Jerónimo, C.; Henrique, R.; Looijenga, L.H.J. Human germ cell tumors are developmental cancers: Impact of epigenetics on pathobiology and clinic. Int. J. Mol. Sci. 2019, 20, 258. [Google Scholar] [CrossRef] [Green Version]
- Gross, N.; Kropp, J.; Khatib, H. MicroRNA signaling in embryo development. Biology 2017, 6, 34. [Google Scholar] [CrossRef]
- Nappi, L.; Nichols, C. MicroRNAs as Biomarkers for Germ Cell Tumors. Urol. Clin. N. Am. 2019, 46, 449–457. [Google Scholar] [CrossRef] [PubMed]
- Singla, N.; Lafin, J.T.; Bagrodia, A. MicroRNAs: Turning the Tide in Testicular Cancer. Eur. Urol. 2019, 76, 541–542. [Google Scholar] [CrossRef]
- Murray, M.J.; Coleman, N. Can circulating microRNAs solve clinical dilemmas in testicular germ cell malignancy? Nat. Rev. Urol. 2019, 16, 505–506. [Google Scholar] [CrossRef] [PubMed]
- Almstrup, K.; Mamp, N.; Belge, G.; Rajpert-De Meyts, E.; Looijenga, L.H.J.; Dieckmann, K.-P. Application of miRNAs in the diagnosis and monitoring of testicular germ cell tumours. Nat. Rev. Urol. 2020, 17, 201–213. [Google Scholar] [CrossRef]
- Lobo, J.; Leão, R.; Gillis, A.J.M.; van den Berg, A.; Anson-Cartwright, L.; Atenafu, E.G.; Kuhathaas, K.; Chung, P.; Hansen, A.; Bedard, P.L.; et al. Utility of Serum miR-371a-3p in Predicting Relapse on Surveillance in Patients with Clinical Stage I Testicular Germ Cell Cancer. Eur. Urol. Oncol. 2020. [Google Scholar] [CrossRef]
- Murray, M.J.; Coleman, N. MicroRNA dysregulation in malignant germ cell tumors: More than a biomarker? J. Clin. Oncol. 2019, 37, 1432–1435. [Google Scholar] [CrossRef]
- Lobo, J.; Gillis, A.J.M.; van den Berg, A.; Dorssers, L.C.J.; Belge, G.; Dieckmann, K.P.; Roest, H.P.; van der Laan, L.J.W.; Gietema, J.; Hamilton, R.J.; et al. Identification and Validation Model for Informative Liquid Biopsy-Based microRNA Biomarkers: Insights from Germ Cell Tumor In Vitro, In Vivo and Patient-Derived Data. Cells 2019, 8, 1637. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Altman, D.; Antes, G.; Atkins, D.; Barbour, V.; Barrowman, N.; Berlin, J.A.; et al. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | n | Location | Hist | Stage | Treatment Protocol/Chemotherapy Regimens | EFS (%) | OS (%) |
|---|---|---|---|---|---|---|---|
| Akyuz 2000 | 56 | O | GCT | I (34%) II (27%) III (34%) IV (5%) | <’86 VAC ‘86–‘89 PVB ‘89–’97 BEP | 57 | 68 overall. By stage: I = 82, II = 79, III = 50, IV = 33 |
| Andres 2010 | 53 | O | GCT | I (63%) II (4%) III (29%) IV (4%) | Unclear | 94 | 97 |
| Baranzelli 2000 | 63 | O | GCT | I (2%) II (43%) III (49%) IV (6%) | TGM85 & TGM90 | 74 | 85 |
| Billmire 2004 | 131 | O | GCT | I (32%) II (12%) III (44%) IV (12%) | POG/CCG intergroup study BEP vs. HDBEP | No overall data. By stage: I = 95, II = 88, III = 97, IV = 87 | No overall data. By stage: I = 95, II = 94, III = 97, IV = 93 |
| Billmire 2014 | 25 | O | GCT | Study on stage I disease only | COG AGCT0132 | 52 | 96 |
| Lo Curto 2003 | 23 | M | GCT | I (44%) II (4%) III (48%) IV (4%) | TCG91 | 81 | 88 |
| Duhil du Benaze 2018 | 48 | O | DYS | NM | TGM85 & TGM90 & TGM95 | 91 | 100 |
| Faure Conter 2017 | 217 | O | GCT | II/III (90%) IV (10%) | Protocols of 8 different trials COG/CCLG/SFCE | 91 overall. By stage: II/III = 91, IV = 88 | 96 overall. By stage: II/III = 97, IV = 91 |
| Frazier 2018 | 278 | M | GCT | NM | PEB and JEB | PEB 90, JEB 85 | NM |
| Fresneau 2015 | 38 | OT | SCST | I (61%) III (39%) | TGM95 | 85 | 94 |
| Lopes 2008 | 37 | M | GCT | NM | ’83–’86 VAB-6 ’87–’91 EPO-VAC ’91–’97 TCG91 | 51 | 73 |
| Lopes 2009 | 45 | M | GCT | NM | GCT91 | NM | NM |
| Lopes 2016 | 206 | M | GCT | NM | GCT99 | 91 | 92 |
| Mann 2000 | 54 | M | GCT | I (35%) II (17%) III (41%) IV (7%) | UK GC II | 91 | 92 |
| Rogers 2004 | 57 | OT | GCT | I (72%) II (28%) | POG9048-CCG8891 | 93 overall. By stage: I = 95, II = 88 | 94 overall. By stage: I = 95, II = 94 |
| Schneider 2003 | 54 | O | SCST | I (88%) II (6%) III (6%) | MAKEI ‘83/86, ’89,’96 | 86 overall. By FIGO stage: Ia = 100, Ic = 76, II/III = 67 | 89 |
| Shaikh 2017 | 124 | M | GCT | NM | AGCT0132 | 3 cycles PEB = 88, 4 cycles PEB = 92 | NM |
| Stern 2002 | 6 | M | GCT | NM | JEB | NM | NM |
| Suita 2002 | 31 | M | GCT | NM | Unclear | NM | 87 |
| Terenziani 2001 | 29 | O | GCT | I (33%) II 15%) III (41%) IV (11%) | <‘80 VAC ’80-’87 PVB >’88 PEB | 82 | 82 |
| Terenziani 2017 | 77 | O | GCT | I (35%) II (17%) III (42%) IV (6%) | TCGM-AIEOP2004 | 85 overall | 99 overall |
| T = 1652 | By stage: I = 72, II–IV = 91 Dysgerminoma = 87 | Stage I = 100, II–IV = 98 Dysgerminoma = 100 |
| Study | n | Location | Hist | Stage | Treatment Protocol/Chemotherapy Regimens | EFS (%) | OS (%) |
|---|---|---|---|---|---|---|---|
| Amini 2016 | 1496 | T | GCT | I (57%) II/III (22%) IV (21%) | Unclear | NM | 94 |
| Cost 2014 | 59 | T | GCT | I (48%) II (23%) III (29%) | Unclear | 87 ped 60 adolescents | 100 ped 85 adol. |
| Lo Curto 2003 | 36 | M | GCT | I (73%) II (8%) III (11%) IV (8%) | TCG91 | 85 | 100 |
| Frazier 2018 | 163 | M | GCT | NM | PEB and JEB | PEB 85 JEB 100 | NM |
| Fresneau 2015 | 11 | OT | SCST | I (100%) | TGM95 | 100 | 100 |
| Guler 2003 | 52 | T | GCT | I (60%) II (15%) III (15%) IV (10%) | BEP, VAC, Vinbl&Bleo | NM | Overall 71. BEP 86, VAC 68, Vinbl&Bleo 64. Histology YST 74, Embryon.carc 64 |
| Lopes 2008 | 35 | M | GCT | NM | ’83–’86 VAB-6 ’87–’91 EPO-VAC ’91–’97 TCG91 | 50 | 73 |
| Lopes 2009 | 22 | M | GCT | NM | GCT91 | NM | NM |
| Lopes 2016 | 126 | M | GCT | NM | GCT99 | 83 | 88 |
| Mann 2000 | 63 | M | GCT | I (72%) II (13%) IV (15%) | GC II (JEB) | 100 | 100 |
| Rescorla 2015 | 80 | T | GCT | Study on stage I disease only | COG AGCT0132 | 74 | 100 overall. Age < 11 yrs 80 Age > 11 yrs 48. Histology pure YST 81, mixed GCT 81 |
| Rogers 2004 | 17 | OT | GCT | II (100%) | POG9048-CCG8891 | 100 | 100 |
| Schlatter 2003 | 63 | T | GCT | Study on stage I disease only | POG9048-CCG8891 | 79 | 100 |
| Shaikh 2017 | 47 | M | GCT | NM | COG AGCT0132 | 3 cycles PEB = 83 4 cycles PEB = 95 | NM |
| Stern 2002 | 4 | M | GCT | NM | JEB | NM | NM |
| Suita 2002 | 52 | M | GCT | NM | Unclear | NM | 93 |
| Terenziani 2002 | 31 | T | GCT | Study on stage I disease only | Surveillance (PEB/PVB for relapse/adolescents) | 81 | 100 |
| Terenziani 2018 | 99 | T | GCT | I (59%) II (7%) III (14%) IV (20%) | TCGM-AIEOP2004 | 73 overall. By stage: I = 65, II = 100, III = 85, IV = 82 | 99 overall. By stage: I-III = 100, IV = 94 |
| T = 2456 |
| Study | N (M:F) | Location | Hist | Stage | Treatment Protocol/Chemotherapy Regimens | EFS (%) | OS (%) |
|---|---|---|---|---|---|---|---|
| Lo Curto 2003 | 2 (?) | M | GCT | NM | TCG91 | NM | NM |
| Frazier 2018 | 69 (?) | M | GCT | NM | PEB and JEB | PEB 77 JEB 77 | NM |
| Grabski 2016 | 19 (15:4) | Med | GCT | I (53%) IV (47%) | Unclear | 29 | 39 |
| Mann 2000 | 13 (?) | M | GCT | I (15%) II (23%) III (23%) IV (39%) | UK GC II | 75 | 83 |
| Marina 2006 | 39 (?) | M | GCT | NM | POG 9049/CCG 8882 | 69 | 71 |
| Schneider 2000 | 26 (?) | Med | GCT | NM | MAKEI ‘83/86, ‘89, ‘96 | 83 overall. By completeness of surgery: incomplete surgical resection 42. Complete resection 94 | 87 overall. By completeness of surgery: incomplete surgical resection 42. Complete resection 100 |
| T = 168 |
| Study | n | Location | Hist | Stage | Treatment Protocol/Chemotherapy Regimens | EFS (%) | OS (%) |
|---|---|---|---|---|---|---|---|
| Lo Curto 2003 | 30 | M | GCT | I (10%) II (3%) III (57%) IV (30%) | TCG91 | 59 | 70 |
| Frazier 2018 | 169 | M | GCT | NM | PEB and JEB | PEB88 JEB86 | NM |
| Lopes 2008 | 22 | M | GCT | NM | ’83-’86 VAB-6 ’87-’91 EPO-VAC ’91-’97 TCG91 | 27 | 55 |
| Lopes 2009 | 24 | M | GCT | NM | GCT91 | NM | NM |
| Lopes 2016 | 73 | M | GCT | NM | GCT99 | 77 | 81 |
| Mann 2000 | 37 | M | GCT | I (5%) II (31%) III (17%) IV (47%) | UK GC II | 87 | 88 |
| Marina 2006 | 88 | M | GCT | NM | POG9048-CCG8891 | NM | NM |
| Stern 2002 | 9 | M | GCT | NM | JEB | NM | NM |
| Suita 2002 | 21 | M | GCT | NM | Unclear | NM | 57 |
| T = 473 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hulsker, C.C.C.; el Mansori, I.; Fiocco, M.; Zsiros, J.; Wijnen, M.H.W.; Looijenga, L.H.J.; Mavinkurve-Groothuis, A.M.C.; van der Steeg, A.F.W. Treatment and Survival of Malignant Extracranial Germ Cell Tumours in the Paediatric Population: A Systematic Review and Meta-Analysis. Cancers 2021, 13, 3561. https://doi.org/10.3390/cancers13143561
Hulsker CCC, el Mansori I, Fiocco M, Zsiros J, Wijnen MHW, Looijenga LHJ, Mavinkurve-Groothuis AMC, van der Steeg AFW. Treatment and Survival of Malignant Extracranial Germ Cell Tumours in the Paediatric Population: A Systematic Review and Meta-Analysis. Cancers. 2021; 13(14):3561. https://doi.org/10.3390/cancers13143561
Chicago/Turabian StyleHulsker, Caroline C. C., Issam el Mansori, Marta Fiocco, József Zsiros, Marc H. W. Wijnen, Leendert H. J. Looijenga, Annelies M. C. Mavinkurve-Groothuis, and Alida F. W. van der Steeg. 2021. "Treatment and Survival of Malignant Extracranial Germ Cell Tumours in the Paediatric Population: A Systematic Review and Meta-Analysis" Cancers 13, no. 14: 3561. https://doi.org/10.3390/cancers13143561