
Clinical Outcomes of Pencil Beam Scanning Proton Therapy in Locally Advanced Non-Small Cell Lung Cancer: Propensity Score Analysis


Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Population
2.2. Radiation Therapy
2.3. Chemotherapy
2.4. Surveillance
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Radiation Therapy Characteristics
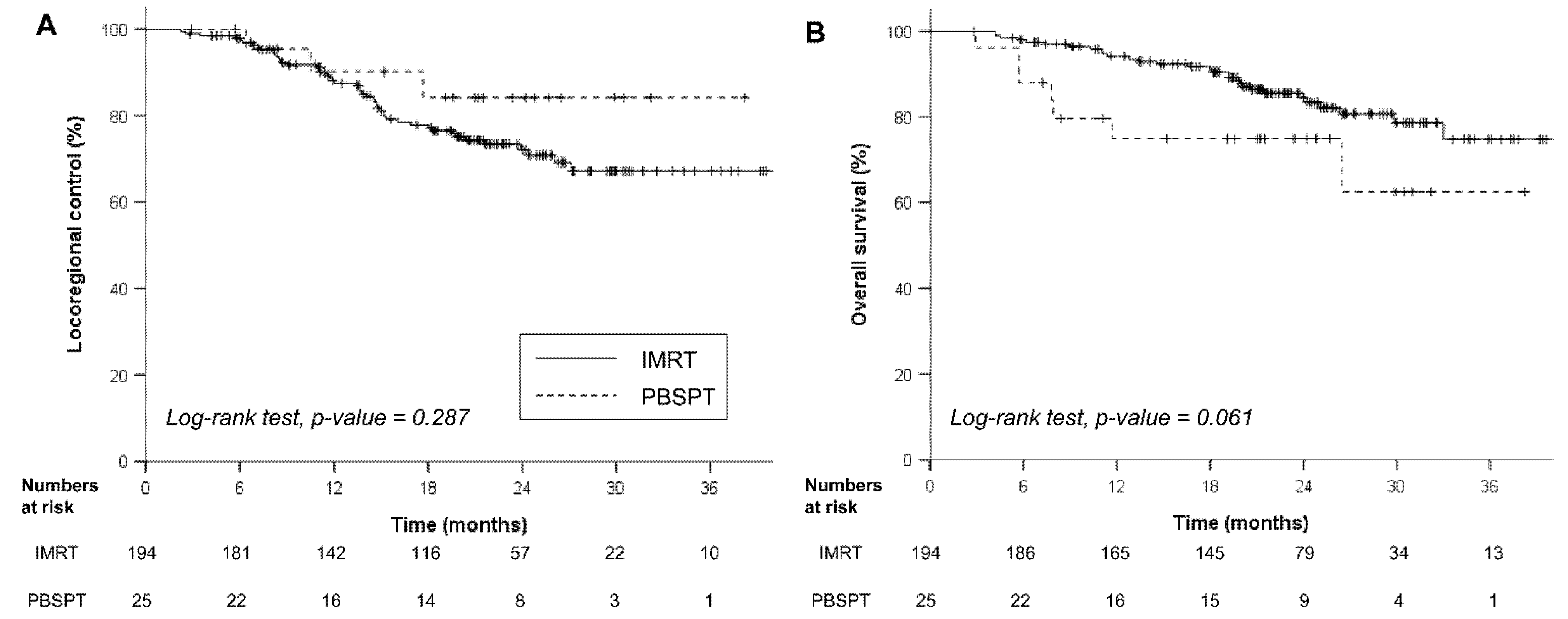
3.3. Oncologic Outcomes
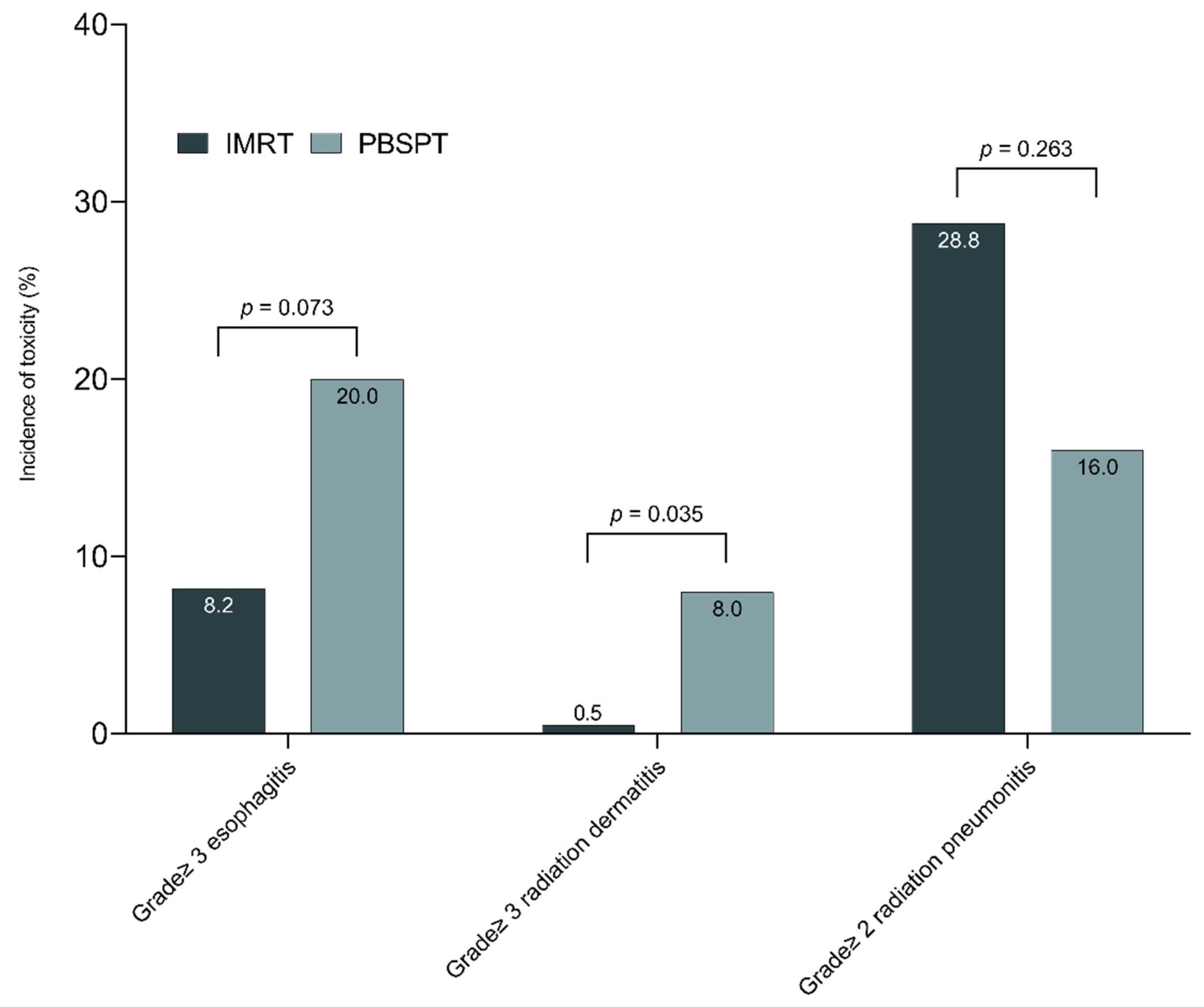
3.4. Toxicity
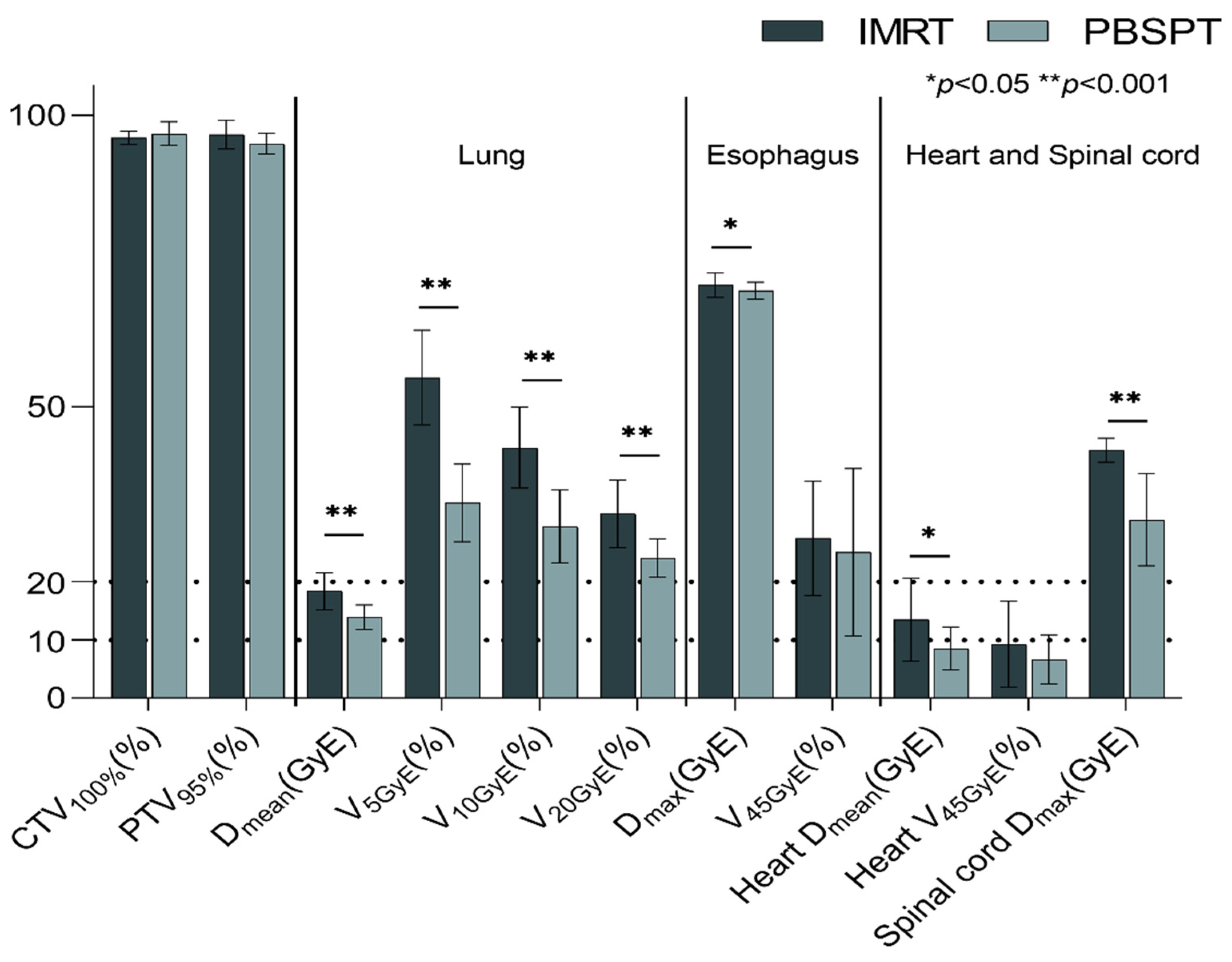
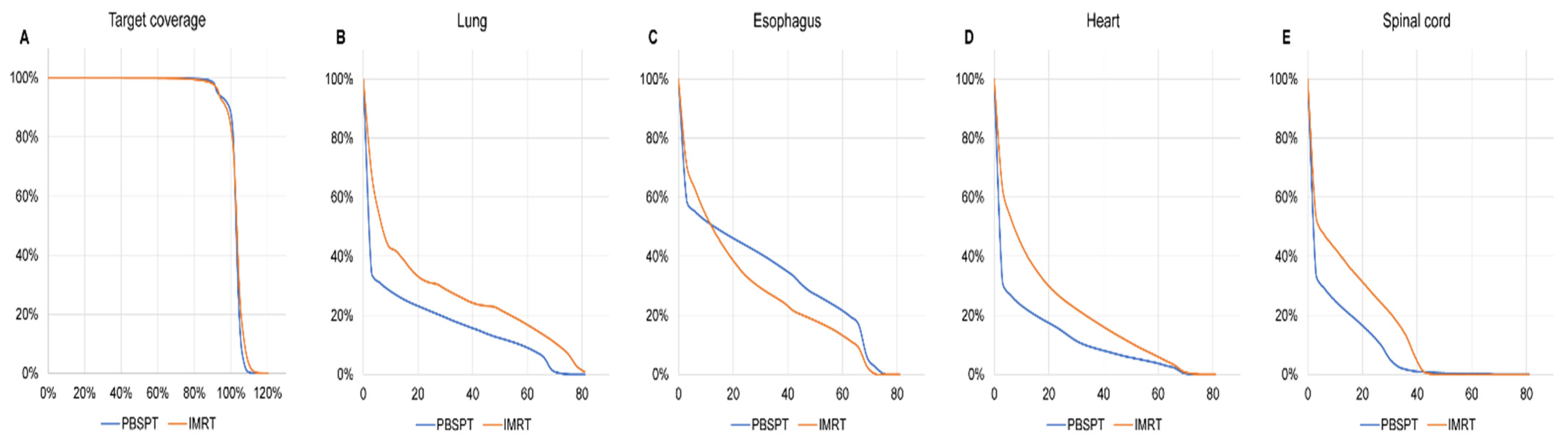
3.5. Dosimetric Comparison for Matched IMRT and PBSPT Plans
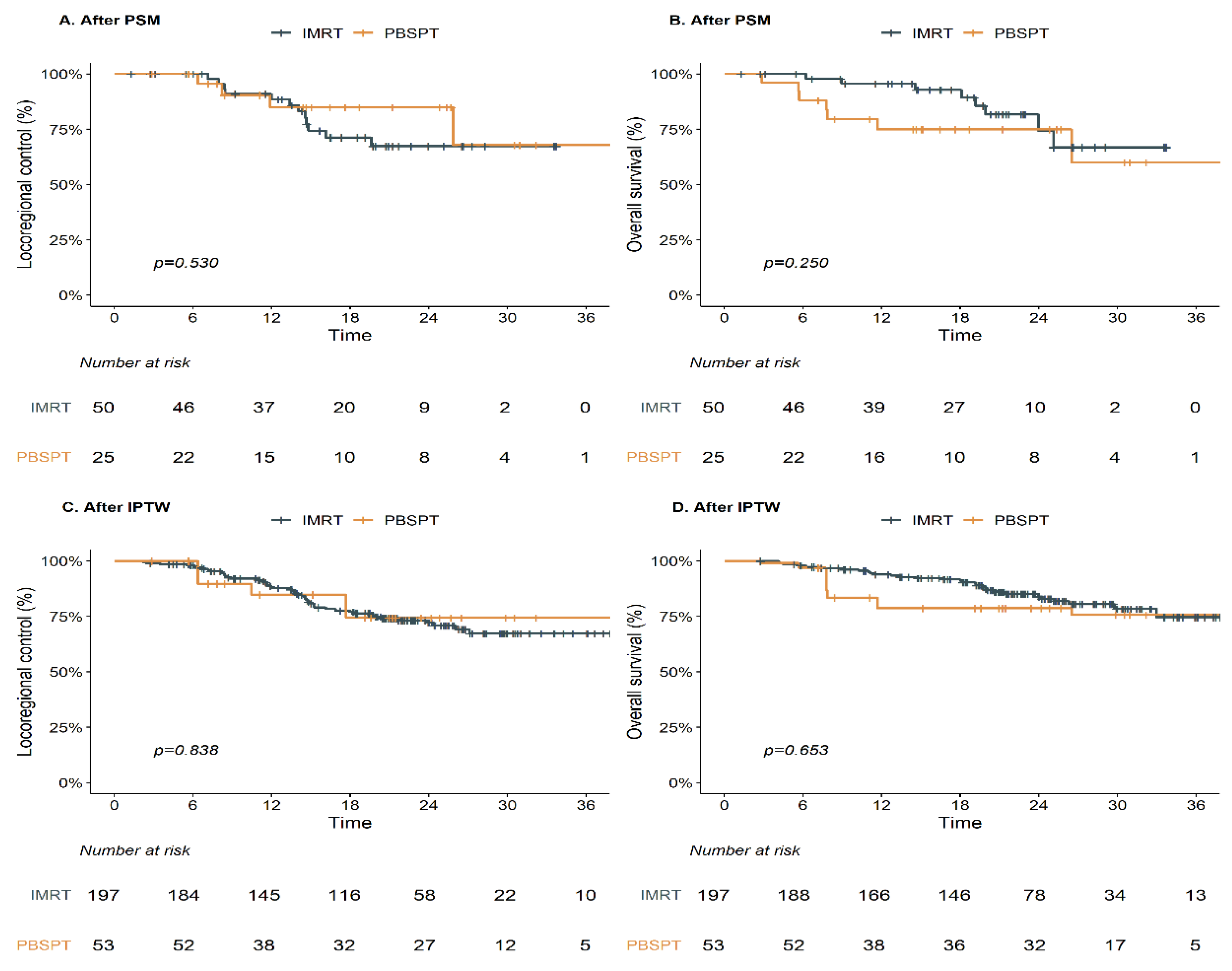
3.6. Oncologic and Toxicity Outcomes for Propensity Score-Adjusted Patients
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bradley, J.D.; Hu, C.; Komaki, R.R.; Masters, G.A.; Blumenschein, G.R.; Schild, S.E.; Bogart, J.A.; Forster, K.M.; Magliocco, A.M.; Kavadi, V.S.; et al. Long-term results of nrg oncology rtog 0617: Standard-versus high-dose chemoradiotherapy with or without cetuximab for unresectable stage iii non-small-cell lung cancer. J. Clin. Oncol. 2020, 38, 706–714. [Google Scholar] [CrossRef]
- Machtay, M.; Bae, K.; Movsas, B.; Paulus, R.; Gore, E.M.; Komaki, R.; Albain, K.; Sause, W.T.; Curran, W.J. Higher biologically effective dose of radiotherapy is associated with improved outcomes for locally advanced non-small cell lung carcinoma treated with chemoradiation: An analysis of the radiation therapy oncology group. Int. J. Radiat. Oncol. Biol. Phys. 2012, 82, 425–434. [Google Scholar] [CrossRef] [Green Version]
- De Ruysscher, D.; Faivre-Finn, C.; Nackaerts, K.; Jordan, K.; Arends, J.; Douillard, J.Y.; Ricardi, U.; Peters, S. Recommendation for supportive care in patients receiving concurrent chemotherapy and radiotherapy for lung cancer. Ann. Oncol. 2020, 31, 41–49. [Google Scholar] [CrossRef] [Green Version]
- Aupérin, A.; Le Péchoux, C.; Rolland, E.; Curran, W.J.; Furuse, K.; Fournel, P.; Belderbos, J.; Clamon, G.; Ulutin, H.C.; Paulus, R.; et al. Meta-analysis of concomitant versus sequential radiochemotherapy in locally advanced non-small-cell lung cancer. J. Clin. Oncol. 2010, 28, 2181–2190. [Google Scholar] [CrossRef]
- Palma, D.A.; Senan, S.; Oberije, C.; Belderbos, J.; de Dios, N.R.; Bradley, J.D.; Barriger, R.B.; Moreno-Jiménez, M.; Kim, T.H.; Ramella, S.; et al. Predicting esophagitis after chemoradiation therapy for non-small cell lung cancer: An individual patient data meta-analysis. Int. J. Radiat. Oncol. Biol. Phys. 2013, 87, 690–696. [Google Scholar] [CrossRef]
- Simone, C.B., 2nd. Thoracic radiation normal tissue injury. Semin. Radiat. Oncol. 2017, 27, 370–377. [Google Scholar] [CrossRef]
- Atkins, K.M.; Rawal, B.; Chaunzwa, T.L.; Lamba, N.; Bitterman, D.S.; Williams, C.L.; Kozono, D.E.; Baldini, E.H.; Chen, A.B.; Nguyen, P.L.; et al. Cardiac radiation dose, cardiac disease, and mortality in patients with lung cancer. J. Am. Coll. Cardiol. 2019, 73, 2976–2987. [Google Scholar] [CrossRef]
- Chang, J.Y.; Zhang, X.; Wang, X.; Kang, Y.; Riley, B.; Bilton, S.; Mohan, R.; Komaki, R.; Cox, J.D. Significant reduction of normal tissue dose by proton radiotherapy compared with three-dimensional conformal or intensity-modulated radiation therapy in stage i or stage iii non-small-cell lung cancer. Int. J. Radiat. Oncol. Biol. Phys. 2006, 65, 1087–1096. [Google Scholar] [CrossRef] [PubMed]
- Nichols, R.C.; Huh, S.N.; Henderson, R.H.; Mendenhall, N.P.; Flampouri, S.; Li, Z.; D’Agostino, H.J.; Cury, J.D.; Pham, D.C.; Hoppe, B.S. Proton radiation therapy offers reduced normal lung and bone marrow exposure for patients receiving dose-escalated radiation therapy for unresectable stage iii non-small-cell lung cancer: A dosimetric study. Clin. Lung Cancer 2011, 12, 252–257. [Google Scholar] [CrossRef] [PubMed]
- Oshiro, Y.; Okumura, T.; Kurishima, K.; Homma, S.; Mizumoto, M.; Ishikawa, H.; Onizuka, M.; Sakai, M.; Goto, Y.; Hizawa, N.; et al. High-dose concurrent chemo-proton therapy for stage iii nsclc: Preliminary results of a phase ii study. J. Radiat. Res. 2014, 55, 959–965. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, J.Y.; Verma, V.; Li, M.; Zhang, W.; Komaki, R.; Lu, C.; Allen, P.K.; Liao, Z.; Welsh, J.; Lin, S.H.; et al. Proton beam radiotherapy and concurrent chemotherapy for unresectable stage iii non-small cell lung cancer: Final results of a phase 2 study. JAMA Oncol. 2017, 3, e172032. [Google Scholar] [CrossRef]
- Nguyen, Q.N.; Ly, N.B.; Komaki, R.; Levy, L.B.; Gomez, D.R.; Chang, J.Y.; Allen, P.K.; Mehran, R.J.; Lu, C.; Gillin, M.; et al. Long-term outcomes after proton therapy, with concurrent chemotherapy, for stage ii-iii inoperable non-small cell lung cancer. Radiother. Oncol. 2015, 115, 367–372. [Google Scholar] [CrossRef] [Green Version]
- Hoppe, B.S.; Henderson, R.; Pham, D.; Cury, J.D.; Bajwa, A.; Morris, C.G.; D’Agostino, H., Jr.; Flampouri, S.; Huh, S.; Li, Z.; et al. A phase 2 trial of concurrent chemotherapy and proton therapy for stage iii non-small cell lung cancer: Results and reflections following early closure of a single-institution study. Int. J. Radiat. Oncol. Biol. Phys. 2016, 95, 517–522. [Google Scholar] [CrossRef]
- Sejpal, S.; Komaki, R.; Tsao, A.; Chang, J.Y.; Liao, Z.; Wei, X.; Allen, P.K.; Lu, C.; Gillin, M.; Cox, J.D. Early findings on toxicity of proton beam therapy with concurrent chemotherapy for nonsmall cell lung cancer. Cancer 2011, 117, 3004–3013. [Google Scholar] [CrossRef]
- Liao, Z.; Lee, J.J.; Komaki, R.; Gomez, D.R.; O’Reilly, M.S.; Fossella, F.V.; Blumenschein, G.R., Jr.; Heymach, J.V.; Vaporciyan, A.A.; Swisher, S.G.; et al. Bayesian adaptive randomization trial of passive scattering proton therapy and intensity-modulated photon radiotherapy for locally advanced non-small-cell lung cancer. J. Clin. Oncol. 2018, 36, 1813–1822. [Google Scholar] [CrossRef]
- Han, Y. Current status of proton therapy techniques for lung cancer. Radiat. Oncol. J. 2019, 37, 232–248. [Google Scholar] [CrossRef]
- Zhang, X.; Li, Y.; Pan, X.; Xiaoqiang, L.; Mohan, R.; Komaki, R.; Cox, J.D.; Chang, J.Y. Intensity-modulated proton therapy reduces the dose to normal tissue compared with intensity-modulated radiation therapy or passive scattering proton therapy and enables individualized radical radiotherapy for extensive stage iiib non-small-cell lung cancer: A virtual clinical study. Int. J. Radiat. Oncol. Biol. Phys. 2010, 77, 357–366. [Google Scholar] [PubMed] [Green Version]
- Kesarwala, A.H.; Ko, C.J.; Ning, H.; Xanthopoulos, E.; Haglund, K.E.; O’Meara, W.P.; Simone, C.B., 2nd; Rengan, R. Intensity-modulated proton therapy for elective nodal irradiation and involved-field radiation in the definitive treatment of locally advanced non-small-cell lung cancer: A dosimetric study. Clin. Lung Cancer 2015, 16, 237–244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stuschke, M.; Kaiser, A.; Pöttgen, C.; Lübcke, W.; Farr, J. Potentials of robust intensity modulated scanning proton plans for locally advanced lung cancer in comparison to intensity modulated photon plans. Radiother. Oncol. 2012, 104, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.Y.; Li, H.; Zhu, X.R.; Liao, Z.; Zhao, L.; Liu, A.; Li, Y.; Sahoo, N.; Poenisch, F.; Gomez, D.R.; et al. Clinical implementation of intensity modulated proton therapy for thoracic malignancies. Int. J. Radiat. Oncol. Biol. Phys. 2014, 90, 809–818. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, N.Y.; DeWees, T.A.; Liu, C.; Daniels, T.B.; Ashman, J.B.; Beamer, S.E.; Jaroszewski, D.E.; Ross, H.J.; Paripati, H.R.; Rwigema, J.M.; et al. Early outcomes of patients with locally advanced non-small cell lung cancer treated with intensity-modulated proton therapy versus intensity-modulated radiation therapy: The mayo clinic experience. Adv. Radiat. Oncol. 2020, 5, 450–458. [Google Scholar] [CrossRef] [Green Version]
- Choi, J.K.; Paek, D.; Lee, J.O. Normal predictive values of spirometry in korean population. Tuberc. Respir. Dis. 2005, 58, 230–242. [Google Scholar] [CrossRef] [Green Version]
- Pellegrino, R.; Viegi, G.; Brusasco, V.; Crapo, R.O.; Burgos, F.; Casaburi, R.; Coates, A.; van der Grinten, C.P.; Gustafsson, P.; Hankinson, J.; et al. Interpretative strategies for lung function tests. Eur. Respir. J. 2005, 26, 948–968. [Google Scholar] [CrossRef] [PubMed]
- Yoo, G.S.; Yu, J.I.; Cho, S.; Jung, S.H.; Han, Y.; Park, S.; Oh, Y.; Lee, B.; Park, H.C.; Lim, D.H.; et al. Comparison of clinical outcomes between passive scattering versus pencil-beam scanning proton beam therapy for hepatocellular carcinoma. Radiother. Oncol. 2020, 146, 187–193. [Google Scholar] [CrossRef]
- Fredriksson, A.; Forsgren, A.; Hårdemark, B. Minimax optimization for handling range and setup uncertainties in proton therapy. Med. Phys. 2011, 38, 1672–1684. [Google Scholar] [CrossRef] [PubMed]
- Hicks, K.A.; Tcheng, J.E.; Bozkurt, B.; Chaitman, B.R.; Cutlio, D.E.; Farb, A.; Fonarow, G.C.; Jacobs, J.P.; Jaff, M.R.; Lichiman, J.H.; et al. 2014 ACC/AHA Key Data Elements and Definitions for Cardiovascular Endpoint Events in Clinical Trials: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Data Standards (Writing Committee to Develop Cardiovascular Endpoints Data Standards). J. Am. Coll. Cardiol. 2015, 66, 403–469. [Google Scholar] [PubMed] [Green Version]
- Liang, X.; Bradley, J.A.; Zheng, D.; Rutenberg, M.; Yeung, D.; Mendenhall, N.; Li, Z. Prognostic factors of radiation dermatitis following passive-scattering proton therapy for breast cancer. Radiat. Oncol. 2018, 13, 72. [Google Scholar] [CrossRef]
- DeCesaris, C.M.; Rice, S.R.; Bentzen, S.M.; Jatczak, J.; Mishra, M.V.; Nichols, E.M. Quantification of acute skin toxicities in patients with breast cancer undergoing adjuvant proton versus photon radiation therapy: A single institutional experience. Int. J. Radiat. Oncol. Biol. Phys. 2019, 104, 1084–1090. [Google Scholar] [CrossRef]
- Tommasino, F.; Durante, M.; D’Avino, V.; Liuzzi, R.; Conson, M.; Farace, P.; Palma, G.; Schwarz, M.; Cella, L.; Pacelli, R. Model-based approach for quantitative estimates of skin, heart, and lung toxicity risk for left-side photon and proton irradiation after breast-conserving surgery. Acta Oncol. 2017, 56, 730–736. [Google Scholar] [CrossRef] [Green Version]
- Chun, S.G.; Hu, C.; Choy, H.; Komaki, R.U.; Timmerman, R.D.; Schild, S.E.; Bogart, J.A.; Dobelbower, M.C.; Bosch, W.; Galvin, J.M.; et al. Impact of intensity-modulated radiation therapy technique for locally advanced non-small-cell lung cancer: A secondary analysis of the nrg oncology rtog 0617 randomized clinical trial. J. Clin. Oncol. 2017, 35, 56–62. [Google Scholar] [CrossRef] [PubMed]
- Saager, M.; Peschke, P.; Brons, S.; Debus, J.; Karger, C.P. Determination of the proton rbe in the rat spinal cord: Is there an increase towards the end of the spread-out bragg peak? Radiother. Oncol. 2018, 128, 115–120. [Google Scholar] [CrossRef]
- Kim, H.; Pyo, H.; Noh, J.M.; Lee, W.; Park, B.; Park, H.Y.; Yoo, H. Preliminary result of definitive radiotherapy in patients with non-small cell lung cancer who have underlying idiopathic pulmonary fibrosis: Comparison between x-ray and proton therapy. Radiat. Oncol. 2019, 14, 19. [Google Scholar] [CrossRef]
- Lee, Y.H.; Kim, Y.S.; Lee, S.N.; Lee, H.C.; Oh, S.J.; Kim, S.J.; Kim, Y.K.; Han, D.H.; Yoo Ie, R.; Kang, J.H.; et al. Interstitial lung change in pre-radiation therapy computed tomography is a risk factor for severe radiation pneumonitis. Cancer Res. Treat. 2015, 47, 676–686. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Yoo, H.; Pyo, H.; Ahn, Y.C.; Noh, J.M.; Ju, S.G.; Lee, W.; Park, B.; Kim, J.M.; Kang, N.; et al. Impact of underlying pulmonary diseases on treatment outcomes in early-stage non-small cell lung cancer treated with definitive radiotherapy. Int. J. Chron. Obstruct. Pulmon. Dis. 2019, 14, 2273–2281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thor, M.; Deasy, J.O.; Hu, C.; Gore, E.; Bar-Ad, V.; Robinson, C.; Wheatley, M.; Oh, J.H.; Bogart, J.; Garces, Y.I.; et al. Modeling the impact of cardio-pulmonary irradiation on overall survival in nrg oncology trial rtog 0617. Clin. Cancer Res. 2020. [Google Scholar] [CrossRef]
- Higgins, K.A.; O’Connell, K.; Liu, Y.; Gillespie, T.W.; McDonald, M.W.; Pillai, R.N.; Patel, K.R.; Patel, P.R.; Robinson, C.G.; Simone, C.B., 2nd; et al. National cancer database analysis of proton versus photon radiation therapy in non-small cell lung cancer. Int. J. Radiat. Oncol. Biol. Phys. 2017, 97, 128–137. [Google Scholar] [CrossRef] [Green Version]
- Smith, W.P.; Richard, P.J.; Zeng, J.; Apisarnthanarax, S.; Rengan, R.; Phillips, M.H. Decision analytic modeling for the economic analysis of proton radiotherapy for non-small cell lung cancer. Transl. Lung Cancer Res. 2018, 7, 122–133. [Google Scholar] [CrossRef] [PubMed]
- Lievens, Y.; Verhaeghe, N.; Neve, W.D.; Madani, I.; Vanderstraeten, B.; Verstraete, J.; Annemans, L. Proton radiotherapy for locally-advanced non-small cell lung cancer, a cost-effective alternative to photon radiotherapy in belgium? J. Thorac. Oncol. 2013, 8, S839–S840. [Google Scholar]
- Particle Therapy Co-Operative Group. Particle Therapy Patient Statistics (per end of 2018). Available online: https://www.ptcog.ch/images/patientstatistics/Patientstatistics-updateDec2018.pdf (accessed on 22 May 2020).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | IMRT n = 194 | PBSPT n = 25 | SMD | p-Value | |
|---|---|---|---|---|---|
| Sex | Male | 150 (77.3) | 21 (84.0) | 0.170 | 0.615 |
| Female | 44 (22.7) | 4 (16.0) | |||
| Age, years | 62.0 [56.0; 67.0] | 67.0 [61.0; 75.0] | 0.685 | 0.003 | |
| ECOG | 0–1 | 191 (98.5) | 23 (92.0) | 0.306 | 0.101 |
| Smoking history | Never smoker | 44 (22.7) | 2 (8.0) | 0.416 | 0.151 |
| Current or ex-smoker | 150 (77.3) | 23 (92.0) | |||
| Histology | Squamous cell carcinoma | 75 (38.7) | 15 (60.0) | 0.468 | 0.067 |
| Adenocarcinoma | 114 (58.8) | 9 (36.0) | |||
| Etc. | 5 (2.6) | 1 (4.0) | |||
| NOS | 3 | 1 | |||
| LCNEC | 2 | ||||
| EGFR mutant, n (%) | 37 (19.1) | 2 (8.0) | 0.328 | 0.266 | |
| ALK translocation, n (%) | 6 (3.1) | 0 (0.0) | 0.253 | 1.000 | |
| Clinical T stage | cT1–2 | 126 (64.9) | 15 (60.0) | 0.102 | 0.791 |
| cT3–4 | 68 (35.1) | 10 (40.0) | |||
| Clinical N stage | cN2 | 72 (26.8) | 13 (52.0) | 0.534 | 0.018 |
| cN3 | 142 (73.2) | 12 (48.0) | |||
| N3 involvement region | Contralateral mediastinum | 84 (43.3) | 5 (20.0) | 0.517 | 0.044 |
| Supraclavicular | 71 (36.6) | 9 (36.0) | 0.012 | 1.000 | |
| Overall stage | IIIA | 23 (11.9) | 9 (36.0) | 0.604 | 0.008 |
| IIIB | 138 (71.1) | 12 (48.0) | |||
| IIIC | 33 (17.0) | 4 (16.0) | |||
| Pre-treatment pulmonary function test | |||||
| FEV1, L | 2.50 (2.10; 3.06) | 2.35 (1.61; 2.81) | 0.487 | 0.040 | |
| FEV1, % | 84.0 (71.0; 95.0) | 72.0 (57.0; 88.0) | 0.420 | 0.042 | |
| FEV1 < 70% (moderate to severe) | 44 (22.7) | 10 (40.0) | 0.100 | ||
| FEV1 < 50% (severe) | 9 (4.6) | 5 (20.0) | 0.013 | ||
| DLco, % | 79.5 (66.0; 92.0) | 65.0 (51.0; 79.0) | 0.654 | 0.002 | |
| DLco < 60% (moderate to severe) | 30 (15.5) | 10 (40.0) | 0.006 | ||
| DLco < 40% (severe) | 2 (1.0) | 1 (4.0) | 0.306 | ||
| Locoregional Control | Univariable Analysis | Multivariable Analysis | |||||
| Variables | (Reference vs.) | HR | (95% CI) | p-Value | |||
| RT modality | (IMRT vs. PBSPT) | 0.54 | (0.17–1.72) | 0.296 | 0.43 | (0.13–1.41) | 0.165 |
| Sex | (female vs. male) | 1.80 | (0.84–3.83) | 0.130 | |||
| Age | (<65 vs. ≥65 years) | 0.68 | (0.37–1.25) | 0.218 | |||
| Histology | (non-ADC vs. ADC) | 0.52 | (0.30–0.92) | 0.024 | 0.58 | (0.33–1.05) | 0.071 |
| EGFR mutation | (wildtype vs. mutant) | 0.51 | (0.22–1.20) | 0.122 | |||
| Clinical T stage | (T1–2 vs. T3–4) | 1.50 | (0.85–2.63) | 0.162 | |||
| Clinical N stage | (N2 vs. N3) | 0.94 | (0.50–1.78) | 0.858 | |||
| Contralateral mediastinal lymph node | (no vs. yes) | 1.20 | (0.69–2.10) | 0.515 | |||
| SCF lymph node | (no vs. yes) | 0.81 | (0.45–1.46) | 0.486 | |||
| GTV | (<100 vs. ≥100 cc) | 1.90 | (1.06–3.38) | 0.030 | 1.74 | (0.96–3.16) | 0.069 |
| PTV | (<550 vs. ≥550 cc) | 1.18 | (0.68–2.05) | 0.567 | |||
| Fractional RT dose | (2.0 vs. 2.2 GyE) | 0.21 | (0.01–3.86) | 0.294 | |||
| Total RT dose | (≤66 vs. >66 GyE) | 0.97 | (0.38–2.44) | 0.944 | |||
| BED10 | (≤80 vs. >80 GyE) | 0.75 | (0.41–1.38) | 0.353 | |||
| Overall survival | Univariable | Multivariable | |||||
| Variables | (reference vs.) | HR | (95% CI) | p-value | HR | (95% CI) | p-value |
| RT modality | (IMRT vs. PBSPT) | 2.17 | (0.95–4.94) | 0.066 | 1.64 | (0.70–3.81) | 0.254 |
| Sex | (female vs. male) | 2.17 | (0.95–4.94) | 0.294 | |||
| Age | (<65 vs. ≥65 years) | 1.56 | (0.68–3.58) | 0.030 | 1.66 | (0.82–3.36) | 0.156 |
| Histology | (non-ADC vs. ADC) | 2.10 | (1.08–4.10) | 0.006 | 0.54 | (0.26–1.13) | 0.103 |
| EGFR mutation | (wildtype vs. mutant) | 0.55 | (0.16–1.17) | 0.098 | 0.66 | (0.21–2.00) | 0.459 |
| Clinical T stage | (T1–2 vs. T3–4) | 1.28 | (0.66–2.49) | 0.470 | |||
| Clinical N stage | (N2 vs. N3) | 0.65 | (0.33–1.31) | 0.230 | |||
| Contralateral mediastinal lymph node | (no vs. yes) | 0.85 | (0.44–1.64) | 0.625 | |||
| SCF lymph node | (no vs. yes) | 0.98 | (0.50–1.90) | 0.950 | |||
| FEV1 (%) | (≥70 vs. <70%) | 0.85 | (0.39–1.86) | 0.687 | |||
| DLco (%) | (≥60 vs. <60%) | 1.64 | (0.75–3.61) | 0.216 | |||
| GTV | (<100 vs. ≥100 cc) | 1.48 | (0.77–2.86) | 0.243 | |||
| Total RT dose | (>66 vs. ≤66 GyE) | 4.55 | (0.63–33.3) | 0.132 | |||
| BED10 | (>80 vs. ≤80 GyE) | 1.01 | (0.48–2.12) | 0.986 | |||
| Category | Grade | IMRT n = 194 n (%) | PBSPT n = 25 n (%) | p-Value |
|---|---|---|---|---|
| Acute toxicity | ||||
| Esophagitis | Grade 0 | 29 (14.9) | 4 (16.0) | 0.286 |
| Grade 1 | 69 (35.6) | 9 (36.0) | ||
| Grade 2 | 80 (41.2) | 7 (28.0) | ||
| Grade 3 | 15 (7.7) | 5 (20.0) | ||
| Grade 4 | 1 (0.5) | 0 (0.0) | ||
| Radiation dermatitis | Grade 0 | 161 (83.0) | 19 (76.0) | 0.013 |
| Grade 1 | 17 (8.8) | 0 (0.0) | ||
| Grade 2 | 15 (7.7) | 4 (16.0) | ||
| Grade 3 | 1 (0.5) | 2 (8.0) | ||
| Late toxicity | ||||
| Radiation pneumonitis | Grade 0 | 115 (59.3) | 18 (72.0) | 0.648 |
| Grade 1 | 23 (11.9) | 3 (12.0) | ||
| Grade 2 | 47 (24.2) | 4 (16.0) | ||
| Grade 3 | 9 (4.6) | 0 (0.0) | ||
| Late esophageal toxicity | Grade 0 | 191 (98.5) | 24 (96.0) | 0.386 |
| Grade 1 | 0 (0.0) | 0 (0.0) | ||
| Grade 2 | 1 (0.5) | 1 (4.0) | ||
| Grade 3 | 2 (1.0) | 0 (0.0) | ||
| Major cardiac adverse events | 18 (9.3) | 2 (8.0) | 1.000 |
| Grade ≥ 3 Acute Esophagitis | Univariable Analysis | Multivariable Analysis | |||||
| Variables | (Reference vs.) | OR | (95% CI) | p-Value | OR | (95% CI) | p-Value |
| RT modality | (IMRT vs. PBSPT) | 2.78 | (0.84–8.00) | 0.070 | 3.68 | (0.97–12.88) | 0.045 |
| Sex | (female vs. male) | 0.33 | (0.13–0.85) | 0.019 | 0.32 | (0.06–1.74) | 0.181 |
| Age | (<65 vs. ≥65 years) | 1.2 | (0.47–2.98) | 0.698 | |||
| Smoking history | (never vs. ever) | 0.39 | (0.15–1.04) | 0.049 | 0.74 | (0.13–4.30) | 0.735 |
| Clinical T stage | (T1–2 vs. T3–4) | 0.89 | (0.33–2.26) | 0.818 | |||
| Clinical N stage | (N2 vs. N3) | 0.53 | (0.21–1.35) | 0.170 | |||
| Contralateral mediastinal lymph node | (no vs. yes) | 0.89 | (0.34–2.21) | 0.803 | |||
| SCF lymph node | (no vs. yes) | 0.86 | (0.31–2.16) | 0.749 | |||
| PTV | (<550 vs. ≥550 cc) | 1.39 | (0.56–3.54) | 0.479 | |||
| Fractional RT dose | (2.0 vs. 2.2 GyE) | 2.37 | (0.76–10.38) | 0.181 | |||
| Total RT dose | (≤66 vs. >66 GyE) | 0.69 | (0.27–1.66) | 0.408 | |||
| Esophagus Dmax | (<70 vs. ≥70 GyE) | 2.65 | (0.94–9.46) | 0.090 | 2.46 | (0.68–10.66) | 0.193 |
| Esophagus V45GyE | (<35 vs. ≥35%) | 4.33 | (1.73–11.50) | 0.002 | 3.98 | (1.12–19.02) | 0.049 |
| Esophagus V55GyE | (<20 vs. ≥20%) | 3.14 | (1.18–9.89) | 0.032 | 0.76 | (0.13–3.69) | 0.736 |
| Esophagus V66GyE | (<10 vs. ≥10%) | 2.05 | (0.83–5.24) | 0.122 | |||
| Grade≥ 2 radiation pneumonitis | Univariable analysis | Multivariable analysis | |||||
| Variables | (reference vs.) | OR | (95% CI) | p-value | OR | (95% CI) | p-value |
| RT modality | (IMRT vs. PBSPT) | 0.47 | (0.13–1.30) | 0.183 | 0.88 | (0.24–2.64) | 0.837 |
| Sex | (female vs. male) | 0.69 | (0.35–1.41) | 0.298 | |||
| Age | (<65 vs. ≥65 years) | 1.07 | (0.58–1.96) | 0.825 | |||
| Smoking history | (never vs. ever) | 0.64 | (0.32–1.30) | 0.208 | |||
| Clinical T stage | (T1–2 vs. T3–4) | 1.06 | (0.57–1.96) | 0.842 | |||
| Clinical N stage | (N2 vs. N3) | 0.64 | (0.32–1.21) | 0.166 | |||
| Contralateral mediastinal lymph node | (no vs. yes) | 0.72 | (0.38–1.32) | 0.298 | |||
| SCF lymph node | (no vs. yes) | 1.01 | (0.54–1.86) | 0.979 | |||
| FEV1 (%) | (≥70 vs. <70%) | 0.80 | (0.38–1.59) | 0.529 | |||
| DLco (%) | (≥60 vs. <60%) | 0.86 | (0.38–1.84) | 0.707 | |||
| PTV | (<550 vs. ≥550 cc) | 1.61 | (0.89–2.95) | 0.121 | |||
| Fractional RT dose | (2.0 vs. 2.2 GyE) | 1.15 | (0.59–2.32) | 0.691 | |||
| Total RT dose | (≤66 vs. >66 GyE) | 0.76 | (0.24–2.03) | 0.605 | |||
| Both-lung Dmean | (<20 vs. ≥20 GyE) | 2.79 | (1.51–5.19) | 0.001 | 1.71 | (0.62–4.74) | 0.297 |
| Both-lung V5GyE | (<65 vs. ≥65%) | 1.86 | (0.90–3.76) | 0.087 | 0.61 | (0.24–1.51) | 0.292 |
| Both-lung V10GyE | (<45 vs. ≥45%) | 3.78 | (2.04–7.10) | <0.001 | 4.37 | (1.63–12.12) | 0.004 |
| Both-lung V20GyE | (<35 vs. ≥35%) | 2.60 | (1.40–4.86) | 0.003 | 0.69 | (0.20–2.23) | 0.542 |
| Variables | Propensity Score Matching | IPTW | |||||
|---|---|---|---|---|---|---|---|
| IMRT | PBSPT | SMD | IMRT | PBSPT | SMD | ||
| n = 50 | n = 25 | n = 197.0 | n = 53.6 | ||||
| Sex | Male | 42 (84.0) | 21 (84.0) | <0.001 | 153.7 (78.7) | 36.2 (67.5) | 0.238 |
| Age, years | 67.7 (7.0) | 67.5 (8.8) | 0.033 | 62.0 (9.0) | 60.1 (8.8) | 0.217 | |
| ECOG | 0–1 | 50 (100.0) | 23 (92.0) | 0.417 | 194 (98.5) | 52.5 (97.9) | 0.039 |
| Histology | ADC | 18 (36.0) | 9 (36.0) | <0.001 | 110.0 (56.4) | 35.3 (65.9) | 0.196 |
| EGFR mutant | 5 (10.00) | 2 (8.0) | 0.070 | 35.3 (17.9) | 14.9 (27.8) | 0.238 | |
| Clinical T stage | cT3–4 | 19 (38.0) | 10 (40.0) | 0.121 | 71.6 (36.4) | 33.8 (63.2) | 0.557 |
| Clinical N stage | cN3 | 26 (52.0) | 12 (48.0) | 0.080 | 138.7 (70.4) | 37.3 (69.6) | 0.017 |
| N3 region | Contralateral mediastinum | 13 (26.0) | 5 (20.0) | 0.143 | 82.4 (41.8) | 20.2 (37.7) | 0.084 |
| Supraclavicular | 14 (28.0) | 9 (36.0) | 0.172 | 68.7 (34.9) | 24.1 (45.0) | 0.207 | |
| Pre-treatment pulmonary function test | |||||||
| FEV1, % | 74.4 (20.0) | 73.1 (24.2) | 0.061 | 81.1 (18.7) | 78.6 (21.7) | 0.112 | |
| DLCO, % | 71.5 (22.0) | 67.0 (19.3) | 0.216 | 78.0 (19.2) | 82.3 (19.4) | 0.121 | |
| Radiation therapy | |||||||
| Gross tumor volume, cc | 191.8 (188.8) | 178.0 (151.2) | 0.080 | 156.9 (162.8) | 176.5 (133.6) | 0.131 | |
| Clinical target volume, cc | 443.4 (307.4) | 453.6 (307.3) | 0.033 | 378.9 (271.6) | 440.3 (260.8) | 0.231 | |
| Planning target volume, cc | 704.8 (405.3) | 734.4 (437.9) | 0.070 | 628.0 (361.1) | 711.7 (380.8) | 0.226 | |
| (Reference: IMRT) | PSM | IPTW | ||||
|---|---|---|---|---|---|---|
| HR | (95% CI) | p-value | HR | (95% CI) | p-value | |
| Locoregional control | 0.46 | (0.13–1.67) | 0.236 | 0.87 | (0.46–1.64) | 0.668 |
| Overall survival | 1.69 | (0.54–5.29) | 0.371 | 1.39 | (0.71–2.71) | 0.339 |
| OR | (95% CI) | p-value | OR | (95% CI) | p-value | |
| Acute esophagitis grade ≥ 3 | 2.91 | (0.68–12.45) | 0.151 | 5.33 | (1.21–23.46) | 0.028 |
| Radiation pneumonitis grade ≥ 2 | 0.54 | (0.34–1.04) | 0.059 | 0.32 | (0.09–1.15) | 0.082 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, N.; Noh, J.M.; Lee, W.; Park, B.; Pyo, H. Clinical Outcomes of Pencil Beam Scanning Proton Therapy in Locally Advanced Non-Small Cell Lung Cancer: Propensity Score Analysis. Cancers 2021, 13, 3497. https://doi.org/10.3390/cancers13143497
Kim N, Noh JM, Lee W, Park B, Pyo H. Clinical Outcomes of Pencil Beam Scanning Proton Therapy in Locally Advanced Non-Small Cell Lung Cancer: Propensity Score Analysis. Cancers. 2021; 13(14):3497. https://doi.org/10.3390/cancers13143497
Chicago/Turabian StyleKim, Nalee, Jae Myoung Noh, Woojin Lee, Byoungsuk Park, and Hongryull Pyo. 2021. "Clinical Outcomes of Pencil Beam Scanning Proton Therapy in Locally Advanced Non-Small Cell Lung Cancer: Propensity Score Analysis" Cancers 13, no. 14: 3497. https://doi.org/10.3390/cancers13143497