
Major Oncogenic Drivers and Their Clinicopathological Correlations in Sporadic Childhood Papillary Thyroid Carcinoma in Belarus

 and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Results
2.1. Prevalence of Known Oncogenes in Childhood Sporadic PTC
2.2. Association of Oncogenes with Clinicopathological Features
2.3. Detection of Novel Fusion Oncogenes by RNA-seq
3. Discussion
3.1. BRAFV600E Mutation in Radiation-Related and Sporadic Pediatric/Young Adult PTC Patients
3.1.1. BRAFV600E Mutation in Radiation-Related and Sporadic PTC from Belarus and Ukraine
3.1.2. BRAFV600E Mutation in Radiation-Related and Sporadic PTC from Different Countries
3.2. RET/PTC1 and RET/PTC3 Rearrangements in Pediatric/Young Adult PTC Patients
3.3. ETV6/NTRK3 Rearrangement in Pediatric/Young Adult PTC Patients
3.4. AKAP9/BRAF Rearrangement in Pediatric/Young Adult PTC Patients
3.5. The RAS Family Gene Mutations in PTC Diagnosed in Pediatric/Young Adult Patients
3.6. Correlation between the Mutational Status and Clinicopathological Characteristics
4. Materials and Methods
4.1. Patients and Tissue Samples
4.2. Nucleic acid Extraction
4.3. Detection of Known Fusion Oncogenes and Point Mutations
4.4. RNA-seq and Data Analysis
4.5. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fugazzola, L.; Pilotti, S.; Pinchera, A.; Vorontsova, T.V.; Mondellini, P.; Bongarzone, I.; Greco, A.; Astakhova, L.; Butti, M.G.; Demidchik, E.P. Oncogenic rearrangements of the RET proto-oncogene in papillary thyroid carcinomas from children exposed to the Chernobyl nuclear accident. Cancer Res. 1995, 55, 5617–5620. [Google Scholar]
- Klugbauer, S.; Lengfelder, E.; Demidchik, E.P.; Rabes, H.M. High prevalence of RET rearrangement in thyroid tumors of children from Belarus after the Chernobyl reactor accident. Oncogene 1995, 11, 2459–2467. [Google Scholar]
- Nikiforov, Y.E.; Rowland, J.M.; Bove, K.E.; Monforte-Munoz, H.; Fagin, J.A. Distinct pattern of ret oncogene rearrangements in morphological variants of radiation-induced and sporadic thyroid papillary carcinomas in children. Cancer Res. 1997, 57, 1690–1694. [Google Scholar] [PubMed]
- Smida, J.; Salassidis, K.; Hieber, L.; Zitzelsberger, H.; Kellerer, A.M.; Demidchik, E.P.; Negele, T.; Spelsberg, F.; Lengfelder, E.; Werner, M.; et al. Distinct frequency of ret rearrangements in papillary thyroid carcinomas of children and adults from Belarus. Int. J. Cancer 1999, 80, 32–38. [Google Scholar] [CrossRef]
- Thomas, G.A.; Bunnell, H.; Cook, H.A.; Williams, E.D.; Nerovnya, A.; Cherstvoy, E.D.; Tronko, N.D.; Bogdanova, T.; Chiappetta, G.; Viglietto, G.; et al. High Prevalence of RET/PTC Rearrangements in Ukrainian and Belarussian Post-Chernobyl Thyroid Papillary Carcinomas: A Strong Correlation between RET/PTC3 and the Solid-Follicular Variant1. J. Clin. Endocrinol. Metab. 1999, 84, 4232–4238. [Google Scholar] [CrossRef] [PubMed]
- Rabes, H.M.; Demidchik, E.P.; Sidorow, J.D.; Lengfelder, E.; Beimfohr, C.; Hoelzel, D.; Klugbauer, S. Pattern of radia-tion-induced RET and NTRK1 rearrangements in 191 post-chernobyl papillary thyroid carcinomas: Biological, phenotypic, and clinical implications. Clin. Cancer Res. 2000, 6, 1093–1103. [Google Scholar]
- Lima, J.; Trovisco, V.; Soares, P.; Máximo, V.; Magalhães, J.; Salvatore, G.; Santoro, M.; Bogdanova, T.; Tronko, M.; Abrosimov, A.; et al. BRAFMutations Are Not a Major Event in Post-Chernobyl Childhood Thyroid Carcinomas. J. Clin. Endocrinol. Metab. 2004, 89, 4267–4271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumagai, A.; Namba, H.; Saenko, V.A.; Ashizawa, K.; Ohtsuru, A.; Ito, M.; Ishikawa, N.; Sugino, K.; Ito, K.; Jeremiah, S.; et al. Low Frequency of BRAFT1796A Mutations in Childhood Thyroid Carcinomas. J. Clin. Endocrinol. Metab. 2004, 89, 4280–4284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Penko, K.; Livezey, J.; Fenton, C.; Patel, A.; Nicholson, D.; Flora, M.; Oakley, K.; Tuttle, R.M.; Francis, G. BRAF Mutations are Uncommon in Papillary Thyroid Cancer of Young Patients. Thyroid 2005, 15, 320–325. [Google Scholar] [CrossRef]
- Powell, N.; Jeremiah, S.; Morishita, M.; Dudley, E.; Bethel, J.; Bogdanova, T.; Tronko, M.; Thomas, G. Frequency ofBRAF T1796A mutation in papillary thyroid carcinoma relates to age of patient at diagnosis and not to radiation exposure. J. Pathol. 2005, 205, 558–564. [Google Scholar] [CrossRef] [PubMed]
- Nikiforova, M.N.; Ciampi, R.; Salvatore, G.; Santoro, M.; Gandhi, M.; Knauf, J.A.; Thomas, G.A.; Jeremiah, S.; Bogdanova, T.; Tronko, M.D.; et al. Low prevalence of BRAF mutations in radiation-induced thyroid tumors in contrast to sporadic papillary carcinomas. Cancer Lett. 2004, 209, 1–6. [Google Scholar] [CrossRef] [PubMed]
- AIRTUM Working Group; CCM; AIEOP Working Group. Italian cancer figures, report 2012: Cancer in children and adoles-cents. Epidemiol. Prev. 2013, 37, 1–225. [Google Scholar]
- Vergamini, L.B.; Frazier, A.L.; Abrantes, F.L.; Ribeiro, K.B.; Rodriguez-Galindo, C. Increase in the Incidence of Differentiated Thyroid Carcinoma in Children, Adolescents, and Young Adults: A Population-Based Study. J. Pediatr. 2014, 164, 1481–1485. [Google Scholar] [CrossRef]
- Izumi, S.; Koyama, K.; Soda, M.; Suyama, A. Cancer incidence in children and young adults did not increase relative to parental exposure to atomic bombs. Br. J. Cancer 2003, 89, 1709–1713. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yeager, M.; Machiela, M.J.; Kothiyal, P.; Dean, M.; Bodelon, C.; Suman, S.; Wang, M.; Mirabello, L.; Nelson, C.W.; Zhou, W.; et al. Lack of transgenerational effects of ionizing radiation exposure from the Chernobyl accident. Science 2021, 372, 725–729. [Google Scholar] [CrossRef] [PubMed]
- Fridman, M.; Lam, A.K.-Y.; Krasko, O.; Schmid, K.W.; Branovan, D.I.; Demidchik, Y. Morphological and clinical presentation of papillary thyroid carcinoma in children and adolescents of Belarus: The influence of radiation exposure and the source of irradiation. Exp. Mol. Pathol. 2015, 98, 527–531. [Google Scholar] [CrossRef] [Green Version]
- Gerlitz, G.; Darhin, E.; Giorgio, G.; Franco, B.; Reiner, O. Novel Functional Features of the LIS-H Domain: Role in Protein Dimerization, Half-Life and Cellular Localization. Cell Cycle 2005, 4, 1632–1640. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agrawal, N.; Akbani, R.; Aksoy, B.A.; Ally, A.; Arachchi, H.; Asa, S.; Auman, J.T.; Balasundaram, M.; Balu, S.; Baylin, S.B.; et al. Integrated Genomic Characterization of Papillary Thyroid Carcinoma. Cell 2014, 159, 676–690. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morton, L.M.; Karyadi, D.M.; Stewart, C.; Bogdanova, T.I.; Dawson, E.T.; Steinberg, M.K.; Dai, J.; Hartley, S.W.; Schonfeld, S.J.; Sampson, J.N.; et al. Radiation-related genomic profile of papillary thyroid carcinoma after the Chernobyl accident. Science 2021, 372, eabg2538. [Google Scholar] [CrossRef]
- Ricarte-Filho, J.C.; Li, S.; Garcia-Rendueles, M.E.; Montero-Conde, C.; Voza, F.; Knauf, J.A.; Heguy, A.; Viale, A.; Bogdanova, T.; Thomas, G.A.; et al. Identification of kinase fusion oncogenes in post-Chernobyl radiation-induced thyroid cancers. J. Clin. Investig. 2013, 123, 4935–4944. [Google Scholar] [CrossRef] [Green Version]
- Rumiantsev, P.O.; Zaletaev, D.V.; Vasil’Ev, E.V.; Saenko, V.A.; Il’In, A.A.; Rumiantseva, U.V.; Alu, A.; Medvedev, V.S. Frequency of RET/PTC rearrangement and somatic BRAF mutation in papillary thyroid cancer. Vopr. Onkol. 2006, 52, 145–149. [Google Scholar]
- Henke, L.E.; Perkins, S.M.; Pfeifer, J.D.; Ma, C.; Chen, Y.; DeWees, T.; Grigsby, P.W. BRAFV600E mutational status in pediatric thyroid cancer. Pediatr. Blood Cancer 2014, 61, 1168–1172. [Google Scholar] [CrossRef]
- Givens, D.J.; Buchmann, L.O.; Agarwal, A.M.; Grimmer, J.F.; Hunt, J.P. BRAF V600E does not predict aggressive features of pediatric papillary thyroid carcinoma. Laryngoscope 2014, 124, E389–E393. [Google Scholar] [CrossRef]
- Buryk, M.A.; Monaco, S.E.; Witchel, S.F.; Mehta, D.K.; Gurtunca, N.; Nikiforov, Y.E.; Simons, J.P. Preoperative cytology with molecular analysis to help guide surgery for pediatric thyroid nodules. Int. J. Pediatr. Otorhinolaryngol. 2013, 77, 1697–1700. [Google Scholar] [CrossRef] [PubMed]
- Ballester, L.Y.; Sarabia, S.F.; Sayeed, H.; Patel, N.R.; Baalwa, J.; Athanassaki, I.; Hernandez, J.A.; Fang, E.; Quintanilla, N.M.; Roy, A.; et al. Integrating Molecular Testing in the Diagnosis and Management of Children with Thyroid Lesions. Pediatr. Dev. Pathol. 2016, 19, 94–100. [Google Scholar] [CrossRef]
- Gertz, R.J.; Nikiforov, Y.; Rehrauer, W.; McDaniel, L.; Lloyd, R.V. Mutation in BRAF and Other Members of the MAPK Pathway in Papillary Thyroid Carcinoma in the Pediatric Population. Arch. Pathol. Lab. Med. 2016, 140, 134–139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hardee, S.; Prasad, M.L.; Hui, P.; Dinauer, C.A.; Morotti, R.A. Pathologic Characteristics, Natural History, and Prognostic Implications of BRAFV600E Mutation in Pediatric Papillary Thyroid Carcinoma. Pediatr. Dev. Pathol. 2017, 20, 206–212. [Google Scholar] [CrossRef] [PubMed]
- Nikita, M.E.; Jiang, W.; Cheng, S.-M.; Hantash, F.M.; McPhaul, M.J.; Newbury, R.O.; Phillips, S.A.; Reitz, R.E.; Waldman, F.M.; Newfield, R.S. Mutational Analysis in Pediatric Thyroid Cancer and Correlations with Age, Ethnicity, and Clinical Presentation. Thyroid 2016, 26, 227–234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prasad, M.L.; Vyas, M.; Horne, M.J.; Virk, R.K.; Morotti, R.; Liu, Z.; Tallini, G.; Nikiforova, M.N.; Christison-Lagay, E.R.; Udelsman, R.; et al. NTRKfusion oncogenes in pediatric papillary thyroid carcinoma in northeast United States. Cancer 2016, 122, 1097–1107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Su, X.; Li, Z.; He, C.; Chen, W.; Fu, X.; Yang, A. Radiation exposure, young age, and female gender are associated with high prevalence of RET/PTC1 and RET/PTC3 in papillary thyroid cancer: A meta-analysis. Oncotarget 2016, 7, 16716–16730. [Google Scholar] [CrossRef] [Green Version]
- Leeman-Neill, R.J.; Bs, L.M.K.; Liu, P.; Brenner, A.V.; Leeman-Neill, R.J.; Bogdanova, T.I.; Evdokimova, V.N.; Hatch, M.; Zurnadzy, L.Y.; Nikiforova, M.N.; et al. ETV6-NTRK3 is a common chromosomal rearrangement in radiation-associated thyroid cancer. Cancer 2014, 120, 799–807. [Google Scholar] [CrossRef] [Green Version]
- Picarsic, J.L.; Buryk, M.A.; Ozolek, J.A.; Ranganathan, S.; Monaco, S.E.; Simons, J.P.; Witchel, S.F.; Gurtunca, N.; Joyce, J.; Zhong, S.; et al. Molecular Characterization of Sporadic Pediatric Thyroid Carcinoma with the DNA/RNA ThyroSeq v2 Next-Generation Sequencing Assay. Pediatr. Dev. Pathol. 2016, 19, 115–122. [Google Scholar] [CrossRef]
- Potter, S.L.; Reuther, J.; Chandramohan, R.; Gandhi, I.; Hollingsworth, F.; Sayeed, H.; Voicu, H.; Kakkar, N.; Baksi, K.S.; Sarabia, S.F.; et al. Integrated DNA and RNA sequencing reveals targetable alterations in metastatic pediatric papillary thyroid carcinoma. Pediatr. Blood Cancer 2021, 68, e28741. [Google Scholar] [CrossRef]
- Franco, A.; Labourier, E.; Ablordeppey, K.K.; Surrey, L.F.; Mostoufi-Moab, S.; Isaza, A.; Adzick, N.S.; Kazahaya, K.; Kumar, G.; Bauer, A.J. miRNA expression can classify pediatric thyroid lesions and increases the diagnostic yield of mutation testing. Pediatr. Blood Cancer 2020, 67, e28276. [Google Scholar] [CrossRef] [PubMed]
- Cordioli, M.I.C.V.; Moraes, L.; Bastos, A.U.; Besson, P.; Alves, M.T.D.S.; Delcelo, R.; Monte, O.; Longui, C.; Cury, A.N.; Cerutti, J.M. Fusion Oncogenes Are the Main Genetic Events Found in Sporadic Papillary Thyroid Carcinomas from Children. Thyroid 2017, 27, 182–188. [Google Scholar] [CrossRef] [PubMed]
- Mitsutake, N.; Fukushima, T.; Matsuse, M.; Rogounovitch, T.; Saenko, V.; Uchino, S.; Ito, M.; Suzuki, K.; Suzuki, S.; Yamashita, S. BRAFV600E mutation is highly prevalent in thyroid carcinomas in the young population in Fukushima: A different oncogenic profile from Chernobyl. Sci. Rep. 2015, 5, 16976. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ciampi, R.; Knauf, J.A.; Kerler, R.; Gandhi, M.; Zhu, Z.; Nikiforova, M.N.; Rabes, H.M.; Fagin, J.A.; Nikiforov, Y.E. Oncogenic AKAP9-BRAF fusion is a novel mechanism of MAPK pathway activation in thyroid cancer. J. Clin. Investig. 2005, 115, 94–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nikiforov, Y.E.; Nikiforova, M.N.; Gnepp, D.R.; Fagin, J.A. Prevalence of mutations of ras and p53 in benign and malignant thyroid tumors from children exposed to radiation after the Chernobyl nuclear accident. Oncogene 1996, 13, 687–693. [Google Scholar]
- Suchy, B.; Waldmann, V.; Klugbauer, S.; Rabes, H.M. Absence of RAS and p53 mutations in thyroid carcinomas of children after Chernobyl in contrast to adult thyroid tumours. Br. J. Cancer 1998, 77, 952–955. [Google Scholar] [CrossRef] [Green Version]
- Sassolas, G.; Hafdi-Nejjari, Z.; Ferraro, A.; Decaussin-Petrucci, M.; Rousset, B.; Borson-Chazot, F.; Borbone, E.; Berger, N.; Fusco, A. Oncogenic Alterations in Papillary Thyroid Cancers of Young Patients. Thyroid 2012, 22, 17–26. [Google Scholar] [CrossRef]
- Alzahrani, A.S.; Murugan, A.K.; Qasem, E.; Alswailem, M.; Al-Hindi, H.; Shi, Y. Single Point Mutations in Pediatric Differentiated Thyroid Cancer. Thyroid 2017, 27, 189–196. [Google Scholar] [CrossRef]
- Fenton, C.; Anderson, J.; Lukes, Y.; Dinauer, C.A.W.; Tuttle, R.M.; Francis, G.L. Ras mutations are uncommon in sporadic thyroid cancer in children and young adults. J. Endocrinol. Investig. 1999, 22, 781–789. [Google Scholar] [CrossRef]
- Mostoufi-Moab, S.; Labourier, E.; Sullivan, L.; Livolsi, V.; Li, Y.; Xiao, R.; Beaudenon-Huibregtse, S.; Kazahaya, K.; Adzick, N.S.; Baloch, Z.; et al. Molecular Testing for Oncogenic Gene Alterations in Pediatric Thyroid Lesions. Thyroid 2018, 28, 60–67. [Google Scholar] [CrossRef] [PubMed]
- Shifrin, A.L.; Fischer, M.; Paul, T.; Erler, B.; Gheysens, K.; Baodhankar, P.; Song-Yang, J.W.; Taylor, S.; Timmaraju, V.A.; Topilow, A.; et al. Mutational analysis of metastatic lymph nodes from papillary thyroid carcinoma in adult and pediatric patients. Surgery 2017, 161, 176–187. [Google Scholar] [CrossRef] [PubMed]
- Nakazawa, T.; Kondo, T.; Kobayashi, Y.; Takamura, N.; Murata, S.-I.; Kameyama, K.; Muramatsu, A.; Ito, K.; Kobayashi, M.; Katoh, R. RET gene rearrangements (RET/PTC1 andRET/PTC3) in papillary thyroid carcinomas from an iodine-rich country (Japan). Cancer 2005, 104, 943–951. [Google Scholar] [CrossRef] [PubMed]
- Geng, J.; Wang, H.; Liu, Y.; Tai, J.; Jin, Y.; Zhang, J.; He, L.; Fu, L.; Qin, H.; Song, Y.; et al. Correlation between BRAF V600E mutation and clinicopathological features in pediatric papillary thyroid carcinoma. Sci. China Life Sci. 2017, 60, 729–738. [Google Scholar] [CrossRef]
- Basolo, F.; Giannini, R.; Monaco, C.; Melillo, R.M.; Carlomagno, F.; Pancrazi, M.; Salvatore, G.; Chiappetta, G.; Pacini, F.; Elisei, R.; et al. Potent Mitogenicity of the RET/PTC3 Oncogene Correlates with Its Prevalence in Tall-Cell Variant of Papillary Thyroid Carcinoma. Am. J. Pathol. 2002, 160, 247–254. [Google Scholar] [CrossRef] [Green Version]
- Santoro, M.; Chiappetta, G.; Cerrato, A.; Salvatore, D.; Zhang, L.; Manzo, G.; Picone, A.; Portella, G.; Santelli, G.; Vecchio, G.; et al. Development of thyroid papillary carcinomas secondary to tissue-specific expression of the RET/PTC1 oncogene in transgenic mice. Oncogene 1996, 12, 1821–1826. [Google Scholar]
- Powell, D.J.; Russell, J.; Nibu, K.; Li, G.; Rhee, E.; Liao, M.; Goldstein, M.; Keane, W.M.; Santoro, M.; Fusco, A.; et al. The RET/PTC3 oncogene: Metastatic solid-type papillary carcinomas in murine thyroids. Cancer Res. 1998, 58, 5523–5528. [Google Scholar]
- Jhiang, S.M.; Cho, J.-Y.; Furminger, T.L.; Sagartz, J.E.; Tong, Q.; Capen, C.C.; Mazzaferri, E.L. Thyroid Carcinomas in RET/PTC Transgenic Mice. Methods Mol. Biol. 1998, 154, 265–270. [Google Scholar] [CrossRef]
- Bogdanova, T.I.; Saenko, V.A.; Brenner, A.V.; Zurnadzhy, L.Y.; Rogounovitch, T.I.; Likhtarov, I.A.; Masiuk, S.; Kovgan, L.M.; Shpak, V.M.; Thomas, G.A.; et al. Comparative Histopathologic Analysis of “Radiogenic” and “Sporadic” Papillary Thyroid Carcinoma: Patients Born Before and After the Chernobyl Accident. Thyroid 2018, 28, 880–890. [Google Scholar] [CrossRef]
- Wang, Y.; Zhang, R.; Luo, Z.; Wu, Y.; Du, X.; Wang, Z.; Zhu, Y.; Li, D.; Ji, Q. High frequency of level II–V lymph node involvement in RET/PTC positive papillary thyroid carcinoma. Eur. J. Surg. Oncol. 2008, 34, 77–81. [Google Scholar] [CrossRef] [PubMed]
- Castro, P.; Rebocho, A.P.; Soares, R.J.; Magalhães, J.; Roque, L.; Trovisco, V.; De Castro, I.V.; Cardoso-De-Oliveira, M.; Fonseca, E.; Soares, P.; et al. PAX8-PPARγ Rearrangement Is Frequently Detected in the Follicular Variant of Papillary Thyroid Carcinoma. J. Clin. Endocrinol. Metab. 2006, 91, 213–220. [Google Scholar] [CrossRef] [Green Version]
- Zhu, Z.; Gandhi, M.; Nikiforova, M.N.; Fischer, A.H.; Nikiforov, Y.E. Molecular Profile and Clinical-Pathologic Features of the Follicular Variant of Papillary Thyroid Carcinoma: An Unusually High Prevalence of ras Mutations. Am. J. Clin. Pathol. 2003, 120, 71–77. [Google Scholar] [CrossRef]
- Cordioli, M.I.C.V.; Moraes, L.; Carvalheira, G.; Sisdelli, L.; Alves, M.T.S.; Delcelo, R.; Monte, O.; Longui, C.A.; Cury, A.N.; Cerutti, J.M. AGK-BRAF gene fusion is a recurrent event in sporadic pediatric thyroid carcinoma. Cancer Med. 2016, 5, 1535–1541. [Google Scholar] [CrossRef] [Green Version]
- Bogdanova, T.I.; Saenko, V.A.; Hashimoto, Y.; Hirokawa, M.; Zurnadzhy, L.Y.; Hayashi, T.; Ito, M.; Iwadate, M.; Mitsutake, N.; Rogounovitch, T.I.; et al. Papillary Thyroid Carcinoma in Ukraine After Chernobyl and in Japan After Fukushima: Different Histopathological Scenarios. Thyroid 2020. [Google Scholar] [CrossRef] [PubMed]
- Handkiewicz-Junak, D.; Swierniak, M.; Rusinek, D.; Oczko-Wojciechowska, M.; Dom, G.; Maenhaut, C.; Unger, K.; Detours, V.; Bogdanova, T.; Thomas, G.; et al. Gene signature of the post-Chernobyl papillary thyroid cancer. Eur. J. Nucl. Med. Mol. Imaging 2016, 43, 1267–1277. [Google Scholar] [CrossRef] [Green Version]
- Leeman-Neill, R.J.; Brenner, A.V.; Little, M.P.; Bogdanova, T.I.; Hatch, M.; Zurnadzy, L.Y.; Mabuchi, K.; Tronko, M.D.; Nikiforov, Y.E. RET/PTC and PAX8/PPARgamma chromosomal rearrangements in post-Chernobyl thyroid cancer and their association with iodine-131 radiation dose and other characteristics. Cancer 2013, 119, 1792–1799. [Google Scholar] [CrossRef] [Green Version]
- Pekova, B.; Dvorakova, S.; Sykorova, V.; Vacinova, G.; Vaclavikova, E.; Moravcova, J.; Katra, R.; Vlcek, P.; Sykorova, P.; Kodetova, D.; et al. Somatic genetic alterations in a large cohort of pediatric thyroid nodules. Endocr. Connect. 2019, 8, 796–805. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wasserman, J.D.; Sabbaghian, N.; Fahiminiya, S.; Chami, R.; Mete, O.; Acker, M.; Wu, M.K.; Shlien, A.; de Kock, L.; Foulkes, W.D. DICER1 Mutations Are Frequent in Adolescent-Onset Papillary Thyroid Carcinoma. J. Clin. Endocrinol. Metab. 2018, 103, 2009–2015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castro, P.; Patino, E.; Fierro, F.; Rojas, C.; Buitrago, G.; Olaya, N. Clinical characteristics, surgical approach, BRAFV600E mutation and sodium iodine symporter expression in pediatric patients with thyroid carcinoma. J. Pediatr. Endocrinol. Metabol. 2020, in press. [Google Scholar] [CrossRef] [PubMed]
- Sisdelli, L.; Cordioli, M.; Vaisman, F.; Moraes, L.; Colozza-Gama, G.A.; Alves, P.A.G., Jr.; Araujo, M.L., Jr.; Alves, M.T.S.; Monte, O.; Longui, C.A.; et al. AGK-BRAF is associated with distant metastasis and younger age in pediatric papillary thyroid carcinoma. Pediatric Blood Cancer 2019, 66, e27707. [Google Scholar] [CrossRef] [PubMed]
- Stanojevic, B.; Dzodic, R.; Saenko, V.; Milovanovic, Z.; Pupic, G.; Zivkovic, O.; Markovic, I.; Djurisic, I.; Buta, M.; Dimitrijevic, B.; et al. Mutational and clinico-pathological analysis of papillary thyroid carcinoma in Serbia. Endocr. J. 2011, 58, 381–393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Espadinha, C.; Santos, J.R.; Sobrinho, L.G.; Bugalho, M.J. Expression of iodine metabolism genes in human thyroid tissues: Evidence for age and BRAFV600E mutation dependency. Clin. Endocrinol. (Oxf) 2009, 70, 629–635. [Google Scholar] [CrossRef]
- Onder, S.; Ozturk Sari, S.; Yegen, G.; Sormaz, I.C.; Yilmaz, I.; Poyrazoglu, S.; Sanli, Y.; Giles Senyurek, Y.; Kapran, Y.; Mete, O. Classic Architecture with Multicentricity and Local Recurrence, and Absence of TERT Promoter Mutations are Correlates of BRAF (V600E) Harboring Pediatric Papillary Thyroid Carcinomas. Endocrinol. Pathol. 2016, 27, 153–161. [Google Scholar] [CrossRef]
- Poyrazoglu, S.; Bundak, R.; Bas, F.; Yegen, G.; Sanli, Y.; Darendeliler, F. Clinicopathological Characteristics of Papillary Thyroid Cancer in Children with Emphasis on Pubertal Status and Association with BRAF(V600E) Mutation. J. Clin. Res. Pediatr. Endocrinol. 2017, 9, 185–193. [Google Scholar] [CrossRef] [Green Version]
- Zou, M.; Baitei, E.Y.; Alzahrani, A.S.; BinHumaid, F.S.; Alkhafaji, D.; Al-Rijjal, R.A.; Meyer, B.F.; Shi, Y. Concomitant RAS, RET/PTC, or BRAF mutations in advanced stage of papillary thyroid carcinoma. Thyroid 2014, 24, 1256–1266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alzahrani, A.S.; Alswailem, M.; Alswailem, A.A.; Al-Hindi, H.; Goljan, E.; Alsudairy, N.; Abouelhoda, M. Genetic Alterations in Pediatric Thyroid Cancer Using a Comprehensive Childhood Cancer Gene Panel. J. Clin. Endocrinol. Metab. 2020, 105. [Google Scholar] [CrossRef] [PubMed]
- Chakraborty, D.; Shakya, S.; Ballal, S.; Agarwal, S.; Bal, C. BRAF V600E and TERT promoter mutations in paediatric and young adult papillary thyroid cancer and clinicopathological correlation. J. Pediatric Endocrinol. Metab. 2020, in press. [Google Scholar] [CrossRef] [PubMed]
- Huang, M.; Yan, C.; Wei, H.; Lv, Y.; Ling, R. Clinicopathological characteristics and prognosis of thyroid cancer in northwest China: A population-based retrospective study of 2490 patients. Thorac Cancer 2018, 9, 1453–1460. [Google Scholar] [CrossRef] [PubMed]
- Oishi, N.; Kondo, T.; Nakazawa, T.; Mochizuki, K.; Inoue, T.; Kasai, K.; Tahara, I.; Yabuta, T.; Hirokawa, M.; Miyauchi, A.; et al. Frequent BRAF (V600E) and Absence of TERT Promoter Mutations Characterize Sporadic Pediatric Papillary Thyroid Carcinomas in Japan. Endocr. Pathol. 2017, 28, 103–111. [Google Scholar] [CrossRef]
- Rosenbaum, E.; Hosler, G.; Zahurak, M.; Cohen, Y.; Sidransky, D.; Westra, W.H. Mutational activation of BRAF is not a major event in sporadic childhood papillary thyroid carcinoma. Mod. Pathol. 2005, 18, 898–902. [Google Scholar] [CrossRef] [PubMed]
- Monaco, S.E.; Pantanowitz, L.; Khalbuss, W.E.; Benkovich, V.A.; Ozolek, J.; Nikiforova, M.N.; Simons, J.P.; Nikiforov, Y.E. Cytomorphological and molecular genetic findings in pediatric thyroid fine-needle aspiration. Cancer Cytopathol. 2012, 120, 342–350. [Google Scholar] [CrossRef]
- Vanden Borre, P.; Schrock, A.B.; Anderson, P.M.; Morris, J.C., 3rd; Heilmann, A.M.; Holmes, O.; Wang, K.; Johnson, A.; Waguespack, S.G.; Ou, S.I.; et al. Pediatric, Adolescent, and Young Adult Thyroid Carcinoma Harbors Frequent and Diverse Targetable Genomic Alterations, Including Kinase Fusions. Oncologist 2017, 22, 255–263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santoro, M.; Thomas, G.A.; Vecchio, G.; Williams, G.H.; Fusco, A.; Chiappetta, G.; Pozcharskaya, V.; Bogdanova, T.I.; Demidchik, E.P.; Cherstvoy, E.D.; et al. Gene rearrangement and Chernobyl related thyroid cancers. Br. J. Cancer 2000, 82, 315–322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pisarchik, A.V.; Ermak, G.; Fomicheva, V.; Kartel, N.A.; Figge, J. The ret/PTC1 rearrangement is a common feature of Chernobyl-associated papillary thyroid carcinomas from Belarus. Thyroid 1998, 8, 133–139. [Google Scholar] [CrossRef]
- Pisarchik, A.V.; Ermak, G.; Demidchik, E.P.; Mikhalevich, L.S.; Kartel, N.A.; Figge, J. Low prevalence of the ret/PTC3r1 rearrangement in a series of papillary thyroid carcinomas presenting in Belarus ten years post-Chernobyl. Thyroid 1998, 8, 1003–1008. [Google Scholar] [CrossRef] [PubMed]
- Elisei, R.; Romei, C.; Vorontsova, T.; Cosci, B.; Veremeychik, V.; Kuchinskaya, E.; Basolo, F.; Demidchik, E.P.; Miccoli, P.; Pinchera, A.; et al. RET/PTC rearrangements in thyroid nodules: Studies in irradiated and not irradiated, malignant and benign thyroid lesions in children and adults. J. Clin. Endocrinol. Metab. 2001, 86, 3211–3216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Detours, V.; Wattel, S.; Venet, D.; Hutsebaut, N.; Bogdanova, T.; Tronko, M.D.; Dumont, J.E.; Franc, B.; Thomas, G.; Maenhaut, C. Absence of a specific radiation signature in post-Chernobyl thyroid cancers. Br. J. Cancer 2005, 92, 1545–1552. [Google Scholar] [CrossRef] [Green Version]
- Bounacer, A.; Wicker, R.; Caillou, B.; Cailleux, A.F.; Sarasin, A.; Schlumberger, M.; Suarez, H.G. High prevalence of activating ret proto-oncogene rearrangements, in thyroid tumors from patients who had received external radiation. Oncogene 1997, 15, 1263–1273. [Google Scholar] [CrossRef] [Green Version]
- Bongarzone, I.; Fugazzola, L.; Vigneri, P.; Mariani, L.; Mondellini, P.; Pacini, F.; Basolo, F.; Pinchera, A.; Pilotti, S.; Pierotti, M.A. Age-related activation of the tyrosine kinase receptor protooncogenes RET and NTRK1 in papillary thyroid carcinoma. J. Clin. Endocrinol. Metab. 1996, 81, 2006–2009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lam, K.Y.; Lo, C.Y.; Leung, P.S. High prevalence of RET proto-oncogene activation (RET/PTC) in papillary thyroid carcinomas. Eur. J. Endocrinol. 2002, 147, 741–745. [Google Scholar] [CrossRef] [Green Version]
- Motomura, T.; Nikiforov, Y.E.; Namba, H.; Ashizawa, K.; Nagataki, S.; Yamashita, S.; Fagin, J.A. ret rearrangements in Japanese pediatric and adult papillary thyroid cancers. Thyroid 1998, 8, 485–489. [Google Scholar] [CrossRef]
- Rhoden, K.J.; Johnson, C.; Brandao, G.; Howe, J.G.; Smith, B.R.; Tallini, G. Real-time quantitative RT-PCR identifies distinct c-RET, RET/PTC1 and RET/PTC3 expression patterns in papillary thyroid carcinoma. Lab. Invest. 2004, 84, 1557–1570. [Google Scholar] [CrossRef] [PubMed]
- Fenton, C.L.; Lukes, Y.; Nicholson, D.; Dinauer, C.A.; Francis, G.L.; Tuttle, R.M. The ret/PTC mutations are common in sporadic papillary thyroid carcinoma of children and young adults. J. Clin. Endocrinol. Metab. 2000, 85, 1170–1175. [Google Scholar] [CrossRef] [PubMed]
- Pauws, E.; Tummers, R.F.; Ris-Stalpers, C.; de Vijlder, J.J.; Voute, T. Absence of activating mutations in ras and gsp oncogenes in a cohort of nine patients with sporadic pediatric thyroid tumors. Med. Pediatr. Oncol. 2001, 36, 630–634. [Google Scholar] [CrossRef] [PubMed]
- Kelly, L.M.; Barila, G.; Liu, P.; Evdokimova, V.N.; Trivedi, S.; Panebianco, F.; Gandhi, M.; Carty, S.E.; Hodak, S.P.; Luo, J.; et al. Identification of the transforming STRN-ALK fusion as a potential therapeutic target in the aggressive forms of thyroid cancer. Proc. Natl. Acad. Sci. USA 2014, 111, 4233–4238. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
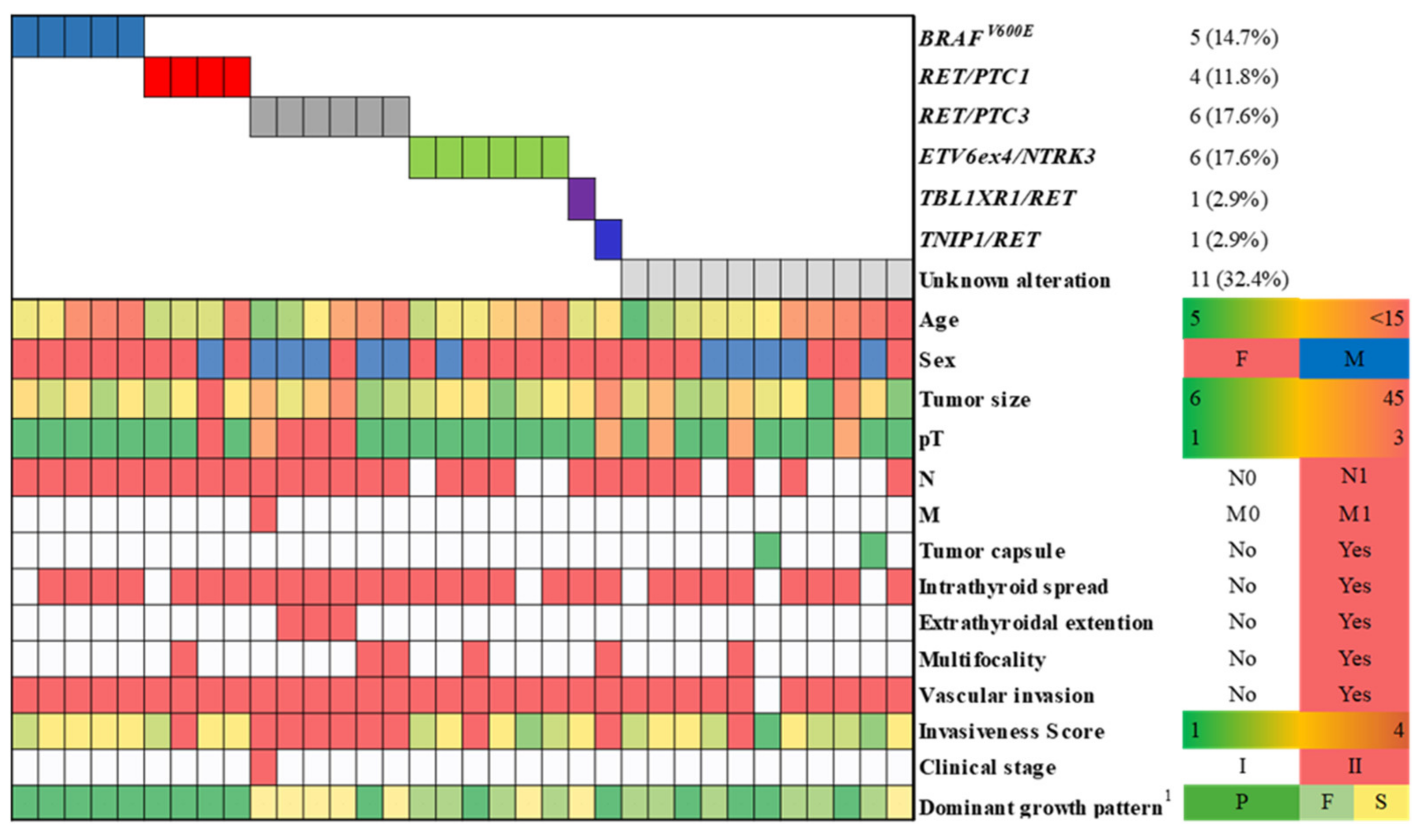
| BRAFV600E | RET/PTC1 | RET/PTC3 | ETV6ex4/NTRK3 | TBL1XR1/RET | TNIP1/RET | Any RET/PTC | Unknown | ||
|---|---|---|---|---|---|---|---|---|---|
| 5 (14.7%) | 4 (11.8%) | 6 (17.6%) | 6 (17.6%) | 1 (2.9%) | 1 (2.9%) | 12 (35.3%) | 11 (32.4%) | ||
| Sex (ref = F) | OR (95% CI) | 0.13 (0.01–3.33) 2 | 9.52 (1.17–76.92) 2 | ||||||
| p-value | 0.215 | 0.035 | |||||||
| Tumor size ≥ 21 mm | OR (95% CI) | 9.00 (0.47–inf) | 2.88 (0.53–15.61) | ||||||
| p-value | 0.100 | 0.219 | |||||||
| pT category 2+3 vs. 1 | OR (95% CI) | 3.86 (0.43–34.44) | 6.00 (0.32–inf) | 3.89 (0.70–21.67) | 0.85 (0.15–4.81) | ||||
| p-value | 0.227 | 0.143 | 0.122 | 0.849 | |||||
| Lymph node metastasis | OR (95% CI) | 19.78 (0.92–425.24) | 0.22 (0.04–1.20) | ||||||
| p-value | 0.057 | 0.080 | |||||||
| N1a | OR (95% CI) | 7.85 (0.49–126.31) | |||||||
| p-value | 0.146 | ||||||||
| N1b | OR (95% CI) | 9.54 (1.40–inf) | 8.92 (1.56–inf) | ||||||
| p-value | 0.025 | 0.017 | |||||||
| Distant metastasis | OR (95% CI) | 7.16 (0.28–184.32) | |||||||
| p-value | 0.235 | ||||||||
| Multifocality | OR (95% CI) | 1.00 (0.05–inf) | |||||||
| p-value | 0.500 | ||||||||
| Extrathyroidal extension | OR (95% CI) | 18.73 (0.73–483.93) | 7.07 (0.40–123.84) | ||||||
| p-value | 0.077 | 0.181 | |||||||
| Tumor capsule | OR (95% CI) | 3.90 (inf–inf) | 8.34 (0.50–138.58) | ||||||
| p-value | 0.998 | 0.139 | |||||||
| Invasiveness score | |||||||||
| 3 | OR (95% CI) | 0.15 (0.01–3.80) | |||||||
| p-value | 0.251 | ||||||||
| 4 | OR (95% CI) | 4.41 (1.35–inf) | 12.35 (1.93–78.96) | 0.15 (0.02–1.27) | |||||
| p-value | 0.021 | 0.008 | 0.081 | ||||||
| Dominant component | |||||||||
| papillary | OR (95% CI) | 6.49 (1.05–inf 3) | 15.09 (0.51–450.29) | ||||||
| p-value | 0.046 | 0.078 | |||||||
| follicular | OR (95% CI) | 10.15 (1.26–81.81) | 0.02 (0.01–0.65) | 4.54 (0.93–22.31) | |||||
| p-value | 0.011 | 0.027 | 0.062 | ||||||
| solid-trabecular | OR (95% CI) | 2.82 (1.03–inf) | 3.40 (0.18–inf) | 6.67 (1.15–38.65) | |||||
| p-value | 0.045 | 0.227 | 0.034 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rogounovitch, T.I.; Mankovskaya, S.V.; Fridman, M.V.; Leonova, T.A.; Kondratovitch, V.A.; Konoplya, N.E.; Yamashita, S.; Mitsutake, N.; Saenko, V.A. Major Oncogenic Drivers and Their Clinicopathological Correlations in Sporadic Childhood Papillary Thyroid Carcinoma in Belarus. Cancers 2021, 13, 3374. https://doi.org/10.3390/cancers13133374
Rogounovitch TI, Mankovskaya SV, Fridman MV, Leonova TA, Kondratovitch VA, Konoplya NE, Yamashita S, Mitsutake N, Saenko VA. Major Oncogenic Drivers and Their Clinicopathological Correlations in Sporadic Childhood Papillary Thyroid Carcinoma in Belarus. Cancers. 2021; 13(13):3374. https://doi.org/10.3390/cancers13133374
Chicago/Turabian StyleRogounovitch, Tatiana I., Svetlana V. Mankovskaya, Mikhail V. Fridman, Tatiana A. Leonova, Victor A. Kondratovitch, Natalya E. Konoplya, Shunichi Yamashita, Norisato Mitsutake, and Vladimir A. Saenko. 2021. "Major Oncogenic Drivers and Their Clinicopathological Correlations in Sporadic Childhood Papillary Thyroid Carcinoma in Belarus" Cancers 13, no. 13: 3374. https://doi.org/10.3390/cancers13133374